Back to Journals » Nature and Science of Sleep » Volume 13
Sleep Efficiency is Inversely Associated with Brachial Artery Diameter and Morning Blood Pressure in Midlife Adults, with a Potential Sex-Effect
Authors Thosar SS ![]() , Chess D, Bowles NP
, Chess D, Bowles NP ![]() , McHill AW
, McHill AW ![]() , Butler MP, Emens JS, Shea SA
, Butler MP, Emens JS, Shea SA ![]()
Received 14 July 2021
Accepted for publication 9 September 2021
Published 22 September 2021 Volume 2021:13 Pages 1641—1651
DOI https://doi.org/10.2147/NSS.S329359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Saurabh S Thosar, 1– 4 Daniel Chess, 1 Nicole P Bowles, 1 Andrew W McHill, 1, 2 Matthew P Butler, 1, 5 Jonathan S Emens, 1, 6 Steven A Shea 1, 4
1Oregon Institute of Occupational Health Sciences, Oregon Health & Science University, Portland, OR, USA; 2School of Nursing, Oregon Health & Science University, Portland, OR, USA; 3Knight Cardiovascular Institute, Oregon Health & Science University, Portland, OR, USA; 4OHSU-PSU School of Public Health, Oregon Health & Science University, Portland, OR, USA; 5Department of Behavioral Neuroscience, Oregon Health & Science University, Portland, OR, USA; 6Portland VA Medical Center, Portland, OR, 97239, USA
Correspondence: Saurabh S Thosar
Oregon Institute of Occupational Health Sciences, 3181 S.W. Sam Jackson Park Road, Mail Code 606, Portland, OR, 97239, USA
Tel +1 503 494-2064
Fax +1 503 494-4278
Email [email protected]
Purpose: Sleep efficiency is inversely associated with cardiovascular risk. Brachial artery diameter and flow-mediated dilation (FMD) are noninvasive cardiovascular disease markers. We assessed the associations between sleep efficiency and these vascular markers in midlife adults, including people with sleep apnea.
Patients and Methods: Thirty (18 males) participants completed an in-laboratory 8-hour sleep opportunity beginning at their habitual bedtimes. Polysomnography was used to assess sleep patterns and sleep efficiency (time asleep/time in bed). We measured systolic and diastolic blood pressure, heart rate, and baseline diameter, and FMD immediately upon awakening in the morning. Mixed model analyses, adjusting for apnea-hypopnea and body mass indices, were used to assess the relationship between overnight sleep efficiency and cardiovascular markers. We also explored sex differences.
Results: Sleep efficiency was negatively associated with baseline brachial artery diameter (p = 0.005), systolic BP (p = 0.01), and diastolic BP (p = 0.02), but not flow-mediated dilation or heart rate (p > 0.05). These relationships were confirmed with correlations between sleep efficiency and baseline diameter (r = − 0.52, p = 0.004), systolic BP (r = − 0.43, p = 0.017), and diastolic BP (r = − 0.43, p = 0.019). There was a sex-specific interaction trend for sleep efficiency and arterial diameter (p = 0.07) and a significant sex-specific interaction (p < 0.05) for BP, such that the relationships between sleep efficiency and cardiovascular markers were significant in women but not in men.
Conclusion: In midlife adults, poor sleep efficiency is associated with increased brachial artery diameter and blood pressure, effects that were primarily driven by significant associations in women. These associations could underlie the observed increase in cardiovascular risk in adults with poor sleep and cardiovascular disease.
Keywords: sleep efficiency, midlife adults, obstructive sleep apnea, morning cardiovascular risk, polysomnography, sex differences
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
Sleep is a fundamental behavior necessary for the optimal functioning of all physiological systems, including the cardiovascular (CV) system.1 Habitual short sleep duration is independently associated with increased CV risk, including increased risk for adverse CV events, even after controlling for traditional risk factors, such as age and body mass index.2,3 In addition to sleep duration, quality of sleep is also critical. For instance, sleep efficiency, which is a marker of sleep quality and defined as the ratio of sleep duration and total time in bed (analogous to total recording time when in the laboratory), is negatively associated with CV risk, including blood pressure and atherosclerosis.4–7 Furthermore, an 11-year longitudinal study from the Sleep Heart Health Study cohort (n = 3810) showed a strong inverse association between sleep efficiency, determined via at-home overnight polysomnography, and major adverse CV events.8 However, the physiological mechanisms by which poor sleep efficiency increases CV disease risk are not well understood.
Vascular endothelial function measured non-invasively as brachial artery flow-mediated dilation (FMD) is a well-established cross-sectional and longitudinal marker of CV disease, with poorer dilation implying increased CV risk.9–11 Numerous studies have investigated the relationship between overnight sleep and FMD, but the findings are equivocal. Aggarwal and colleagues discovered that in adult women, subjective poor sleep quality measured using the Pittsburgh Sleep Quality Index (PSQI) was associated with increased endothelial nuclear factor kappa B activation but not associated with FMD.12 Scott and colleagues found similar results using actigraphically measured sleep in a small sample of young and predominantly male adults.13 In contrast, Cooper and colleagues discovered a positive relationship between FMD and sleep quality measured using PSQI and objectively measured rapid eye movement sleep.14 Furthermore, in a sample of participants with existing CV risk (eg, hypertension), Hill and colleagues found a linear relationship between sleep efficiency determined using actigraphy and FMD.15
The discrepancies between these findings could be attributed to various factors, including the age groups studied, the presence of underlying sleep disorders, and the methodology of sleep measurement (subjective vs objective measurements). Indeed, subjective sleep markers are not robust predictors of CV risk,16 and isolated use of actigraphy can overestimate sleep.17 More importantly, previous studies have likely not controlled for the marked time-of-day variation in FMD, as the timing of FMD measurements in these studies is often unreported. FMD has a time-of-day variation driven by the circadian system, with low FMD in the morning and a recovery by noon — a difference of nearly 75% between 6 AM and 11 AM.18–20 The timing of the morning minimum in FMD also corresponds to the time window of increased frequency in major adverse CV events.21,22 There is also evidence that baseline diameter measured as part of FMD is positively associated with CV risk.23–26 Yet, previous reports have not specified the associations between sleep efficiency and baseline diameter. Finally, research on midlife adults in this area is generally lacking but is important considering midlife adults are likely to be at higher risk for CV disease than younger people and have an increased likelihood of an underlying sleep disorder that could impact CV health.27 Furthermore, overt sleep disorders that disrupt sleep quality, such as obstructive sleep apnea, have been found to impair FMD.28
We aimed to explore the relationship between sleep efficiency, determined via gold-standard overnight in-laboratory polysomnography, and baseline diameter and FMD, measured in the morning while controlling for the effects of the internal body clock in midlife adults. We hypothesized that because midlife adults are likely to be at increased CV risk, overnight sleep efficiency will be positively associated with FMD and negatively associated with baseline diameter measured immediately upon awakening in the morning.27 To increase clinical relevance, we also measured standard clinical CV variables, eg, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR), and hypothesized that sleep efficiency would be inversely related to these parameters. Our sample also included people with untreated sleep apnea, which is a common disorder in midlife and can progressively increase CV risk with increasing severity of apnea by various mechanisms, including increased nocturnal blood pressure and increased variability in blood pressure.29–32 Lastly, we explored sex differences as doing so could identify protective or maladaptive CV mechanisms in one group.33
Materials and Methods
Study Approval
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board for human subject protection at the Oregon Health & Science University approved the experimental protocol, and all participants provided written informed consent before study participation.
