Back to Journals » Nature and Science of Sleep » Volume 12
Sleep Patterns and Quality in Omani Adults
Authors Al-Abri MA ![]() , Al lawati I, Zadjali F, Ganguly S
, Al lawati I, Zadjali F, Ganguly S
Received 8 October 2019
Accepted for publication 10 March 2020
Published 14 April 2020 Volume 2020:12 Pages 231—237
DOI https://doi.org/10.2147/NSS.S233912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sutapa Mukherjee
Mohammed A Al-Abri,1 Ibtisam Al lawati,2 Fahad Zadjali,3 Shyam Ganguly4
1Department of Physiology, College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Sultanate of Oman; 2Department of Physiology, Oman College of Health Sciences, Muscat, Sultanate of Oman; 3Department of Biochemistry, College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Sultanate of Oman; 4Department of Family Medicine and Public Health, College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Sultanate of Oman
Correspondence: Mohammed A Al-Abri
Department of Physiology, College of Medicine and Health Sciences, Sultan Qaboos University Hospital, Al-Khoud 123, P.O. Box 38, Muscat, Sultanate of Oman
Tel +968 24144702
Email [email protected]
Background: Sleep patterns have changed continuously worldwide and it can be influenced by social, cultural, and environmental factors. These patterns may be associated with poor sleep quality and daytime sleepiness. The aim of the study was to investigate sleep patterns and quality in Omani adults using actigraphy.
Subjects and Methods: This was a cross-sectional study conducted between June 2015 and February 2017. Four hundred subjects agreed to participate in the study (52% male, 48% female). Subjects were randomly selected and enrolled in the study among young adults and middle aged individuals living in the City of Muscat. Subjects were asked to fill-in Epworth sleepiness scale (ESS) and Pittsburgh sleep quality index (PSQI). Actigraphy was used to measure their sleep patterns for one week.
Results: The mean age of participants was 32.80± 11.50 years. Four sleep patterns were identified: monophasic, bi-phasic (post-dawn), bi-phasic (afternoon siesta), and polyphasic (three sleep periods/24 hours). The study revealed that 35% of participants had biphasic-siesta sleep pattern, 28% polyphasic, 26% monophasic, and 11% biphasic-dawn. The biphasic siesta pattern was found to be associated with younger age group (25– 34 years) (P=0.001). Polyphasic sleep was associated with higher ESS score (P=0.001) but not with poor sleep quality (P=0.24). There was no significant difference in night sleep duration among all the sleep patterns (P=0.07) but the polyphasic sleep pattern had higher total 24-hour day sleep duration (P=0.03). Nearly 90% of participants practiced afternoon siestas with mean duration of 45± 43 minutes.
Conclusion: The predominant sleep pattern among Omanis was biphasic-siesta and majority of people practiced afternoon siesta. Polyphasic sleep pattern is associated with daytime sleepiness.
Keywords: sleep patterns, sleepiness, siesta, polyphasic, fragmented sleep
Introduction
Sleep is an imperative physiological aspect that maintains circadian rhythm and hence a healthy life. It is a prominence of unconsciousness in which the brain is more responsive to internal than external stimuli.1 Sleep pattern is dictated by the body to specify the sleep and wake timings aligned by natural daylight and night cycles. A healthy sleep pattern is branded by individual satisfaction, specific sleep timing, sufficient duration, high efficiency, and continuous alertness throughout waking hours.2 Sleep/wakefulness rhythm in humans depends upon a balance between homeostatic sleep duration, tendency, need, and an internal circadian rhythm that altogether determine the ideal timing of a fittingly structured and restorative sleep occurrence inhibiting the various bodily functions associated with being awake.3,4 Generally, sleep patterns are classified into three categories. Monophasic sleep pattern is defined as sleeping once per day at nighttime only.5 Its the most common sleeping pattern and essentially adopted in the most developed societies.6 Biphasic sleep pattern is defined as sleeping twice per day, that comprises most commonly long sleep duration at night (6–7 hours) with a short nap during the day (≤1hour) and is the prevailing norm in Spain and many Latin American countries.6 The third pattern is the polyphasic sleep that consists of multiple sleep periods per day that commonly encompasses short night sleep duration of not more than 3 hours along with 2–3 short naps of 20–30 minutes throughout the day. This pattern is common in working people and students to reduce the sleep duration and to increase the working hours.7 It was observed that people in the Middle East may have all these kinds of sleep patterns.8,9 Nevertheless, there is no study confirming the pattern of sleep using an objective method such as actigraphy.
