Back to Journals » Open Access Emergency Medicine » Volume 18
Small Bowel Adenocarcinoma Presenting as a Chronic Pelvic Mass Mimicking Gynecologic Malignancy: A Case Report and Focused Narrative Review
Authors Sbitan L ![]() , Qandeel H
, Qandeel H ![]() , Imhaisen M, Hasan HA
, Imhaisen M, Hasan HA ![]() , Abohijleh Y
, Abohijleh Y ![]() , Nabhan AI
, Nabhan AI ![]() , Bani-Hani K
, Bani-Hani K
Received 15 February 2026
Accepted for publication 19 June 2026
Published 22 June 2026 Volume 2026:18 603817
DOI https://doi.org/10.2147/OAEM.S603817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Lana Sbitan,1,2,* Haitham Qandeel,1,2,* Mustafa Imhaisen,1 Hamzah A Hasan,3,4 Yazan Abohijleh,5 Ayman Issa Nabhan,6 Kamal Bani-Hani1,2
1Department of General Surgery, Prince Hamza Hospital, Jordanian Ministry of Health, Amman, Jordan; 2Department of General Surgery, Urology and Anesthesia, Faculty of Medicine, The Hashemite University, Zarqa, Jordan; 3Department of Internal Medicine, Prince Hamza Hospital, Amman, Jordan; 4Department of Internal Medicine, Faculty of Medicine, The Hashemite University, Zarqa, Jordan; 5Department of Radiology, Prince Hamza Hospital, Amman, Jordan; 6Department of Orthopedic Surgery, Tartus National Hospital, Tartus, Syria
*These authors contributed equally to this work
Correspondence: Ayman Issa Nabhan, Department of Orthopedic Surgery, Tartus National Hospital, Tartus, Syria, Tel +963-937731820, Email [email protected]
Background: Small bowel adenocarcinoma (SBA) is considered an unusual malignancy with vague presentations thus risk of delayed diagnosis. Despite being rarely reported in the literature, SBA can present with gynecological manifestations, especially adnexal mass, misleading surgeons in dealing with it as a primary gynecological malignancy.
Methods: We report a case of a 60 year old female patient who had SBA with pelvic mass as initial presentation. Identification of intestinal origin was done intraoperatively. Surgical resection of tumor and adnexal involvement with referral for oncological chemotherapy was done. Through this case we highlight the challenges experienced by surgeons in diagnosing SBA with gynecological disease, as well the clinical implications of atypical SBA presentations. Reported following CARE guidelines. In addition to the case reported, a focused narrative review of literature was performed. Searching Pubmed database from inception to December 2025 using related keywords, identification of case reports reporting SBA presentation with gynecological disease was done. Data related to patient demographics, clinical manifestations, diagnostic, treatment strategies, and oncological outcomes, were extracted and pattern identification was conducted. A diagnostic algorithm was developed and presented to improve diagnostic delay in approaching adnexal masses with “Red Flags” suspicious of SBA.
Results: Fourteen cases describing small bowel adenocarcinoma (SBA) presenting with gynecologic manifestations were identified – published between the years (1995– 2024). Approximately the age range of patients was between 12 and 65 years with most patients presenting in the fifth and sixth decades. The jejunum was the most common primary tumor site (10/14 cases, 71%), followed by the ileum (4/14 cases, 29%). The most common initial presentation reported across the studies was ovarian/adnexal mass. Diagnostic delay was common, ranging from several weeks to over 12 months, with SBA rarely suspected preoperatively. Recurrent red flags included iron-deficiency anemia, chronic gastrointestinal symptoms, unintentional weight loss, obstructive symptoms, disproportionate ovarian tumor size, and discordance between clinical presentation and gynecologic findings. Ovarian metastases were present in all reported cases (14/14 cases, 100%), while peritoneal, mesenteric, nodal, hepatic, and uterine involvement occurred less frequently. The definitive diagnosis was established following surgical exploration through histopathological and immunohistochemistry evaluation. Surgical management was dependent on timely diagnosis, with both bowel and gynecological resections required, followed by postoperative chemotherapy. Outcomes were also dependent on disease stage at the time of diagnosis.
Conclusion: Atypical adnexal masses in association with gastrointestinal or systemic red flags should raise the possibility of SBA. We propose a clinical diagnostic framework to help general surgeons and gynecologists with early identification of SBA presenting as pelvic mass, thus providing appropriate management of this rare clinical entity.
Keywords: small bowel adenocarcinoma, ovarian metastasis, pelvic mass, diagnostic delay, gynecologic malignancy mimic, ileum, jejunum
Introduction
In the literature, small bowel adenocarcinoma (SBA) is described as an unusual malignancy with an approximate incidence of 1–3% of all carcinoma affecting the gastrointestinal (GI) tract.1 When analysing the most common SBA sites of origin, duodenum is mostly affected (approximately 55–82%), jejunum (about 11–25%), and lastly ileum (7–17%).2 Early diagnosis of SBA is considered a challenge that requires sharp clinical sense as most patients present with non-specific symptoms like anemia – which is mostly due to Iron deficiency – vague GI symptoms – nausea, vomiting, and abdominal pain – weight loss, or, in advanced cases, bowel obstruction.3 Differential diagnoses commonly include primary ovarian epithelial tumors, metastatic gastrointestinal malignancies, endometriosis-associated neoplasms, and other pelvic malignancies.3
SBA management is primarily surgical, via oncological resection of affected segments, unless metastasis was detected, in such cases patients may need radiotherapy or systemic chemotherapy.4,5 The commonest sites of SBA metastasis are regional/distant lymph nodes, liver and peritoneum, with rare cases reporting involvement of adnexal metastases.5
Staging of SBA, thus early diagnosis, plays a critical role in the prognosis and survival of patients.6 Metastatic disease limits management options and is often associated with poor outcomes, while early-stage tumors are mostly resectable with preferable prognosis.6
Pelvic mass presentation is challenging for gynecologists, due to significant overlap between GI and gynecological malignancies, as sometimes both share clinical, laboratory and radiological presentations, making differentiating between both challenging.7 SBA with adnexal metastases may solely present with pelvic symptoms, with imaging and tumor markers assessment mimicking primary gynecological disease, which was previously reported in the literature.8,9 Notwithstanding this overlap, there are currently no established clinical frameworks to guide early identification of SBA in patients presenting with suspected gynecologic malignancy, careful review of patients’ clinical history makes identifying triggers that prompt early gastroenterology and surgical consultations when dealing with chronic pelvic masses justifiable, although poorly described in the literature.
