Back to Journals » Nature and Science of Sleep » Volume 18

Sleep Duration, Chronotype, and Mortality in Parkinson’s Disease: A Prospective Cohort Study
Authors Partinen E ![]() , Ylikoski A, Sieminski M
, Ylikoski A, Sieminski M ![]() , Kaps M, Partinen M, Hublin C
, Kaps M, Partinen M, Hublin C ![]()
Received 28 October 2025
Accepted for publication 9 February 2026
Published 13 March 2026 Volume 2026:18 568358
DOI https://doi.org/10.2147/NSS.S568358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Eemil Partinen,1– 4 Ari Ylikoski,5 Mariusz Sieminski,6 Madli Kaps,7 Markku Partinen,2,4 Christer Hublin8
1Sleep Disorder Outpatient Clinic, Department of Psychiatry, Helsinki University Central Hospital, Helsinki, Finland; 2Helsinki Sleep Clinic, Terveystalo Healthcare, Helsinki, Finland; 3Department of Neurology, Helsinki University Central Hospital, Helsinki, Finland; 4Department of Clinical Neurosciences, Clinicum, University of Helsinki, Helsinki, Finland; 5The Social Insurance Institution of Finland (KELA), Helsinki, Finland; 6Department of Emergency Medicine, Medical University of Gdansk, Gdansk, Poland; 7Department of Psychiatry, Helsinki University Central Hospital, Helsinki, Finland; 8Finnish Institute of Occupational Health, Helsinki, Finland
Correspondence: Eemil Partinen, Email [email protected]
Aim: Sleep disturbances are a common non-motor symptoms in Parkinson’s disease (PD) and may occur already in the prodromal phase. In the general population, shorter sleep duration is linked to higher mortality, while longer sleep duration has been associated with an increased risk of developing PD. We examined the relationships between sleep duration, chronotype, and mortality in patients with PD.
Methods: A total of 855 randomly selected patients with PD completed a structured questionnaire including self-reported sleep duration and chronotype. Mortality data were collected from the national death registry.
Results: Altogether 435 subjects (238 men; 54.7%) were included. The mean follow-up time was 4.3 (0.3– 7.0) years, during which 99 participants had died. In a univariable model, longer sleep duration was associated with higher mortality [HR 1.31, 95% confidence interval (1.15– 1.49), P< 0.0001]. In a fully adjusted model, longer sleep duration [HR 1.17 (1.01– 1.35), P=0.035], older age, male gender, PD duration and depression were associated with higher mortality. BMI and high physical activity were associated with lower mortality. Although short sleep showed an association with mortality in univariable analyses, this association did not persist after multivariable adjustment [HR 0.82 (0.52– 1.30), P=0.401]. Chronotype was not associated with mortality. Long sleepers were older, had lower mean levodopa-dose, took more naps, and were sleepier than short sleepers.
Conclusion: Self-reported longer sleep duration was associated with higher mortality in patients with Parkinson’s disease, whereas chronotype was not associated with mortality. This does not imply a protective effect of shorter sleep duration. Further studies are needed to clarify whether sleep duration reflects disease-related factors, behavioral patterns, or progression of Parkinson’s disease.
Keywords: Parkinson’s disease, mortality, sleep duration, sleep apnea, restless legs, sleep length, chronotype, morningness, eveningness
Introduction
Sleep disturbances are among the most common non-motor symptoms in Parkinson’s disease (PD).1,2 In Finland, the prevalence of Parkinson’s disease has been estimated at 268 per 100,000 population (95% highest density regions 263–274), underscoring its substantial public health impact.3 Changes in sleep structure, circadian rhythmicity and sleep duration may be observed already in the prodromal stage of PD.4,5 In our earlier work using the same cohort, we reported that sleep talking and REM sleep behaviours together with sleep talking were linked to increased mortality.6 Sleep disturbances have been linked to alterations in brain function and neuronal activity. Nocturnal hypoxemia has been linked to changes in cortical EEG activity, suggesting that disturbed sleep can affect neuronal functioning.7 In the present study, we examine how sleep duration and chronotype relate to mortality, thereby addressing additional dimensions of sleep and circadian health in Parkinson’s disease.
In general population, several studies have demonstrated that sleep duration may have either a U-shaped risk profile or a linear profile, where shorter sleep is associated with increased mortality.8 The lowest mortality risk is observed between 7 and 8 hours of nighttime sleep.9–11 The mechanisms underlying this association are unclear. Shorter sleep duration has been linked to risk of dementia.12 Recent studies have associated longer sleep duration in older adults with a higher risk of developing Parkinson’s disease and incident dementia in the general aging population, whereas one study linked shorter sleep duration in middle-aged individuals to a younger age at PD diagnosis.13–18 Additionally, tau pathology is more pronounced in individuals with Alzheimer’s disease and longer sleep duration.19
Chronotype is correlated with the molecular mechanisms of the circadian system. Various external, internal and behavioural factors, such as light, temperature, exercise, and age, can adjust the chronotype.20 It is suggested that changes in circadian rhythm may be related to the pathophysiology of PD, although dopaminergic medications may also modify the chronotype.21,22 A recent study indicated that PD Patients with different chronotypes do not significantly differ from each other in terms of disease duration, sleepiness and medication.23 Disruption of circadian rhythmicity, but not timing, has been linked to an increased risk of developing PD.24 In studies conducted in the general population, a later chronotype appears to be related to higher morbidity and mortality.25,26
Based on the most recent studies we hypothesized that longer sleep duration may be associated with increased mortality in patients with Parkinson’s disease (PD). The theory is that fragmented sleep and more severe underlying neuropathology could lead to longer sleep as a compensatory mechanism. Consequently, longer sleep may indicate more severe PD pathology and be linked to higher mortality rates.
