Back to Journals » Infection and Drug Resistance » Volume 19
Smoking and Clostridioides difficile Colonization in Adults Aged ≥40 Years: Findings from a Community-Based Gut Microbiota Study
Authors Chen HM, Yang TW, Ko WC ![]() , Hung YP
, Hung YP ![]() , Tsai CS, Tsai PJ
, Tsai CS, Tsai PJ ![]()
Received 21 October 2025
Accepted for publication 16 January 2026
Published 17 February 2026 Volume 2026:19 571988
DOI https://doi.org/10.2147/IDR.S571988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Hong-Ming Chen,1,2,* Te-Wei Yang,3,* Wen-Chien Ko,3,4 Yuan-Pin Hung,5,6 Chin-Shiang Tsai,3,4 Pei-Jane Tsai7
1Institute of Basic Medical Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Yanshuei District Health Station, Tainan, Taiwan; 3Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 4Center for Infection Control, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 5Department of Microbiology and Immunology, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 6Department of Internal Medicine, Tainan Hospital, Ministry of Health and Welfare, Tainan, Taiwan; 7Department of Medical Laboratory Science and Biotechnology, College of Medicine, National Cheng Kung University, Tainan, Taiwan
*These authors contributed equally to this work
Correspondence: Pei-Jane Tsai, Department of Medical Laboratory Science and Biotechnology, College of Medicine, National Cheng Kung University, Tainan, Taiwan, Email [email protected]
Background: Asymptomatic Clostridioides difficile colonization (CdC) serves as a reservoir for pathogen transmission and may precede clinical infection. While risk factors for CdC have been well described in hospitalized populations, community-based data—particularly regarding lifestyle-associated factors and gut microbiota alterations—remain limited in Taiwan. This study aimed to determine the prevalence and risk factors of community-acquired CdC and to explore associated gut microbiota differences.
Materials and Methods: We conducted a cross-sectional study analyzing 250 residual stool samples from adults aged ≥ 40 years who participated in community health screenings in Tainan City between 2006 and 2009. CdC was detected by polymerase chain reaction targeting the triosephosphate isomerase (tpi) gene. Demographic characteristics, lifestyle factors, and laboratory parameters were collected and analyzed. Exploratory 16S rRNA gene sequencing was performed on selected samples to compare gut microbiota composition between CdC and non-CdC groups.
Results: The prevalence of CdC was 11.6% (29/250). Cigarette smoking was identified as the sole independent factor associated with CdC (adjusted OR 2.35, 95% CI 1.05– 5.28; P = 0.038). Exploratory microbiota analysis revealed differences in community composition between CdC and non-CdC samples, including increased relative abundance of Proteobacteria in CdC.
Conclusion: Cigarette smoking was associated with an increased likelihood of community-acquired CdC in southern Taiwan. Distinct gut microbiota profiles were observed in individuals with CdC, supporting a potential link between smoking-related microbiota alterations and susceptibility to asymptomatic colonization. These findings underscore the relevance of modifiable lifestyle factors in the epidemiology of community CdC and warrant further investigation.
Keywords: Clostridioides difficile colonization, smoking, gut microbiota, community, Taiwan
Introduction
Clostridioides difficile (C. difficile) is a gram-positive, anaerobic, spore-forming bacillus that can cause a spectrum of gastrointestinal diseases ranging from mild diarrhea to fulminant colitis with toxic megacolon.1,2 C. difficile infection (CDI) has become a major global public health concern, with increasing incidence reported in both healthcare and community settings.3 While CDI has traditionally been regarded as a healthcare-associated infection, accumulating evidence indicates that asymptomatic C. difficile colonization (CdC) plays a critical role in the epidemiology of CDI.4 Asymptomatic carriers may serve as a reservoir for transmission and are at increased risk of subsequent symptomatic infection, particularly when host defenses or gut microbiota integrity are disrupted.5
Most existing epidemiological studies on CdC have focused on hospitalized populations, in whom established risk factors include antibiotic exposure, hospitalization, gastric acid suppression, tube feeding, and immunosuppressive therapies.6 In contrast, data on CdC in community-dwelling adults remain limited, especially in population in Taiwan. Community-acquired CdC is epidemiologically important because it represents a potential upstream source of C. difficile introduced into healthcare facilities and may reflect distinct risk profiles compared with hospitalized patients.7 However, the prevalence, risk factors, and microbiota characteristics of community-acquired CdC in Taiwan have not been well characterized.
