Back to Journals » OncoTargets and Therapy » Volume 9
Smad3 and phospho-Smad3 are potential markers of invasive nonfunctioning pituitary adenomas
Authors Liu C, Li Z, Wu D, Li C, Zhang Y ![]()
Received 2 November 2015
Accepted for publication 8 February 2016
Published 15 April 2016 Volume 2016:9 Pages 2265—2271
DOI https://doi.org/10.2147/OTT.S99699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Min Li
Chunhui Liu,1,2 Zhenye Li,1–3 Dan Wu,4 Chuzhong Li,1–3 Yazhuo Zhang1–3
1Beijing Neurosurgical Institute, Capital Medical University, 2Beijing Institute for Brain Disorders, Brain Tumor Center, 3Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, 4Department of Neurology, Beijing Renhe Hospital, Beijing, People’s Republic of China
Background: Transforming growth factor-β (TGF-β) signaling plays important roles in tumor development. Nevertheless, the roles of TGF-β/Smad signaling in nonfunctioning pituitary adenomas (NFPAs) have not been fully studied.
Methods: Tumor samples were obtained from patients who had NFPAs and underwent endoscopic transsphenoidal surgery or craniotomy at Beijing Tiantan Hospital from March 2008 to December 2012. Immunohistochemistry was performed to determine the expression of Smad transducer proteins in NFPAs. Ki-67 was evaluated as an indicator of the proliferative activity of NFPAs.
Results: A total of 161 patients with NFPAs were identified; 59 (36.6%) had invasive NFPAs and 102 (63.4%) had noninvasive NFPAs. Protein levels of Smad3 and phospho-Smad3 (p-Smad3) were significantly lower in patients with invasive NFPAs than in patients with noninvasive NFPAs (P<0.05 and P<0.01, respectively). The Ki-67 index was markedly greater in invasive NFPAs than in noninvasive NFPAs (P<0.05) and was significant correlated with p-Smad3 levels (P<0.05, r=-0.702).
Conclusion: A low level of Smad3 and p-Smad3 proteins was associated with the invasion of NFPAs.
Keywords: nonfunctioning pituitary adenoma, invasion, transforming growth factor-β, Smad, Ki-67
Introduction
Pituitary adenomas (PAs), with a prevalence of 80–90/100,000 people,1,2 comprise ~15% of intracranial tumors. Majority of PAs secrete pituitary hormones, resulting in elevated blood hormone levels and clinical syndromes. Nonfunctioning pituitary adenomas (NFPAs) constitute ~30% of PAs and do not cause clinical hormone hypersecretion.3 Most PAs are histologically benign. However, as hormonal inactivity leads to delayed diagnosis, a part of NFPAs becomes invasive.4 Invasive NFPAs often invade cavernous sinus; hence, curative radical surgery becomes difficult. In addition, there are no effective drugs for NFPAs and radiotherapy remains controversial. Therefore, NFPAs are a therapeutic challenge.
The effects of transforming growth factor-β (TGF-β) signaling are diverse in different tumor periods and tumor types.5–7 TGF-β ligands carry out biological effects by binding to TGF-β receptor complexes (TGF-β RI/II) and activating them. Smads are TGF-β signal transducer proteins. Activated TGF-β receptor complexes can phosphorylate Smad2 and Smad3, which associate with Smad4 to form a complex to get into the nucleus and regulate transcriptional activity. Smad7 is an inhibitory factor that restrains the phosphorylation of Smad2 and Smad3.7–9
It has been suggested that TGF-β/Smad signaling may be associated with the development and invasion of NFPAs in our previous work.10 However, the validity of this conclusion remains uncertain due to a small sample size and potential selection bias. Therefore, we built a PA database at Beijing Tiantan Hospital, which includes information on all patients with PAs. In this study, with the use of the database, we aimed to investigate whether TGF-β/Smad signaling is associated with the invasion of NFPAs and evaluate the proliferative activity (Ki-67) in NFPAs.