Data Availability
Deidentified data will be made available upon reasonable request to the corresponding author.
Participants
We report data that were collected as part of a more extensive study of the circadian system’s effects on cardiovascular risk (ClinicalTrials.gov Identifier: NCT02202811). We have previously published limited circadian data from these studies.19,34 Volunteers were recruited using flyers on campus, internet research recruitment websites, and word of mouth.
We excluded volunteers if they reported: 1) a history of any chronic disease (except untreated sleep apnea or untreated high blood pressure [BP < 160/100 mmHg]); 2) pregnancy; 3) current smoking or a history of more than 5 pack-years; 4) use of any prescription or non-prescription medications, or 5) history of travel across more than three time zones in the last three months or shift work in the past six months. We verified the absence of recent drug or medication use by urinalysis (Drugsmart 12 panel cup, Speares Medical Inc, SC, USA). We confirmed non-smoking status by cotinine measurements (NicAlert®, Nymox Corporation, NJ, USA). Each participant also filled out numerous questionnaires, including two sleep profile questionnaires (Sleep Disorders Questionnaire and the Owl & Lark Questionnaire), and underwent a clinical history interview, 12-lead electrocardiogram, clinical, biochemical screening tests of blood, and a physical examination. In addition, we determined each participant’s psychological suitability using the Beck Depression Inventory-II questionnaire and a structured interview (Mini International Neuropsychiatric Interview) with study staff approved by a physician. Participants were excluded if they had a history of severe psychiatric illnesses or psychiatric disorders and no history of treatment with antidepressants, neuroleptic medications, or major tranquilizers.
Pre-Admission at-Home Routine
To stabilize the internal body clock and sleep, for 1–3 weeks before the overnight study, we asked participants to maintain a self-selected overnight eight-hour schedule in bed. We monitored compliance to this schedule by 1) using a mobile actigraphy device (ActiGraph wGT3X-BT, Actigraph Corporation, FL, USA); 2) tracking participants’ call-ins to a time-stamped voicemail box before bed and upon waking; and 3) a detailed sleep diary.
Inpatient Laboratory Studies (Figure 1)
Participants were admitted to the Oregon Clinical and Translational Research Institute (OCTRI) laboratory at OHSU approximately 6 hours after each individual’s habitual wake time determined from the at-home routine. Upon admission, we conducted a drug screen and pregnancy test (in pre-menopausal females). Following a negative screen, participants were fitted with polysomnography electrodes and transducers, and an intravenous line was placed in the non-dominant arm. Lights were set to ~150 lux initially and dimmed to <3 lux approximately seven hours before the sleep opportunity. Six hours before the sleep opportunity, participants were provided with dinner devoid of antioxidants (eg, no oranges or raw tomatoes), chocolate, and caffeine. A light snack was provided 1.5 h before the sleep opportunity. Participants were provided a sleep opportunity in a sound-attenuated, temperature-controlled (20.6–22.2°C) and dark (<1 lux) room at their habitual bedtime established during the at-home routine. Participants remained on bed rest throughout the sleep opportunity, except when they had to use a bedside commode (provided by research nursing while maintaining environmental conditions, including dim light and minimal sound). Eight hours after beginning the sleep opportunity, participants were awoken using a standardized mild auditory stimulus, and the light level was increased to ~3 lux. SBP, DBP, and HR were measured approximately 5 minutes after awakening in a supine position without a posture change, followed by an ultrasound assessment of brachial artery dimensions at rest (see details below).
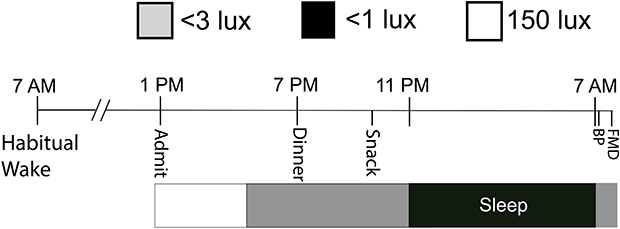 |
Figure 1 Protocol figure. Participants were admitted to the Oregon Clinical and Translational Research Institute (OCTRI) laboratory at OHSU approximately 6 hours after each individual’s habitual wake time. Lights were set to ~150 lux initially and dimmed to <3 lux approximately seven hours before the sleep opportunity. Six hours before the sleep opportunity, participants were provided with dinner, and a light snack was provided 1.5 h before the sleep opportunity. Participants were provided a sleep opportunity in a sound-attenuated, temperature-controlled (20.6–22.2°C) and dark (<1 lux) room at their habitual bedtime established during the at-home routine. Cardiovascular parameters were evaluated after awakening. |
Overnight Polysomnography
We collected and scored sleep, cardiac and respiratory variables using polysomnography, including electrocardiogram, electroencephalogram, electrooculogram, and submental electromyograms according to the American Academy of Sleep Medicine guidelines35 as previously published by our group.20 Specifically, an overnight sleep study (Cadwell Easy III, Cadwell® Industries, Kennewick, WA, USA) was conducted on all participants using two frontal and central leads with reference electrodes placed at contralateral mastoid processes. We measured electrooculogram (EOG) using two offset electrodes placed lateral to the eyes and chin electromyogram (EMG) using two electrodes placed on the chin. Respiratory effort was monitored by thoracic and abdominal piezoelectric belts, whereas airflow was monitored using a nasal cannula. Sleep scoring was performed by a certified polysomnography technologist. Sleep efficiency was calculated as total sleep duration ÷ total recording time (time from lights out to lights on).