The gut microbiota plays a central role in colonization resistance against C. difficile through mechanisms including bile acid metabolism, nutrient competition, short-chain fatty acid production, and modulation of host immune responses.8,9 Disruption of the gut microbial ecosystem, or dysbiosis, has been consistently associated with increased susceptibility to C. difficile colonization and infection.10 While antibiotic exposure is the most well-recognized driver of dysbiosis, lifestyle-related factors may also influence gut microbiota composition and function.11 Cigarette smoking has been shown to alter gut microbial diversity and relative abundance of key bacterial taxa, potentially impairing colonization resistance.12,13 Epidemiological studies have reported higher rates of CDI among smokers compared with non-smokers,14 but the association between smoking, gut microbiota alterations, and CdC in community settings remains poorly understood.
In Taiwan, previous studies on C. difficile have largely focused on hospitalized patients, toxigenic strains, or clinical infection outcomes, with various colonization rates in inpatient populations.15,16 Investigations of gut microbiota in Taiwanese patients have primarily addressed CDI treatment and microbiota restoration, rather than asymptomatic colonization in the community.17,18 To date, community-based data integrating epidemiological risk factors and gut microbiota profiling for CdC in Taiwan are scarce. Therefore, we conducted a cross-sectional, community-based study among adults aged ≥40 years who participated in routine health screening programs in southern Taiwan. The objectives were to determine the prevalence of community-acquired CdC, identify associated demographic and lifestyle-related risk factors—particularly cigarette smoking—and explore gut microbiota differences between individuals with and without CdC using 16S rRNA metagenomic analysis. By integrating epidemiological and microbiome data, this study aims to provide insight into potential lifestyle-associated pathways contributing to CdC and to generate hypotheses for future longitudinal and mechanistic investigations.
Materials and Methods
Sample Collection, Genomic DNA Extraction and C. difficile Colonization Detection
This cross-sectional study utilized residual fecal DNA samples obtained from the Tainan City Government Biobank. A total of 250 stool DNA samples were derived from immunochemical fecal occult blood test (iFOBT) specimens collected during community-based health screening programs conducted by the former Tainan County Health Bureau between 2006 and 2009. These screening programs were part of a nationwide colorectal cancer screening initiative in Taiwan, targeting adults aged ≥40 years, with triennial screening for individuals aged 40–64 years and annual screening for those aged ≥65 years. Participation in the screening program was voluntary. Therefore, the study population may not fully represent all community-dwelling adults, particularly those who prefer alternative screening modalities such as colonoscopy. This potential selection bias was considered in the interpretation of the results.
Fecal DNA Extraction and Detection of C. difficile Colonization
Fecal DNA was extracted from residual iFOBT specimens using a phenol/chloroform/isoamyl alcohol extraction method. Extracted DNA samples were stored long-term at −25 °C without additional preservatives, consistent with standard biobank storage procedures at the time of collection. Prior to analysis, DNA integrity was assessed by agarose gel electrophoresis. CdC was identified by polymerase chain reaction (PCR) targeting the triosephosphate isomerase (tpi) gene, a species-specific housekeeping gene widely used for molecular identification of C. difficile.19 The tpi gene was selected to detect overall C. difficile carriage regardless of toxigenic status, as the primary objective of this study was to assess CdC and its epidemiological associations rather than to differentiate toxigenic and non-toxigenic strains.
PCR amplification was performed using previously validated primers (forward: 5′-ATT TAC AGGAGA AGT TTC ACC TCT-3′ and reverse: 5′-GCC CAG ATT GGC TCA TAT GCA AC-3′). Detection of the expected 300-bp tpi amplicon was considered indicative of CdC.
Collection of Demographic, Lifestyle, and Laboratory Variables
Demographic characteristics, lifestyle factors, and laboratory data were obtained from standardized questionnaires and medical records maintained by the Tainan County Health Bureau. Lifestyle variables were collected as categorical data and included cigarette smoking status, alcohol consumption, betel nut use, oral hygiene practices, physical activity, and dietary habits. Laboratory parameters included serum albumin, liver enzymes, blood urea nitrogen, serum creatinine, uric acid, fasting glucose, lipid profile, complete blood count, hepatitis B surface antigen, hepatitis C antibody, and iFOBT results.
16S rRNA Metagenomic Analysis of the Gut Microbiota
To explore gut microbiota differences associated with CdC and smoking status, 16S rRNA gene sequencing was performed on a subset of samples. Ten samples from participants with CdC and ten samples from participants without CdC (NCdC) were selected based on DNA availability and quality. The microbiota analysis was designed as an exploratory, hypothesis-generating investigation rather than a definitive comparative analysis.