Materials and methods
Patients and specimens
From March 2008 to December 2012, patients with NFPAs who underwent endoscopic transsphenoidal surgery or craniotomy at Beijing Tiantan Hospital were included in this study. Patients with previous radiation therapy or recurrence were excluded. NFPA was diagnosed according to clinical feature, hormonal levels, magnetic resonance imaging, histopathological examination, and immunohistochemical staining for all anterior pituitary hormones. Invasive PAs were defined as Knosp classification grade IV.11 NFPA samples were obtained from patients, and immunohistochemistry was performed to evaluate protein levels. The study protocol was approved by the Ethics Committee of Beijing Tiantan Hospital, and written informed consent was obtained from all the patients.
Tissue microarray
Formalin-fixed, paraffin-embedded tissue blocks were sliced, and hematoxylin–eosin-stained slides were produced. Three core biopsies with a 2.0 mm diameter were selected from the paraffin-embedded tissues. The cores were transferred to tissue microarray (TMA) using the Minicore tissue-arraying instrument (Mitogen, Alphelys, France). Samples were randomly ordered and anonymized on the TMA slides. TMAs were cut into 4 μm sections using a serial microtome.
Immunohistochemistry
All the TMA slides were evaluated in advance using a hematoxylin–eosin staining to assess tumor content and quality. The TMAs were placed in a Leica BOND-III arrayer (Leica Microsystems, Wetzlar, Germany), which is a fully automated, random, and continuous access slide staining system that processes immunohistochemistry tests simultaneously. Bond™ Polymer Refine Detection (Leica Microsystems) was used for the detection of primary antibodies. Immunostainings were standardized using appropriate positive and negative controls for each antibody. All the TMAs were stained in the same run for each antibody to avoid interassay variability. The slides were digitally scanned, and protein expression was examined using Aperio AT2 (Leica Microsystems). The following antibodies were used: Ki-67 (1:100; Abcam, Cambridge, UK), Smad2 (1:100; Abcam), phospho-Smad2 (p-Smad2; Ser465/467) (1:100; Abcam), Smad3 (1:100; Abcam), p-Smad3 (Ser423/425) (1:100; Abcam), and Smad4 (1:100; Abcam).
The sections were examined and scored by two pathologists who were unaware of clinical records of patients. For Smad2, Smad3, and Smad4, the cytoplasmic staining pattern was considered to be the positive expression. For p-Smad2 and p-Smad3, the nuclear staining pattern was considered to be the positive expression. Five fields at 200× magnification were randomly selected. A semiquantitative system was used to evaluate the staining scores. The proportion of positive cells was scored as follows: 0 (<5%), 1 (6%–25%), 2 (26%–50%), 3 (51%–75%), and 4 (>75%). Staining intensity was evaluated as follows: 0 (no staining), 1 (weak staining, light yellow), 2 (moderate staining, yellowish brown), and 3 (strong staining, brown). Sum score was determined by multiplying the positive proportion score by intensity score: negative (0), weakly positive (1–4), moderately positive (5–8), and strongly positive (9–12). In this study, the expression was considered low expression when the score was less than nine, and high expression when the score was ≥9.12
Statistical analysis
SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Data were expressed as mean ± standard deviation. Differences between the groups were determined by one-way analysis of variance or independent two-sample Student’s t-test. Correlation analysis was assessed by Spearman’s rank correlation. P<0.05 was considered statistically significant.
Results
Patient characteristics
A total of 161 patients with NFPA who underwent endoscopic transsphenoidal surgery or craniotomy were included in this study. These patients had a medium age of 52 years; 98 (60.9%) were men and 63 (39.1%) were women. Of the 161 patients, 59 (36.6%) had invasive NFPAs and 102 (63.4%) had noninvasive NFPAs (Table 1). Visual deficit and hypopituitarism were more common in patients with invasive NFPAs than in patients with noninvasive NFPAs, and tumor size was larger in patients with invasive NFPAs than in patients with noninvasive NFPAs.