Blood Pressure and Heart Rate
SBP, DBP, and HR were measured in the supine position after at least 10 minutes of bed rest using an electronic transducer in the dominant arm and the oscillometric method (Philips SureSigns VS2+ vital signs monitor).36
Flow-Mediated Dilation
FMD of the dominant brachial artery was measured using established guidelines after the above measurements and after at least 20 minutes in a supine resting condition and as performed previously.19,20,37 A 5×84 cm automatic blood pressure cuff (E-20 rapid cuff inflator; D.E. Hokanson, Bellevue, Wash., USA) was placed on the dominant forearm. Images of the brachial artery were obtained with a 2-D high-resolution ultrasound system (Teratech Corp., Burlington, Mass., USA), using a 5- to 12-MHz multifrequency linear-array transducer. Doppler flow signals were corrected at an insonation angle of 60°, and we placed the sample volume in the middle of the artery. Diameter images and Doppler measurements of blood velocity were continuously recorded for 1 minute at baseline before cuff inflation. The automatic blood pressure cuff was then rapidly inflated to 250 mm Hg and maintained for 5 min until cuff deflation. Diameter and blood velocity recordings resumed 1 min before cuff deflation and continued for 3 min after deflation. Ultrasound images were continuously recorded at 5 frames per second with Camtasia (TechSmith, Okemos, Mich., USA) and stored as.avi files for offline analyses.
Arterial Diameters and Blood Velocities
Offline analyses of brachial artery diameters were performed using automated edge-detection software (Brachial Analyzer, Medical Imaging Applications LLC, Coralville, IA, USA) as previously described.38–40 The peak dilation after cuff deflation was determined using the highest 3-second moving average and was presented as a percentage change from baseline diameter (FMD%). Brachial artery shear rate was used as an estimate of arterial shear stress (we did not measure blood viscosity) and calculated using the formula: Vm ÷·D, where Vm is mean blood velocity (cm·s−1) and D is mean arterial diameter (cm). Shear rate area under the curve (SRauc) was calculated as the area from the time of deflation up until peak diameter. FMD% was also normalized to SRauc for analysis. All analyses were performed with blinding of the participant number, date, and time of the image.
Statistical Methods
We first tested the data for outliers; data points outside the mean ± 3 SD were excluded from analyses. To decide whether to include participants with moderate-severe sleep apnea in the analyses, we used a Welch t-test to rule out significant differences between people with moderate or severe OSA (apnea-hypopnea index≥15/hour) and no or mild OSA (apnea-hypopnea index <15/hour) with regard to age, body mass index, sleep duration, efficiency, SBP, DBP, HR, and FMD. Subsequently, we performed a mixed model analysis to test if overnight sleep efficiency significantly predicted morning baseline diameter, FMD, SBP, DBP, and HR while controlling for apnea-hypopnea index and body mass index. Because hyperemic shear and resting baseline diameter can affect FMD response, we used four additional approaches for FMD: 1) we included baseline diameter as a covariate in the linear model, 2) we normalized FMD to SRauc as a dependent variable 3) we normalized FMD to SRauc as a dependent variable in addition to including baseline diameter as a covariate, and 4) we adjusted for allometrically scaled baseline diameter using a linear model with diameter change expressed in the natural log as a dependent variable and baseline diameter expressed in the natural log as a covariate.41 To further inform our results about FMD, we also assessed the relationship between baseline diameter and FMD. To corroborate the strength of relationships between sleep efficiency and CV variables, we conducted Pearson’s correlations. We did not adjust p-values for bivariate correlations because these CV variables are correlated with each other. To test if our results were affected by the presence of moderate- severe sleep apnea, we separately ran the analysis including only those people (apnea-hypopnea index < 15/hour, n = 19).
Finally, using the entire dataset, we ran an additional model by adding sex as a group variable and sleep efficiency × sex as an interaction term to explore sex differences. Analyses were performed using StataIC 14 (StataCorp LLC, College Station, TX, USA), and statistical significance was set at p<0.05.
Results
We studied 32 individuals (20 Males, 12 Females). Two male participants were identified as outliers for their apnea–hypopnea index and heart rate levels, respectively, and were removed prior to statistical analysis. Thus, the final sample size was 30 participants (18 Males, 12 Females; Table 1). Of the 12 females, 6 were perimenopausal, 3 were postmenopausal, 1 had an endometrial ablation, 1 had a hysterectomy, and 1 had an intrauterine device. Women were not on oral birth control medications. All perimenopausal women were studied in the follicular phase of their menstrual cycle. The ethnic breakdown included 27 people self-identifying as not Hispanic or Latino, 1 Hispanic or Latino, and 2 declined to provide an answer. The racial breakdown included 26 people self-identifying as White, 1 Black or African American, 1 American Indian or Alaskan Native and Black or African American, 1 Asian and White, and 1 identifying as other.
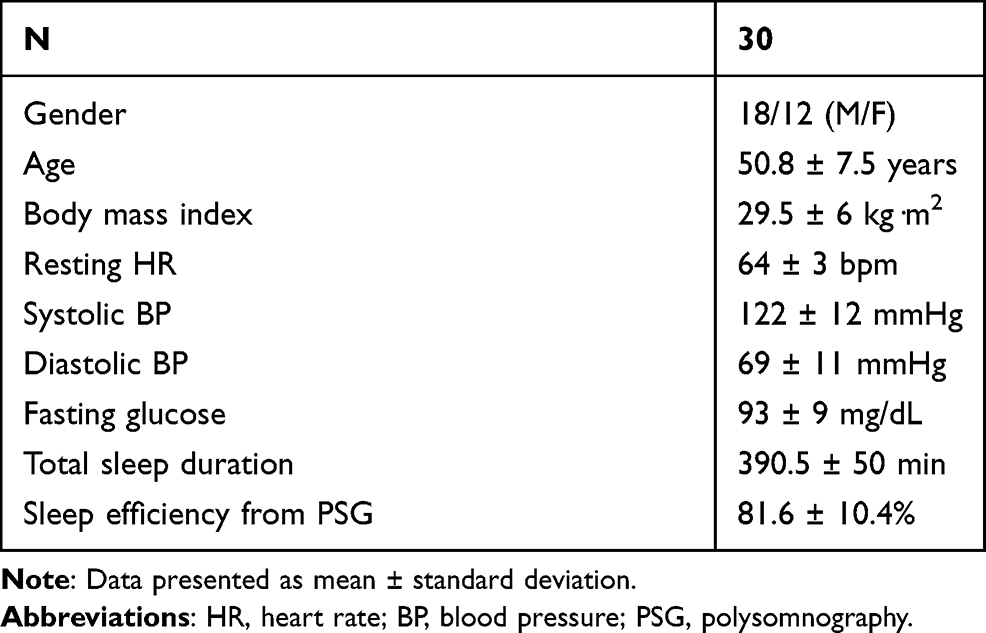 |
Table 1 Baseline Participant Information |
There were no differences between people with and without moderate-severe OSA (Table 2).