Sequencing targeted the bacterial 16S rRNA gene, and relative abundances of bacterial taxa were analyzed at the phylum and genus levels. Microbiota composition was visualized using bar plots and heatmaps of relative abundance. Linear discriminant analysis effect size (LEfSe) was applied to identify taxa differentially enriched between groups, emphasizing effect size and biological relevance.
Statistical Analyses
Statistical analyses were performed using SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as median with interquartile range (IQR) and were compared using the Mann–Whitney U-test. Categorical variables are presented as counts and percentages and were compared using the Fisher’s exact test, as appropriate.
Variables with P < 0.10 in univariate analysis were considered for inclusion in multivariable logistic regression models to identify independent factors associated with C. difficile colonization. Odds ratios (ORs) and adjusted odds ratios (aORs) are reported with 95% confidence intervals (CIs). A two-sided P value < 0.05 was considered statistically significant.
Ethic Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of National Cheng Kung University Hospital (A-ER-106-383). Based on this approval, permission was obtained from the Tainan City Government to access specimens from the Tainan City Government Biobank. All subjects provided informed consent prior to specimen storage.
Results
In this study, 250 residual stool specimens from adult participants were collected and subjected to genomic DNA extraction and C. difficile tpi gene PCR analysis. A flowchart of the process is shown in Figure 1. As shown in Table 1, twenty-nine (11.6%) participants tested positive tpi genes in their stool samples, indicating C. difficile carriage. The remaining 221 (88.4%) participants did not have a C. difficile carriage. The average age was similar between CdC and NCdC group, approximately 50 (51 [47.5–53.5] vs 50 [44–53], P = 0.140). A higher proportion of participants aged > 60 years was found in CdC group than in NCdC group, with statistical significance in the univariate analysis (13.8% vs 3.2%, P=0.027). In univariate analysis, male sex was more frequent in the CdC group than in the NCdC