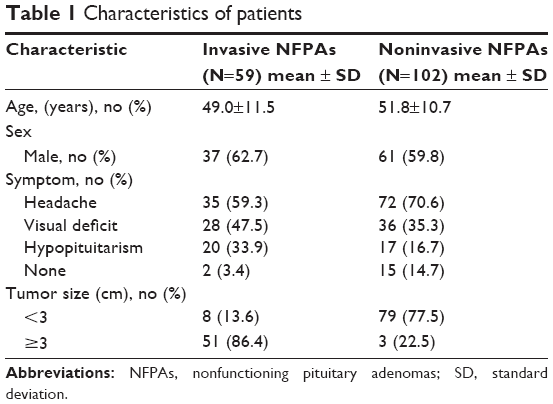 | Table 1 Characteristics of patients |
Expression of Smad2 and p-Smad2 in NFPAs
To determine the expression of Smad2 and p-Smad2 in invasive and noninvasive NFPAs, we evaluated the protein levels of Smad2 and p-Smad2 by immunohistochemistry. We found that there was no significant difference in the Smad2 or p-Smad2 protein levels between invasive and noninvasive NFPAs (Figure 1). Smad2 was highly expressed in 33.9% (20 of 59 cases) of invasive NFPAs and 29.4% (30 of 102 cases) of noninvasive NFPAs (P=0.553). p-Smad2 was highly expressed in 39.9% (23 of 59 cases) of invasive NFPAs and 33.3% (34 of 102 cases) of noninvasive NFPAs (P=0.470).
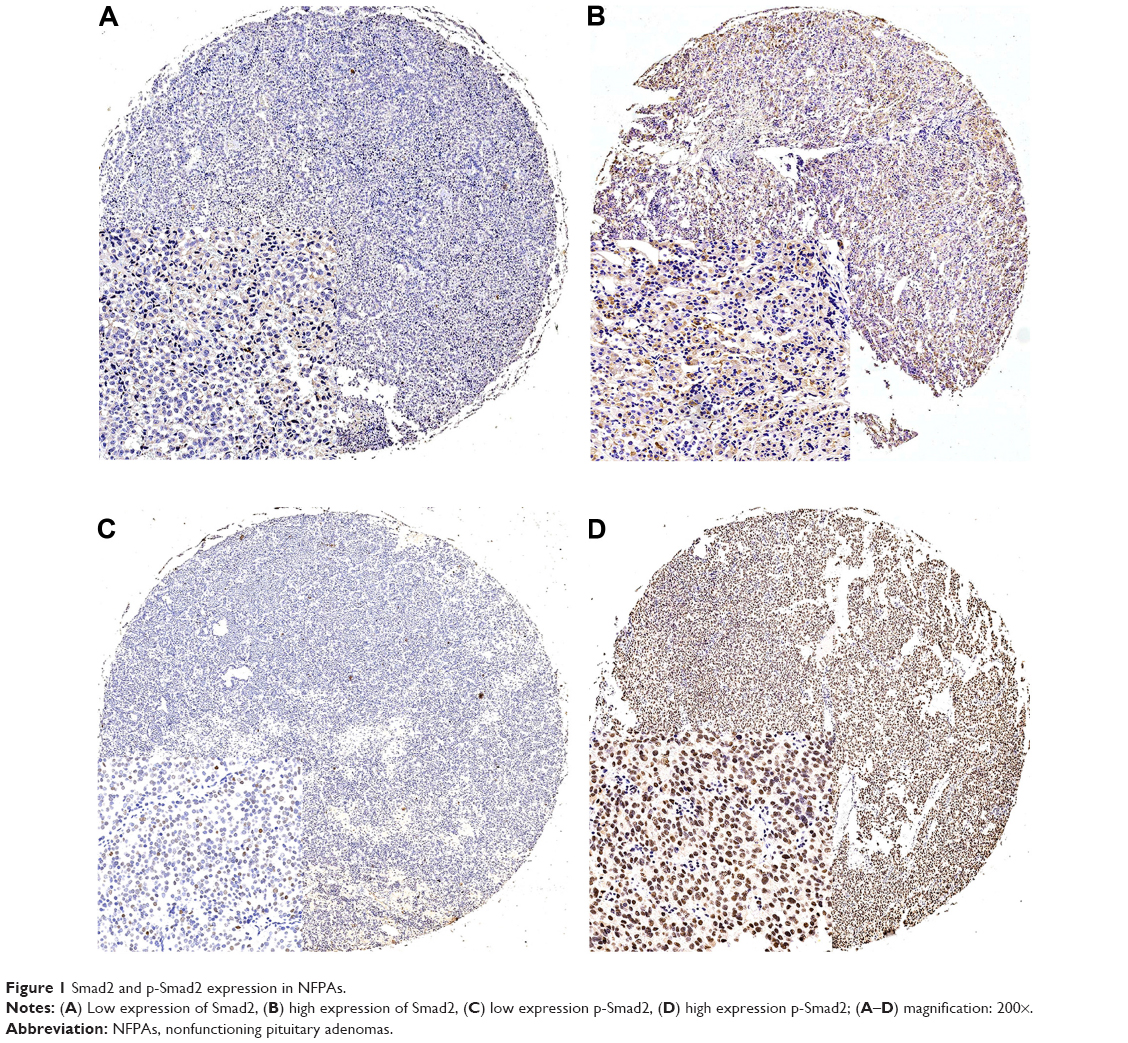 | Figure 1 Smad2 and p-Smad2 expression in NFPAs. |
Expression of Smad3 and p-Smad3 in NFPAs
