Back to Journals » Nature and Science of Sleep » Volume 13
Sleep Education for Elders Program (SLEEP): Promising Pilot Results of a Virtual, Health Educator-Led, Community-Delivered Sleep Behavior Change Intervention
Authors Tucker RM, Contreras DA, Carlson BR, Carter A, Drake CL ![]()
Received 27 January 2021
Accepted for publication 21 April 2021
Published 19 May 2021 Volume 2021:13 Pages 625—633
DOI https://doi.org/10.2147/NSS.S304035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Robin M Tucker,1 Dawn A Contreras,2 Breanne R Carlson,2 Anita Carter,2 Christopher L Drake3
1Department of Food Science and Human Nutrition, Michigan State University, East Lansing, MI, 48824, USA; 2Health and Nutrition Institute, Michigan State University Extension, Michigan State University, East Lansing, MI, 48824, USA; 3Division of Sleep Medicine, Henry Ford Health System, Detroit, MI, 48202, USA
Correspondence: Robin M Tucker
Department of Food Science and Human Nutrition, Michigan State University, 2110 S. Anthony Hall, 474 S. Shaw Ln, East Lansing, MI, 48824, USA
Tel +1-517-353-3408
Email [email protected]
Purpose: Sleep problems pose serious public health concerns, and evidence suggests that the problem is worsening. Both sufficient sleep quantity and quality are needed for optimal health, particularly among older adults, but access to sleep care can be difficult. This study examined the efficacy of a six-week sleep behavior change program designed for older adults that was delivered virtually by health educators.
Participants and Methods: This quasi-experimental pilot study (intervention n = 22; control n = 31) explored the effects of the Sleep Education for Elders Program (SLEEP) on sleep outcomes, which included: 1) sleep quality, measured by the Pittsburgh Sleep Quality Index (PSQI); 2) sleep duration, extracted from the PSQI; 3) insomnia symptoms, measured by the Insomnia Severity Index; 4) sleep hygiene behaviors, obtained from the Sleep Hygiene Index; and 5) excessive daytime sleepiness, measured by the Epworth Sleepiness Scale.
Results: After SLEEP, the intervention group experienced significantly improved sleep quality (p < 0.001), a reduction in maladaptive sleep hygiene behaviors (p = 0.007), and reduced daytime sleepiness (p < 0.027) compared to the control group. Effect sizes for all five sleep measures were medium or large. In the intervention group, all changes were judged to be clinically meaningful (≥ 0.5 SD) except for improvements in daytime sleepiness.
Conclusion: These data support the efficacy of a group-based, virtual behavior change intervention in improving sleep outcomes among older adults.
Keywords: insomnia, sleep hygiene, adult, public health, multidimensional sleep health
Introduction
The purpose of this pilot study was to test the hypothesis that a community-based, virtually delivered behavior change program – the SLeep Education for Elders Program (SLEEP) – would improve sleep outcomes among community-dwelling older adults with self-identified, but not necessarily diagnosed, sleep problems. SLEEP was designed to address sleep difficulties, which present a serious global public health problem. In developed countries, more than 1 in 3 adults1–4 frequently fail to achieve the recommended sleep duration of at least 7 h/night.5 Further, evidence suggests that the prevalence of sleep problems has worsened over time.6 Reasons for this change result from recent health, social, economic, and technological trends, including a global pandemic.6,7 While the effects of the recent pandemic and the related need for social distancing have been problematic for everyone, these requirements have been particularly deleterious for the quality of life and health of older adults.8,9 Insufficient and poor-quality sleep exacerbate health problems by increasing the risk and/or severity of dementia, obesity, type 2 diabetes, hypertension, cardiovascular disease, severe psychological distress, and mortality.10–14 Moreover, inadequate sleep compromises immune response, leaving older adults susceptible to infectious diseases.15 In the United States, poor sleep quality also nearly tripled the odds of entering skilled nursing care,16 and the odds of falling ranged from 1.5–4.5 times higher for older adults reporting poor or insufficient sleep.17,18 Given the widespread prevalence of and health care costs associated with sleep problems, interventions that are effective, affordable, and accessible are needed.
Cognitive Behavioral Therapy for Insomnia (CBTi) is considered the gold standard for treating insomnia.19,20 CBTi is a standardized approach to treating insomnia that includes sleep education, behavioral recommendations, and cognitive therapy to alter thinking patterns that interfere with sleep21 and is typically delivered in primary care or outpatient mental health facilities.22 Unfortunately, the number of patients needing care frequently exceeds CBTi-trained therapist availability.22,23 Another barrier to care, at least in the United States, is the avoidance of treatment due to concerns about costs, time constraints, and accessibility.24 Further, some individuals might believe that their sleep problems do not rise to the level of a diagnosable sleep condition, or some might feel that sleep is not an actionable priority; yet, they might still be dissatisfied with their sleep duration and quality.25,26 Fortunately, evidence-based sleep behavior change training has been shown to be effective in addressing sleep problems for many individuals,19,26–31 even without all of the components of CBTi.19,26
As telemedicine continues to increase in availability and popularity,32 virtual delivery of health education and behavior change programming has also increased, but the effectiveness of this delivery modality remains largely under-characterized.19,33,34 There is evidence to support the use of internet-delivered CBTi,22 but less is known about the effectiveness of virtual, group-based, non-CBTi sleep programming targeted to community-dwelling older adults as evidenced by the limited number of published studies in this population.35–37 Further work is needed to confirm and expand on the potential benefits of virtual sleep behavior change interventions for older adults. To address these gaps in the literature, the SLEEP program was developed and tested.