The study also aimed to investigate whether a later chronotype (the natural inclination for sleep timing) is related to increased mortality in PD patients. To test these hypotheses, we analysed data from a randomly selected prospective cohort study.
Methods
Study Subjects
A total of 1,500 subjects were randomly selected from 7,500 members of the Finnish Parkinson’s Association. Between 2010 and 2011, a structured questionnaire was sent to 1,447 eligible subjects. The inclusion criteria required participants to be alive, able to provide consent, and have a diagnosis of Parkinson’s disease made by a neurologist. The questionnaire was specifically designed for patients with Parkinson’s disease and the questions on sleep were based mainly on the validated Basic Nordic Sleep Questionnaire.27 Details about the questionnaire and the study population can be found in earlier publications.28 The participants were informed of the purpose of the study and gave their written informed consent. All who had given consent were recontacted during 2015 and 2016. Non-respondents received a reminder and were contacted via telephone. Mortality data were collected from the national death registry.
This study was approved by the regional ethics review board of the Helsinki and Uusimaa Hospital District (Ethics approval permit number: HUS 400/13/01/09) and was conducted in accordance with the Declaration of Helsinki.
Sleep Duration and Chronotype
Sleep duration (TST) was defined as the duration from going to bed to waking up, with the self-reported time to fall asleep subtracted. We used following questions: “At what time do you usually go to bed in the evenings?” and “At what time do you usually wake up on weekdays / workdays?”. Self-reported median time to fall asleep was subtracted from sleep period. “How long does it usually take you to fall asleep in the evenings?”, options were: In more than 40 minutes (we used 50 min), in 31–40 minutes (We used 35 min), In 21–30 minutes (35 min), In 10–20 minutes (15 minutes), In less than 10 minutes (5 minutes). We also recorded median total sleep time per 24 hours (TST24h), using a question: “How many hours do you sleep on average per 24 hours, including naps?”. Sleep duration was analysed as a continuous and categorical variable using 7 and 8 hours as a cut off. These values were used because we noticed an increase in the mortality when sleep duration exceeded 8 hours per night. These thresholds also reflect previous literature and resulted in approximately similar group sizes. Chronotype was assessed using a simplified morningness-eveningness question: “Are you a morning or evening person? (circle the option that best describes you).” The seven options were: 1. I am very alert/active in the morning and sleepy early in the evening (definitively morning person); 2. I am to some extent alert in the morning and sleepy in the evening (more morning than evening person); 3. Neither morning nor evening person; 4. I am to some extent alert in the evening and sleepy in the morning (more evening than morning person); 5. I am very alert/active in the evening and sleepy in the morning (definitively evening person); 6. I am alert/active in the evening and alert/active in the morning (needing very little sleep at night); 7. I am sleepy in the evening and sleepy in the morning (I am almost always sleepy). The types 1 + 2 and 4 + 5 were pooled to reflect morningness and eveningness, respectively. Other categories (3, 6 and 7) were defined as “unspecified”.29,30
Confounding Variables
We selected confounding variables based on epidemiological and clinical knowledge of factors potentially associated with both mortality and sleep duration. Socioeconomic status, smoking, and alcohol use were not included in the analysis due to a significant amount of missing data. Body mass index (BMI) was calculated based on self-reported weight and height. The STOP questionnaire assessed sleep-disordered breathing, using a STOP score of ≥2 as the cutoff for a high risk of sleep apnea.31 Total daily levodopa equivalent doses (LED) were determined with distinct conversion factors for various self-reported medications.32
Depression was screened using the WHO-5 Well-Being Scale, which has a Cronbach’s alpha ranging from 0.84 to 0.89. A WHO-5 score of ≤50 in scale from 0 to 100 (raw score of 12 to 13) indicates a risk for depression.33 WHO-5 shows high validity with adequate detection of depression in patients with Parkinson’s disease, which does not differ compared to BDI (P = 0.234).34 Another reason to choose the WHO-5 scale over the Beck Depression Inventory was to avoid false-positive depression scores due to poor sleep in subjects with sleep disorders.
Daytime sleepiness was measured using the Epworth Sleepiness Scale (ESS), for which we had a licence from Mapi Research Trust. Napping frequency was assessed through the question, “How often do you take naps?” Individuals who responded “daily or almost daily” were categorized as taking daily naps. Self-reported sleep need was evaluated using the question, “How much sleep do you need per day (how many hours would you sleep if you could sleep as long as you wanted)?” Sleep debt was calculated by subtracting total sleep time (TST) from sleep need. Disturbed nighttime sleep was assessed using a self-reported questionnaire item on the frequency of nighttime awakenings; participants reporting awakenings on three or more nights per week were classified as having disturbed nighttime sleep.