In our study, we report a case of chronic pelvic mass presentation followed over one year in gynecology before developing acute intestinal obstruction, masking the diagnosis of ileum invasive papillary adenocarcinoma with ovarian, fallopian tubes and uterine metastases. In addition to reporting this rare case, we highlight, through a focused literature review, the critical diagnostic hazard in the evaluation of chronic pelvic masses and the results of delayed multidisciplinary involvement. Therefore, this paper aims to review existing literature on the topic of SBA with gynecological metastases – with focus on presentation, diagnostic pathway, and multidisciplinary interventions – and propose a clinical algorithm to encourage early multidisciplinary involvement in similar cases.
Materials and Methods
Our case report was prepared and reported following the CARE guidelines.10 Clinical data was acquired from the patient’s medical records, operative findings, histopathological results, and follow-up documentation after written informed consent was obtained for publication.
Furthermore, a focused narrative review was performed to identify published cases of small bowel adenocarcinoma (SBA) presenting with gynecologic manifestations or mimicking primary gynecologic malignancy. PubMed database was searched from inception up to December 2025 using combinations of the following keywords: “small bowel adenocarcinoma”, “ovarian metastasis”, “pelvic mass”, “diagnostic delay”, “gynecologic malignancy mimic”, “ileum”, “jejunum”, “duodenum”, and “surgical oncology”. We included English-language case reports describing SBA with gynecologic or adnexal involvement. Data related to patient demographics, clinical manifestations, diagnostic, treatment strategies, and oncological outcomes, were extracted and pattern identification was conducted. Fourteen eligible cases were identified and included in the final qualitative analysis. A diagnostic algorithm was developed and presented to improve diagnostic delay in approaching adnexal masses with “Red Flags” suspicious of SBA.
Case Presentation
Patient Demographics and Background
A 60-year-old female patient with a medical history of type 2 diabetes mellitus controlled on Metformin. The patient had no surgical history, she had four children via vaginal deliveries, and was postmenopausal upon presentation. She had no significant family history of gastrointestinal or gynecological malignancies, nor hematological disorders.
Clinical History and Longitudinal Gynecologic Follow-up
Approximately one year before definitive diagnosis, the patient presented with severe symptomatic anemia (hemoglobin 5.2 g/dL) requiring transfusion of three units of packed red blood cells. At that time, no overt gastrointestinal bleeding, abdominal symptoms, or clear source of anemia was identified. She was referred for multidisciplinary outpatient evaluation.
Over the following months, the patient experienced persistent fatigue, palpitations, dizziness, unintentional weight loss, intermittent abnormal vaginal bleeding, and episodes of hematochezia. Subsequent gynecologic evaluation included endometrial sampling, which was nondiagnostic.
The patient was later readmitted with fever, recurrent anemia, and a newly identified pelvic mass. Initial investigations suggested a right tubo-ovarian abscess, and she underwent image-guided drainage with antibiotic therapy, resulting in temporary clinical improvement. Gastroenterological evaluation, including colonoscopy, failed to identify a definitive source for her symptoms.
Upon gynecology follow up pelvic magnetic resonance imaging (MRI) and a new endometrial biopsy were requested and scheduled for the patient. Pelvic MRI was done in July 2025, evidence of defined irregularly shaped mass in the right hemipelvis with measurements about (8.8 × 5.2×6) cm suggestive of enteric origin with invasion of uterine fundus was found. Referral to the general surgery clinic was done via gynecology clinic.
Acute Deterioration
Prior to her scheduled general surgery appointment, the patient was readmitted with acute clinical deterioration. The patient presented to the emergency department with fever, diffuse abdominal pain, vomiting, worsening anemia (her hb upon admission was 4.7 g/dL), new-onset hematochezia, and obstipation. This admission marked the shift from chronic pelvic presentation to acute abdominal process requiring multidisciplinary surgical intervention after resuscitation.
Physical Examination Findings
On examination, the patient was looking ill and appeared pale. On vital signs assessment, she was tachycardic (pulse = 135) and febrile (Temperature = 38.5) with hemodynamic compromise signs related to the severe anemia she was having. Documented abdominal examination revealed; marked abdominal distension with diffuse tenderness, reduced bowel sounds and signs of peritonism (guarding and rebound tenderness). On deep palpation, a palpable pelvic mass was noted in the right lower quadrant. In addition, fresh blood with an empty rectum was found on digital rectal examination. Such findings were suggestive of superimposed acute intraabdominal issue on the previous chronic pelvic mass detected.
Laboratory Investigations
The laboratory findings of the patient were inconsistent with isolated gynecological process, more suggestive of ongoing inflammatory and bleeding GI pathology. On complete blood count (CBC) testing, the patient had severe anemia (hemoglobin (Hb) 4.7 g/dL) with leukocytosis (white blood cell count (WBC) 22,000/µL). Marked elevation of C-reactive protein (400 mg/L). No significant abnormalities were found in liver and renal function tests, as well coagulation profile. For further assessment of primary gynecological tumor possibility, tumor markers were requested and were reported within limits (CA-125 at 20.5 U/mL, CA 19–9 at 53 U/mL, and carcinoembryonic antigen (CEA) at 6.8 ng/mL).