Materials and Methods
Program Background and Theoretical Foundations
SLEEP was developed by sleep researchers, a certified sleep medicine specialist, Michigan State University (MSU) Extension educators, and older adults living in the community. A total of 6, 30-minute sessions were created; topics for sleep in order by session included: introduction to sleep and health with a focus on recommended duration guidelines; sleep hygiene best practices, Stimulus Control Therapy, mindfulness and relaxation, relationships between sleep and physical activity, and sleep myths.
Each session was led by a facilitator and co-facilitator who had received training on the program. Each session, except for the first, started with a discussion of successes and barriers regarding achieving the previous week’s goal. After experiences were shared, a 3-minute video was shown to the group. This video covered the information related to the topic for that week and served as a means to ensure that program fidelity is maintained. After viewing the video, the facilitator led the discussion of the video following a provided script. Educational points were emphasized by the facilitator. Participants were then asked to develop a goal for the following week based on the material covered that week. Participants wrote and verbally stated a specific goal they wanted to achieve based on the information learned in the program. The goals were structured to include what, when, how long, and how often the participant would perform the desired action in the next week. Examples of goals selected by participants included going to bed and getting up at the same time for three days in a row, removing technology from the bedroom, or using relaxation techniques to help quickly return to sleep after waking. Participants were asked to rate their confidence level of achieving the goal on a scale from 1 (not at all confident) to 10 (completely confident). If the participant’s rating was below 7, they were asked to brainstorm ways to increase their confidence level to a rating of at least 7. The following week, participants reported back to the group on how well they achieved their goal. Participants could indicate that they fully met the goal, partially met the goal, or did not meet the goal. Those whose goals were not met were assisted by the group and facilitator with problem-solving possible solutions, and participants were reminded that not all behaviors or recommendations would pertain to or work for them. Instead, they were encouraged to view the 6-week period as an opportunity for discovery in order to identify approaches that worked for them personally.
The topics covered in the SLEEP curriculum were selected both due to their effectiveness in improving sleep outcomes and with consideration about how health educators who were not sleep experts could effectively deliver the information in the short timeframe available. For example, basic concepts related to sleep hygiene were shared because sleep hygiene practices are recommended to improve sleep quality.38 Topics included: going to bed only when tired, getting out of bed if unable to fall asleep, maintaining consistent bed and wake times, using the bedroom only for sleep or sexual activity, avoiding alcohol, avoiding blue light, etc. Stimulus Control Therapy (SCT) principles were emphasized as SCT has been shown to increase sleep duration.27 Relaxation and mindfulness techniques were shared to assist with both initially falling asleep as well as returning to sleep. Relaxation training is a proven intervention for improving sleep duration and quality.26 The relationships between exercise and sleep were explained. Exercise has been shown to improve sleep quality and reduce the time needed to fall asleep.39 Low-intensity exercises, like tai chi40 and yoga,41 have both been shown to be effective in aiding sleep in an older adult population. Sleep Restriction Therapy (SRT) was considered for inclusion due to its inclusion as part of CBTi and its effectiveness as a monotherapy in improving select sleep outcomes.37 However, due to the limited time available to educate on the topic, the duration of the program, the lack of personalized interaction, and the concern that participants might over-restrict their sleep time, SRT was not included.
Theoretical frameworks for SLEEP included the Health Belief Model42 and Social Cognitive Theory.43 These approaches shaped which material was covered and how the sessions were structured. For example, the consequences of poor sleep were explained during the first session while the benefits and barriers to changes were discussed by the group at each session. Each session involved setting a goal for the following week, and beliefs regarding self-efficacy in achieving the goal were assessed. Participants who had experienced success in meeting their goal were able to model positive behavior for the rest of the group.
Recruitment
Recruitment was accomplished by inviting individuals who self-identified as having sleep problems and had previously enrolled in MSU Extension programming to participate. The intervention group participants were available during the class times; whereas, the control group participants were not, making this a quasi-experimental study design as randomization did not occur. The control group received no intervention between baseline and follow-up. A total of 78 participants gave consent to participate in the study.
Measures
All participant data were collected online using the Qualtrics survey platform (Qualtrics, Provo, UT, USA). Questions about participant characteristics were asked in order to describe the populations. Sex, age, and race were collected. Self-reported height and weight were used to calculate body mass index (BMI). Participants were asked if they had a diagnosed sleep problem or self-identified insomnia.