Restless Legs Syndrome (RLS) symptoms were assessed using a validated question with 100% sensitivity and 96.8% specificity: “When you try to relax in the evening or trying to sleep, do you experience unpleasant, restless feelings in your legs that are relieved by movement?”.35 The response options were: 1) “never (or less than once per month)”, 2) “less frequently than once per week”, 3) “on 1–2 evening/night per week”, 4) “on 3–5 evenings/nights per week”, and 5) “every evening/night or almost every evening/night”. Participants were classified as having RLS if they reported symptoms on at least 3 evenings/nights per week, following international criteria.36
Weekly metabolic equivalent values in minutes (MET-minutes) were calculated from self-reported weekly physical activities in different activity categories.37 Physical activities were divided into groups (<100; 100 ≤ and <1000; ≥1000 MET-minutes) representing sedentary, normal activity, and highly active lifestyles.38 Data on the use of hypnotics (including Z-drugs and benzodiazepines), antipsychotics (used as sleep aids), and sedating antidepressants were also collected.
Statistical Analysis and Selection of the Models
All analyses were performed using Stata 19.5 (StataCorp LLC, USA). Descriptive statistics for continuous variables are presented as means with 95% confidence intervals (CIs). The Shapiro–Wilk test was conducted to check for normality in the distributions. Depending on the distribution of the continuous variables, either the Student’s t-test or the Mann–Whitney U-test was applied. Categorical variables are reported in terms of frequency and percentages and were analysed using Pearson’s chi-square test and Fisher’s exact test. A P-value <0.05 was considered statistically significant.
The time variable was defined as the number of days from the date when the first questionnaire was answered to the latest known time point when the patient was alive (which could include the date of the second questionnaire, the last known contact, or the confirmed time of death). Variables included in the mortality models were selected based on established predictors and potential confounding factors. Physical activity was incorporated into the models as a known factor influencing survival and a possible surrogate marker for overall poor health. We included frequent daytime napping in the analyses as a potentially clinically significant sleep related variable and potential confounder. For mortality analyses, we used the Nelson-Aalen estimator and Cox proportional hazards models. Models were constructed using both forward and backward stepwise methods (for entry p< 0.1, for removal p>0.15). Variables were retained if their removal worsened model fit using the Akaike information criterion (AIC). Primary model 1 was designed to assess total sleep duration, while primary model 2 focused on evaluating the associations between chronotype and mortality. A limited number of biologically plausible interaction terms were tested, including interactions between chronotype and total sleep time (TST), 24-hour total sleep time (TST24h) and sleep timing variables, as well as between sleep duration, age and gender. Sensitivity analyses were performed to assess the reliability of the findings, including models using alternative sleep duration definitions (TST and TST24h) and models with and without adjustment for physical activity or daytime napping. Fully adjusted models including all available covariates were also examined. Model stability was assessed by calculating the events-per-variable ratio (EPV). The command “margins” was used to evaluate the average predicted probability of death with different sleep duration estimates.
The proportionality assumption in the Cox proportional hazards models was confirmed using time-interaction covariates and using Schoenfeld residuals (global and covariate-specific tests) and visual inspection of scaled Schoenfeld residual plots. To assess the robustness of the observed associations to potential unmeasured confounding, we calculated E-values for the primary sleep duration and mortality association.
Results
A total of 855 participants completed the initial questionnaire, resulting in a response rate of 59%. Information regarding mortality was collected through a follow-up questionnaire and the national death registries. Thirty-nine participants were lost to follow-up due to factors such as potential name changes, relocation abroad, lack of address or telephone information, or being untraceable in address registers. Complete data were gathered from 435 subjects who fully answered the first questionnaire and provided mortality information through the second questionnaire and national registries, yielding a response rate of 51% from the initial 855 participants.
Of the final study population, 336 individuals were alive at follow-up, while 99 had died. The mean follow-up period was 4.3 years, with a range from 0.3 to 7.0 years. The selection process for the study population is illustrated in Supplement Figure 1.
The final study population was older compared to those excluded due to incomplete data, as shown in Supplement Table 1. Sleep duration was in similar range between included and excluded subjects.
The demographics of the study population are presented in Table 1, which included 238 men and 197 women, all of whom were Caucasian. The subjects who passed away were generally older, slightly thinner, had a longer duration of Parkinson’s disease, experienced higher levels of depression, and took daily naps more frequently. Additionally, they reported longer nighttime sleep and total 24-hour sleep durations. These deceased individuals were less physically active and encountered more nighttime awakenings compared to those who were still alive at follow-up. However, there was no difference in chronotype between the deceased and the surviving subjects.