Radiologic Evaluation
Contrast-enhanced computed tomography of the chest, abdomen, and pelvis with oral and intravenous contrast demonstrated evidence of defined irregularly shaped mass in the right hemipelvis with measurements about (10.8 × 5.2×7) cm suggestive of enteric origin mostly from the distal part of small bowel, heterogenously enhancing lesion mostly representing neoplastic lesion with invasion of adjacent uterine fundus (Figure 1).
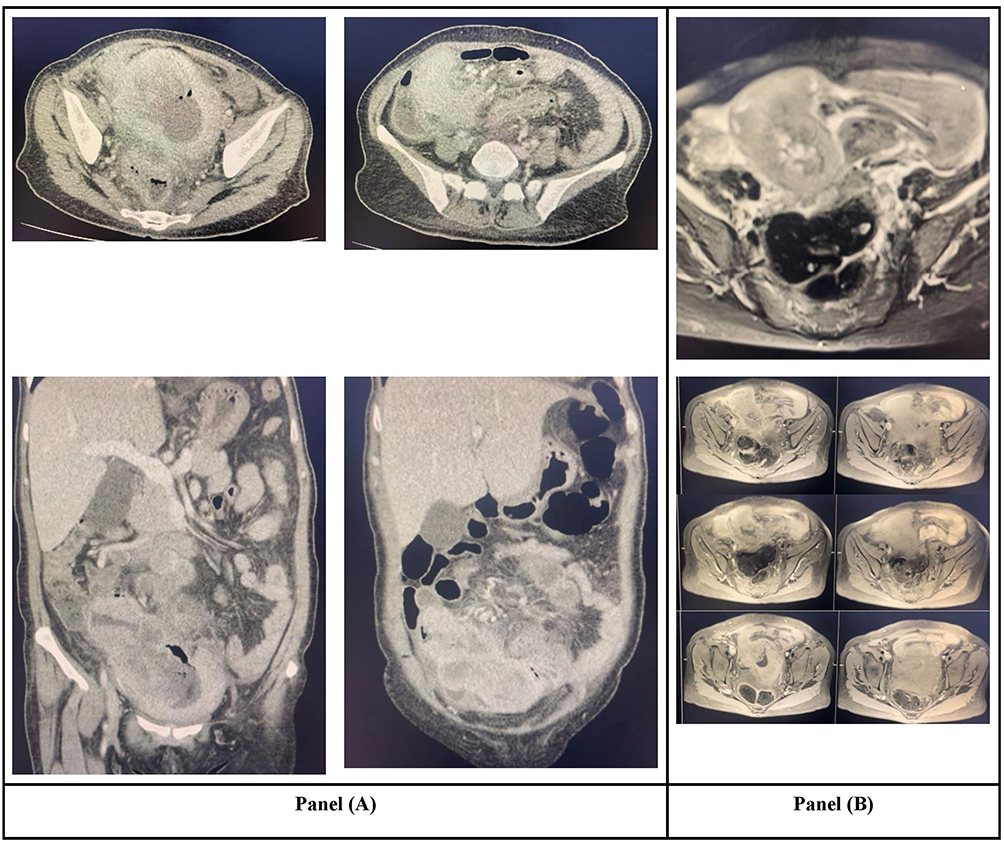 |
Figure 1 Preoperative Cross-Sectional Imaging of the Pelvic Mass. (A) Contrast-enhanced computed tomography (CT) of the abdomen and pelvis in the venous phase demonstrating a large, heterogeneous pelvic mass with mixed solid and cystic components on axial images, initially interpreted as a primary ovarian neoplasm. (B) T2-weighted fat-suppressed sequence showing a predominantly hyperintense multiloculated mass with solid components; T1-weighted fat-suppressed images obtained before and after contrast administration. |
In addition, right pelvic mesenteric lymph node enlargement was noted measuring about 1.2 cm in short axis diameter, dilated small bowel loops with air-fluid levels, collapsed distal bowel, and mild pelvic fluid, were found.
The combination of clinical deterioration, obstructive symptoms, laboratory and radiological findings prompted urgent exploratory surgical intervention.
Operative Findings and Surgical Procedure
After aggressive resuscitation, preoperative optimization and multidisciplinary (general surgery, gynecology and gastroenterology teams) discussion, a decision of exploratory laparotomy was taken.
Upon entering the abdominal cavity, the following findings were noted: extensive inflammatory adhesions involving the distal ileum, sigmoid colon, uterus, and adnexal structures. A large distal ileal mass located approximately 5 cm proximal to the ileocecal valve was identified, together with multiple enlarged mesenteric lymph nodes and localized abscess cavities.
The distal ileum was determined to be the primary site of malignancy with secondary involvement of regional lymph nodes and gynecologic structures. Segmental ileal resection with regional lymphadenectomy and primary ileo-ileal anastomosis was performed (Figure 2A). Given the extent of pelvic involvement, subtotal hysterectomy with bilateral salpingo-oophorectomy was subsequently undertaken by the gynecology team (Figure 2B).