Quantity and quality of sleep are influenced by the invention of electric lighting, industry, and technology, in addition to social, behavioral, and environmental factors. Modern lifestyle introduced longer working hours, more shift-work, late-night socialization, and availability of technology which collectively altered natural sleep–wake cycle and led to increased sleep deprivation along with fatigue, tiredness, and excessive daytime sleepiness.10 Additionally, fragmented sleep my alter sleep homeostasis and impair the circadian rhythm and can cause phase shift. Afternoon napping may cause delayed nocturnal sleep onset and therefore decrease night sleep duration.11 This is associated with poor sleep quality and increased risk of cardio-metabolic disorders.12,13
Arab Muslims have certain sleep patterns. They have five obligatory prayers per day and the first prayer is dawn prayer, one hour before sunrise. This can split night sleep duration into two segments.14,15 Moreover, recent changes in life-styles due to fast economic development and use of modern technology by the local population accompanied by their ritual duties have led to different sleep habits that may not be shared by other populations in different parts of the world.16 It necessitates staying awake late until or beyond mid-night, followed by a short awaking for dawn prayer before the sunrise.14 This may therefore lead to a longer afternoon siesta the following day leading to a segmented sleep pattern.17 The current study aimed to assess the habitual sleep patterns and quality among Omani adults that could be used to understand the sleep habits among people in this part of the world.
Methods
Study Design and Sample
This cross-sectional study was conducted in Muscat, the capital city of Oman, from summer 2015 until summer 2017. The Muslim’s holy month of Ramadan and the following month in the lunar calendar were excluded because of change in people’s rituals and eating habits. The Medical Research Ethics Committee at Sultan Qaboos University approved the study design and methods with code MREC # 1078 and this study was conducted in accordance with the Declaration of Helsinki. The target group was Omani adults, aged 18–64 years of both genders. Eight hundred questionnaires were randomly distributed by the researcher in Muscat, the largest metropolitan area in Oman; either directly or through electronic and paper announcements. Subjects were excluded if they met any of the following criteria: past/present medical history including cancer, psychiatric illness, pregnancy and breast feeding (women), mothers having children below one year, and shift workers. The participants had not traveled across the time zone for at least one month.
Questionnaires
Study questionnaires were self-administered questions. The participants filled out an identification form with their personal data, education level, and health status. Each volunteer signed a written informed consent form. Two previously validated Arabic questionnaires were used: Epworth Sleepiness Scale (ESS)18 and the Pittsburgh Sleep Quality Index (PSQI).19 Values of ESS score ≥10 were considered to indicate significant daytime sleepiness.20 Sleep quality over the past month was evaluated using the Arabic PSQI. Participants with a global score of greater than 5 were classified as poor sleepers. Those with a score of 5 or less were categorized as good sleepers.21 Additional questions were added to identify the sleep patterns and food habits: 1) what time do you usually sleep at night during the weekdays (Sunday to Thursday) and weekends (Friday and Saturday)? 2) Do you usually sleep after dawn prayer? And if yes, How long? 3) What time do you usually wake up in the morning during the weekdays and weekends? 4) Do you usually sleep in the afternoon? If yes, for how long? 5) Do you usually wake up during the night sleep? How many times? 6) Do you snore, gasp or have apnea during night sleep? 7) Do you feel sleepy while driving?
Based on frequency of sleep periods throughout the day, sleep patterns were classified into three categories: 1) monophasic pattern which essentially consists of sleeping once per day, 2) biphasic pattern – sleeping twice per day, and 3) polyphasic pattern – the practice of sleeping multiple times in a 24-hour period, usually three periods or more.22 Biphasic pattern was further sub-divided into bi-dawn and bi-siesta pattern.
Night and day sleep duration were categorized based on American National Sleep Foundation recommendation23 as follows: normal (7–9 hours), short (< 7 hours), and long (> 9 hours). Afternoon siesta was categorized as short ≤ 1 hour, and long > 1 hour.24
Methods of Sleep Patterns' Measurement
Actigraphy watch (SOMNOWATCH TM Plus, SOMNO medics, Germany, 2014) was the actigraphy device selected for this study. The participants were requested to wear the actigraphy watch for 7 days for 24 hours a day. The participants were asked to run their daily activities as usual and avoid traveling across time zone during the period of the study. Sleep patterns on weekdays (Sunday to Thursday) and weekends (Friday and Saturday) were also analyzed. Subjects were also provided with the home sleep study (AASM level III) (Somnotouch, Somnomedics, Germany) for one night to exclude obstructive sleep apnea. Actigraphy recordings were manually scored and timing of sleep and wake up was obtained. Nocturnal sleep duration and afternoon siesta were also calculated.