group (55.2% vs 42.5%), although this association did not reach statistical significance. There were no significant differences in biochemical laboratory data, hemogram data, or positive iFOBT proportions between the two groups. In terms of lifestyle, CdC group had a higher percentage of smoking history than NCdC group (41.4% vs 23.5%, P=0.042). No significant differences between the two groups in terms of body fat, alcohol consumption, betel nut use, oral hygiene, physical activity, or dietary habits. Multivariate logistic regression analysis showed that smoking was independently associated with CdC (Table 2).
 |
Figure 1 Flowchart of participant selection and detection of Clostridioides difficile colonization in this community-based study. |
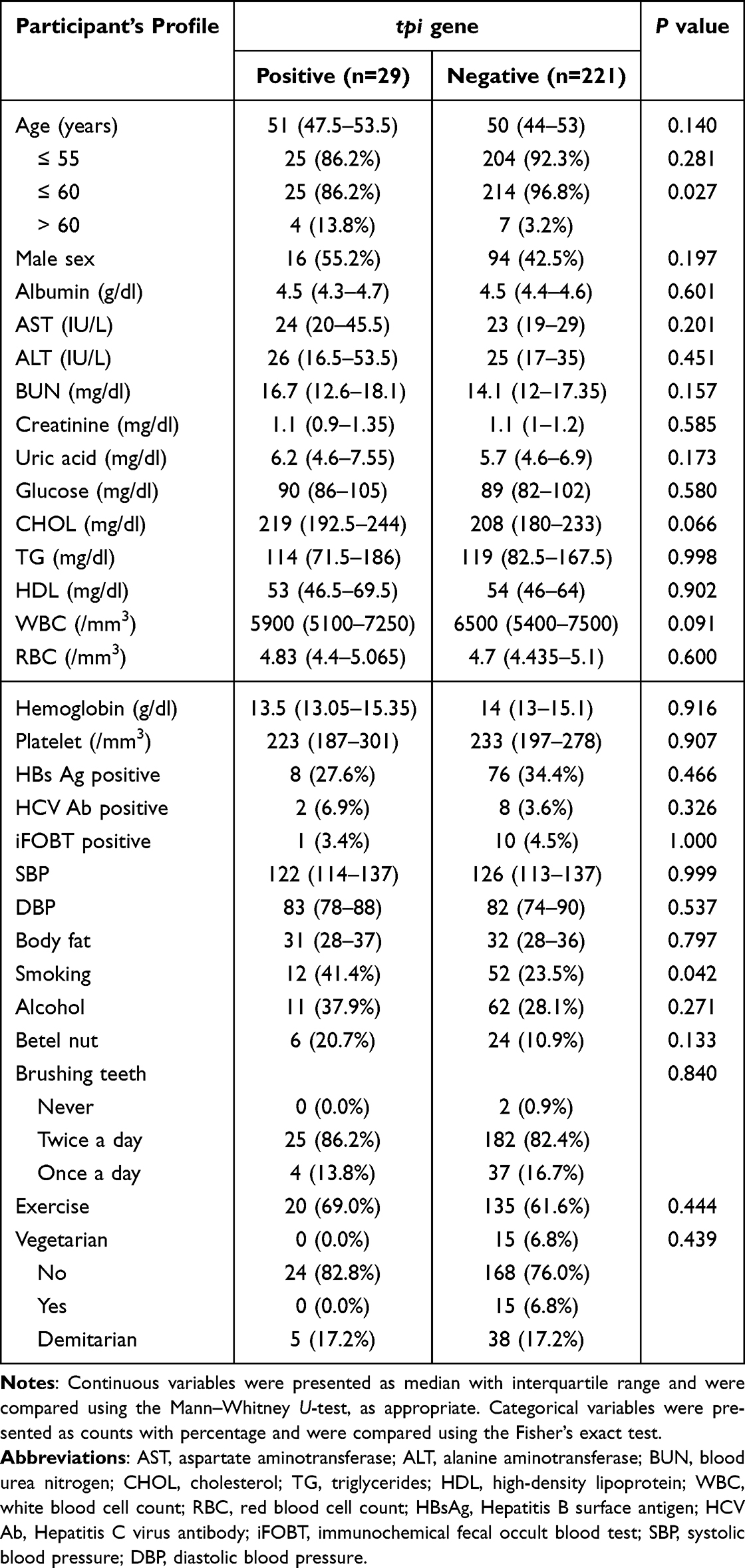 |
Table 1 Baseline Demographic Characteristics, Lifestyle Factors, and Laboratory Parameters According to Clostridioides difficile Colonization Status Among Community Residents (n=250) |
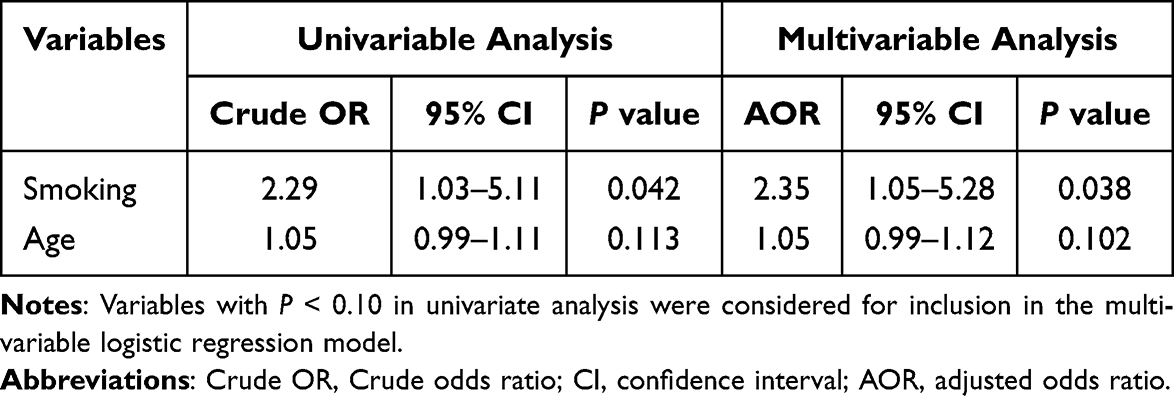 |
Table 2 Multivariable Logistic Regression for Clinical Factors Associated with Clostridioides difficile Colonization in the Community |
In the 16S metagenome analysis of the gut microbiota, Firmicutes was the most abundant phylum, followed by Bacteroidetes, Actinobacteria and Proteobacteria in both CdC and NCdC samples. Proteobacteria was more abundant in CdC than in NCdC; in contrast, Bacteroidetes and Fusobacteria were more abundant in NCdC than in CdC (Figure 2). At the genus level, Subdoligranulum, Klebsiella, Blautia, and Bifidobacterium were more abundant in CdC than in NCdC. Romboutsia, Faecalibacterium, Enterococcus, and Prevotella 9 (a SILVA genus-level taxon label)20 were more abundant in NCdC than in CdC (Figure 3). The relative abundances of 35 different genera in both CdC and NCdC groups are depicted in a species abundance heatmap (Figure 4). LEfSe analysis identified enrichment of the genera Virgibacillus and Oceanobacillus in the CdC group, with a linear discriminant analysis (LDA) score above 4 (Figure 5). However, the order Fusobacteriales (p_Fusobacteria) and family Prevotellaceae (g_Prevotella 9) were identified as taxa enriched in the NCdC group, with LDA score below −4.