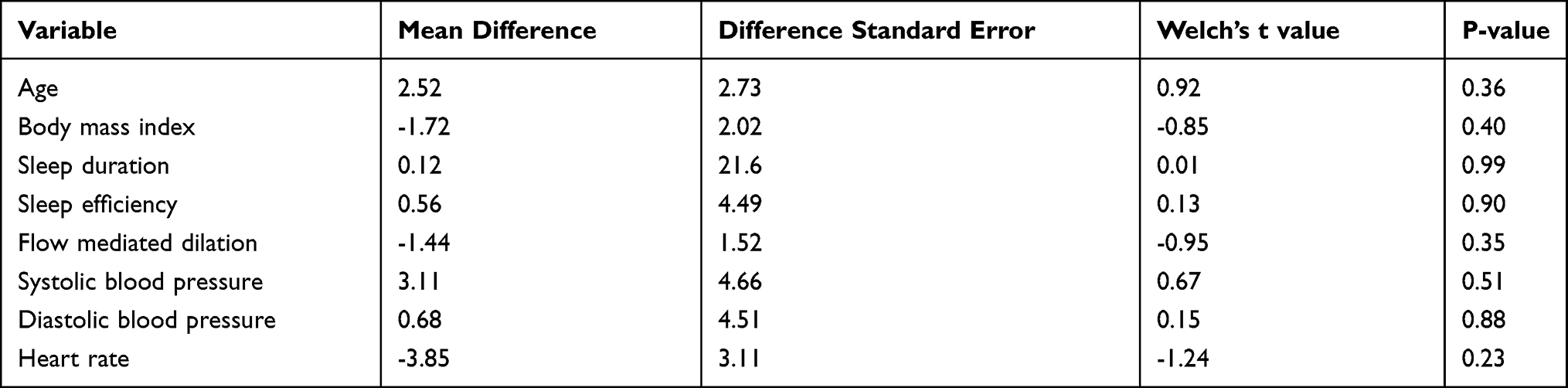 |
Table 2 Differences Between People with and without Moderate-Severe Obstructive Sleep Apnea |
Sleep Efficiency and CV Outcomes
Overnight sleep efficiency significantly predicted baseline diameter (t = 3.04, p = 0.005), such that for every percent decrease in sleep efficiency, baseline diameter increased by 0.04 mm (Figure 2). Sleep efficiency did not predict FMD regardless of how it was calculated: FMD without adjusting for baseline diameter (t = 1.72, p = 0.099), FMD normalized to SRauc(t = 1.13, p = 0.27), FMD adjusted for baseline diameter as a covariate (t = 0.82, p = 0.42), FMD adjusted for shear rate and baseline diameter (t = 1.09, p = 0.29), or FMD using allometric scaling of baseline diameter (t = 0.96, p = 0.35). It also did not predict HR (t = −0.09, p=0.9). SBP (t = −2.66, p=0.013) and DBP (t=−2.59, p = 0.016), were significantly predicted by overnight sleep efficiency (Figure 3). SBP and DBP increased by 0.6 mmHg for every percent decrease in sleep efficiency.
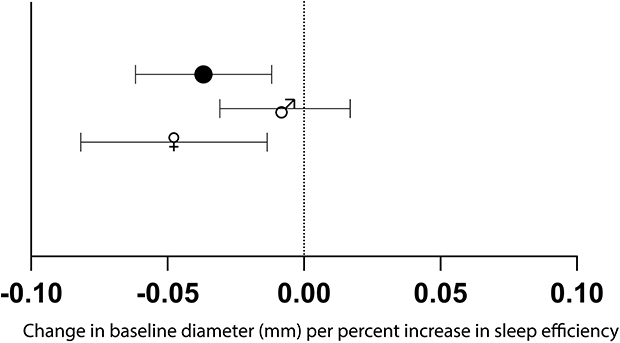 |
Figure 2 Forest plots (with 95% CI) of sleep efficiency versus baseline diameter in the entire sample (●), men (♂), women (♀). The x-axis shows the marginal effects’ coefficient for baseline diameter. The overall significant relationship between sleep efficiency and baseline diameter appears to be driven by females. |
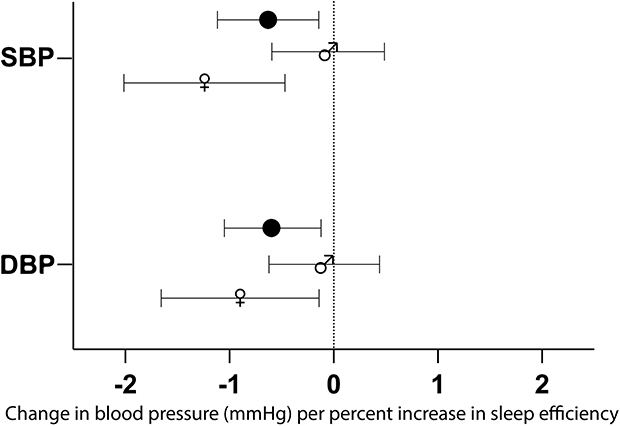 |
Figure 3 Forest plots (with 95% CI) of sleep efficiency versus systolic (SBP) and diastolic (DBP) blood pressure in the entire sample (●), men (♂), women (♀). The x-axis shows the marginal effects’ coefficients for blood pressure. The overall significant relationship between sleep efficiency and blood pressure appears to be driven by females. |
In Pearson correlations, sleep efficiency was significantly correlated with baseline diameter (r = −0.52, p=0.004), SBP (r = −0.43, p=0.017), and DBP (r = −0.43, p = 0.019) (Figure 4), but not with HR (r = −0.05, p = 0.79), or FMD (r = 0.3, p = 0.13). FMD was not significantly correlated with baseline diameter (r = −0.37, p = 0.06).