Validated surveys were used to assess program effectiveness on sleep outcomes. The Pittsburgh Sleep Quality Index (PSQI) measures perceived sleep quality over the past month, and also asks about sleep duration.44 Sleep duration was extracted from the PSQI.45–47 Scores range from 0–21, and scores ≥5 indicate poor sleep quality. The Insomnia Severity Index (ISI) measures perceived nocturnal and diurnal insomnia symptoms over the past two weeks.48 Scores range from 0–28. Scores of 0–7 suggest no clinically significant insomnia; scores 8–14 suggest insomnia symptoms of mild to moderate severity; scores 15–21 indicate moderate insomnia severity; and scores 22–28 indicate severe insomnia symptoms with daytime impairment.48 The Sleep Hygiene Index (SHI) is comprised of 13 statements that describe behaviors that are not conducive to sleep, like napping more than 2 hours a day or doing important work in the bedroom.49 Possible responses include never, rarely, sometimes, frequently, or always. Scores range from 0–52; higher scores suggest poorer sleep hygiene practices. The Epworth Sleepiness Scale (ESS) evaluated daytime sleepiness.50 Scores range from 0–24. Per the ESS manual, scores of 0–5 indicate lower normal daytime sleepiness, scores of 6–10 indicate higher normal daytime sleepiness; scores of 11–12 indicate mild excessive daytime sleepiness; scores of 13–15 suggest moderate excessive daytime sleepiness; scores of 16–24 suggest severe excessive daytime sleepiness.
In addition to the validated surveys, open-ended questions about program satisfaction and behavior changes were asked. These questions were designed to capture feedback from participants and to identify the recommendations participants felt were especially effective. Participants were also asked if they felt they would be able to maintain these changes over the next six months.
Statistical Analysis
Data were analyzed using IBM SPSS Version 26 (IBM Corporation, Armonk, New York). Normality was assessed using Shapiro–Wilk tests and pre-post-test results for continuous data were assessed using independent t-tests or Mann–Whitney U-tests where appropriate. Chi-square tests for homogeneity were used to assess differences in the distribution of categorical variables between intervention and control groups. Significance was set at alpha <0.05. Corrections for multiple comparisons were not performed given the exploratory nature of the study;51 however, between group effect sizes (Cohen’s d) are presented in order to provide context to significance testing.52 These effect sizes were calculated using G*Power 3.1.53 Given that this was a pilot study, in order to avoid inadvertent inflation of effect sizes,54 covariates were not used in any analysis. Clinical relevance was assessed using the method put forth by Norman et al55 who suggest that a change of at least 0.5 SD represents meaningful and perceptible change to most patients. This analysis is presented in the text. Means and standard deviations (SD) are presented.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Michigan State University Human Research Protection Program (STUDY00003748), East Lansing, MI. Participants provided informed consent after the primary investigator explained the study. Participants were awarded a $10 gift card for completing both surveys.
Results
Participant Characteristics
Among the intervention group, 24 participants consented, and 23 (95.8%) completed testing; however, 1 participant only attended 1 class, so those responses were not analyzed. The total sample size for the intervention group was 22, and all participants attended at least 2 of the 6 classes. Among control group participants, 54 enrolled and 31 (57.4%) completed testing.
Demographic data are shown in Table 1. The study population was predominantly female, White, and obese; there were no differences between groups at baseline among these factors. The two groups differed in terms of age (P < 0.001), with the control group significantly younger than the intervention group, but the number of people suffering from self-described sleep problems did not differ between groups. Relevant sleep measures did not differ between groups at baseline (P > 0.076 for all; Table 2). Comparisons were made between participants in the control group who completed testing and those who were lost to follow-up. At baseline, participants in the control group who completed the follow-up survey had worse ISI (13.4 ± 5.2 vs 8.8 ± 4.1, p = 0.001) and PSQI scores (10.0 ± 3.4 vs 7.5 ± 2.5, p = 0.004) compared to those lost to follow-up. However, an additional baseline comparison between the intervention group and the entire control group (completers plus those lost to follow-up) also revealed no differences in baseline sleep measures.
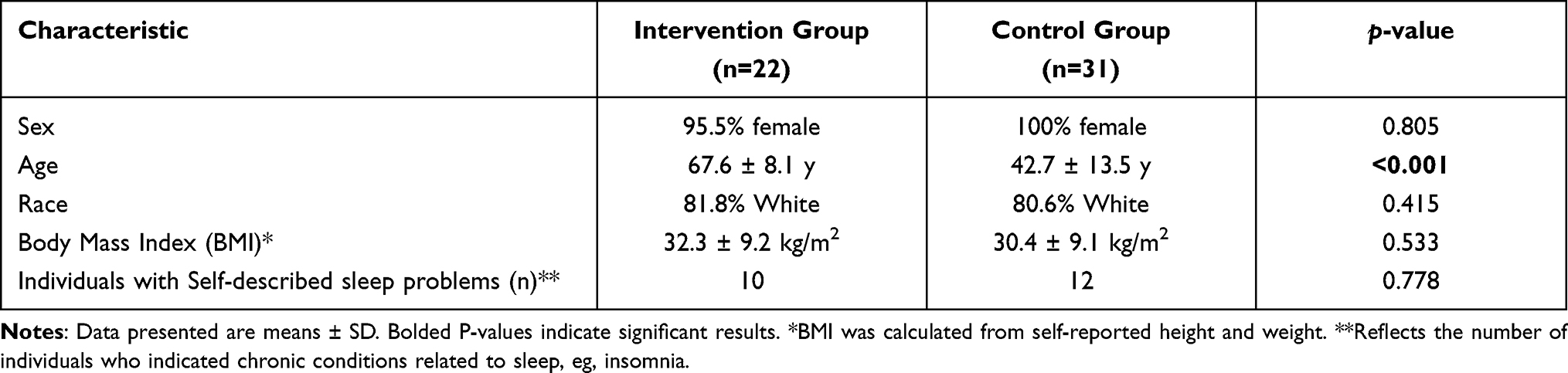 |
Table 1 Baseline Characteristics by Group |
 |
Table 2 Baseline Sleep Measures by Group |
Post-Program Comparisons Between SLEEP Intervention and Control Groups
Compared to the control group, the SLEEP intervention group experienced significant improvements in sleep quality, sleep behaviors, and daytime sleepiness (Table 3; P ≤ 0.027 for all). Between group effect sizes for all sleep measures were medium to large (Table 3).
