Back to Journals » Clinical Ophthalmology » Volume 14
Small Incision Lenticule Extraction (SMILE) in Patients with Corneal Guttae
Received 15 June 2020
Accepted for publication 5 August 2020
Published 25 August 2020 Volume 2020:14 Pages 2485—2490
DOI https://doi.org/10.2147/OPTH.S267847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bu Ki Kim,1 Young Taek Chung2
1Onnuri Smile Eye Clinic, Gangnam-Daero 65 Gil, Seoul, Seocho-gu, Republic of Korea; 2Onnuri Eye Hospital, Baekje-Daero, Wansan-Gu, Jeonju-si, Jeollabuk-do, Republic of Korea
Correspondence: Young Taek Chung 325, Baekje-Daero, Wansan-Gu, Jeonju-si, Jeollabuk-do, Republic of Korea
Tel +82 63 277 2774
Email [email protected]
Purpose: To report 12-month results of small incision lenticule extraction (SMILE) in the treatment of myopia with corneal guttae (CG).
Methods: We conducted a retrospective analysis of 12 eyes from six patients who had preoperative CG without clinical sign of Fuchs’ endothelial corneal dystrophy (FECD) and had SMILE for correction of myopia. Preoperative and 12-month postoperative measurements included uncorrected distance visual acuity (UDVA), spherical equivalent (SE), endothelial cell density (ECD), the coefficient of variation (CV), the percentage of hexagonal cells (HEX), and central corneal thickness (CCT). The changes in ECD, CV, HEX, and CCT after SMILE were subjected to statistical analysis.
Results: Twelve months postoperatively, the mean SE was − 0.10 ± 0.32 D and all eyes had a UDVA of 0 logMAR or better. No eyes developed corneal edema or other complication during the follow-up period. There were no significant changes in the ECD, CV, or HEX at 12 months (all p> 0.05).
Conclusion: SMILE yielded improvement in visual acuity and no adverse effects to corneal endothelial cells were found when correcting myopia or myopic astigmatism in patients with CG. However, studies with a greater number of patients and longer follow-up periods are needed to establish the long-term outcomes and safety.
Keywords: small incision lenticule extraction, SMILE, corneal guttae, Fuchs’ endothelial corneal dystrophy
Introduction
Primary corneal guttae (CG) is associated with abnormal excrescences of basement membrane and fibrillar collagens produced by distressed endothelium. They are seen as a Descemet’s membrane with a beaten metal appearance on slit-lamp examination and as dark areas on specular microscopy.1 Secondary CG is associated with degenerative corneal disease, trauma, and inflammation and that usually disappears on removal of the cause. Primary CG, however, occasionally progress to Fuchs’ endothelial dystrophy (FECD) with corneal endothelial decompensation.2 Some studies reported endothelial cell loss and loss of best corrected visual acuity after laser in situ keratomileusis (LASIK) in patients with mild CG or FECD.3–5 The exact mechanism of endothelial damage after LASIK remains unknown, but several theories have been postulated, including mechanical trauma from shockwaves, an acute rise in intraocular pressure (IOP), and stromal hydration beyond which the abnormal endothelium cannot recover.6,7
Small incision lenticule extraction (SMILE) is a relatively new procedure used to correct myopia and myopic astigmatism, only utilizing a femtosecond laser to make an intrastromal lenticule, after which the lenticule is extracted though a small incision.8 Because SMILE does not include an excimer laser like those used in cases involving endothelial damage after LASIK in patients with CG, studies to determine the safety of SMILE in patients with CG are needed. However, no study involving SMILE in patients with CG has been reported. In this study, the outcomes of SMILE in 12 eyes of six patients who had preoperative CG without clinical sign of FECD were reviewed.