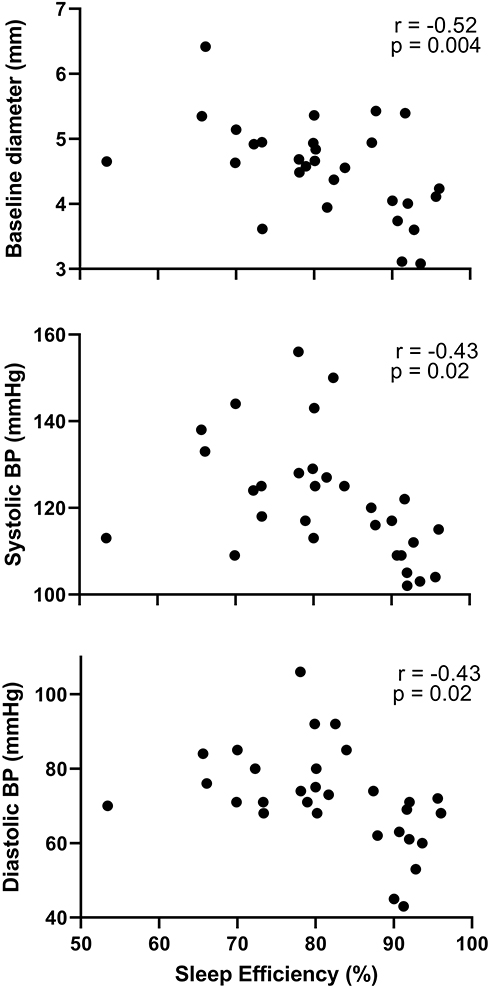 |
Figure 4 Pearson’s correlation between sleep efficiency and baseline diameter, and systolic and diastolic BP. |
Sleep Efficiency and CV Outcomes in People without Untreated Moderate-Severe Sleep Apnea (n = 19)
Overnight sleep efficiency significantly predicted baseline diameter (t = −2.82, p = 0.01). For every percent decrease in sleep efficiency, baseline diameter increased by 0.05 mm. Sleep efficiency did not predict FMD regardless of how it was calculated: FMD without adjusting for baseline diameter (t = 1.51, p = 0.16), FMD normalized to SRauc(t = 1.59, p = 1.4), FMD adjusted for baseline diameter as a covariate (t = 0.89, p = 0.39), FMD adjusted for shear rate and baseline diameter (t = 1.51, p=0.16), or FMD using allometric scaling of baseline diameter (t = 0.93, p = 0.37). SBP (t = −2.75, p=0.015) and DBP (t = −2.21, p = 0.04), but not HR (t = −0.88, p = 0.4) were significantly predicted by overnight sleep efficiency. For every percent increase in sleep efficiency, SBP increased by 1 mmHg and DBP increased by 0.9 mmHg.
Sleep efficiency was significantly correlated with baseline diameter (r=−0.60, p=0.007), SBP (r=−0.53, p=0.019), DBP (r=−0.46, p=0.049), but not with HR (r=−0.06, p=0.8), or FMD (r=0.34, p=0.18).
Sex Difference Analyses
There was a non-significant trend for an interaction between sex and sleep efficiency (t = −1.9, p = 0.07) such that overnight sleep efficiency significantly predicted baseline diameter in women (z=−2.74, p=0.006), but not men (z=−0.58, p=0.6) (Figure 2). Similarly, we discovered a significant interaction between sex and sleep efficiency for SBP (t=−2.82, p=0.01) and DBP (t=−2.07, p=0.049). BP was inversely associated with overnight sleep efficiency in women (SBP: z=−3.6, p < 0.001; DBP: z=−2.78, p=0.005), but these relationships were not significant in men for SBP (z=−0.19, p=0.85) or DBP (z=−0.33, p=0.74) (Figure 3). The interactions between sex and sleep efficiency were not significant for FMD (p=0.19), or HR (p=0.31).
Discussion
Sleep disturbance is known to be associated with increased cardiovascular risk, with impaired peripheral vascular function suggested as an underlying mechanism.42 We discovered that in midlife adults, while controlling for the effects of circadian rhythms, polysomnographically recorded overnight sleep efficiency is negatively associated with baseline brachial artery diameter, SBP, and DBP, but not HR or FMD. Importantly, these relationships remained when analyzed using correlation analyses. Lastly, exploratory analyses suggest that these relationships between sleep efficiency and morning cardiovascular risk markers in our sample are driven by associations amongst women but not men.
Sleep Efficiency and Baseline Diameter
Our study population’s baseline brachial artery diameter (mean 4.5 mm) is within the normative ranges for midlife adults.43 Furthermore, the median sleep efficiency in our sample was 81%. Based on our results, a 5% decrease in sleep efficiency could lead to a 0.2 mm increase in baseline brachial artery diameter. Baseline brachial artery diameter is directly associated with increased cardiovascular risk, specifically decreasing cardiovascular event-free survival by 15% for each 1 mm increase in baseline diameter.23–26 It has previously been shown that an increase in brachial artery diameter is likely a homeostatic and adaptive process to maintain vascular shear in the presence of cardiovascular risk factors.43 It can also be a maladaptive process in the face of aging.43 Additionally, our participants were devoid of any overt chronic disease (except sleep apnea), but because this was a midlife sample, we cannot exclude the presence of subclinical cardiovascular disease, especially because disorders such as obstructive sleep apnea can accelerate vascular aging.44 Still, our results persisted after controlling for the apnea–hypopnea index. One person had a surprisingly low sleep efficiency (53%) that could be due to sleep apnea (AHI=22.9/h) or a first night effect.45,46 The contribution of this individual was tested in a sensitivity analysis. Excluding this participant did not affect the pattern of results, and indeed, the correlations were strengthened (baseline diameter r = −0.58, SBP r = −0.58, DBP r = −0.52).
Discussion of potential mechanisms is speculative at this point, and more experimental work needs to be done in a larger sample to reproduce these findings. It is unlikely that one night of low sleep efficiency may change baseline brachial artery diameter. Indeed, we showed in a previous study that baseline morning brachial artery diameter does not differ depending on whether participants slept or stayed awake through the preceding night.20 However, sleep timing in the current study was selected based on our participants’ habitual sleeping behaviors, and thus we would hypothesize that our observations may be indicative of a chronic sleep phenotype. Poor sleep efficiency and increased resting baseline diameter may be parts of increased cardiovascular risk composition.