 |
Figure 2 Comparison of gut microbiota composition at the phylum level between participants with Clostridioides difficile colonization (CdC) and those without colonization (NCdC), based on exploratory 16S rRNA gene sequencing. (A) Comparison of relative abundances between the CdC and NCdC groups. (B) Relative abundances of selected phyla in individual samples from the CdC (n = 10) and NCdC (n = 10) groups. At the phylum level, Proteobacteria showed higher relative abundances in the CdC group, whereas Bacteroidetes and Fusobacteria showed higher relative abundances in the NCdC group. |
 |
Figure 3 Comparison of gut microbiota composition at the genus level between participants with Clostridioides difficile colonization (CdC) and those without colonization (NCdC) based on exploratory 16S rRNA gene sequencing. (A) Comparison of relative abundances between the CdC and NCdC groups. (B) Relative abundances of selected genera in individual samples from the CdC (n = 10) and NCdC (n = 10) groups. Taxa are labeled according to taxonomic prefixes (p_, phylum; o_, order; g_, genus). Genera including Subdoligranulum, Klebsiella, Blautia, and Bifidobacterium showed higher relative abundances in the CdC group, whereas Romboutsia, Faecalibacterium, Enterococcus, and Prevotella 9 (a SILVA genus-level taxon label)20 showed higher relative abundances in the NCdC group. |
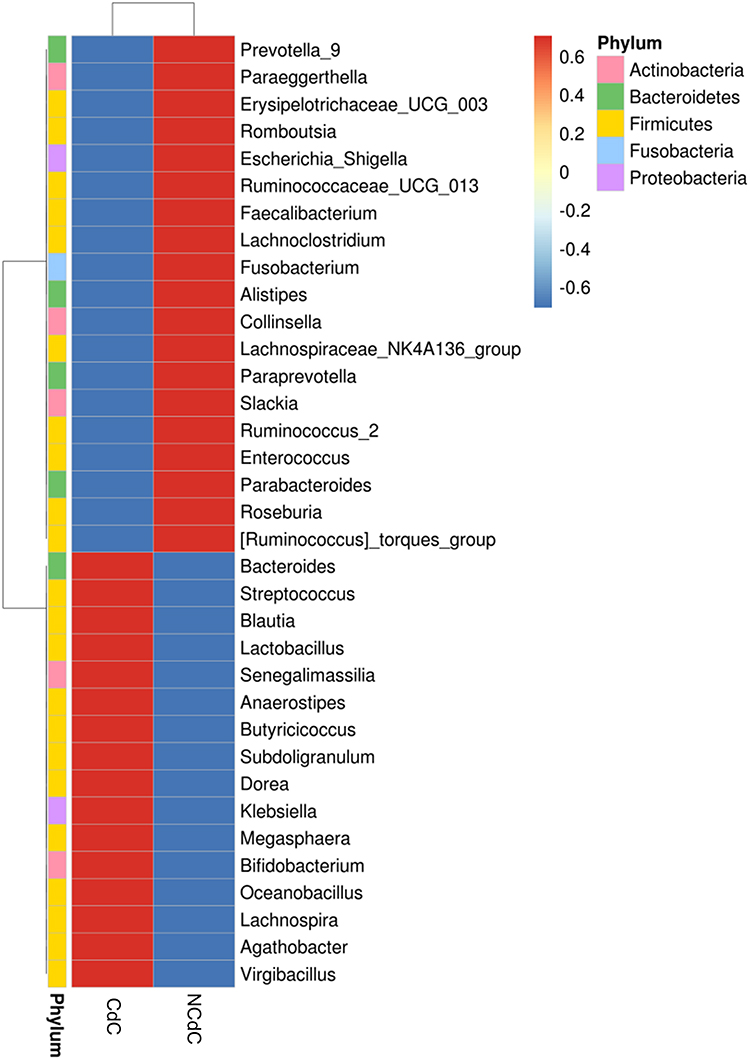 |
Figure 4 Heatmap showing the relative abundance of the 35 most prevalent bacterial genera across samples from participants with Clostridioides difficile colonization (CdC) and those without colonization (NCdC) in the exploratory microbiota analysis. |
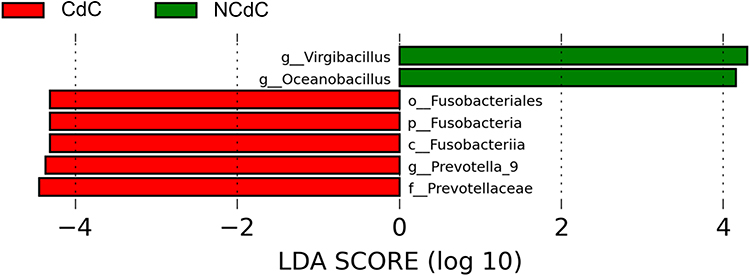 |
Figure 5 Linear discriminant analysis effect size (LEfSe) identifying bacterial taxa differentially enriched between participants with Clostridioides difficile colonization (CdC) and those without colonization (NCdC) in the exploratory microbiota analysis. Taxa are labeled according to standard taxonomic prefixes (p_, phylum; o_, order; g_, genus). LDA scores indicate the effect size of differentially abundant taxa. |
16S metagenome analysis of the gut microbiota in smokers and non-smokers showed that the phyla Actinobacteria and Firmicutes were more abundant in smokers than in non-smokers (Figure 6). In contrast, the phyla Chloroflexi, Proteobacteria, and Fusobacteria were more abundant in non-smokers than in smokers. The genera Romboutsia, Blautia, and Bifidobacterium were more abundant in smokers than in non-smokers. However, the genera Bacteroides, Klebsiella, Agathobacter, and Enterococcus were more abundant in non-smokers than in smokers.