Statistical Analysis
Sampling Design and Subjects
Simple random sampling method was used in this survey-based research. An adequate sample size of 384 subjects was estimated based on the prevalence of event of interest (50%), with a margin of error of 10% on either side of the estimate with 95% confidence intervals.25 Descriptive analysis for continuous variables was used to calculate mean, median, and standard deviation (SD). Prevalence and frequencies were expressed as percentages. Chi-squared tests were used for establishing the relationship between the two categorical variables, and comparison of median duration of sleep between weekdays and weekends were compared using Mann–Whitney tests. Kruskal–Wallis one-way analysis of variance was used to compare the duration of sleep between the sleep patterns. A p-value (two-tailed) of less than 0.05 was considered as statistically significant. All data were coded and analyzed with the Statistical Package for Social Sciences Software (SPSS Version 22.0, Inc., Chicago, IL, USA). Participants who fully completed the study were included in the data analysis. Non-responders or those with incomplete actigraphy data (he/she used the watch for less than one week) were excluded.
Results
Demographic Description
Eight hundred questionnaires were distributed and four hundred and five subjects (50%) completed the study (52% male, 48% female). Two thirds of the participants had full time jobs (60.25%) and 29.88% were students, 7.41% were unemployed housewives, and 2.47% were retired. The mean age of the subjects was 32.82 years and men (35.6±10.8 years) were older than women (29.7±11.60 years). The rest of the demographic data can be found in Table 1.
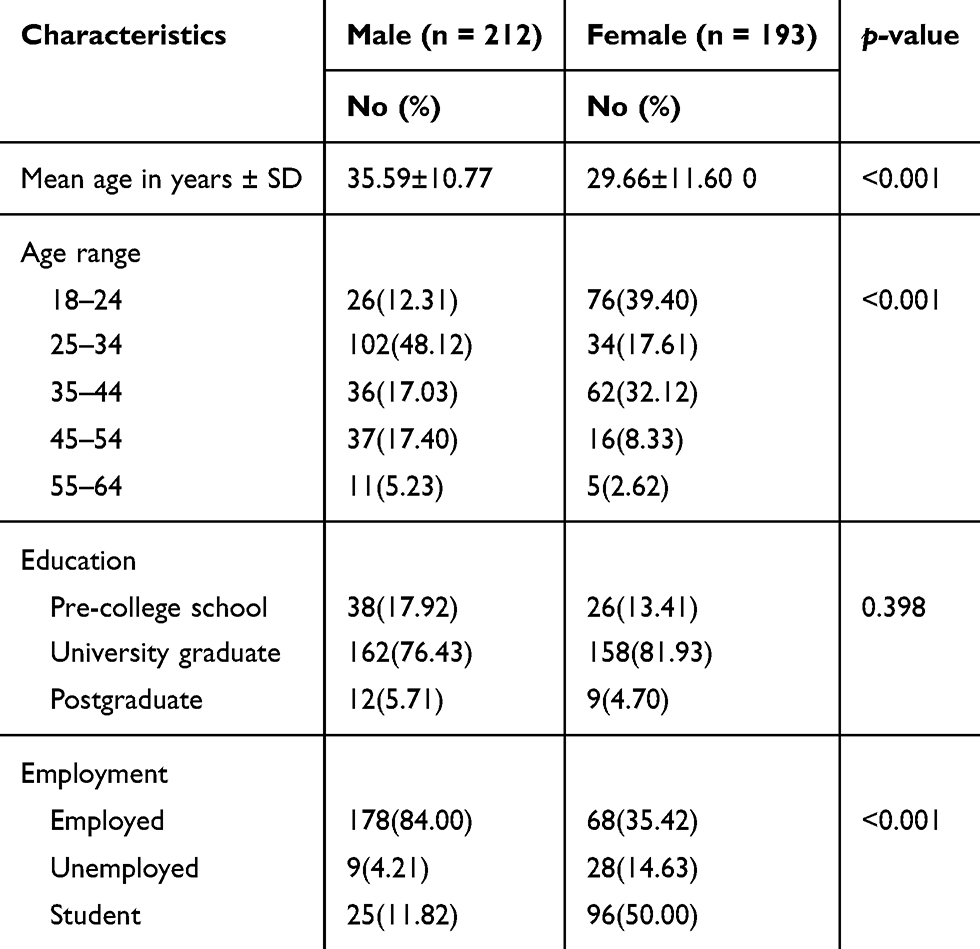 |
Table 1 Distribution of 405 Omani Adults According to Their Socio-Demographic Characteristics |
Sleep Characteristics
The study revealed that 35% of participants had biphasic-siesta sleep pattern, 28% polyphasic, 26% monophasic, and 11% biphasic-dawn. Detailed distribution of sleep patterns among age groups and genders is shown in Figure 1.