Methods
Study Design
We conducted a retrospective analysis of 12 eyes (six patients) who had preoperative CG, that were treated with SMILE at the Onnuri Smile Eye Clinic, Seoul, Korea, from August 2016 to April 2018. The study was approved by the Public Internal Regulatory Board of the Ministry of Health and Welfare, Korea (P01-201901-21-009). All procedures conformed to the tenets of the Declaration of Helsinki, and written, informed consent for study participation was obtained from all participants. Inclusion criteria for the study were, minimum age of 18 years, corrected distance visual acuity (CDVA) of 20/25 or better, and had central CG on specular microscopic exam. Exclusion criteria were, a prior history of ocular trauma or surgery, diagnosed autoimmune disease, corneal topographic findings suspicious for keratoconus and corneal scarring or stromal edema on slit-lamp examination.
Preoperatively, patients underwent a complete ophthalmologic examination including uncorrected distance visual acuity (UDVA), CDVA, manifest and cycloplegic refractions, slit-lamp microscopy examination, IOP, dilated fundus examination, dual rotating Scheimpflug analyzer (Galilei®; Ziemer Ophthalmology, Port, Switzerland), and specular microscopy (noncom Robo-ca®; Konan Medical, Hyogo, Japan).
Surgical Technique
The same experienced surgeon (KBK) performed SMILE procedure using Visumax® femtosecond laser (Carl Zeiss Meditec AG, Jena, Germany), and the target refraction was emmetropia in all eyes. The following laser parameters were used: 500 kHz repetition rate, 140 nJ pulse energy, 4.0 µm spot spacing, 120 µm cap thickness, 6.5 to 6.7 mm lenticule diameter according to the diameter of the scotopic pupil and manifest refraction. The lenticule was separated with a blunt spatula using Chung’s swing technique, as described previously.9 After removing the lenticule, the stromal pocket was flushed with balanced salt solution (BSS; Alcon). After the procedure, patients were treated with 0.5% moxifloxacin (Vigamox®; Alcon) for five days, 0.1% fluorometholone (Opti-V®; Reyon Pharmaceutical, Seoul, Republic of Korea) for four weeks, and preservative-free hyaluronic acid lubricating drops (Tearinfree®; DHP Korea, Seoul, Republic of Korea) for at least four weeks.
Endothelial Measurements
The corneal endothelial cells were assessed using a noncontact specular microscopy (noncom Robo-ca®; Konan Medical, Hyogo, Japan) by a single experienced examiner before and 12 months after SMILE. The patient was positioned on a chair in front of the specular microscopy, and the chin was placed on the chin rest. The patient was asked to fixate the eye for a few seconds on the light coming from inside the device until the instrument automatically took a clear image of the corneal endothelium. The measurements were done three times and the average was taken. The parameters used for analysis included endothelial cell density (ECD) (cells/mm2), the coefficient of variation (CV) of the cell area (standard deviation divided by the mean), the percentage of hexagonal cells (HEX), and central corneal thickness (CCT) values. The postoperative ECD was adjusted by the following formula, because the magnification after SMILE procedure was altered and the amount of endothelial cells were over or underestimated:10,11 ECDt=[1+(CCTpost ⨰ Kpost/nc)]/[1+(CCTpre ⨰ Kpre/nc)] ⨰ ECDm, where ECDt and ECDm refer to the true value and the measured value of postoperative ECD, respectively, CCTpre and CCTpost are the CCT preoperatively and postoperatively, Kpre and Kpost are the keratometry of the anterior surface of cornea before and after procedure, and the refractive index of the cornea is nc=1.376. CG was graded according to the scale described by Zoega et al.1
Statistical Analysis
Statistical analyses were performed using SPSS for Windows statistical software (ver. 20.0; IBM Corporation, Armonk, NY, USA). Wilcoxon test or Mann–Whitney U-test were used to identify differences between values. All values are given as means ±SD. Statistical analyses of visual acuity used logarithms of the minimum angle of resolution (logMAR). Statistical differences with p<0.05 were considered significant.
Results
This study included 12 eyes of six patients: four men and two women. All patients had multiple CG on both eyes. No patient had an ocular history or symptoms other than refractive error. Their mean age and preoperative spherical equivalent (SE) of patients were 33.17 ± 4.45 and −4.28 ± 1.47 diopters (D), respectively. At 12 months after SMILE, the mean postoperative SE was −0.10 ± 0.32 D; all eyes were within ± 0.5 D. And all eyes had a UDVA of 0 logMAR or better, all eyes had a CDVA of −1.0 logMAR or better. No eye had lost two or more lines of CDVA from preoperative level (Table 1).