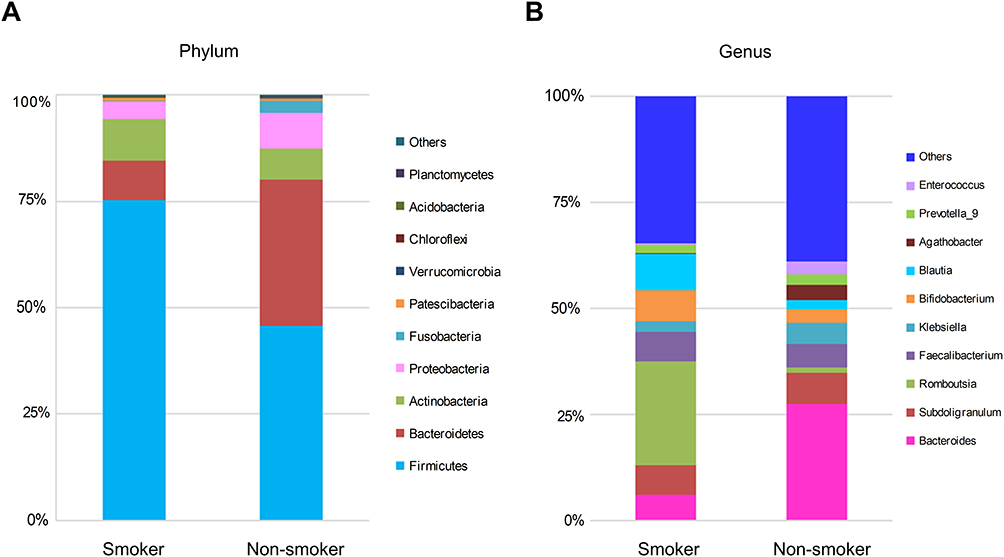 |
Figure 6 Exploratory comparison of gut microbiota composition between smokers and non-smokers at the phylum (A) and genus (B) levels based on 16S rRNA gene sequencing. |
Discussion
In this community-based cross-sectional study of adults aged ≥40 years in southern Taiwan, cigarette smoking was identified as an independent risk factor for CdC. Individuals with CdC also exhibited distinct gut microbiota profiles compared with non-colonized participants. Although causality cannot be inferred, these findings suggest a potential link between smoking-related gut microbiota alterations and susceptibility to CdC in the community. By focusing on community-dwelling adults rather than hospitalized populations, this study highlights asymptomatic colonization as a potential upstream reservoir that may contribute to C. difficile transmission and subsequent healthcare-associated infection.
While established risk factors for CdC have been largely derived from inpatient settings,21 lifestyle-associated factors in the community remain underexplored. Smoking has been associated with an increased risk of CDI in population-based studies,14 but data linking smoking to CdC and gut microbiota changes are limited. Our findings provide epidemiological support for the hypothesis that smoking-related dysbiosis may partially impair colonization resistance, thereby facilitating CdC even in otherwise healthy individuals. Age did not remain independently associated with CdC in multivariable analysis, suggesting that microbiota- and lifestyle-related factors may play a more prominent role than chronological age alone in this population. This attenuation may also be attributable to the relatively narrow age distribution of this community-based cohort, which predominantly included adults aged ≥40 years with limited representation of the very elderly.