 |
Table 3 Follow-Up Sleep Measures by Group |
Clinical Relevance of Changes Within the SLEEP Intervention Group
Based on the work of Norman et al55 which proposes clinical relevance in health-related quality of life outcomes occurs when changes meet or exceed one-half of the baseline standard deviation, clinical relevance was assessed for the intervention group (Table 4). All outcomes except daytime sleepiness met or exceeded the 0.5 SD criterion. For the control group, none of the changes between baseline and follow-up testing met or exceeded the 0.5 SD cut-off (data not shown).
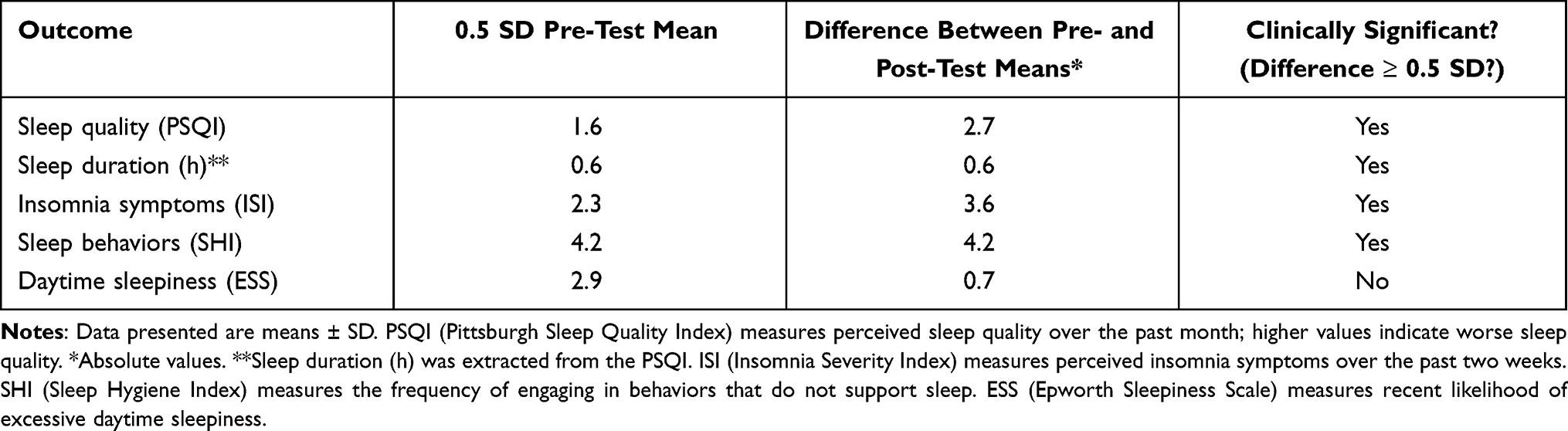 |
Table 4 Clinical Relevance Based on 0.5 SD Difference Criterion for the Intervention Group |
Popular Behavior Changes
The most salient changes in behavior by the intervention group involved maintaining a regular sleep schedule and using relaxation techniques to fall or return to sleep. These changes were mentioned by 72.7% (n=16) of participants. When asked how likely they were to maintain sleep-related changes over the next 6 months, 95.5% (n=21) said they were either extremely likely (54.5%; n=12) or moderately likely (40.9%, n=9) to maintain changes. Participants were also asked if they would recommend the program to friends and family, and 95.5% (n=21) answered yes. Feedback from the one participant who did not recommend the program centered around disliking the discussion-based format.
Qualitative Program Feedback
Examples of open-ended feedback included the following comments. “I took the class and was very impressed. Many suggestions have been taken to heart and gave me thoughtful direction to help my sleep. Thank you.” “I enjoyed doing the sleep goal each week … It really helped me reflect and think of ways/things to change and improve.” “Just want to thank you for the class, and hope you let us all know when the next one will be so we can refer friends and relatives.” Participant responses were overwhelmingly positive. In terms of suggestions for the future, two participants asked for information on diet and sleep to be included and two requested follow-up classes to check-in on progress.