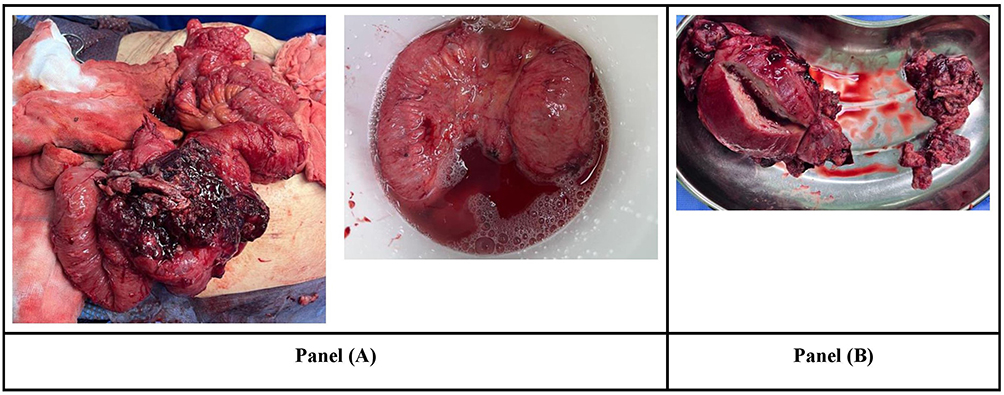 |
Figure 2 Intraoperative Gross Findings. (A) Intraoperative gross specimen of the small intestine demonstrating a firm, circumferential ileal mass causing luminal narrowing, consistent with the primary small bowel adenocarcinoma. (B) Gross surgical specimen following gynecologic resection, showing the adnexal and uterine tissues involved by metastatic disease, initially suspected to represent a primary gynecologic malignancy. |
Histopathological and Immunohistochemical Findings
A fungating mass measuring (6 × 6) cm was identified in the small bowel specimen, located 12 cm from the margin, with mesenteric fat extension, on gross examination. Regarding, proximal and distal resection margins, they were deemed grossly uninvolved.
Microscopic examination revealed invasive poorly differentiated high-grade papillary adenocarcinoma, with infiltration into the mucosa, submucosa, muscularis propria, and perienteric fat. In addition, extensive tumor necrosis, lymphovascular invasion, and high mitotic activity were documented. All surgical margins were also histologically free (Figure 3).
 |
Figure 3 Histopathologic Features of the Primary Small Bowel Adenocarcinoma. Low-power hematoxylin and eosin–stained section demonstrating; irregular, infiltrative glandular structures arranged in a complex, back-to-back and cribriform pattern, embedded within a desmoplastic stroma. The glands are angulated and crowded, lacking normal mucosal architecture, consistent with an invasive adenocarcinoma. There is loss of normal villous architecture, favoring a primary small bowel origin rather than a benign or borderline lesion. Areas of luminal necrotic debris and architectural complexity further support malignant glandular differentiation. |
Tumor deposits with similar histomorphological features were demonstrated in the adnexa and parametrium specimen, supporting the metastasis involvement. Uterus had significant atrophic endometrium, unremarkable myometrium, with no evidence of primary malignancy.
Furthermore, Immunohistochemical analysis demonstrated tumor cell positivity for CK7, focal nuclear expression of CDX2, and negativity for CK20 and WT1. The combined histopathological, immunophenotypic, and intraoperative findings confirmed the diagnosis of poorly differentiated small bowel adenocarcinoma with metastatic involvement of the ovaries and parametrium.
Postoperative Course and Follow-Up
Postoperative recovery was smooth with no documented surgical complications and slow return of bowel function. On day 5 post-operative, the patient was discharged in a stable condition. Following the results of histopathologic examination, the patient was referred to the medical oncology team, with the decision to start systemic chemotherapy. Three months postoperatively, on clinic follow-up visit, the patient still showed good recovery while still under ongoing oncologic treatment.
Refer to Figure 4, summarizing the timeline of patient presentation and highlighting the diagnostic delay.
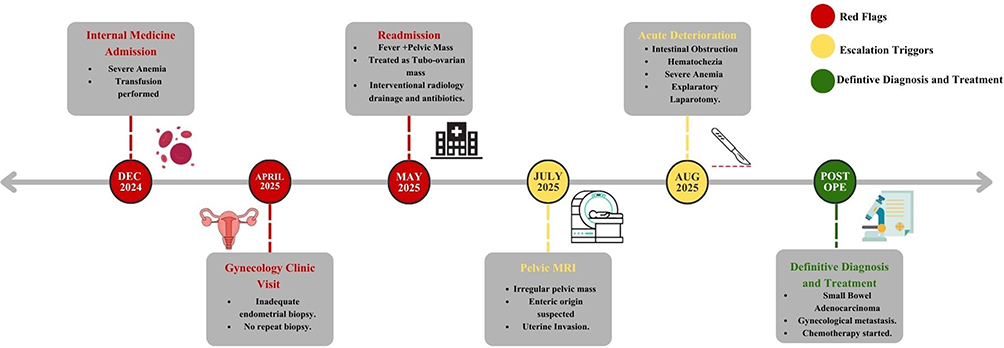 |
Figure 4 Timeline of Clinical Course Highlighting the Diagnostic Delay and the Need for Surgical Intervention. |
Discussion
Focused Narrative Review of SBA Presenting with Gynecologic Disease
Table 1 represents a summary of reported cases of SBA presenting with gynecologic metastasis identified through our extensive literature search. Furthermore, a detailed description of each reported case is provided in Supplementary Table 1.