Next, we sought to investigate the protein levels of Smad3 and p-Smad3 by immunohistochemistry in invasive and noninvasive NFPAs. Surprisingly, we found that the protein levels of Smad3 and p-Smad3 were significantly lower in invasive NFPAs than in noninvasive NFPAs (Figure 2). Smad3 was highly expressed in 15.3% (nine of 59 cases) of invasive NFPAs and 31.4% (32 of 102 cases) of noninvasive NFPAs (P<0.05). p-Smad3 was highly expressed in 10.2% (six of 59 cases) of invasive NFPAs and 40.2% (41 of 102) of noninvasive NFPAs (P<0.01).
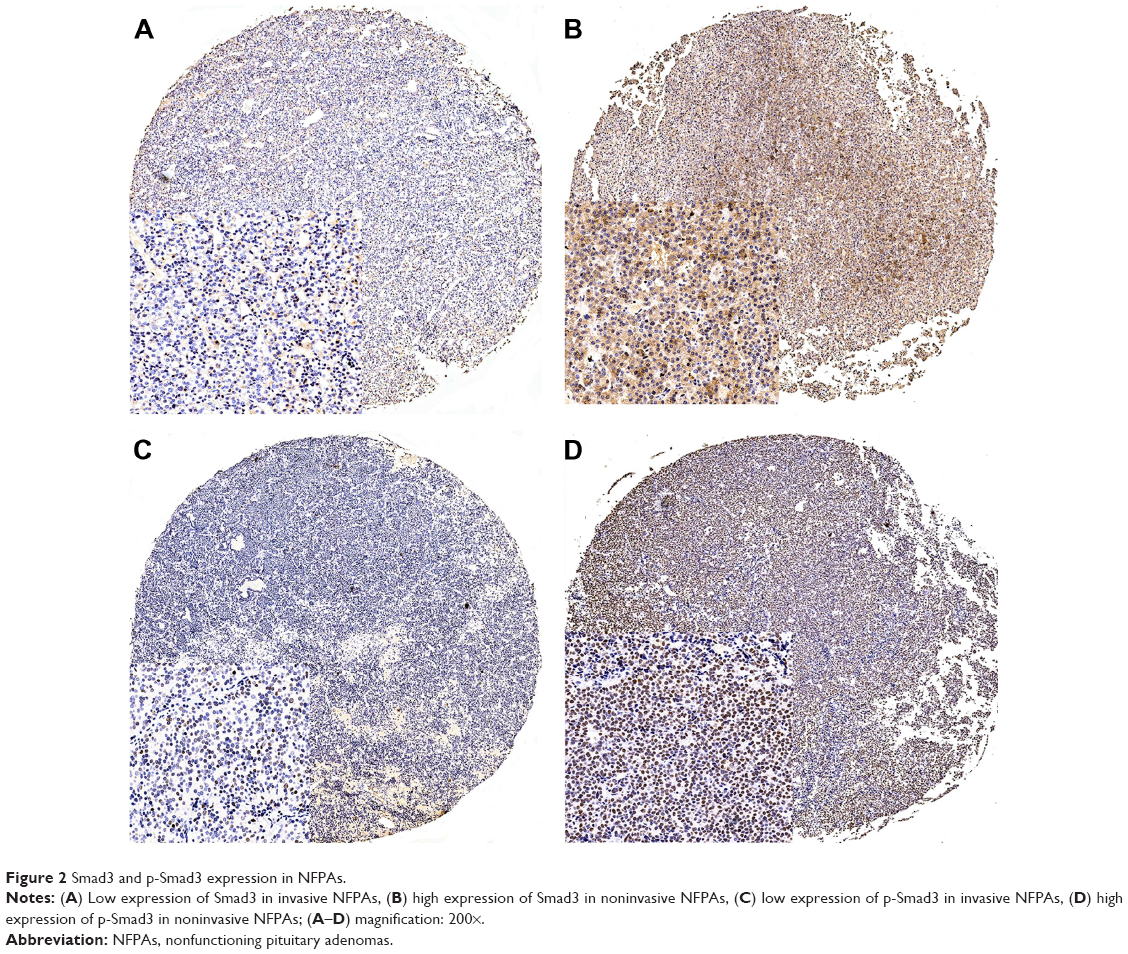 | Figure 2 Smad3 and p-Smad3 expression in NFPAs. |
Expression of Smad4 in NFPAs
We then investigated the protein levels of Smad4 by immunohistochemistry in invasive and noninvasive NFPAs. We found that there was no significant difference