Discussion
This pilot study sought to determine the effectiveness of a community-based, health educator-led, virtually delivered sleep education program for older adults. Compared to the control group, the intervention group experienced significant improvements in sleep quality (lower PSQI scores), sleep hygiene-related behaviors (lower SHI scores), and excessive daytime sleepiness scores (lower ESS scores). The effect sizes for these outcomes, as well as sleep duration and insomnia symptoms, ranged from medium to large.56 These results suggest that online delivery of behavior-based sleep education programming is a promising, cost-effective strategy to improve the sleep of community-dwelling older adults.
Effects of SLEEP
The medium to large effect sizes observed in this study generally agree with the work of others based on several recent meta-analyses19,26,35 and individual reports.37 One of these meta-analyses studied the effects of cognitive and behavioral interventions on sleep outcomes and reported medium to large effect sizes for sleep efficiency and ISI.19 The second meta-analysis reported medium effect sizes for sleep quality based on studies of adults without sleep disorders.26 A notable exception in that study was the small effect on total sleep time; however, this lack of intervention effect on total sleep time has been reported elsewhere.22 The final meta-analysis examined the effects of digital CBTi interventions and reported an effect size of 0.392 (Cohen’s d) for improvement in ISI-measured insomnia symptoms,35 which is not that different from the current study’s ISI effect size of 0.49. In terms of individual studies that delivered group-based programming to older adults that was not CBTi, we are aware of only one that reported effect sizes,37 and these were also medium to large in size. Our findings suggest that SLEEP generated medium to large effect sizes, which is consistent with the literature. For SLEEP, the largest effect sizes were observed for sleep hygiene behaviors and sleep quality.
While statistical significance is important to the researcher, clinical relevance, or whether the participant can actually perceive a beneficial change resulting from treatment, is meaningful to both the researcher and the participant. One method of assessing clinical relevance for health-related quality of life measures has been put forth by Norman et al55 who suggest that a change of at least 0.5 SD from baseline scores represents meaningful and perceptible change to most patients. Using this guideline, sleep quality, sleep duration, insomnia symptoms, and sleep hygiene behaviors experienced both beneficial and perceptible changes. These perceptible changes are supported by the participant comments regarding the program.
Participant feedback regarding the course was almost uniformly positive and perceived likelihood of maintaining changes appeared promising. Suggestions for improvement from this pilot group included the addition of a discussion about the effects of diet on sleep and the desire for follow-up sessions. As a result of this feedback, information about diet and sleep has been added to facilitator training, and monthly emails reminding participants of the 6 main concepts covered in class have been implemented. These monthly “nudges” have been appreciated by a number of participants who said they were good reminders to resume or maintain their improved sleep hygiene behaviors.
SLEEP Curriculum Design Elements
The goal setting element of SLEEP likely plays an important role in the successes observed. Goal setting has been shown to be an effective strategy for addressing a variety of health concerns, including diabetes,57 physical activity,58 and weight management.59 Researchers of goal setting suggest that making goals specific and publicly sharing them promote goal attainment.60 By setting clearly defined personal goals based on the sleep recommendations taught in class and sharing them with the group, participants were able to practice new techniques to successfully resolve sleep problems. These successes supported a sense of self-efficacy, or the belief that an individual has the skills and abilities to be successful in accomplishing a specific task.61 According to Social Cognitive Theory, self-efficacy is an important determinant of behavior change43 and has been shown to be a significant factor in engaging in desirable health behaviors in a variety of populations.62–64 Greater self-efficacy increases the likelihood of goal attainment60 and can be cultivated by successfully mastering an activity as well as developed through observational learning – watching and listening to the experiences of people like oneself to better understand what success can look like.43 The group-based instruction style of SLEEP promotes sharing successes and brainstorming solutions to barriers. When others in the group demonstrate positive behaviors and share what has worked for them, these behaviors become normative. These norms positively influence behavior.43,65 For these reasons, we believe the goal setting component of the program is a key part of its success.
While the SLEEP program was developed for older adults, we did not restrict participation based on age. This is because the literature suggests that treatment effects of sleep programming are not related to age19 and there are no age-specific recommendations in terms of sleep behaviors or education topics.38 While the age of participants in the SLEEP intervention group was higher than the control group, we do not believe this significantly affected the outcome. Future work should investigate whether age plays a role in participant success in SLEEP.
The virtual delivery method and use of health educators within a group setting means that SLEEP can help to address the limited number of CBTi therapists available to treat sleep problems.22 All training and course materials are freely available online. Costs associated with program delivery involve facilitator time and access to an online video conferencing platform. Worksheets and handouts are emailed to clients. The program was developed with Michigan State University (MSU) Extension educators, but anyone can be trained to deliver SLEEP. The connection with MSU Extension makes SLEEP highly scalable as Cooperative Extension Service educators are available throughout the United States.