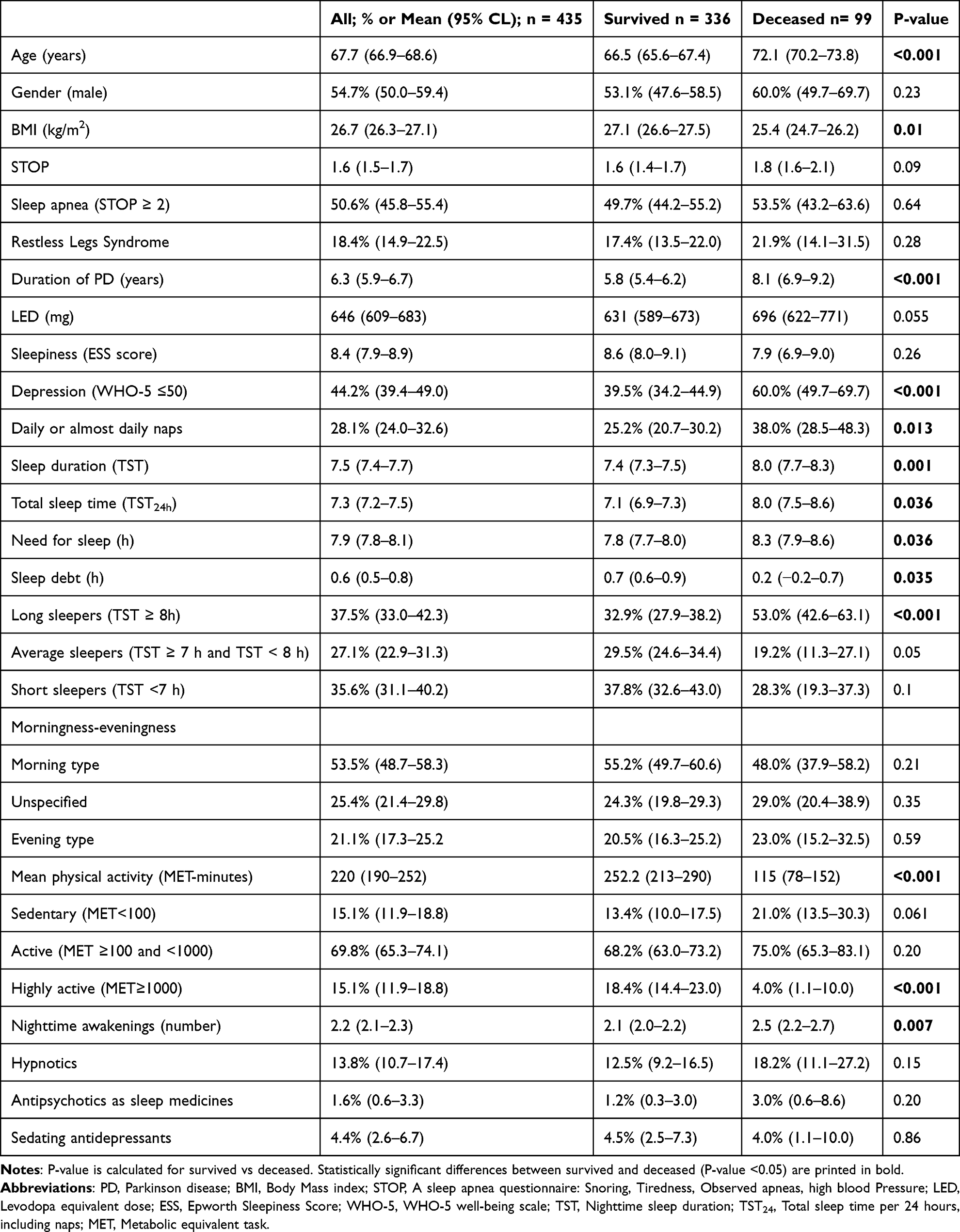 |
Table 1 Demographic Characteristics of Participants |
The calculated mean nighttime sleep duration (TST), based on bedtimes and sleep latency, was 7.5 hours (95% confidence interval (CI), 7.4–7.7; median, 7.5; interquartile range [IQR], 6.5–8.5). The self-reported mean total daily sleep time (TST24h) was 7.3 hours (95% CI, 7.2–7.5; median, 7; IQR, 6.0–8.0).
Cox Hazard Models
We examined the relationship between sleep duration and mortality using survival models (Table 2). Longer sleep duration was associated with higher mortality. This relationship was assessed through various methods, including plotting data, categorizing variables, and conducting margins analysis. Unadjusted Nelson-Aalen survival curves for different sleep durations are presented in Figure 1.
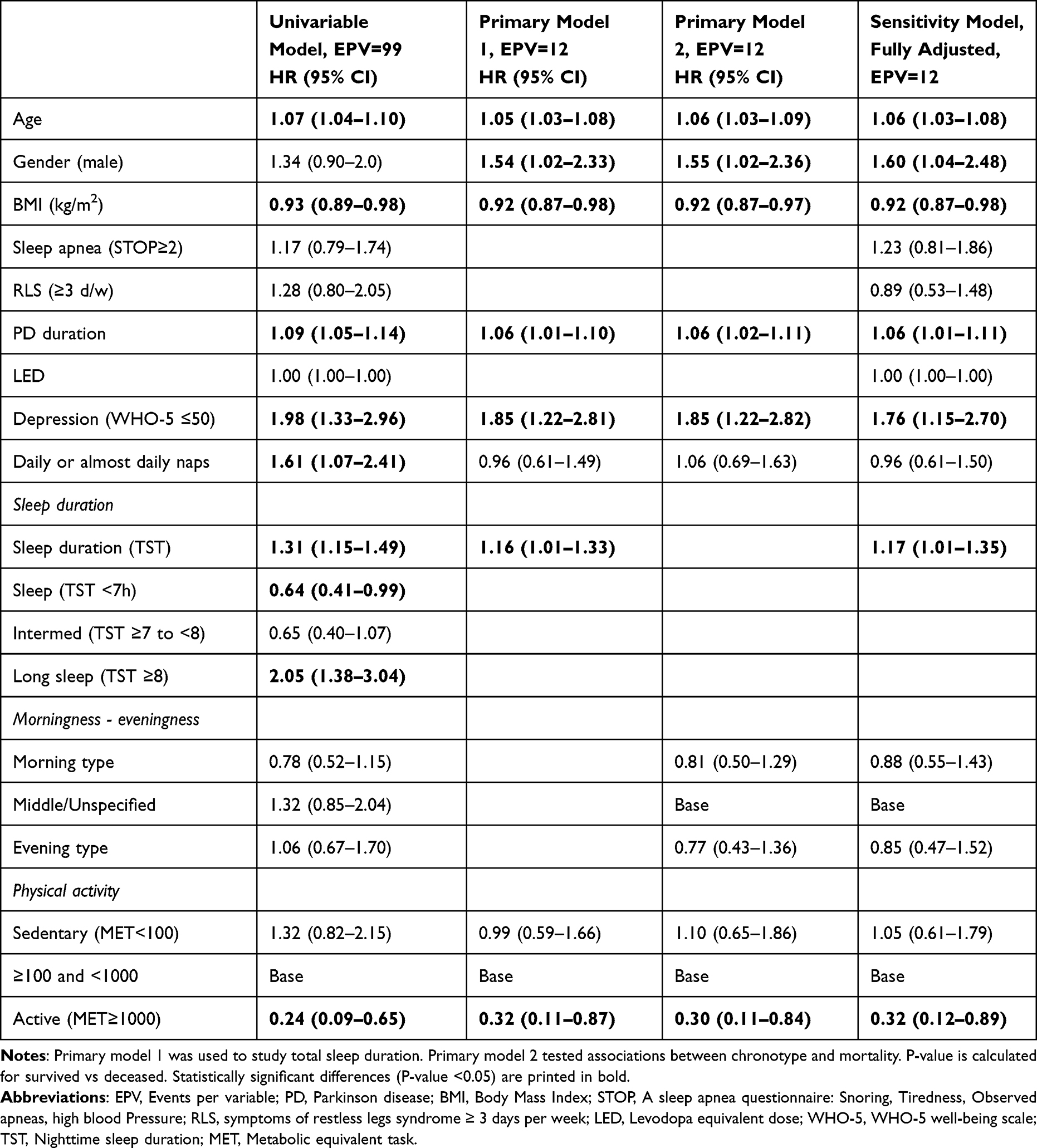 |
Table 2 Hazard Ratios for Mortality in Parkinson’s Disease (N=435, Number of Events = 99) |
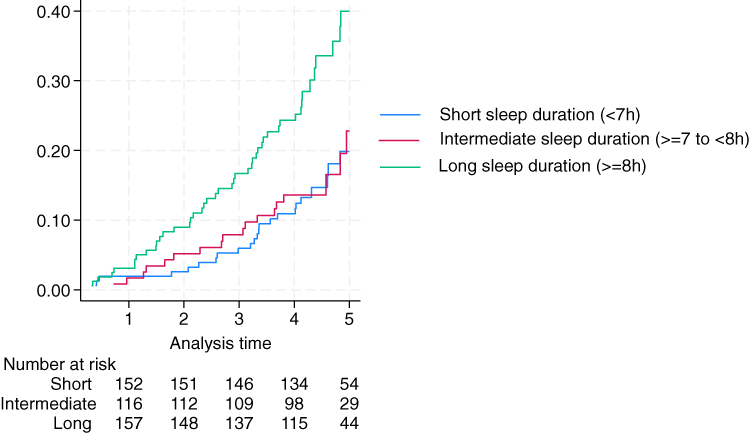 |
Figure 1 Unadjusted Nelson-Aalen survival estimates for different sleep durations. |
No violations of the proportional hazards assumption were detected based on Schoenfeld residuals (global and covariate-specific tests) and visual inspection of scaled Schoenfeld residual plots (Supplement Figures 2–11).
In univariable models, several factors were linked to higher mortality, including age, lower body mass index (BMI), the duration of Parkinson’s disease (PD), depression, daily or almost daily napping, and sleep duration. However, chronotype did not show any significant association with mortality.