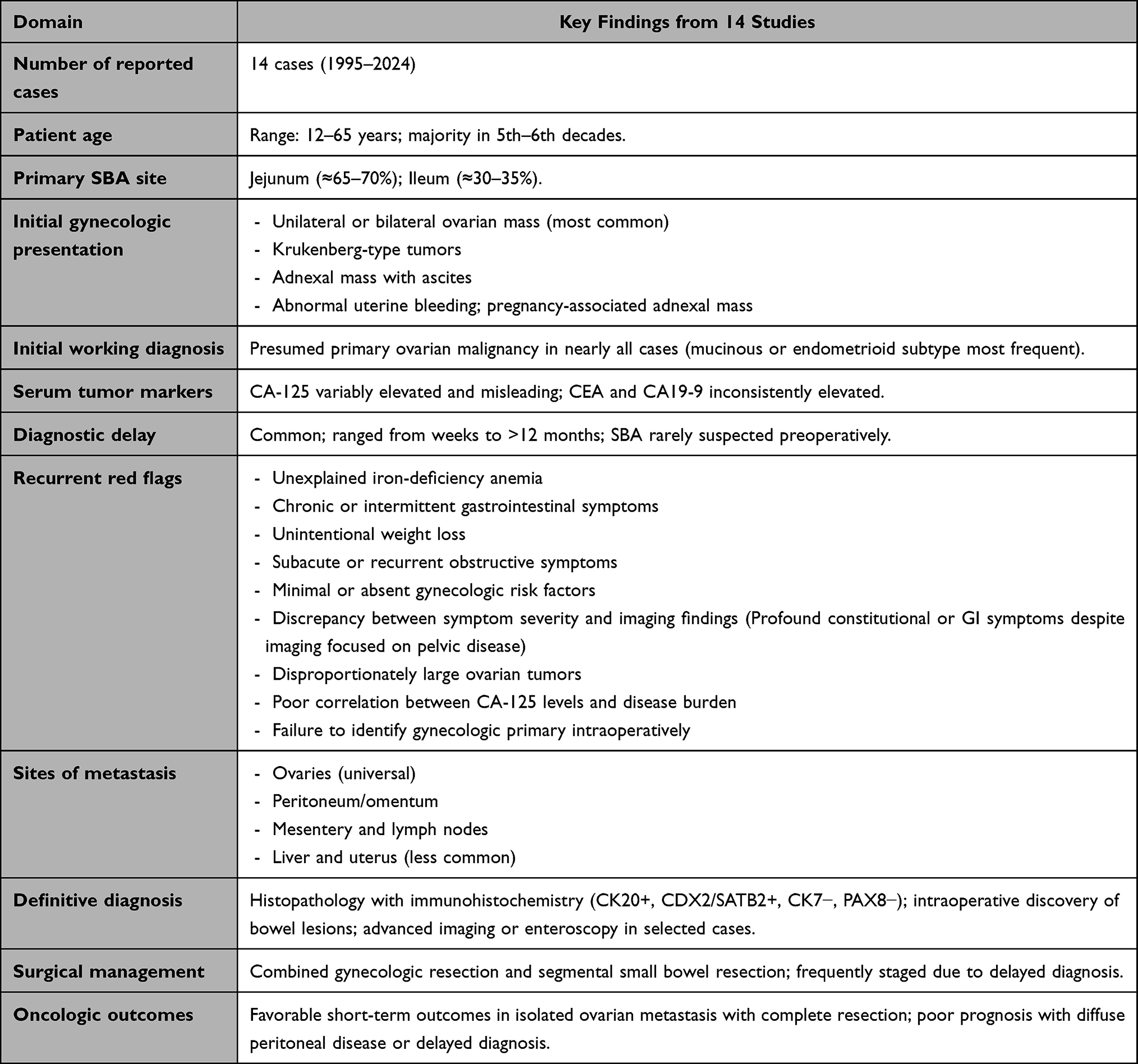 |
Table 1 Summary of Reported Cases of Small Bowel Adenocarcinoma Presenting with Gynecologic Metastasis |
Frequency and Patterns of Gynecologic Presentation
Only fourteen cases were found published between 1995 and 2024 describing SBA presenting with gynecological manifestations primarily.9–22 Approximately the age range of patients was between 12 and 65 years with most patients presenting in the fifth and sixth decades. The jejunum was the most common primary tumor site (10/14 cases, 71%), followed by the ileum (4/14 cases, 29%). Across the reported cases, pelvic ovarian masses were documented as the initial manifestation, imitating primary ovarian tumor presentation, which is similar to our case.9–12,15,17–19,21 In addition, other reported presentations included: adnexal masses,13,14,20 abnormal uterine bleeding, pelvic pain, and abdominal distension. In all reported cases, as in ours too, small bowel primary tumor was not suspected with the previous manifestations as first presentation of each case. Even though in all reported cases, vague GI symptoms were recognized months preceding the diagnosis.9–22 Thus, gynecological management was mainly observed in each case with delayed identification of intestinal origin of the condition.
Gynecological metastasis of primary SBA is described in the literature, although rare. Most patients are diagnosed at a late stage, even though a pattern of gynecological presentation associated with vague GI/constitutional symptoms can be identified across the cases reported in the literature.
Historical, Clinical, and Radiologic Red Flags
Multiple red flags can be identified across the reported cases, which should prompt suspicion of GI origin in patients presenting with gynecological manifestations, including both GI and constitutional associated presentations (Table 1).10,13,15,16,20 Starting with, unexplained weight loss, progressive iron deficiency anemia, fever, and generalized fatigue. In addition, vague GI symptoms like: altered bowel habits, recurrent nausea/vomiting, vague ill-localized and intermittent abdominal pain, as well as episodes of partial or subacute bowel obstruction. However, such symptoms could be transient and insignificant to the patient.
Radiologically, several reports described disproportionately large ovarian masses, associated mesenteric lymphadenopathy, bowel wall abnormalities, or imaging findings suggestive of an enteric origin. Furthermore, a mismatch between the severity of constitutional symptoms and the apparent burden of pelvic disease was frequently observed.