 |
Figure 1 Sleep patterns among the study sample based on one week of actigraphy recording. Data shown are percentage to total for males and females separately. |
The average duration of night sleep of the whole cohort was 6.92±1.33 hours with men sleeping significantly (P=0.005) shorter periods (6.72±1.28 hours) than women (7.11±1.36 hours). However, the total 24-hour day sleep duration was 7.91 ±1.46 hours and there was no significant difference between men and women (7.80±1.50, 7.98±1.47 hours respectively) (P=0.13).
There was significant variation (P=0.002) among age groups in sleep patterns, with the younger (18–34 years) population tending to have more of a biphasic siesta sleep pattern, which is the case with employed people (P=0.013). Detailed characteristics of sleep duration among all sleep patterns are described in Tables 2 and 3.
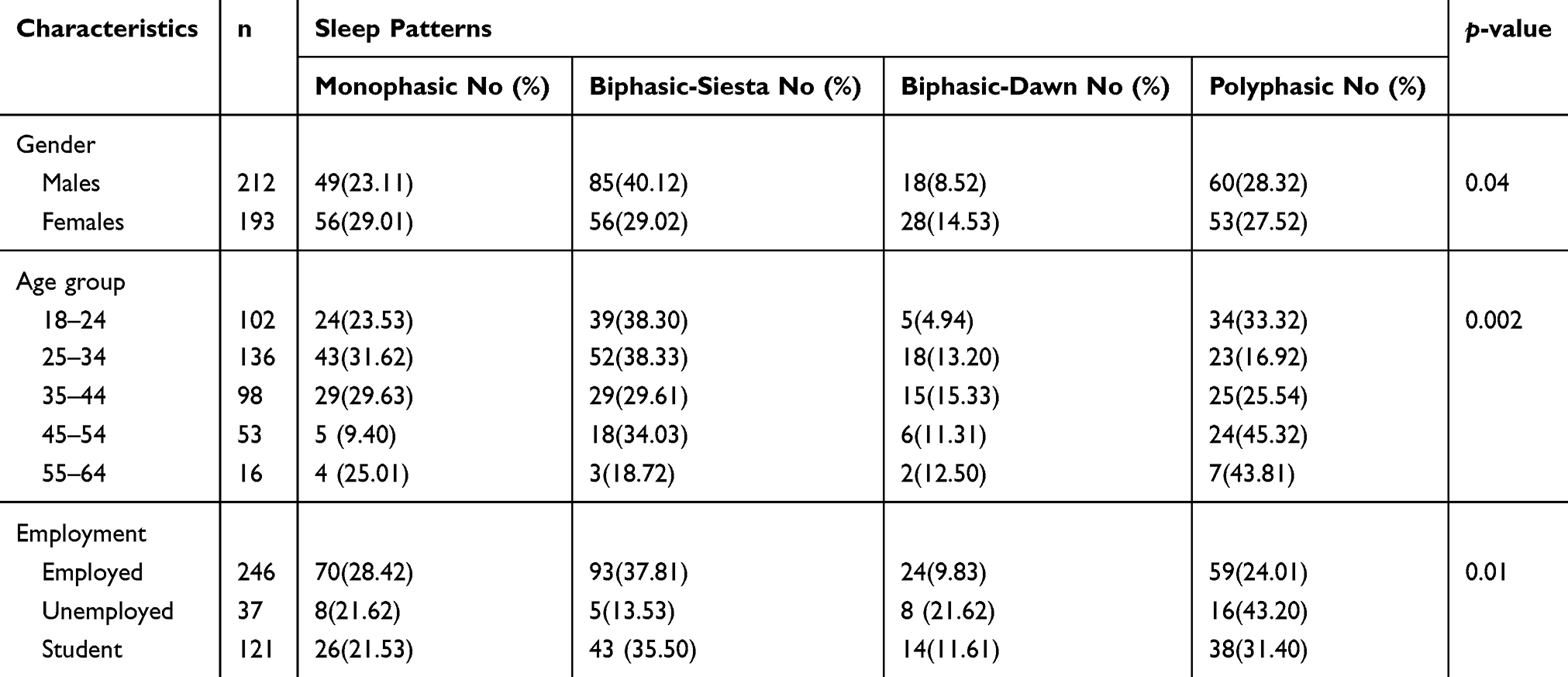 |
Table 2 Actigraphy-Based Sleep Pattern in Relation to Gender, Age, and Employment Status in Omani Adults |
 |
Table 3 Mean Duration of Sleep Characteristics Between the Four Types of Sleep Patterns |
Additional results not tabulated, showed that men had significantly (P=0.02) longer siesta duration compared to women (50.22±44.20, 40.31±41.40 minutes respectively). Furthermore, actigraphy recordings indicated that participants tended to sleep late at night with 80% of participants sleep around 12:00 am.