Strengths and Limitations
Validated tools and the control group strengthen the confidence in study findings. However, while validated tools were used to assess sleep outcomes, there was no objective measure of sleep duration. Still, sleep duration information was extracted from the PSQI, which is in accordance with the practices of other researchers.45–47 The intervention group sample size is consistent with the median sample size (n=18) reported in a meta-analysis of 87 sleep studies conducted on adults without diagnosed sleep disorders.26 Still, the small sample size and relatively smaller effect sizes could obscure our ability to detect differences in sleep duration and ISI scores. That the sample was almost entirely female reduces generalizability to males. Another limitation involves study design. This study was a quasi-experimental trial rather than a randomized control trial, and as such, the study is at higher risk for bias. Participants interested in sleep education who had previously enrolled in MSU Extension programming were offered the opportunity to participate. These individuals may be more highly motivated to participate in sleep- or health-related programming compared to the general population; however, these individuals – those interested and willing to participate in sleep-related programming – are the target audience for SLEEP.45 Finally, differences in ages between the two groups were present, with the intervention group younger than the control group. Older age has been associated with an increased likelihood of sleep disturbance66 but adults younger than 65 years are more likely to not meet sleep duration recommendations.67 While sleep measures did not differ from baseline between the two groups, future work should examine the effects of the program on younger individuals.
Conclusion
Given the widespread prevalence of sleep problems in the adult population combined with lack of access to care, effective, scalable public health interventions are desperately needed. SLEEP improved sleep quality, reduced maladaptive sleep hygiene behaviors, and reduced daytime sleepiness compared to the control group. Effect sizes for all sleep measures, which included sleep quality, sleep duration, insomnia symptoms, sleep hygiene behaviors, and excessive daytime sleepiness, were medium or large. In the intervention group, changes in sleep measures were judged to be clinically meaningful (≥0.5 SD) for all measures except daytime sleepiness. These results support the efficacy of a group-based, virtual education intervention delivered by health educators in improving sleep outcomes among older adults.
Acknowledgments
The authors wish to thank Chen Du, MS, RDN, CNSC, LD for data analysis support.
Disclosure
All authors report grants from Michigan Health Endowment Fund, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Liu Y, Wheaton AG, Chapman DP, Cunningham TJ, Lu H, Croft JB. Prevalence of healthy sleep duration among adults — United States, 2014. Morb Mortal Wkly Rep. 2016;65:137–141. doi:10.15585/mmwr.mm6506a1
2. Lin C-L, Lin C-P, Chen S-W, Wu H-C, Tsai Y-H. The association between sleep duration and overweight or obesity in Taiwanese adults: a cross-sectional study. Obes Res Clin Pract. 2018;12:384–388. doi:10.1016/j.orcp.2016.07.005
3. Furihata R, Uchiyama M, Suzuki M, et al. Association of short sleep duration and short time in bed with depression: a Japanese general population survey. Sleep Biol Rhythms. 2015;13:136–145. doi:10.1111/sbr.12096
4. Chaput J-P, Wong SL, Michaud I. Duration and quality of sleep among Canadians aged 18 to 79. Health Rep. 2017;28:28–33.
5. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1:233–243. doi:10.1016/j.sleh.2015.10.004
6. Sheehan CM, Frochen SE, Walsemann KM, Ailshire JA, Are US adults reporting less sleep?: findings from sleep duration trends in the National Health Interview Survey, 2004–2017. Sleep N Y N. 2019;42.
7. Salehinejad MA, Majidinezhad M, Ghanavati E, et al. Negative impact of COVID-19 pandemic on sleep quantitative parameters, quality, and circadian alignment: implications for health and psychological well-being. EXCLI J. 2020;19:1297–1308. doi:10.17179/excli2020-2831
8. Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, et al. Impact of social isolation due to COVID-19 on health in older people: mental and physical effects and recommendations. J Nutr Health Aging. 2020;24(9):938–947. doi:10.1007/s12603-020-1500-7
9. Morrow-Howell N, Galucia N, Swinford E. Recovering from the COVID-19 pandemic: a focus on older adults. J Aging Soc Policy. 2020;32:526–535. doi:10.1080/08959420.2020.1759758
10. Chaput J-P, Dutil C, Featherstone R, et al. Sleep duration and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S218–S231. doi:10.1139/apnm-2020-0034
11. Rod NH, Kumari M, Lange T, Kivimäki M, Shipley M, Ferrie J. The joint effect of sleep duration and disturbed sleep on cause-specific mortality: results from the Whitehall II Cohort Study. PLoS One. 2014;9:e91965. doi:10.1371/journal.pone.0091965
12. Shi L, Chen S-J, Ma M-Y, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16. doi:10.1016/j.smrv.2017.06.010
13. Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246–256. doi:10.1016/j.sleep.2016.08.006
14. Goldstein SJ, Gaston SA, McGrath JA, Jackson CL. Sleep health and serious psychological distress: a nationally representative study of the United States among White, Black, and Hispanic/Latinx adults. Nat Sci Sleep. 2020;12:1091–1104. doi:10.2147/NSS.S268087
15. Besedovsky L, Lange T, Born J. Sleep and immune function. Pflüg Arch Eur J Physiol. 2012;463:121–137. doi:10.1007/s00424-011-1044-0
16. Spira AP, Covinsky K, Rebok GW, Stone KL, Redline S, Yaffe K. Objectively measured sleep quality and nursing home placement in older women. J Am Geriatr Soc. 2012;60:1237–1243. doi:10.1111/j.1532-5415.2012.04044.x
17. Wu L, Sun D. Sleep duration and falls: a systemic review and meta‐analysis of observational studies. J Sleep Res. 2017;26:293–301. doi:10.1111/jsr.12505
18. Brassington GS, King AC, Bliwise DL. Sleep problems as a risk factor for falls in a sample of community-dwelling adults aged 64–99 years. J Am Geriatr Soc. 2000;48:1234–1240. doi:10.1111/j.1532-5415.2000.tb02596.x
19. van Straten A, van der Zweerde T, Kleiboer A, Cuijpers P, Morin CM, Lancee J. Cognitive and behavioral therapies in the treatment of insomnia: a meta-analysis. Sleep Med Rev. 2018;38:3–16. doi:10.1016/j.smrv.2017.02.001
20. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med. 2004;164:1888–1896.