Notably, CA-125 levels were proven nonspecific and often misleading in cases of SBA presenting with gynecologic disease,10,13,15,20 while CEA or CA19-9 levels elevation if found were more in favour of intestinal origin of symptoms.10,19
Missing such clues contributes to the common diagnostic delay noticed among most cases and may mislead to consider such presentations as primary ovarian tumors.
Diagnostic Pathways and Timing of SBA Identification
Unfortunately, over the reported cases, a significant delay was noted in the diagnosis of SBA only after disease progression/metastasis or gynecological prolonged intervention.9–22 Which was also the main dilemma of our case. The primary approach with most patients focused on gynecological origin of symptoms, with delayed multi-disciplinary involvement, reported delays ranged from several weeks to more than 12 months. Final and definitive diagnosis of SBA was only through histopathology postoperatively and immunohistochemistry intestinal markers (CK20, CDX2, SATB2). Importantly, usual GI investigations, like conventional colonoscopy and upper endoscopy failed to diagnose or at least hint at SBA suspicion as reported in Maekawa et al and Takahashi et al papers, as well as experienced with our patient9,15 This recognized pattern prompted the integration of second-line investigations as device-assisted enteroscopy or colonofiberscopy,22 when previously mentioned red flags presented associated with gynecological manifestations, which may shorten the diagnostic delay and alert the surgical team to suspect small bowel origin.
These findings support a lower threshold for dedicated small bowel investigation when gastrointestinal red flags coexist with unexplained adnexal pathology.
Surgical Strategies and Oncologic Outcomes
The chosen surgical management option for SBA with gynecological disease was variable across reported studies and dependent on timing of diagnosis and disease progression. Most cases with early identified SBA were managed with segmental small bowel resection and gynecologic metastasectomy, followed by chemotherapy according to the metastasis level. Which offered the best prognosis among the cases.10,11,14,15,17–21 In addition, variable regimens of post-operative chemotherapy, reported regimens included 5-fluorouracil–based combinations,12,15 CAPOX,20 FOLFOX,9 FOLFIRI, capecitabine monotherapy, and biologic agents such as bevacizumab,22 were administered with no clear benefits noticed for a specific regimen.
Molecular characterization was infrequently reported; however, notable findings included mismatch repair deficiency associated with Lynch syndrome in one patient and molecular confirmation of metastatic origin through shared BRAF mutation profiling in another.8,20 These observations highlight the emerging importance of molecular testing in confirming tumor origin, identifying hereditary cancer syndromes, and potentially guiding systemic treatment decisions.
Notably, the two patients with isolated ovarian metastases reported by Maekawa et al and Iwata et al remained disease-free at 24-month follow-up after complete surgical resection and adjuvant systemic therapy, whereas patients with diffuse peritoneal dissemination generally experienced disease progression or disease-related mortality.16,20
Overall, the outcomes of reported cases encourage early suspicion, thus diagnosis of SBA for better management and improved prognosis.
Clinical Implications and Proposed Diagnostic Algorithm
Clinical Implications for Gynecologic and General Surgeons
Our case report and focused review present multiple implications to improve practice when dealing with small bowel tumors with gynecological disease for both general surgeons and gynecologists. Primarily, the presence of gastrointestinal symptoms, anemia, or constitutional symptoms in association with large, unilateral, or bilateral pelvic masses should encourage the involvement of multidisciplinary teams and a GI primary should be taken into consideration. Furthermore, when evaluating a pelvic mass, reliance on imaging or CA-125 tumor markers alone is inadequate, other marker elevations like CEA or CA19-9 should raise the possibility for SBA, especially when correlated with clinical presentation and vague GI complaints. For surgeons intraoperatively, encountering ovarian masses with atypical features, or absence of peritoneal involvement should prompt full inspection and palpation of small bowel. Moreover, emphasizing early multidisciplinary involvement, including gastroenterology and oncology teams, ensures a systematic approach and the use of advanced investigations as enteroscopy, and targeted immunohistochemistry, which improves the chances of achieving a single-stage oncological resection, correct diagnosis and better prognosis.
All in all, recognizing the red flags we have mentioned in a patient presenting with gynecological manifestations starts with a thorough history taking and examination, thus preventing unnecessary radical gynecologic surgery, shortening diagnostic delay, and enhancing oncological results.
Proposed Diagnostic Algorithm for Gynecological Manifestations with Red Flags
Based on our experience, extensive literature review and study of reported cases, we propose a stepwise diagnostic framework for patients presenting with adnexal pelvic masses with a suspicion of SBA masquerading as primary gynecologic tumor. First assessment depends on performing a thorough history taking and examination, extending beyond pelvic findings, with a focus on historical red flags including: persistent intermittent gastrointestinal symptoms, unexplained weight loss, and iron deficiency anemia not responsive to treatment and with no identified cause. Then proceeding to identify suspicious red flags via laboratory evaluation, interpretation of CA-125 tumor marker should be done in association with other GI markers (as elevations of CEA or CA19-9 is suggestive of non-gynecological origin). In such cases, radiological assessment should also be taken into consideration especially if images are suggestive of bilateral ovarian involvement, relative absence of peritoneal involvement, or large mucinous tumors. If such red flags are present in the patient, then an early multidisciplinary approach with advanced GI evaluation should be considered (Figure 5). Furthermore, Intraoperative systematic evaluation of small bowel should be deemed essential.