Short sleep duration (< 7 hours per night) was linked to lower mortality, with a hazard ratio (HR) of 0.64 (95% CI 0.41–0.99), P=0.044. In contrast, average sleep duration (between 7 and 8 hours) was not associated with mortality, yielding an HR of 0.65 (95% CI 0.40–1.07), P=0.091. Longer sleep duration (≥ 8 hours) was linked to increased mortality, with an HR of 2.05 (95% CI 1.38–3.04), P<0.0001. This is seen also in margins plot given in Supplement Figure 12. When adjusted for same covariates as in model 1 (Table 2), short sleep duration (< 7 hours per night) was no longer associated with lower mortality, showing an HR of 0.82 (95% CI 0.52–1.30), P=0.401.
The use of sleep medications was not associated with mortality in the univariable models: hypnotics (HR 1.37, 95% CI 0.80–2.33), P=0.255, antipsychotics (HR 3.00, 95% CI 0.93–9.43), P=0.065, and sedating antidepressants (HR 0.85, 95% CI 0.31–2.30), P=0.744.
We constructed Cox proportional hazards models using the most promising variables from the univariable models, with gender included as a potential confounder. In all models, we used the middle categorical value of physical activity as a reference. Primary model 1 tested the association between sleep duration and mortality, while Primary model 2 focused on chronotype and its association with mortality. Interaction variables involving age, gender, chronotype and total sleep time (TST), or TST over 24 hours (TST24h) did not demonstrate significance and were excluded from all models. Additionally, sensitivity analyses indicated that disturbed nighttime sleep did not impact the results. Model 1 without physical activity yielded similar results, with TST remaining associated with mortality (HR 1.22 (95% CI, 1.06–1.40), p = 0.005).