in the Smad4 protein levels between invasive NFPAs and noninvasive NFPAs (Figure 3). Smad4 was highly expressed in 37.3% (22 of 59 cases) of invasive NFPAs and 36.3% (37 of 102 cases) of noninvasive NFPAs (P=0.898).
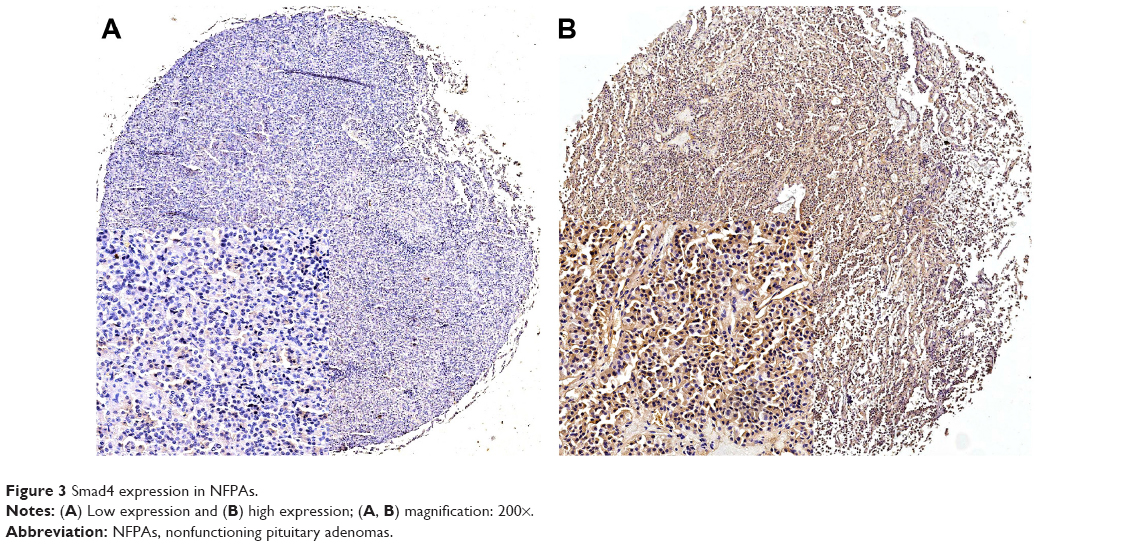 | Figure 3 Smad4 expression in NFPAs. |
Expression of Ki-67 in NFPAs
Ki-67 can serve as an indicator of proliferative activity in NFPAs. We thus evaluated the levels of Ki-67 by immunohistochemistry in invasive and noninvasive NFPAs. We found that the Ki-67 index was markedly greater in invasive NFPAs than in noninvasive NFPAs (P<0.05). Furthermore, Spearman’s rank correlation analysis showed that the Ki-67 index was significantly correlated with p-Smad3 levels (P<0.05, r=-0.702), but not with the levels of Smad2, p-Smad2, Smad3, or Smad4 (Figure 4).