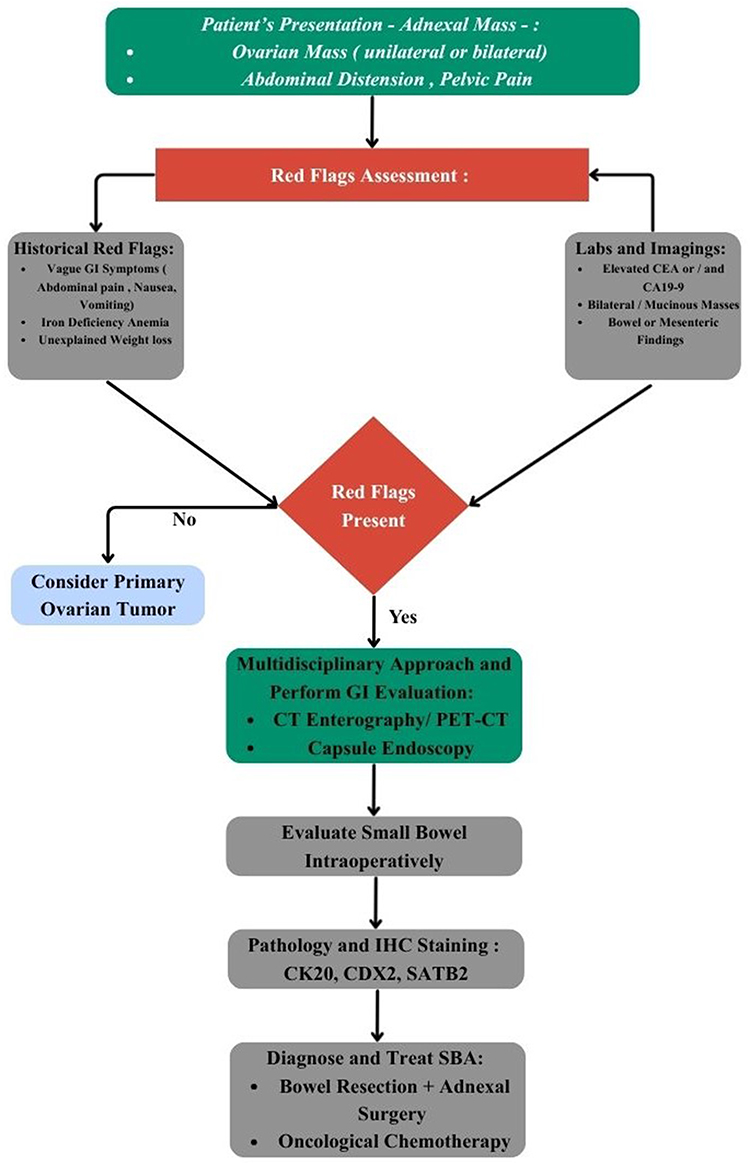 |
Figure 5 Diagnostic Algorithm For Adnexal Masses with “Red Flags” Suspicious of Small Bowel Adenocarcinoma. |
Future Research Directions
Future research should focus on designing multicenter registries for better understanding of incidence, outcomes patterns and diagnostic timelines of small bowel adenocarcinoma. Especially, developing translational research with a focus on molecular signatures differentiating between primary gynecological tumors from GI metastasis, which may contribute to improving preoperative risk stratification by employing precision medicine techniques for tailored surgical planning. Additionally, future studies should prospectively evaluate and validate our proposed diagnostic algorithm to assess its effect on diagnostic delay, surgical decision, and outcomes.
Strengths and Limitations
A critical strength of our paper is the combination of a focused narrative review with an illustrative case from our clinical practice, performing a real contextualization of recurrent and unfortunate clinical patterns and diagnostic pitfalls identified across similar reported cases in the literature. On the other hand, limitations include reliance on retrospective data acquired from rare case reports with heterogeneous reporting. In addition, the study is inherently limited by the single-case nature of the primary report, restricting the generalizability of individual clinical observations. The rarity of SBA presenting with gynecologic disease resulted in a limited sample size of only fourteen reported cases over nearly three decades, precluded meaningful statistical analysis or direct comparison of diagnostic and therapeutic strategies. Furthermore, important clinicopathological variables, molecular characteristics, treatment details, and long-term oncologic outcomes were inconsistently reported across studies, limiting more robust comparative analysis. Nevertheless, the merging of findings and identification of patterns across independent cases, integrated with our case, enforces the clinical relevance of the presented diagnostic framework and encourages further work on the topic.
Conclusion
Small bowel adenocarcinoma, especially when associated with gynecological disease, can mimic gynecological primary malignancy, leading to delayed identification and late-stage disease. Our case, together with the fourteen cases identified in the literature, demonstrates a recurring pattern in which SBA initially mimics primary gynecologic disease, frequently resulting in delayed diagnosis and advanced-stage presentation. Early recognition of red flags and application of our proposed algorithm may shorten diagnostic delay, enable multidisciplinary, timely management, and prevent unnecessary radical gynecological surgery.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval
Institutional approval was essential for the preparation and publication of this case. Ethical approval was acquired and our study was approved by the Institutional Review Board of Prince Hamza Hospital, Ministry of Health, Jordan.
Patient Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
The authors declare no funding received for this work.
Disclosure
The authors declare no conflict of interest while working on this paper.
References
1. Bouali M, Sylvestre K, Benghait H, et al. Small bowel adenocarcinoma a rare cause of upper gastrointestinal obstruction (a case report and literature review). Int J Surg Case Rep. 2022;91:106763. doi:10.1016/j.ijscr.2022.106763
2. Aparicio T, Zaanan A, Svrcek M, et al. Small bowel adenocarcinoma: epidemiology, risk factors, diagnosis and treatment. Dig Liver Dis. 2014;46(2):97–12. doi:10.1016/j.dld.2013.04.013
3. Khosla D, Dey T, Madan R, et al. Small bowel adenocarcinoma: an overview. World J Gastrointest Oncol. 2022;14(2):413–422. PubMed PMID: 35317322; PubMed Central PMCID: PMC8918997. doi:10.4251/wjgo.v14.i2.413
4. Gelsomino F, Balsano R, De Lorenzo S, Garajová I. Small bowel adenocarcinoma: from molecular insights to clinical management. Curr Oncol. 2022;29(2):1223–1236. PubMed PMID: 35200603; PubMed Central PMCID: PMC8870676. doi:10.3390/curroncol29020104
5. Neugut AI, Marvin MR, Chabot JA. Adenocarcinoma of the small bowel. In: Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt; 2001.