21. Edinger JD, Means MK. Cognitive–behavioral therapy for primary insomnia. Clin Psychol Rev. 2005;25:539–558. doi:10.1016/j.cpr.2005.04.003
22. Seyffert M, Lagisetty P, Landgraf J, et al. Internet-delivered cognitive behavioral therapy to treat Insomnia: a systematic review and meta-analysis. PLoS One. 2016;11:e0149139. doi:10.1371/journal.pone.0149139
23. Vitiello MV, McCurry SM, Rybarczyk BD. The future of cognitive behavioral therapy for insomnia: what important research remains to be done? J Clin Psychol. 2013;69:1013–1021. doi:10.1002/jclp.21948
24. Crowley R, Daniel H, Cooney TG, Engel LS. Envisioning a better U.S. health care system for all: coverage and cost of care. Ann Intern Med. 2020;172:S7–S32. doi:10.7326/M19-2415
25. Aloia M, Lee-Chiong T, White D. Wake Up Call: Global Sleep Satisfaction Trends. Philips; 2020. Available from: https://www.google.com/search?q=Wake+Up+Call%3A+Global+Sleep+Satisfaction+Trends&rlz=1C5CHFA_enUS909US909&oq=Wake+Up+Call%3A+Global+Sleep+Satisfaction+Trends&aqs=chrome.69i57.431j0j4&sourceid=chromeiUTF-8.
26. Murawski B, Wade L, Plotnikoff RC, Lubans DR, Duncan MJ. A systematic review and meta-analysis of cognitive and behavioral interventions to improve sleep health in adults without sleep disorders. Sleep Med Rev. 2018;40:160–169. doi:10.1016/j.smrv.2017.12.003
27. Bootzin RR, Epstein DR. Understanding and treating insomnia. Annu Rev Clin Psychol. 2011;7:435–458. doi:10.1146/annurev.clinpsy.3.022806.091516
28. Murawski B, Plotnikoff RC, Rayward AT, et al. Efficacy of an m-health physical activity and sleep health intervention for adults: a randomized waitlist-controlled trial. Am J Prev Med. 2019;57:503–514. doi:10.1016/j.amepre.2019.05.009
29. Okun M, Johanson KA, Bohlen A, Felicano L. 0386 Stimulus control therapy versus sleep hygiene education in older adults with insomnia. Sleep. 2019;42:A156–A157. doi:10.1093/sleep/zsz067.385
30. Morin CM, Bootzin RR, Buysse DJ, Edinger JD, Espie CA, Lichstein KL. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998–2004). Sleep. 2006;29:1398–1414. doi:10.1093/sleep/29.11.1398
31. Joshi S. Nonpharmacologic therapy for insomnia in the elderly. Clin Geriatr Med. 2008;24:107–119. doi:10.1016/j.cger.2007.08.005
32. Win AZ. Telehealth can bridge the gap for rural, disabled, and elderly patients. J Am Med Dir Assoc. 2015;16:268–269. doi:10.1016/j.jamda.2015.01.077
33. LeBlanc LA, Lerman DC, Normand MP. Behavior analytic contributions to public health and telehealth. J Appl Behav Anal. 2020;53:1208–1218. doi:10.1002/jaba.749
34. Vincent N, Lewycky S. Logging on for better sleep: RCT of the effectiveness of online treatment for insomnia. Sleep. 2009;32:807–815. doi:10.1093/sleep/32.6.807
35. Soh HL, Ho RC, Ho CS, Tam WW. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med. 2020;75:315–325. doi:10.1016/j.sleep.2020.08.020
36. Morin C, Azrin N. Behavioral and cognitive treatments of geriatric insomnia. J Consult Clin Psychol. 1988;56:748–753. doi:10.1037/0022-006X.56.5.748
37. Epstein DR, Sidani S, Bootzin RR, Belyea MJ. Dismantling multicomponent behavioral treatment for insomnia in older adults: a randomized controlled trial. Sleep. 2012;35:797–805. doi:10.5665/sleep.1878
38. Kamel NS, Gammack JK. Insomnia in the elderly: cause, approach, and treatment. Am J Med. 2006;119:463–469. doi:10.1016/j.amjmed.2005.10.051
39. Yang P-Y, Ho K-H, Chen H-C, Chien M-Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: a systematic review. J Physiother. 2012;58:157–163. doi:10.1016/S1836-9553(12)70106-6
40. Irwin MR, Olmstead R, Motivala SJ. Improving sleep quality in older adults with moderate sleep complaints: a randomized controlled trial of Tai Chi Chih. Sleep. 2008;31:1001–1008.