In the fully adjusted sensitivity model, sleep duration, age, gender, PD duration, and depression all showed associations with increased mortality. Conversely, higher BMI and high levels of physical activity (defined as weekly metabolic equivalent of task [MET] minutes ≥1000) were associated with lower mortality. High probability of sleep apnea (STOP≥2 points) was not associated with mortality.
The E-value for the association between sleep duration and mortality was 1.95 and 1.57 for the lower confidence limit.
Sleep Duration
To confirm the findings, all models were reanalyzed using total sleep time over a 24-hour period (TST24h). TST24h was linked to higher mortality in the univariable model, showing a hazard ratio (HR) of 1.24 (95% CI, 1.14–1.35), P<0.0001. With the covariates from primary Model 1, the HR for TST24h was 1.18 (95% CI, 1.07–1.31), P=0.001. The fully adjusted sensitivity model (Table 2) produced an identical estimate for TST24h: HR 1.18 (95% CI, 1.07–1.31), P=0.002.
The study also evaluated the potential of sleep duration (TST) to categorize subjects into different phenotypes, as illustrated in Table 3. Long sleepers were generally older, took lower mean doses of levodopa, napped more frequently, reported greater levels of sleepiness, and were more often evening-oriented compared to short sleepers. Notably, long sleep duration was not linked to factors that typically disturb nighttime sleep, such as depression or nighttime awakenings often associated with insomnia. Additionally, the use of sleep medication was similar across individuals with varying sleep durations. We also used TST24h to categorize sleep duration. The results were in the same magnitude as using TST as the base value.
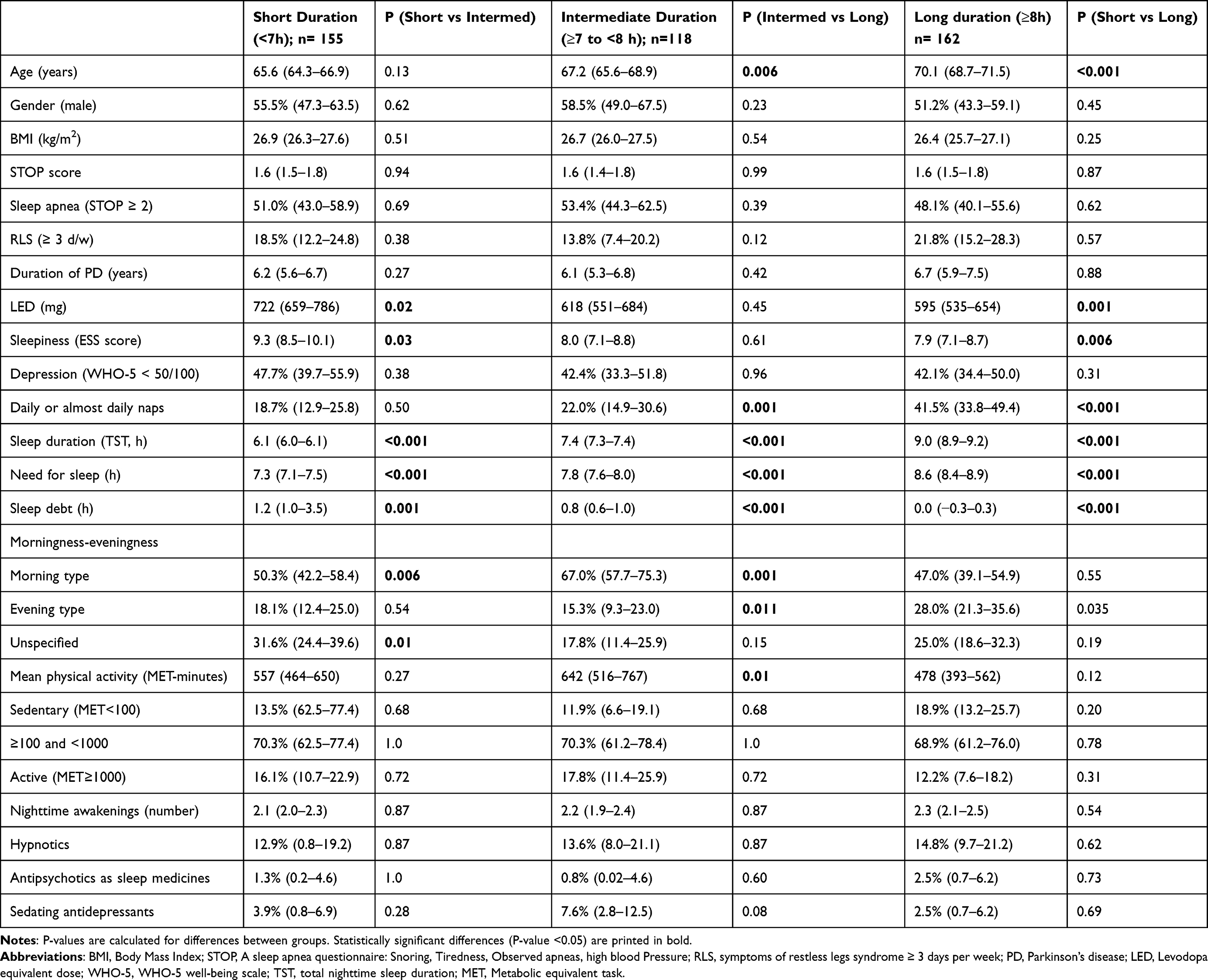 |
Table 3 Characteristics of Participants with Different Nighttime Sleep Duration |
Self-reported sleep needs correlated with increased mortality in a univariable model, the HR was 1.23 (95% CI, 1.10–1.38), P=0.001, but not in the multivariable model, adjusted for age, gender, BMI, PD duration, LED, naps, depression, and physical activity, with an HR of 1.14 (95% CI, 0.99–1.31), P=0.06. Conversely, sleep debt was negatively associated with mortality, with an HR of 0.79 (95% CI, 0.70–0.90) in the univariable model and an HR of 0.83 (95% CI, 0.73–0.95), P=0.005 in the multivariable model.