Sleep Efficiency and Blood Pressure
We found that sleep efficiency is inversely related to SBP and DBP measured soon after awakening. Although this is a statistical association and not a proven mechanistic link, our data suggest that for every 5% decline in sleep efficiency, one can expect both SBP and DBP to be 3 mmHg higher. Such a sleep-related increase in morning BP along with the commonly observed morning surge in BP can significantly increase the risk of adverse CV events in midlife adults, especially if they have underlying CV disease such as hypertension.47,48 Our blood pressure results are similar to the previous epidemiological association between actigraphy-measured sleep parameters and blood pressure from the CARDIA study in midlife adults.49 After examining polysomnography reports, we noticed that 4/30 participants were already awake before the mild auditory stimulus. To account for the morning BP surge timing,50 we adjusted for the duration of awakening in an additional model, and our statistical inferences were the same.
Sleep Efficiency and FMD
We did not find a significant relationship between sleep efficiency and FMD. In that regard, our results are similar to those of Scott and colleagues and Aggarwal and colleagues, who also found that low sleep efficiency and quality, respectively, did not impair FMD.12,13 Furthermore, we normalized FMD to hyperemic shear to account for any shear-related differences and controlled for the effects of baseline diameter as a covariate and using allometric scaling, and our results remained the same. These adjustments did not change the results likely due to the non-significant inverse relationship between FMD and baseline diameter. Nonetheless, given our lack of a priori power analyses, this non-significant finding should be interpreted with caution.
Morning Cardiovascular Risk
Major adverse cardiovascular events occur most commonly in the morning, and several cardiovascular risk variables have a morning peak driven by the circadian system.51 All our measurements were made during this cardiovascular risk window. A combination of poor sleep-quality driven increases in blood pressure, circadian driven increases in cardiovascular risk markers, and blood pressure increases due to typical morning behaviors could potentially increase the risk of a severe adverse cardiovascular event in people with existing CV risk.51
Sex-Differences
There are well-known sex-difference in cardiovascular disease, yet the differential mechanisms in men and women are not well understood.33 Our exploratory analyses suggest that the significant relationship between sleep efficiency and cardiovascular risk markers, including baseline diameter, and SBP and DBP, is driven by women and not men. These findings may have important implications, considering the known sex differences in CV disease and sleep across the lifespan.33,52,53 During midlife, close to peri- and post-menopause, sleep quality deteriorates, whereas cardiovascular risk increases abruptly in women compared to prior decades.54,55 Sleep restriction increases sleep efficiency and is a commonly prescribed treatment for insomnia, which is common in women with the onset of menopause.53,56,57 Our results suggest that theoretically, such behavioral treatments that improve sleep efficiency could also improve cardiovascular health in midlife by reducing blood pressure and leading to adaptations in the vasculature, which should be further assessed. On the other hand, such treatments do not necessarily increase sleep duration, so the effects of increasing sleep efficiency vs sleep duration could be tested on CV parameters.
Strength and Limitations
Our use of tightly controlled outpatient and in-laboratory procedures present several strengths and limitations to be considered. We included people with untreated sleep apnea as this syndrome is common in the general population.29,30 Yet, there were no significant differences between people with and without moderate to severe sleep apnea. Our results for the relationship between overnight sleep efficiency and morning CV risk markers held even after excluding people with moderate-severe sleep apnea suggesting that the results were independent of apnea status. We studied midlife (mean age 51 years) and overweight (mean BMI 29.5 kg/m2) adults who are likely at a higher risk for cardiovascular disease than the younger population previously studied to answer this question. Our participants were in bed for an 8 h sleep opportunity at habitual timing in a light-controlled environment, thereby avoiding any changes in circadian timing of the sleep episode that could disrupt sleep.58 However, we cannot discount the wake-promoting system’s overactivity due to the first-night effect due to sleeping in a new environment,45,46 or the effect on sleep efficiency due to limiting the time in bed to 8 h. Future studies need to account for these limitations. We measured sleep via polysomnography and made measurements immediately upon awakening, which advances previous investigations in this area12,13 especially due to the adequate experimental control of circadian effects. We cannot infer causality and could not examine mechanisms underlying the relationship between sleep efficiency and CV markers, which are limitations. Since these data were collected as part of multi-day circadian protocols requiring data collection across the day and the night, it was not possible to have a single sonographer make all measurements. Staffing for these studies was variable to avoid systemic effects. The sonographer training in our laboratory consists of individualized hands-on training and the collection of at least 20 full FMD images under the supervision of an experienced operator. Formal feedback is provided after each set of 5 images. Subsequently, new operators are required to acquire at least an additional 10 (5 consecutive) polished images verified by an expert. For continued practice, all operators make approximately 100 measurements each year. For analysis, the intra-class correlation between analyzers needs to be ≥0.9. Our rigorous selection of participants, self-selected strict at-home sleep routine before the in-laboratory visit, excellent experimental control all considerably strengthen the confidence in our findings. Properly powered studies using at least two nights of polysomnography (to account for a first night effect) are perhaps essential to conclusively assess the relationship between sleep efficiency and FMD.
In conclusion, we discovered that in midlife adults, overnight sleep efficiency is inversely associated with baseline brachial artery diameter and SBP and DBP, but not FMD or HR. These associations were driven by a significant effect in women, but not in men. Future studies in people with existing cardiovascular risk are warranted to understand the clinical significance of these findings. If these findings persist in adults with existing cardiovascular disease, disturbed sleep could be implicated as a mechanism in the morning increase in adverse cardiovascular events.
Acknowledgments
We thank volunteer participants for their time and efforts. We thank Mr Noal Clemons for study management and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by NIH grants R01 HL125893, R35 HL155681, R21 HL140377, F32 HL131308, KL2 TR002370, K01 HL146992, UL1TR000128, National Space Biomedical Research Institute through NCC 9-58, and Medical Research Foundation of Oregon, and the Oregon Institute of Occupational Health Sciences at Oregon Health & Science University via funds from the Division of Consumer and Business Services of the State of Oregon (ORS 656.630).
Disclosure
Dr Saurabh S Thosar reports a patent 9750481 issued to Indiana University.
Dr Steven A Shea reports grants from NIH, during the conduct of the study. No conflicts of interest, financial or otherwise, are declared by the authors.