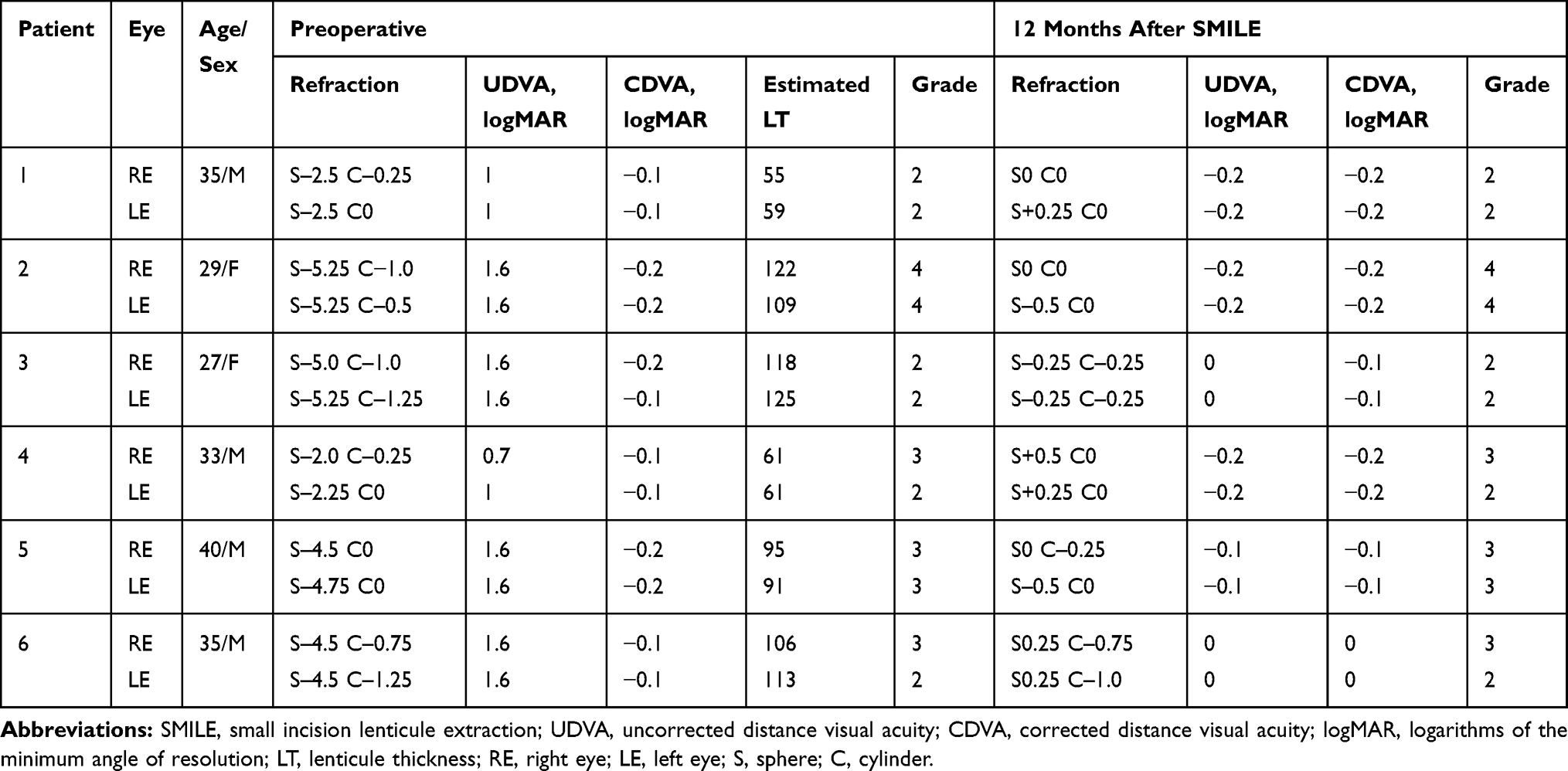 |
Table 1 Patient Demographics and Postoperative Results |
The efficacy (postoperative UDVA/preoperative CDVA) and safety (postoperative CDVA/preoperative CDVA) indexes were 0.98 ± 0.22 and 0.97 ± 0.21, respectively, at 12 months after SMILE procedure.