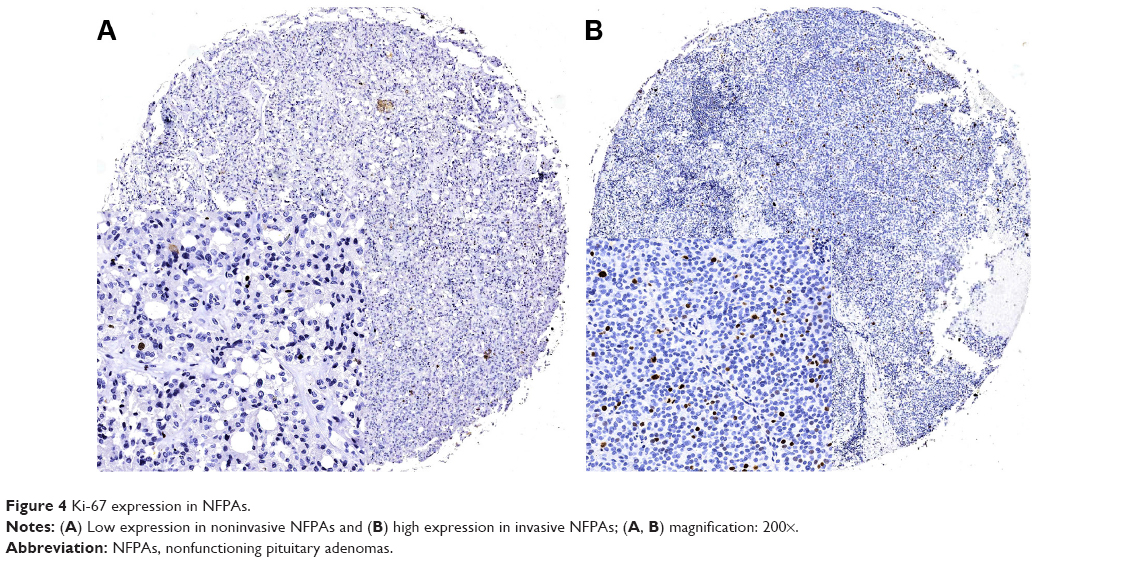 | Figure 4 Ki-67 expression in NFPAs. |
Discussion
In the present study, we investigated TGF-β/Smad signaling and its proliferative activity in a large number of invasive and noninvasive NFPAs. We found that a low level of Smad3 and p-Smad3 was associated with the invasion of NFPAs, and that proliferative activity was greater in invasive NFPAs than in noninvasive NFPAs.
Smad3 is a key factor in TGF-β/Smad3-mediated tumor suppressor effect. Wolfraim et al13 demonstrated that a reduction in Smad3 expression contributes to promote T-cell leukemogenesis. Moreover, Sodir et al14 reported that Smad3 deficiency promotes tumorigenesis in distal colon. In addition, it has been reported that Smad3 mutation in human cancer can functionally inactivate the Smad3 protein.15 In this study, we found that the expression of Smad3 and p-Smad3 was decreased in invasive NFPAs as compared with noninvasive NFPAs. Furthermore, we found that the Ki-67 index, an indicator for the proliferative activity of tumor cells, was markedly greater in invasive NFPAs than in noninvasive NFPAs and was significant correlated with p-Smad3 levels. These data suggest that Smad3 may act as a tumor suppressor in NFPAs and that TGF-β signaling may contribute to the invasion of NFPAs.
Smad2 and Smad4 have been identified as tumor suppressors in various human tumors,16–19 including gastric, esophagus, liver, and breast cancers. Liu et al20 reported that Smad4 expression is reduced in ductal breast carcinoma as compared with surrounding uninvolved ductal breast epithelia, suggesting that Smad4 has a potential role in the development of breast carcinoma and is a potential prognostic marker of breast carcinoma.20 However, in the present study, we found that there was no significant difference in Smad2 and Smad4 protein levels between invasive NFPAs and noninvasive NFPAs. The discrepancy on Smad2 and Smad4 between PAs and other tumors suggests that the roles of Smad2 and Smad4 in PAs may be different and need to be further investigated.