References
1. Grandner MA, Alfonso-Miller P, Fernandez-Mendoza J, Shetty S, Shenoy S, Combs D. Sleep: important considerations for the prevention of cardiovascular disease. Curr Opin Cardiol. 2016;31(5):551. doi:10.1097/HCO.0000000000000324
2. Daghlas I, Dashti HS, Lane J, et al. Sleep duration and myocardial infarction. J Am Coll Cardiol. 2019;74(10):1304–1314. doi:10.1016/j.jacc.2019.07.022
3. Krittanawong C, Kumar A, Wang Z, et al. Sleep duration and cardiovascular health in a representative community population (from NHANES, 2005 to 2016). Am J Cardiol. 2020;127:149–155. doi:10.1016/j.amjcard.2020.04.012
4. Massar SA, Liu JC, Mohammad NB, Chee MW. Poor habitual sleep efficiency is associated with increased cardiovascular and cortisol stress reactivity in men. Psychoneuroendocrinology. 2017;81:151–156. doi:10.1016/j.psyneuen.2017.04.013
5. Kadoya M, Koyama H, Kurajoh M, et al. Sleep, cardiac autonomic function, and carotid atherosclerosis in patients with cardiovascular risks: HSCAA study. Atherosclerosis. 2015;238(2):409–414. doi:10.1016/j.atherosclerosis.2014.12.032
6. Hirata T, Nakamura T, Kogure M, et al. Reduced sleep efficiency, measured using an objective device, was related to an increased prevalence of home hypertension in Japanese adults. Hypertens Res. 2020;43(1):23–29. doi:10.1038/s41440-019-0329-0
7. Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren W. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34(11):1487–1492. doi:10.5665/sleep.1382
8. Yan B, Yang J, Zhao B, Fan Y, Wang W, Ma X. Objective sleep efficiency predicts cardiovascular disease in a community population: the sleep heart health study. J Am Heart Assoc. 2021;10(7):e016201. doi:10.1161/JAHA.120.016201
9. Ras RT, Streppel MT, Draijer R, Zock PL. Flow-mediated dilation and cardiovascular risk prediction: a systematic review with meta-analysis. Int J Cardiol. 2013;168(1):344–351. doi:10.1016/j.ijcard.2012.09.047
10. Inaba Y, Chen JA, Bergmann SR. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: a meta-analysis. Int J Cardiovasc Imaging. 2010;26(6):631–640. doi:10.1007/s10554-010-9616-1
11. Shechter M, Issachar A, Marai I, et al. Long-term association of brachial artery flow-mediated vasodilation and cardiovascular events in middle-aged subjects with no apparent heart disease. Int J Cardiol. 2009;134(1):52–58. doi:10.1016/j.ijcard.2008.01.021
12. Aggarwal B, Makarem N, Shah R, et al. Effects of inadequate sleep on blood pressure and endothelial inflammation in women: findings from the American Heart Association go red for women strategically focused research network. J Am Heart Assoc. 2018;7(12):e008590. doi:10.1161/JAHA.118.008590
13. Scott MC, Hogwood AC, Fralin RC, Weggen JB, Zúñiga TM, Garten RS. Low sleep efficiency does not impact upper or lower limb vascular function in young adults. Exp Physiol. 2020;105(8):1373–1383. doi:10.1113/EP088658
14. Cooper DC, Ziegler MG, Milic MS, et al. Endothelial function and sleep: associations of flow‐mediated dilation with perceived sleep quality and rapid eye movement (REM) sleep. J Sleep Res. 2014;23(1):84–93. doi:10.1111/jsr.12083
15. Hill LK, Wu JQ, Hinderliter AL, Blumenthal JA, Sherwood A. Actigraphy-derived sleep efficiency is associated with endothelial function in men and women with untreated hypertension. Am J Hypertens. 2021;34(2):207–211. doi:10.1093/ajh/hpaa167
16. King CR, Knutson KL, Rathouz PJ, Sidney S, Liu K, Lauderdale DS. Short sleep duration and incident coronary artery calcification. JAMA. 2008;300(24):2859–2866.
17. de Souza L, Benedito-Silva AA, Pires MLN, Poyares D, Tufik S, Calil HM. Further validation of actigraphy for sleep studies. Sleep. 2003;26(1):81–85. doi:10.1093/sleep/26.1.81
18. Otto ME, Svatikova A, de Mattos Barretto RB, et al. Early morning attenuation of endothelial function in healthy humans. Circulation. 2004;109(21):2507–2510. doi:10.1161/01.CIR.0000128207.26863.C4
19. Thosar S, Berman A, Herzig M, et al. Circadian rhythm of vascular function in midlife adults. Arterioscler Thromb Vasc Biol. 2019;39(6):1203–1211. doi:10.1161/ATVBAHA.119.312682
20. Thosar SS, Berman AM, Herzig MX, Roberts SA, Lasarev MR, Shea SA. Morning impairment in vascular function is unrelated to overnight sleep or the inactivity that accompanies sleep. Am J Physiol Regul, Integr Comp Physiol. 2018;315(5):R986–R993. doi:10.1152/ajpregu.00143.2018
21. Muller JE, Stone PH, Turi ZG, et al. Circadian variation in the frequency of onset of acute myocardial infarction. New Engl J Med. 1985;313(21):1315–1322. doi:10.1056/NEJM198511213132103
22. Muller JE, Ludmer PL, Willich SN, et al. Circadian variation in the frequency of sudden cardiac death. Circulation. 1987;75(1):131–138. doi:10.1161/01.CIR.75.1.131
23. Yeboah J, Crouse JR, Burke GL, Hsu F-C, Herrington DM. Flow-mediated dilation of brachial artery predicts incident cardiovascular events in older adults (cardiovascular health study). Am Heart Assoc. 2006;10:840.
24. Laclaustra M, Frangi AF, Frangi AG, Casasnovas JA, Cia P. Association of endothelial function and vascular data with LDL-c and HDL-c in a homogeneous population of middle-aged, healthy military men: evidence for a critical role of optimal lipid levels. Int J Cardiol. 2008;125(3):376–382. doi:10.1016/j.ijcard.2007.03.001
25. Maruhashi T, Soga J, Fujimura N, et al. Brachial artery diameter as a marker for cardiovascular risk assessment: FMD-J study. Atherosclerosis. 2018;268:92–98. doi:10.1016/j.atherosclerosis.2017.11.022
26. Holewijn S, Den Heijer M, Swinkels DW, Stalenhoef AF, De Graaf J. Brachial artery diameter is related to cardiovascular risk factors and intima‐media thickness. Eur J Clin Invest. 2009;39(7):554–560. doi:10.1111/j.1365-2362.2009.02152.x
27. North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. 2012;110(8):1097–1108. doi:10.1161/CIRCRESAHA.111.246876
28. Ip MS, Tse H-F, Lam B, Tsang KW, Lam W-K. Endothelial function in obstructive sleep apnea and response to treatment. Am J Respir Crit Care Med. 2004;169(3):348–353. doi:10.1164/rccm.200306-767OC
29. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81. doi:10.1016/j.smrv.2016.07.002
30. Garvey JF, Pengo MF, Drakatos P, Kent BD. Epidemiological aspects of obstructive sleep apnea. J Thorac Dis. 2015;7(5):920.