Weekdays and Weekend Sleep Pattern
There was no significant variation in sleep patterns between weekdays and weekends (P=0.22), with biphasic-siesta still the predominant pattern (30.50%). Majority of participants practiced afternoon siesta (85%) with mean duration of 45±43 minutes with significant variation between weekdays and weekends (P=0.002). There was also significant variation between weekdays and weekends in night sleep durations (P<0.001) and total day sleep durations (P<0.001) Table 4.
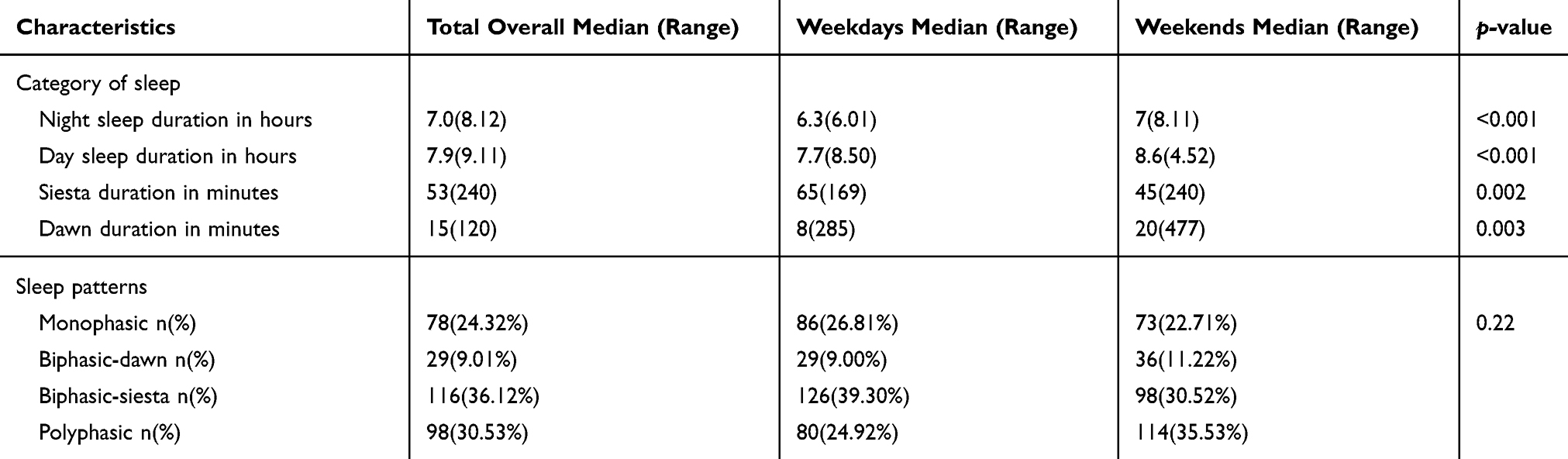 |
Table 4 Characteristics of Sleep Patterns During Weekdays and Weekends (n=405) |
Sleep Pattern and Daytime Sleepiness
The study sample showed mean ESS score of 8.24±3.97 with 29.10% of the sample scoring > 10. Polyphasic sleepers had significantly more daytime sleepiness (9.47±4.26) compared to other sleep patterns (P=0.001).
Sleep Pattern and Sleep Quality
The overall quality of sleep among participants was good with PSQI score of 5.91±3.31. Biphasic-siesta sleepers reported the worst sleep quality (6.35±3.52). However, polyphasic sleepers had the highest quality of sleep indexed by PSQI (5.55±3.01) but not significantly different from other sleep patterns (P =0.24).