In the exploratory 16S rRNA metagenomic analysis, we observed differences in gut microbiota composition associated with smoking status and CdC. Smokers exhibited higher relative abundances of Actinobacteria and Firmicutes, whereas non-smokers showed relatively higher proportions of Proteobacteria and Fusobacteria. These findings are consistent with prior reports indicating that smoking is associated with alterations in gut microbial composition,13,22 although the specific taxa affected have varied across studies. Given the limited sample size, these observations should be interpreted cautiously and viewed as hypothesis-generating rather than definitive.
Comparison between CdC and NCdC groups revealed distinct microbial profiles, including increased relative abundance of Proteobacteria and enrichment of certain genera such as Klebsiella in individuals with CdC. Alterations in taxa associated with short-chain fatty acid production and colonization resistance have been implicated in previous studies of CdC.23 However, inconsistencies across studies and the presence of taxa with overlapping functional roles underscore the complexity of host–microbiota–pathogen interactions. In this context, our findings suggest that gut microbiota differences may contribute to CdC susceptibility but are unlikely to act as the sole determinant.
LEfSe analysis identified Virgibacillus and Oceanobacillus as taxa enriched in the CdC group. These genera have been reported in microbial community analysis about fermentation starters,24 but less described in the human gut. Their biological relevance remains unclear. Rather than serving as definitive biomarkers, their identification in this study highlights potential ecological signatures associated with CdC that warrant validation in larger, longitudinal cohorts with functional microbiome profiling.
Several limitations of this study should be acknowledged. First, the detection of CdC was based on PCR targeting the tpi gene, which identifies species-level carriage but does not distinguish between toxigenic and non-toxigenic strains. Consequently, the reported colonization rate may overestimate the prevalence of toxigenic C. difficile. However, the primary objective of this study was to characterize asymptomatic colonization as an epidemiological reservoir rather than to assess toxin-mediated disease or current prevalence estimation, and non-toxigenic strains may still reflect relevant ecological dynamics within the gut microbiota.
Second, the cross-sectional design precludes causal inference regarding the relationships among smoking, gut microbiota alterations, and CdC. Information on certain established risk factors, including prior antibiotic exposure, proton pump inhibitor use, and recent hospitalization, was not available and may have contributed to residual confounding. Third, participation in the community screening program was voluntary, which may introduce selection bias and limit the generalizability of the findings to individuals who preferentially undergo alternative screening modalities.
Finally, the gut microbiota analysis was conducted on a limited number of samples and was intended as an exploratory, hypothesis-generating investigation. The small sample size restricts statistical power and limits the ability to draw definitive conclusions regarding specific microbial taxa. Future longitudinal studies with larger cohorts, detailed medication histories, and functional microbiome analyses are warranted to validate these findings and to elucidate the mechanistic pathways linking lifestyle factors, gut microbiota, and CdC.
In conclusion, this community-based study of adults aged ≥40 years in southern Taiwan showed cigarette smoking was identified as an independent risk factor for CdC. Individuals with CdC exhibited distinct gut microbiota profiles compared with non-colonized participants, suggesting a potential association between smoking-related microbiota alterations and colonization susceptibility. Although causal relationships cannot be established, these findings highlight the importance of considering modifiable lifestyle factors in the epidemiology of community-acquired CdC. Further longitudinal studies with larger cohorts and functional microbiome analyses are needed to validate these observations and to clarify their implications for C. difficile transmission and prevention.
Acknowledgments
We wish to express our deepest gratitude to all Tainan citizens who participated in this study. We also express our gratitude to all team members involved in this research for their dedication and to the Tainan City Government Biobank for providing fecal DNA samples and related data.