Discussion
The data support our hypotheses regarding the relationship between higher Parkinson’s disease (PD) mortality and longer sleep duration. Our analysis revealed that longer sleep duration was consistently associated with increased mortality across all tested models. At the same time sleep debt was associated with lower mortality rates. Interestingly, we did not observe any increase in mortality among subjects with a later chronotype. Additionally, factors such as age, duration of PD, and depression were associated with higher mortality rates, whereas a higher body mass index (BMI) and increased physical activity were associated with lower mortality. Because physical activity could act as a collider, its inclusion could introduce bias. However, results regarding sleep duration were similar with and without adjustment for physical activity.
We used a single item to evaluate morningness–eveningness, similar to the final question of the reduced Morningness–Eveningness Questionnaire, which has the highest correlation with the full MEQ.39 Single-item measures of morningness–eveningness cannot capture intermediate chronotypes and the subjectively perceived chronotype could misalign with intrinsic circadian preference. Although we did not observe an association between circadian preference and mortality, objectively measured circadian rhythms may still be relevant to Parkinson’s disease progression and survival.
Both nighttime sleep duration (TST) and 24-hour sleep duration (TST24h), which includes daytime napping, were used in this study. The average TST24h, derived from a single question, was shorter than the TST calculated from the time of falling asleep to the time of waking up.
Previous research indicates that individuals with poor sleep frequently underestimate their subjective sleep duration. In an earlier study, 37% of participants reported chronic insomnia symptoms, which may contribute to underestimation.2
The results are consistent with findings from a large survey examining estimation bias and the agreement between self-reportedsleep duration methods. Sleep durations reported using a single subjective assessment tended to be shorter than those calculated from sleep onset to offset.40 These findings indicate that measuring total sleep time based on sleep onset and offset provides a reasonable estimate of average nightly sleep duration.
Analyses were conducted using both TST and TST24h estimations. The choice of method did not alter the observed effects of sleep duration on mortality. Longer sleep duration was consistently associated with higher mortality, regardless of the measurement approach. When using categorical values, higher mortality was observed among subjects with TST >8 hours. This change is unlikely to happen exactly at 8 hours. In addition individuals tend to report sleep duration in rounded numbers, so our reported categories should be interpreted as approximations rather than exact biological thresholds.
Longer naps have been linked to neurodegeneration.41 A large US study found that increased daytime napping, but not total sleep time, correlated with Parkinson’s disease (PD) and poor health.42 In addition to poor health, frequent napping may indicate daytime sleepiness and unmet sleep needs. In our study, short sleepers had higher daytime sleepiness, as measured by ESS, and higher LED (see Table 3). However, frequent napping was linked to mortality only in univariable analysis. While increased napping could be a risk factor for PD, nighttime sleep duration appears more critical to mortality in people with PD.
There is evidence that longer sleep duration is associated with a higher risk of developing Parkinson’s disease (PD).13,14 The Nurses’ Health Study indicated that more years in rotating shift work and short sleep were associated with a lower risk of developing PD.13 Additionally, a higher awakening index in polysomnography appears to protect against Parkinson’s disease.14 Indirectly, our results in patients with PD align with the adverse effects of long sleep duration related to development of PD, as they demonstrate that longer sleep duration is also related to a worse prognosis of PD.
The relationship between sleep duration and mortality is complex. In general, shorter sleep or a U-shaped sleep length has been associated with higher mortality. This information has been available in the literature for decades. In this PD population, shorter sleep was associated with lower mortality, which should not be interpreted as evidence of a protective effect.
Longer sleep duration may be related to sleep fragmentation, which has been associated with increased Parkinson’s disease (PD) pathology in older individuals without a PD diagnosis.43 In our study, nighttime awakenings, depression rates, hypnotic use, and medication intake did not differ by sleep duration or relate to mortality. Additionally, the rate of depression did not correlate with sleep duration. The use of hypnotics was similar among subjects with different sleep durations. No association was found between the intake of hypnotics or other medications and mortality. Although the exact dosing times of dopaminergic drugs were not recorded, the mean levodopa equivalent dose (LED) was lower among subjects with longer total sleep time (TST) compared to short sleepers, with no difference in disease duration. The difference in daily levodopa dose could be attributed to different disease phenotypes, such as poor response to treatment, insufficient treatment, or incorrect diagnosis. It has been proposed that the “sleepy” Parkinson subtype, characterized by daytime sleepiness, could be more vulnerable to dopamine D3 agonist side effects, but lower levodopa intake alone likely does not explain higher mortality.44
We included weekly physical activity in the models as a potential marker of overall health. Physical activity has been associated with better outcomes in PD.45 Also in our study, higher physical activity was observed as a protective trait. However, no increase in mortality was observed among sedentary subjects. We hypothesized that more active subjects might sleep less, but this could not be confirmed. There was no association between the amount of physical activity and sleep duration.