Conclusion
In summary, this study showed that the protein levels of Smad3 and p-Smad3 are decreased in invasive NFPAs. This decrease in Smad3 and p-Smad3 may be associated with the invasion of NFPAs, and Smad3 and p-Smad3 may be useful biomarkers for the diagnosis of invasive NFPAs. Patients who have NFPAs with low expression of Smad3 and p-Smad3 may benefit from aggressive treatment and close surveillance.
Acknowledgments
This work was supported by the National High Technology Research and Development Program of China (863 Program) (2014AA020610), the Research Special Fund for Public Welfare Industry of Health (201402008), and the National Natural Science Foundation of China (31200796).
Disclosure
The authors report no conflicts of interest in this work.
References
Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A. High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab. 2006;91(12):4769–4775. | ||
Fernandez A, Karavitaki N, Wass JA. Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol (Oxf). 2010;72(3):377–382. | ||
Katznelson L, Alexander JM, Klibanski A. Clinical review 45: clinically nonfunctioning pituitary adenomas. J Clin Endocrinol Metab. 1993;76(5):1089–1094. | ||
Colao A, Di Somma C, Pivonello R, Faggiano A, Lombardi G, Savastano S. Medical therapy for clinically non-functioning pituitary adenomas. Endocr Relat Cancer. 2008;15(4):905–915. | ||
Wakefield LM, Roberts AB. TGF-beta signaling: positive and negative effects on tumorigenesis. Curr Opin Genet Dev. 2002;12(1):22–29. | ||
Massague J. TGFbeta in cancer. Cell. 2008;134(2):215–230. | ||
Massague J. TGFbeta signalling in context. Nat Rev Mol Cell Biol. 2012;13(10):616–630. | ||
Heldin CH, Miyazono K, ten Dijke P. TGF-beta signalling from cell membrane to nucleus through SMAD proteins. Nature. 1997;390(6659):465–471. | ||
Nakao A, Afrakhte M, Moren A, et al. Identification of Smad7, a TGFbeta-inducible antagonist of TGF-beta signalling. Nature. 1997;389(6651):631–635. | ||
Zhenye L, Chuzhong L, Youtu W, et al. The expression of TGF-beta1, Smad3, phospho-Smad3 and Smad7 is correlated with the development and invasion of nonfunctioning pituitary adenomas. J Transl Med. 2014;12:71. | ||
Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery. 1993;33(4):610–617; discussion 617–618. | ||
Li ZY, Zhang XH, Chen Y, et al. Clinical significance of B7-H4 expression in matched non-small cell lung cancer brain metastases and primary tumors. Onco Targets Ther. 2013;6:869–875. | ||
Wolfraim LA, Fernandez TM, Mamura M, et al. Loss of Smad3 in acute T-cell lymphoblastic leukemia. N Engl J Med. 2004;351(6):552–559. | ||
Sodir NM, Chen X, Park R, et al. Smad3 deficiency promotes tumorigenesis in the distal colon of ApcMin/+ mice. Cancer Res. 2006;66(17):8430–8438. | ||
Ku JL, Park SH, Yoon KA, et al. Genetic alterations of the TGF-beta signaling pathway in colorectal cancer cell lines: a novel mutation in Smad3 associated with the inactivation of TGF-beta-induced transcriptional activation. Cancer Lett. 2007;247(2):283–292. | ||
Hahn SA, Schutte M, Hoque AT, et al. DPC4, a candidate tumor suppressor gene at human chromosome 18q21.1. Science. 1996;271(5247):350–353. | ||
Wang LH, Kim SH, Lee JH, et al. Inactivation of SMAD4 tumor suppressor gene during gastric carcinoma progression. Clin Cancer Res. 2007;13(1):102–110. | ||
Natsugoe S, Xiangming C, Matsumoto M, et al. Smad4 and transforming growth factor beta1 expression in patients with squamous cell carcinoma of the esophagus. Clin Cancer Res. 2002;8(6):1838–1842. | ||
Yakicier MC, Irmak MB, Romano A, Kew M, Ozturk M. Smad2 and Smad4 gene mutations in hepatocellular carcinoma. Oncogene. 1999;18(34):4879–4883. | ||
Liu N-n, Xi Y, Callaghan MU, et al. SMAD4 is a potential prognostic marker in human breast carcinomas. Tumor Biol. 2013;35(1):641–650. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.