Discussion
The key findings of this cross-sectional study indicated that the vast majority of our local population has segmented sleep patterns. The biphasic-siesta sleep pattern was the prevailing pattern that accounted for more than one third of the sample followed by the polyphasic pattern. In contrast, monophasic sleepers who slept a single portion only throughout the night were the least common among the participants. Furthermore, our study indicated that younger age groups have more segmented sleep patterns, either biphasic siesta or polyphasic, that may carry a potential risk of cardiometabolic disorders which needs further prospective follow-up study.26
Our study revealed high prevalence of relatively short night sleep duration (<7 hours) across three sleep patterns (biphasic siesta, biphasic dawn, and polyphasic) in comparison to global standards of nocturnal sleep durations.27 However, the biphasic-dawn sleepers had almost normal nocturnal sleep duration of seven hours. Additionally, our study indicated that the vast majority of participants practiced afternoon siesta with median range of 53 minutes. Polyphasic sleepers had significantly longer afternoon siesta (>one hour) and therefore longer total 24-hour day sleep. Furthermore, participants practiced afternoon siesta more during weekdays than weekends, and that might be attributed to short nocturnal sleep duration.
Our results indicated that sleeping less than seven hours per night are in accord with findings of other studies that have assessed nocturnal sleep duration. National Sleep Foundation recommends that adults need 7–9 hours of sleep per night, although individual differences occur.28 It was reported a century ago that the average adult American slept nine hours a night but since then the average has gradually declined, especially in the last four decades, to approximately 6.5 hours, as reported by epidemiological and community-based studies.29,30 Another survey showed that the odds of short night sleep duration among Americans had significantly increased during the period from 1975 to 2006, especially among full-time workers.31
However, the total duration of sleep per 24 hours in our sample was similar to findings of other studies with an average of 7–8 hours. Comparing our results with other communities, a survey on 35,327 adults in ten countries showed an average duration of 7 hours and 34 minutes per 24 hours. Among which, the least was practiced by Japanese with an average of 6 hours, 53 minutes, and the most in Portuguese who slept 8 hours, 24 minutes on average.32
Segmented sleep pattern among Omani population which consists mainly of short night sleep and afternoon naps could also be explained by three main factors: environmental factor, work timing, and ritual obligations. The study revealed that employed participants whom constituted around two thirds of the sample, practiced more biphasic siesta and polyphasic sleep patterns. Majority of Omani population work in the public sector and the work shifts usually start at 7:30 or 8:00 am and ends at around 2–3 pm. Therefore there is time during the day for napping after a late lunch, particularly in summer with average day temperature of 40°C.33
Segmented sleep pattern, including daytime nap or siesta, is common throughout the Mediterranean and Southern Europe, Spain, Southern Italy, many Hispanic American countries, the Philippines, parts of Africa, China, and Japan.34–36 Daytime napping is also common in other communities; for example among Brazilian Native Terena adults, 72.4% of them had regular daytime naps at least once a week, while, in Japan, only 12.0% took regular daytime naps.34,37 Unlike our study sample who had long afternoon nap duration (> 60 min), other communities have daytime naps that last 40–60 min.38 However, segmented sleep pattern of short night sleep and sleep after dawn prayer before the sunrise (biphasic dawn) is probably unique to Muslim communities, including Oman.
The high prevalence of short night sleep duration among the study sample could be the leading cause for excessive daytime sleepiness with ESS score more than 10 among almost one third of the participants, but the overall sleep quality was good, as indicated by PSQI score. Furthermore, polyphasic sleepers had significantly more daytime sleepiness than other sleep patterns but they have a relatively better quality of sleep, as indicated by PSQI. Compared to other studies, it was estimated that 25% of Americans reported excessive daytime sleepiness.39 Likewise, a study in South Korea found that the prevalence of excessive daytime sleepiness was 12.2% and they attributed that to different factors such as habitual snoring and insufficient nocturnal sleep.40
Another study by Bahammam et al found that there was no difference in sleep architecture or daytime sleepiness in the consolidated and split-sleep schedules (dawn prayer) when the total sleep duration was maintained. Therefore, segmental sleep does not cause excessive daytime sleepiness or poor sleep quality.14
Conclusion
The overall findings of the study indicated that biphasic siesta sleep is a predominant pattern among Omani adults. In addition, both polyphasic and biphasic siesta sleep patterns are associated with daytime sleepiness. There are multiple factors behind these findings which encompass work, culture, and environment. However, further investigations are required to confirm the impact of these sleep patterns on people’s health.
Acknowledgment
The study was funded by the research council of Oman.
Disclosure
The abstract was presented at the World Sleep Medicine Congress, Prague, 2017, and published in Journal of Sleep Medicine (Sleep Medicine 40 (2017) e3-e185). The authors report no conflicts of interest in this work.