6. Gu Y, Deng H, Wang D, Li Y. Metastasis pattern and survival analysis in primary small bowel adenocarcinoma: a SEER-Based Study. Front Surg. 2021;8:759162. PubMed PMID: 34950695; PubMed Central PMCID: PMC8691381. doi:10.3389/fsurg.2021.759162
7. Tonni G, Palicelli A, Bassi MC, et al. Gastrointestinal Stromal Tumors (GISTs) mimicking primary ovarian tumors or metastasizing to the ovaries: a systematic literature review. Cancers. 2024;16(13):2305. PubMed PMID: 39001368; PubMed Central PMCID: PMC11240519. doi:10.3390/cancers16132305
8. Zhu L, Liu Y, Chen S, Yang G, Wang C. Extremely rare mucinous adenocarcinoma of the small bowel causing bilateral metastatic Kukenberg tumors of the ovaries: a case report. Medicine. 2024;103(44):e40397. doi:10.1097/MD.0000000000040397
9. Takahashi Y, Iijima T, Ishidera Y, et al. Primary small bowel adenocarcinoma with metastatic ovarian tumor in a pregnant woman. Case Rep Oncol. 2024;17(1):882–890. PubMed PMID: 39144241; PubMed Central PMCID: PMC11324275. doi:10.1159/000540524
10. CARE Case Report Guidelines [Internet]. CARE Case Report Guidelines. [cited February 2, 2025]. Available from: https://www.care-statement.org.
11. Tsuruchi N, Kubota H, Tsukamoto N, Kurano A. Primary jejunal adenocarcinoma masquerading as a primary ovarian malignancy. Gynecol Oncol. 1995;58(1):129–132. PubMed PMID: 7789880. doi:10.1006/gyno.1995.1196
12. Dunsmore KP, Lovell MA. Small bowel adenocarcinoma metastatic to the ovaries in a 12-year-old girl. J Pediatr Hematol Oncol. 1998;20(5):498–501. PubMed PMID: 9787329. doi:10.1097/00043426-199809000-00019
13. Kilic G, Abadi M. Jejunal adenocarcinoma presenting as a primary ovarian carcinoma. Gynecol Oncol. 2000;78(2):255–258. PubMed PMID: 10926813. doi:10.1006/gyno.2000.5872
14. Andresen DM, Pedersen FH, Rasmussen KL. Adenocarcinoma of the small intestine mistaken as a primary ovarian cancer. Arch Gynecol Obstet. 2001;265(4):214–215. PubMed PMID: 11789749. doi:10.1007/s004040000155
15. Husain S, Thompson D, Thomas L, Donaldson B, Sabbagh R. Adnexal mass: an unusual presentation of small-bowel adenocarcinoma. J Natl Med Assoc. 2006;98(5):799–802. PubMed PMID: 16749659; PubMed Central PMCID: PMC2569296.
16. Maekawa H, Sato K, Komatsu Y, Orita H, Sakurada M. Jejunal cancer detected after a resection of bilateral ovarian metastasis: report of a case. Surg Today. 2010;40(11):1084–1087. PubMed PMID: 21046510. doi:10.1007/s00595-009-4174-7
17. Huang YY, Pratt JJ, Dabner M, Tjhin W. Challenging diagnosis of a jejunal adenocarcinoma with ovarian metastasis: report of an unusual case. BMJ Case Rep. 2013;2013:bcr2013008842. PubMed PMID: 23580681; PubMed Central PMCID: PMC3645799. doi:10.1136/bcr-2013-008842
18. Mitsushita J, Netsu S, Suzuki K, Nokubi M, Tanaka A. Metastatic ovarian tumors originating from a small bowel adenocarcinoma - a case report and brief literature review. Int J Gynecol Pathol. 2017;36(3):253–260. PubMed PMID: 27513076. doi:10.1097/PGP.0000000000000314
19. An-Chieh Liu A, Chen CH, Liu WM, Chang CW. A rare Krukenberg tumor arising from a primary adenocarcinoma of the small intestine. Taiwan J Obstet Gynecol. 2018;57(2):319–322. PubMed PMID: 29673681. doi:10.1016/j.tjog.2018.02.025
20. Iwata N, Shikama A, Takao W, et al. Ovarian metastases from ileum cancer in a patient with germline EPCAM gene deletion successfully treated with surgical resection and CAPOX chemotherapy: a case report. BMC Med Genet. 2020;21(1):76. PubMed PMID: 32272879; PubMed Central PMCID: PMC7144057. doi:10.1186/s12881-020-01013-1
21. Yang H, Yuan R, Alex D, et al. Metastatic small bowel adenocarcinoma mimicking a primary ovarian mucinous tumour - clinical, radiologic, pathologic and molecular correlation. Int J Surg Pathol. 2023;31(1):110–118. PubMed PMID: 35477328. doi:10.1177/10668969221098083
22. Nagao S, Matsuura M, Kurokawa S, Tamate M, Akimoto T, Saito T. A rare case of small intestinal cancer with uterine metastasis after surgery for ovarian metastasis, diagnosed using immunostaining. Case Rep Oncol Med. 2024;2024:8551816. PubMed PMID: 39156866; PubMed Central PMCID: PMC11330332. doi:10.1155/2024/8551816
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.