Preoperatively, CG were discovered using specular microscopy. Six eyes were grade 2, four eyes were grade 3, and two eyes were grade 4. The mean ECD was 2816.4 ± 121.6 cells/mm2, and the mean CCT was 563.9 ± 21.97 µm. The mean CV and HEX were 30.5 ± 5.44 and 48.75 ± 8.86%, respectively. Twelve months postoperatively, CG was not increased in number using specular microscopy, and there was no significant change in ECD, CV, and HEX using Mann–Whitney U-test (Table 2). The mean CCT was significantly decreased after SMILE procedure (p<0.001), and there was no significant difference between CCT change (88.92 ± 34.29 µm) and estimated lenticule thickness (92.92 ± 26.92 µm) (p=0.887). There was no case of CG grade change or corneal edema.
 |
Table 2 Changes in Corneal Endothelial Parameters and CCT After SMILE |
There were no complications such as, keratitis, epithelial ingrowth, corneal decompensation or ectasia during the follow-up period. Figure 1 shows the case of patient no. five, and other cases were similar.
 |
Figure 1 Continued. |
 |
Figure 1 The preoperative and postoperative dual rotating Scheimpflug (DRS) image and specular microscopic findings of right eye of patient no. five. (A) Multiple CG are observed in the corneal endothelium on preoperative specular microscopy exam. (B) Preoperative DRS image showed no distinct abnormality except mild elevation at the temporal cornea in the posterior elevation map. (C) Postoperative specular microscopy exam showed multiple CG, however there was no increase in numbers compared to the preoperative findings. (D) Postoperative DRS image. There was no interval change except thinning and flattening of the central cornea compared to preoperative findings. |
Discussion
LASIK can safely treat a healthy endothelium;12,13 however, some studies have reported LASIK-induced damage in patients with CG or FECD. Vroman et al3 and Dastjerdi and Sugar4 reported cases of endothelial decompensation after LASIK in patients with FECD, and one of these cases eventually required penetrating keratoplasty. Moshifar et al5 reported one year results of LASIK in seven eyes with CG and a family history of endothelial dystrophy, and found that six eyes had a statistically significant decrease in the ECD (12.4 ± 2.7%). However, eyes with FECD treated with Descemet stripping endothelial keratoplasty were able to tolerate LASIK.14
Although several mechanisms of endothelial damage after LASIK in CG or FECD patients have been hypothesized, including stress waves from excimer laser, IOP changes, and corneal stromal hydration, the exact mechanism is unknown. Because IOP change and stromal hydration take place in SMILE also, the biggest difference between LASIK and SMILE is type of laser. Excimer laser ablates the corneal surface to make changes in the corneal curvature with a 193 nm wavelength. In principle, when this wavelength is applied to the superficial cornea this does not cause damage to the endothelium, and 193 nm excimer laser incision to 90% of corneal depth did not cause endothelial cell loss on rabbit experiments.15 There are many reports that superficial corneal ablation using excimer laser did not cause endothelial impairment when the endothelium is healthy.12,13 However, there are some studies of endothelial cell health after LASIK that have other conclusions. Kim et al16 evaluated the effects of LASIK on the corneal endothelium 15 min, one day, and one month after surgery. Corneal endothelium showed transient edema within 15 min after surgery; however these changes were not present at one-day evaluation. Edelhauser17 reported changes in endothelial cell shape and function with excimer laser corneal stroma ablation within 200 µm of corneal endothelium on rabbit experiments. We can speculate endothelial cell changes occur after excimer laser ablation subclinically and resolve quickly if the endothelium is healthy, however if endothelium is compromised preoperatively, the endothelium can be permanently damaged with excimer laser.