31. Lattanzi S, Brigo F, Silvestrini M. Sleep and blood pressure. J Clin Hypertens. 2018;20(12):1721–1723. doi:10.1111/jch.13423
32. Lattanzi S, Brigo F, Silvestrini M. Obstructive sleep apnea syndrome and the nocturnal blood pressure profile. J Clin Hypertens. 2018;20(6):1036–1038. doi:10.1111/jch.13316
33. Regitz-Zagrosek V, Kararigas G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol Rev. 2017;97(1):1–37. doi:10.1152/physrev.00021.2015
34. Thosar SS, Rueda JF, Berman AM, et al. Separate and interacting effects of the endogenous circadian system and behaviors on plasma aldosterone in humans. Am J Physiol Regul, Integr Comp Physiol. 2019;316(2):R157–R164. doi:10.1152/ajpregu.00314.2018
35. Iber C, Ancoli-Israel S, Chesson A, Quan SF. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Vol. 1. Westchester, IL: American Academy of Sleep Medicine; 2007.
36. Borow KM, Newburger JW. Noninvasive estimation of central aortic pressure using the oscillometric method for analyzing systemic artery pulsatile blood flow: comparative study of indirect systolic, diastolic, and mean brachial artery pressure with simultaneous direct ascending aortic pressure measurements. Am Heart J. 1982;103(5):879–886.
37. Thijssen DH, Black MA, Pyke KE, et al. Assessment of flow-mediated dilation in humans: a methodological and physiological guideline. Am J Physiol Heart Circulatory Physiol. 2011;300(1):H2–H12. doi:10.1152/ajpheart.00471.2010
38. Thosar SS, Wiggins CC, Shea SA, Wallace JP. Brachial artery endothelial function is stable across the morning in young men. Cardiovasc Ultrasound. 2015;13(1):1. doi:10.1186/s12947-015-0036-1
39. Thosar SS, Bielko SL, Mather KJ, Johnston JD, Wallace JP. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med Sci Sports Exerc. 2015;47(4):843–849. doi:10.1249/MSS.0000000000000479
40. Johnson BD, Mather KJ, Newcomer SC, Mickleborough TD, Wallace JP. Vitamin C prevents the acute decline of flow-mediated dilation after altered shear rate patterns. Appl Physiol, Nutr Metab. 2012;38(3):268–274. doi:10.1139/apnm-2012-0169
41. Atkinson G, Batterham AM. Allometric scaling of diameter change in the original flow-mediated dilation protocol. Atherosclerosis. 2013;226(2):425–427. doi:10.1016/j.atherosclerosis.2012.11.027
42. Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res. 2012;21(4):427–433. doi:10.1111/j.1365-2869.2011.00990.x
43. Chung WB, Hamburg NM, Holbrook M, et al. The brachial artery remodels to maintain local shear stress despite the presence of cardiovascular risk factors. Arterioscler Thromb Vasc Biol. 2009;29(4):606–612. doi:10.1161/ATVBAHA.108.181495
44. Yim-Yeh S, Rahangdale S, Nguyen ATD, et al. Obstructive sleep apnea and aging effects on macrovascular and microcirculatory function. Sleep. 2010;33(9):1177–1183. doi:10.1093/sleep/33.9.1177
45. Tamaki M, Nittono H, Hayashi M, Hori T. Examination of the first-night effect during the sleep-onset period. Sleep. 2005;28(2):195–202. doi:10.1093/sleep/28.2.195
46. Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26(3):342–392. doi:10.1093/sleep/26.3.342
47. Kario K, Shimada K, Pickering TG. Clinical implication of morning blood pressure surge in hypertension. J Cardiovasc Pharmacol. 2003;42:S87–S91. doi:10.1097/00005344-200312001-00019
48. Manfredini R, Boari B, Smolensky MH, et al. Circadian variation in stroke onset: identical temporal pattern in ischemic and hemorrhagic events. Chronobiol Int. 2005;22(3):417–453. doi:10.1081/CBI-200062927
49. Knutson KL, Van Cauter E, Rathouz PJ, et al. Association between sleep and blood pressure in midlife: the CARDIA sleep study. Arch Intern Med. 2009;169(11):1055–1061. doi:10.1001/archinternmed.2009.119
50. White WB. The risk of waking-up: impact of the morning surge in blood pressure. Am Heart Assoc. 2010;10:835–837.
51. Thosar SS, Shea SA. Circadian control of human cardiovascular function. Curr Opin Pharmacol. 2021;57:89–97. doi:10.1016/j.coph.2021.01.002
52. Mong JA, Cusmano DM. Sex differences in sleep: impact of biological sex and sex steroids. Philos. Trans. R Soc B Biol Sci. 2016;371(1688):20150110. doi:10.1098/rstb.2015.0110
53. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
54. Matthews KA, Wing RR, Kuller LH, Meilahn EN, Plantinga P. Influence of the perimenopause on cardiovascular risk factors and symptoms of middle-aged healthy women. Arch Intern Med. 1994;154(20):2349–2355. doi:10.1001/archinte.1994.00420200105011
55. Moreno-Frías C, Figueroa-Vega N, Malacara JM. Relationship of sleep alterations with perimenopausal and postmenopausal symptoms. Menopause. 2014;21(9):1017–1022. doi:10.1097/GME.0000000000000206
56. Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3(5 suppl):S7–S10. doi:10.5664/jcsm.26929
57. Maurer LF, Espie CA, Omlin X, et al. Isolating the role of time in bed restriction in the treatment of insomnia: a randomized, controlled, dismantling trial comparing sleep restriction therapy with time in bed regularization. Sleep. 2020;43(11):zsaa096. doi:10.1093/sleep/zsaa096
58. Dijk DJ, Czeisler CA. Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci Letters. 1994;166(1):63–68.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.