References
1. Buysse D. Sleep health: can we define it? Does it matter? Sleep. 2014;37(1):9–17. doi:10.5665/sleep.3298
2. Roepke SE, Duffy JF. Differential impact of chronotype on weekday and weekend sleep timing and duration. Nat Sci Sleep. 2010;2010:213–220. doi:10.2147/NSS.S12572
3. Capellini I, Nunn CL, McNamara P, Preston BT, Barton RA. Energetic constraints, not predation, influence the evolution of sleep patterning in mammals. Funct Ecol. 2008;22(5):847–853. doi:10.1111/j.1365-2435.2008.01449.x
4. Deboer T. Sleep homeostasis and the circadian clock: do the circadian pacemaker and the sleep homeostat influence each other’s functioning? Neurobiol Sleep Circadian Rhythms. 2018;5:68–77. doi:10.1016/j.nbscr.2018.02.003
5. Matuzaki L, Santos-Silva R, Marqueze EC, de Castro Moreno CR, Tufik S, Bittencourt L. Temporal sleep patterns in adults using actigraph. Sleep Sci. 2014;7(3):152–157. doi:10.1016/j.slsci.2014.09.012
6. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala NB. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. 2012;35:1173–1181. doi:10.5665/sleep
7. Akacem LD, Simpkin CT, Carskadon MA, et al. The timing of the circadian clock and sleep differ between napping and non-napping toddlers. PLoS One. 2015;10(4):e0125181. doi:10.1371/journal.pone.0125181
8. Saeed Z, Hasan Z, Atif M. Sleep patterns of medical students; their relationship with academic performance: a cross sectional survey. Prof Med J. 2015;22:913–923.
9. Merdad RA, Merdad LA, Nassif RA, El-Derwi D, Wali SO. Sleep habits in adolescents of Saudi Arabia; distinct patterns and extreme sleep schedules. Sleep Med. 2014;15(11):1370–1378. doi:10.1016/j.sleep.2014.06.008
10. Shochat T. Impact of lifestyle and technology developments on sleep. Nat Sci Sleep. 2012;4:19–31. doi:10.2147/NSS.S18891
11. Mongrain V, Dumont M. Increased homeostatic response to behavioral sleep fragmentation in morning types compared to evening types. Sleep. 2007;30:773–780. doi:10.1093/sleep/30.6.773
12. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33(2):414–420. doi:10.2337/dc09-1124
13. Fang W, Li Z, Wu L, et al. Longer habitual afternoon napping is associated with a higher risk for impaired fasting plasma glucose and diabetes mellitus in older adults: results from the Dongfeng-Tongji cohort of retired workers. Sleep Med. 2013;14(10):950–954. doi:10.1016/j.sleep.2013.04.015
14. Bahammam AS, Sharif MM, Spence DW, Pandi-Perumal SR. Sleep architecture of consolidated and split sleep due to the dawn (Fajr) prayer among muslims and its impact on daytime sleepiness. Ann Thorac Med. 2012;7:36–41. doi:10.4103/1817-1737.91560
15. Bahammam AS. Sleep from an Islamic perspective. Ann Thorac Med. 2011;6(4):187–192. doi:10.4103/1817-1737.84771
16. Al-Hazzaa HM, Musaiger AO, Abahussain NA, Al-Sobayel HI, Qahwaji DM. Lifestyle correlates of self‐reported sleep duration among Saudi adolescents: a multicentre school‐based cross‐sectional study. Child Care Health Dev. 2014;40:533–542. doi:10.1111/cch.12051
17. Al-Hazzaa HM, Musaiger AO, Abahussain NA, Al-Sobayel HI, Qahwaji DM. Prevalence of short sleep duration and its association with obesity among adolescents 15-to 19-year olds: a cross-sectional study from three major cities in Saudi Arabia. Ann Thorac Med. 2012;7:133. doi:10.4103/1817-1737.98845
18. Al-Abri M, Al-Hamhami A, Al-Nabhani H, Al-Zakwani I. Validation of the arabic version of the epworth sleepiness scale in Oman. Oman Med J. 2013;28:454–456. doi:10.5001/omj
19. Suleiman KH, Yates BC, Berger AM, et al. Translating the Pittsburgh sleep quality index into Arabic. West J Nurs Res. 2010;32(2):250–268. doi:10.1177/0193945909348230
20. Johns MW. A new method for measuring daytime sleepiness: the epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