SMILE corrects myopia using only a femtosecond laser to make an intrastromal lenticule, then the lenticule is extracted through a small incision.7 Femtosecond laser uses ultra-short pulses of focused near-infrared light (1053 nm) to create microcavitations that separate the cornea tissue without thermal or shockwave to surrounding tissue.18,19 There are some reports that SMILE has no adverse effects on the corneal endothelium.20,21 Kamiya et al22 reported there was no significant difference in ECD after femtosecond laser-assisted keratoplasty (FLAK) and after conventional penetrating keratoplasty, even though energy was higher (300 nJ in FLAK vs 140 nJ in our study), spot distance was narrower (3.0 µm in FLAK vs 4.0 µm in our study), and depth of laser was deeper (vertically full thickness in FLAK vs minimal residual stromal bed 310 µm in our study). Park et al23 reported a positive outcome after SMILE in a patient with posterior polymorphic corneal dystrophy, which has been described as a contraindication of LASIK24 because of the risk of corneal decompensation.
In our study, we used SMILE to correct myopia or myopic astigmatism in patients with CG. Twelve months after the procedure, all patients had excellent visual acuity, and no eyes developed corneal edema or other complications. When comparing the preoperative and postoperative ECD, CV, and HEX, no significant endothelial change was found. To the best of our knowledge, this is the first study of SMILE in patients with CG. The results suggest that SMILE can be successfully performed in patients with CG with no adverse effects postoperatively at 12 months. However, because the exact mechanism of corneal endothelial damage in patients with FECD after LASIK is unknown, we cannot definitively conclude that SMILE is safe for patients with CG. Studies of SMILE that include more patients with FECD or CG are needed, and further comparisons of the effects on the corneal endothelium between SMILE and LASIK should be performed.
Conclusion
SMILE yielded improvement in visual acuity and no adverse effects to corneal endothelial cells were found when correcting myopia or myopic astigmatism in patients with CG. Surgeons should therefore carefully evaluate the eyes of patients, including the preoperative corneal endothelium, and choose the proper procedure, based on all of the findings. However, an important limitation of this study is the smaller number of eyes evaluated and a short follow-up period. Hence, further studies with larger sample size and longer periods of follow-up are needed to substantiate these findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zoega GM, Fujisawa A, Sasaki H, et al. Prevalence and risk factors for cornea guttata in the Reykjavik Eye Study. Ophthalmology. 2006;113(4):565–569. doi:10.1016/j.ophtha.2005.12.014
2. Eghrari AO, Riazuddin SA, Gottsch JD. Fuchs corneal dystrophy. Prog Mol Biol Transl Sci. 2015;134:79–97. doi:10.1016/bs.pmbts.2015.04.005
3. Vroman DT, Solomon KD, Holzer MP, et al. Endothelial decompensation after laser in situ keratomileusis. J Cataract Refract Surg. 2002;28(11):2045–2049. doi:10.1016/S0886-3350(01)01352-9
4. Dastjerdi MH, Sugar A. Corneal decompensation after laser in situ keratomileusis in Fuchs’ endothelial dystrophy. Cornea. 2003;22(4):379–381. doi:10.1097/00003226-200305000-00020
5. Moshirfar M, Feiz V, Feilmeier MR, et al. Laser in situ keratomileusis in patients with corneal guttata and family history of Fuchs’ endothelial dystrophy. J Cataract Refract Surg. 2005;31(12):2281–2286. doi:10.1016/j.jcrs.2004.05.061
6. Malaise-Stals J, Collignon-Brach J, Weekers JF. Corneal endothelial cell density in acute angle-closure glaucoma. Ophthalmologica. 1984;189(3):104–109. doi:10.1159/000309393
7. McCartney MD, Wood TO, McLaughlin BJ. Moderate Fuchs’ endothelial dystrophy ATPase pump site density. Invest Ophthalmol Vis Sci. 1989;30:1560–1564.
8. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95(3):335–359. doi:10.1136/bjo.2009.174284
9. Kim BK, Mun SJ, Lee DG, et al. Chung’s swing technique: a new technique for small-incision lenticule extraction. BMC Ophthalmol. 2016;16(1):154. doi:10.1186/s12886-016-0321-2
10. Munoz G, Albarran-Diego C, Sakla HF, et al. Effects of LASIK on corneal endothelium using the 15-kHz IntraLase femtosecond laser. J Refract Surg. 2011;27(9):672–677. doi:10.3928/1081597X-20110415-02
11. Nawa Y, Ueda T, Masuda K, et al. Evaluation of the corneal endothelium after hyperopic laser in situ keratomileusis. J Cataract Refract Surg. 2003;29(8):1543–1545. doi:10.1016/S0886-3350(03)00460-7
12. Simaroj P, Kosalprapai K, Chuckpaiwong V. Effect of laser in situ keratomileusis on the corneal endothelium. J Refract Surg. 2003;19(2 suppl):S237–240.
13. Klingler KN, McLaren JW, Bourne WM, et al. Corneal endothelial cell changes 5 years after laser in situ keratomileusis: femtosecond laser versus mechanical microkeratome. J Cataract Refract Surg. 2012;38(12):2125–2130. doi:10.1016/j.jcrs.2012.07.034
14. Ratanasit A, Gorovoy MS. Laser-assisted in situ keratomileusis or photorefractive keratectomy after descemet stripping automated endothelial keratoplasty. Cornea. 2011;30(7):787–789. doi:10.1097/ICO.0b013e31820686e3
15. Dehm EJ, Puliafito CA, Adler CM, et al. Corneal endothelial injury in rabbits following excimer laser ablation at 193 and 248 nm. Arch Ophthalmol. 1986;104(9):1364–1368. doi:10.1001/archopht.1986.01050210118037
16. Kim T, Sorenson AL, Krishnasamy S, et al. Acute corneal endothelial changes after laser in situ keratomileusis. Cornea. 2001;20(6):597–602. doi:10.1097/00003226-200108000-00008
17. Edelhauser HF. The resiliency of the corneal endothelium to refractive and intraocular surgery. Cornea. 2000;19(3):263–273. doi:10.1097/00003226-200005000-00002
18. Chen Y, Hu DN, Xia Y, et al. Comparison of femtosecond laser-assisted deep anterior lamellar keratoplasty and penetrating keratoplasty for keratoconus. BMC Ophthalmol. 2015;15(1):144. doi:10.1186/s12886-015-0140-x
19. Netto MV, Mohan RR, Medeiros FW, et al. Femtosecond laser and microkeratome corneal flaps: comparison of stromal wound healing and inflammation. J Refract Surg. 2007;23(7):667–676. doi:10.3928/1081-597X-20070901-05
20. Zhang H, Wang Y, Xie S, et al. Short-term and long-term effects of small incision lenticule extraction (SMILE) on corneal endothelial cells. Cont Lens Anterior Eye. 2015;38(5):334–338. doi:10.1016/j.clae.2015.03.011
21. Wang DY, Liu ML, Chen YL, et al. Short term effects of small incision lenticule extraction surgery on corneal endothelium. Int J Ophthalmol. 2016;9(4):536–539. doi:10.18240/ijo.2016.04.09
22. Kamiya K, Kobashi H, Shimizu K, et al. Clinical outcomes of penetrating keratoplasty performed with the VisuMax femtosecond laser system and comparison with conventional penetrating keratoplasty. PLoS One. 2014;9(8):e105464. doi:10.1371/journal.pone.0105464
23. Park JH, Lee JH, Koo HJ. Small-incision lenticule extraction in posterior polymorphic corneal dystrophy. J Cataract Refract Surg. 2016;42(5):795–797. doi:10.1016/j.jcrs.2016.04.001
24. Huerva V, Mateo AJ. Posterior polymorphous dystrophy and LASIK. Arch Soc Esp Oftalmol. 2008;83:607–614. doi:10.4321/S0365-66912008001000008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.