Author Contributions
Chin-Shiang Tsai and Pei-Jane Tsai contributed equally to this work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Cheng Kung University Hospital, Taiwan [NCKUH-11410014; NCKUH-11511003].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Czepiel J, Dróżdż M, Pituch H, et al. Clostridium difficile infection: review. Eur J Clin Microbiol Infect Dis. 2019;38:1211–10. doi:10.1007/s10096-019-03539-6
2. Di Bella S, Sanson G, Monticelli J, et al. Clostridioides difficile infection: history, epidemiology, risk factors, prevention, clinical manifestations, treatment, and future options. Clin Microbiol Rev. 2024;37:e0013523. doi:10.1128/cmr.00135-23
3. Finn E, Andersson FL, Madin-Warburton M. Burden of Clostridioides difficile infection (CDI) - a systematic review of the epidemiology of primary and recurrent CDI. BMC Infect Dis. 2021;21:456. doi:10.1186/s12879-021-06147-y
4. Furuya-Kanamori L, Marquess J, Yakob L, et al. Asymptomatic Clostridium difficile colonization: epidemiology and clinical implications. BMC Infect Dis. 2015;15:516. doi:10.1186/s12879-015-1258-4
5. Ling Z, Ding W, Liu X, et al. Gut microbiota dysbiosis and systemic immune dysfunction in critical ill patients with multidrug-resistant bacterial colonization and infection. J Transl Med. 2025;23:981. doi:10.1186/s12967-025-07049-2
6. Anjewierden S, Han Z, Brown AM, Donskey CJ, Deshpande A. Risk factors for Clostridioides difficile colonization among hospitalized adults: a meta-analysis and systematic review. Infect Control Hosp Epidemiol. 2021;42:565–572. doi:10.1017/ice.2020.1236
7. Gupta A, Khanna S. Community-acquired Clostridium difficile infection: an increasing public health threat. Infect Drug Resist. 2014;7:63–72. doi:10.2147/IDR.S46780
8. Pickard JM, Zeng MY, Caruso R, Núñez G. Gut microbiota: role in pathogen colonization, immune responses and inflammatory disease. Immunol Rev. 2017;279:70–89. doi:10.1111/imr.12567
9. Naz F, Petri WA. Host immunity and immunization strategies for Clostridioides difficile infection. Clin Microbiol Rev. 2023;36:e0015722. doi:10.1128/cmr.00157-22
10. Spigaglia P. Clostridioides difficile and gut microbiota: from colonization to infection and treatment. Pathogens. 2024;13:646. doi:10.3390/pathogens13080646
11. Ren Y, Wu J, Wang Y, et al. Lifestyle patterns influence the composition of the gut microbiome in a healthy Chinese population. Sci Rep. 2023;13:14425. doi:10.1038/s41598-023-41532-4
12. Huang C, Shi G. Smoking and microbiome in oral, airway, gut and some systemic diseases. J Transl Med. 2019;17:225. doi:10.1186/s12967-019-1971-7
13. Gui X, Yang Z, Li MD. Effect of cigarette smoke on gut microbiota: state of knowledge. Front Physiol. 2021;12:673341. doi:10.3389/fphys.2021.673341
14. Rogers MAM, Greene MT, Saint S, et al. Higher rates of Clostridium difficile infection among smokers. PLoS One. 2012;
15. Hung YP, Tsai PJ, Hung KH, et al. Impact of toxigenic Clostridium difficile colonization and infection among hospitalized adults at a district hospital in southern Taiwan. PLoS One. 2012;7:1–7. doi:10.1371/journal.pone.0042415
16. Hung YP, Lee JC, Lin HJ, et al. Clinical impact of Clostridium difficile colonization. J Microbiol Immunol Infect. 2015;48:241–248. doi:10.1016/j.jmii.2014.04.011
17. Lee PC, Chang TE, Wang YP, et al. Alteration of gut microbial composition associated with the therapeutic efficacy of fecal microbiota transplantation in Clostridium difficile infection. J Formos Med Assoc. 2022;121:1636–1646. doi:10.1016/j.jfma.2021.11.001
18. Lee CC, Tu YC, Wu HT, et al. Clostridium Butyricum miyairi bacteriocin treatment for Clostridioides difficile infections with clinical isolates: insights from in vitro, ex vivo, and mouse model studies. J Glob Antimicrob Resist. 2025;44:49–58. doi:10.1016/j.jgar.2025.03.007
19. Dhalluin A, Lemée L, Pestel-Caron M, et al. Genotypic differentiation of twelve Clostridium species by polymorphism analysis of the triosephosphate isomerase (tpi) gene. Syst Appl Microbiol. 2003;26:90–96. doi:10.1078/072320203322337362
20. Henderson G, Yilmaz P, Kumar S, et al. Improved taxonomic assignment of rumen bacterial 16S rRNA sequences using a revised SILVA taxonomic framework. PeerJ. 2019;7:e6496. doi:10.7717/peerj.6496
21. Loo VG, Bourgault A-M, Poirier L, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. 2011;365:1693–1703. doi:10.1056/NEJMoa1012413
22. Imade EE, Obayagbona NO. Impact of cigarette smoking on gut microbial dysbiosis: a structured literature review. Gut Microbiome. 2024;
23. Seekatz AM, Theriot CM, Rao K, et al. Restoration of short chain fatty acid and bile acid metabolism following fecal microbiota transplantation in patients with recurrent Clostridium difficile infection. Anaerobe. 2018;53:64–73. doi:10.1016/j.anaerobe.2018.04.001
24. Chen C, Ni D, Yang Y, Tian J, Yang F, Ye X. Characterizing the microbial community constructure and the metabolites among different colour Moutai Daqu. Food Chem X. 2025;26:102223. doi:10.1016/j.fochx.2025.102223
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.