21. Buysse D, Reynolds CF, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
22. Campbell S, Murphy P. The nature of spontaneous sleep across adulthood. J Sleep Res. 2007;16(1):24–32. doi:10.1111/j.1365-2869.2007.00567.x
23. Lombardi DA, Folkard S, Willetts JL, Smith GS. Daily sleep, weekly working hours, and risk of work-related injury: US National Health Interview Survey (2004–2008). Chronobiol Int. 2010;27(5):1013–1030. doi:10.3109/07420528.2010.489466
24. Stang A, Dragano N, Poole C, et al. Daily siesta, cardiovascular risk factors, and measures of subclinical atherosclerosis: results of the Heinz Nixdorf Recall Study. Sleep. 2007;30(9):1111. doi:10.1093/sleep/30.9.1111
25. Suresh K, Chandrashekara S. Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci. 2012;5(1):7–13. doi:10.4103/0974-1208.97779
26. Laposky AD, Bass J, Kohsaka A, et al. Sleep and circadian rhythms: key components in the regulation of energy metabolism. FEBS Lett. 2008;582(1):142–151. doi:10.1016/j.febslet.2007.06.079
27. Honma K, Honma S, Kohsaka M, Fukuda N. Seasonal variation in the human circadian rhythm: dissociation between sleep and temperature rhythm. Am J Physiol. 1992;262(5 Pt 2):R885–R891. doi:10.1152/ajpregu.1992.262.5.R885
28. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–243. doi:10.1016/j.sleh.2015.10.004
29. Soldatos CR, Allaert FA, Ohta T, Dikeos DG. How do individuals sleep around the world? Results from a single-day survey in ten countries. Sleep Med. 2005;6(1):5–13. doi:10.1016/j.sleep.2004.10.006
30. Adenekan B, Pandey A, McKenzie S, Zizi F, Casimir GJ, Jean-Louis G. Sleep in America: role of racial/ethnic differences. Sleep Med Rev. 2013;17(4):255–262. doi:10.1016/j.smrv.2012.07.002
31. Knutson KL, Van Cauter E, Rathouz PJ, DeLeire T, Lauderdale DS. Trends in the prevalence of short sleepers in the USA: 1975–2006. Sleep. 2010;33(1):37–45. doi:10.1093/sleep/33.1.37
32. Liu X, Uchiyama M, Kim K, et al. Sleep loss and daytime sleepiness in the general adult population of Japan. Psychiatry Res. 2000;93(1):1–11. doi:10.1016/S0165-1781(99)00119-5
33. Milner CE, Cote KA. Benefits of napping in healthy adults: impact of nap length, time of day, age, and experience with napping. J Sleep Res. 2009;18:272–281. doi:10.1111/j.1365-2869.2008.00718
34. Furihata R, Kaneita Y, Jike M, Ohida T, Uchiyama M. Napping and associated factors: a Japanese nationwide general population survey. Sleep Med. 2016;20:72–79. doi:10.1016/j.sleep.2015.12.006
35. Sayón-Orea C, Bes-Rastrollo M, Carlos S, Beunza JJ, Basterra-Gortari FJ, Martínez-González MA. Association between sleeping hours and siesta and the risk of obesity: the SUN mediterranean cohort. Obes Facts. 2013;6(4):337–347. doi:10.1159/000354746
36. Lin D, Sun K, Li F, et al. Association between habitual daytime napping and metabolic syndrome: a population-based study. Metabolism. 2014;63(12):1520–1527. doi:10.1016/j.metabol.2014.08.005
37. Reimão R, Souza JC, Gaudioso CE, et al. Siestas among Brazilian Native Terena adults: a study of daytime napping. Arq Neuropsiquiatr. 2000;58(1):39–44. doi:10.1590/S0004-282X2000000100006
38. Bursztyn M, Ginsberg G, Stessman J. The siesta and mortality in the elderly: effect of rest without sleep and daytime sleep duration. Sleep. 2002;25(2):187–191. doi:10.1093/sleep/25.2.187
39. Baldwin CM, Ervin A-M, Mays MZ, et al. Sleep disturbances, quality of life, and ethnicity: the Sleep Heart Health Study. J Clin Sleep Med. 2010;6(02):176–183. doi:10.5664/jcsm.27768
40. Joo S, Baik I, Yi H, Jung K, Kim J, Shin C. Prevalence of excessive daytime sleepiness and associated factors in the adult population of Korea. Sleep Med. 2009;10(2):182–188. doi:10.1016/j.sleep.2008.03.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.