41. Manjunath NK, Telles S. Influence of Yoga & Ayurveda on self-rated sleep in a geriatric population. Indian J Med Res. 2005;121:683–690.
42. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Educ Q. 1988;15:175–183. doi:10.1177/109019818801500203
43. Bandura A. Health promotion from the perspective of social cognitive theory. Psychol Health. 1998;13:623–649. doi:10.1080/08870449808407422
44. Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
45. Gebhart C, Erlacher D, Schredl M. Moderate exercise plus sleep education improves self-reported sleep quality, daytime mood, and vitality in adults with chronic sleep complaints: a waiting list-controlled trial. Sleep Disord. 2011;2011:1–10. doi:10.1155/2011/809312
46. Perlman CA, Johnson SL, Mellman TA. The prospective impact of sleep duration on depression and mania. Bipolar Disord. 2006;8:271–274. doi:10.1111/j.1399-5618.2006.00330.x
47. Hung H-C, Yang Y-C, Ou H-Y, Wu J-S, Lu F-H, Chang C-J. The association between self-reported sleep quality and overweight in a Chinese population. Obesity. 2013;21:486–492. doi:10.1002/oby.20259
48. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307. doi:10.1016/S1389-9457(00)00065-4
49. Mastin DF, Bryson J, Corwyn R. Assessment of sleep hygiene using the Sleep Hygiene Index. J Behav Med. 2006;29:223–227. doi:10.1007/s10865-006-9047-6
50. Johns MW. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep. 1992;15:376–381. doi:10.1093/sleep/15.4.376
51. McDonald JH 6.1: multiple comparisons. Statistics LibreTexts. June 27, 2017. Available from: https://stats.libretexts.org/Bookshelves/Applied_Statistics/Book%3A_Biological_Statistics_(McDonald)/06%3A_Multiple_Tests/6.01%3A_Multiple_Comparisons.
52. Feise RJ. Do multiple outcome measures require p-value adjustment? BMC Med Res Methodol. 2002;2:8. doi:10.1186/1471-2288-2-8
53. G*Power 3.1 manual. October 15, 2020. Available from: https://www.psychologie.hhu.de/fileadmin/redaktion/Fakultaeten/Mathematisch-Naturwissenschaftliche_Fakultaet/Psychologie/AAP/gpower/GPowerManual.pdf.
54. de Boer MR, Waterlander WE, Kuijper LD, Steenhuis IH, Twisk JW. Testing for baseline differences in randomized controlled trials: an unhealthy research behavior that is hard to eradicate. Int J Behav Nutr Phys Act. 2015;12:12. doi:10.1186/s12966-015-0162-z
55. Norman GR, Sloan JA, Wyrwich KW Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care 2003:582–592.
56. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
57. Fredrix M, McSharry J, Flannery C, Dinneen S, Byrne M. Goal-setting in diabetes self-management: a systematic review and meta-analysis examining content and effectiveness of goal-setting interventions. Psychol Health. 2018;33(8):955–977. doi:10.1080/08870446.2018.1432760
58. McEwan D, Harden SM, Zumbo BD, et al. The effectiveness of multi-component goal setting interventions for changing physical activity behaviour: a systematic review and meta-analysis. Health Psychol Rev. 2016;10:67–88. doi:10.1080/17437199.2015.1104258
59. O’Hara BJ, Gale J, McGill B, et al. Weight-related goal setting in a telephone-based preventive health-coaching program: demonstration of effectiveness. Am J Health Promot. 2017;31:491–501. doi:10.1177/0890117116660776
60. Latham GP, Locke EA. Self-regulation through goal setting. Organ Behav Hum Decis Process. 1991;50:212–247. doi:10.1016/0749-5978(91)90021-K
61. Raedeke TD, Dlugonski D. High versus low theoretical fidelity pedometer intervention using social-cognitive theory on steps and self-efficacy. Res Q Exerc Sport. 2017;88:436–446. doi:10.1080/02701367.2017.1368976
62. AbuSabha R, Achterberg C. Review of self-efficacy and locus of control for nutrition-and health-related behavior. J Am Diet Assoc. 1997;97:1122–1132. doi:10.1016/S0002-8223(97)00273-3
63. Conn VS, Tripp‐Reimer T, Maas ML. Older women and exercise: theory of planned behavior beliefs. Public Health Nurs. 2003;20:153–163. doi:10.1046/j.1525-1446.2003.20209.x
64. Schwarzer R, Renner B. Social-cognitive predictors of health behavior: action self-efficacy and coping self-efficacy. Health Psychol. 2000;19(5):487–495. doi:10.1037/0278-6133.19.5.487
65. Sheeran P, Maki A, Montanaro E, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. 2016;35:1178–1188. doi:10.1037/hea0000387
66. Prinz PN. Sleep and sleep disorders in older adults. J Clin Neurophysiol. 1995;12:139–146. doi:10.1097/00004691-199503000-00004
67. Centers for Disease Control and Prevention. Short sleep duration among US adults. 2017. Available from: https://www.cdc.gov/sleep/data_statistics.html.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.