The reasons for this finding are not clear. Longer sleep may reflect neurodegeneration of wake-promoting systems.18,43 Behavioral factors may also play a role, as individuals who sleep less and report less sleepiness may have a more active lifestyle, which is associated with better overall health outcomes. Several biological pathways could link sleep duration to PD progression, including impaired glymphatic flow, neuroinflammation and altered sleep architecture.44,45 However, these mechanisms were not assessed in this study. Future studies should integrate objective sleep measures, biomarkers and longitudinal design to clarify whether sleep duration reflects PD pathology, progression or prognosis.
The strength of our study lies in its prospective design and large sample size of patients with PD, which enables the investigation of associations between sleep behaviour and mortality in PD. Included and excluded participants were similar across baseline characteristics, though excluded individuals were slightly older. Because age relates to both sleep measures and mortality, this difference could introduce some selection bias. Complete information about the variables used in the study was available. The sample includes subjects from all geographic areas in Finland. Inclusion bias was minimized by allowing family members and healthcare personnel to assist in completing the questionnaire. If subjects did not respond, they were contacted by telephone.
This study has several limitations. Causal inferences cannot be made from an observational study. Residual confounding and misclassification of sleep measures may remain despite adjustments. Because sleep duration and chronotype were assessed cross-sectionally, we could not account for changes over time or prior to the first questionnaire. Unfortunately, wake after sleep onset times (WASO) were not collected, so total sleep times (TST) may be overestimations of true sleeping times. However, the conclusions would likely remain the same even if WASO had been available as it would probably affect all sleep duration categories similarly. In addition, our results were not affected by factors that could lead to increased WASO, such as sleep apnea, disturbed nighttime sleep, or RLS.
Self-estimated sleep duration is an easy and feasible way of estimating habitual sleep time. Self-estimated sleep duration may differ from the actual sleep duration. Many biases arise from self-reported data that can result in over and underestimation of sleep duration. To minimise bias, we used a validated Basic Nordic Sleep Questionnaire to inquire about bedtimes and sleep duration.27 Nevertheless, conditions such as insomnia or sleep apnea can affect the perception of sleep duration, often leading to a misestimation of actual sleep time. Calculating sleep duration from sleep onset and offset may be more accurate than a single question asking for sleep length.40 Although self-reports of sleep durations are not exact, they can still be useful for identifying general sleep patterns in epidemiological studies, especially when polysomnography is not feasible. For a more accurate assessment of habitual sleep length, combining self-reports with objective measures like actigraphy or smart devices can provide a more comprehensive picture. Unfortunately, such devices are not feasible in an epidemiological and registry based study.
Classification of chronotype is highly subjective in our study. Some misclassification is therefore possible, but is likely minor problem and would bias associations toward the null. Despite limitations, single-item chronotype assessments are widely used and accepted in large epidemiological studies.
One limitation is the lack of information regarding the duration of daytime naps. The frequency of naps per week was recorded, but the average length of naps was not separately assessed.
Another limitation is the absence of data on the exact time of death (over 24 hours). Although the date of death was requested, the estimated time of death was not specified. However, previous studies indicate that cardiovascular deaths most commonly occur in the morning hours between 9 and 11 am, and patients with Parkinson’s disease (PD) often die around 9 am.46
Causality between mortality and sleep duration cannot be inferred from these observational data. These findings should be interpreted in light of the questionnaire-based assessment and require replication in independent cohorts, preferably with objective sleep measurements. The information is based on a questionnaire without objective measurements, which affects data accuracy, particularly in estimations of sleep duration and chronotype. Self-reported sleep duration tends to overestimate objectively measured sleep duration, although correlations are consistent across age, sex, and varying sleep durations.47 Clinical confirmation of Parkinson’s disease was not possible due to resource constraints; however, only cases diagnosed by a neurologist and recorded in the Finnish Parkinson’s Disease Registry were included. Some diagnostic inaccuracies may persist given the difficulty distinguishing PD from other extrapyramidal disorders.
Conclusions
Self-reported longer sleep duration was associated with higher mortality in this cohort of patients with PD, whereas chronotype was not associated with mortality. The underlying mechanisms warrant further investigation. Longer sleep may reflect disease-related factors or behavioral patterns rather than a direct causal effect. Future studies should explore if sleep duration is a marker of disease progression or whether related factors, such as social activity and well-being, contribute to prognosis. These findings do not imply that shorter sleep is beneficial, but it is worth exploring if sleep-related factors could be modifiable risk factors in PD.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Gratitude is extended to all the patients and their relatives who participated and assisted in this study. Much of the data collection was conducted by assistants Raili Reemets, Anselmi Kuusi, and Ilona Kuusi. Appreciation is also extended to the personnel of the Finnish Parkinson Society, particularly Kirsi Martikainen, who assisted with data collection and participant enrollment. Generative AI tool (Avidnote AI assistant of the University of Helsinki) was used to for language improvement.
Author Contributions
Eemil Partinen: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, visualization and writing original draft.
Ari Ylikoski: Conceptualization, data curation, investigation, methodology, writing – review & editing.
Mariusz Sieminski: Conceptualization, methodology, writing – review & editing.
Madli Kaps: Investigation, methodology, writing – review & editing.
Markku Partinen: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, supervision, writing – review & editing.
Christer Hublin: Conceptualization, methodology, interpretation, supervision, writing – review & editing.
All authors took part in revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was supported by funding from the Finnish Parkinson Foundation. Open access funded by Helsinki University Library.
Disclosure
Eemil Partinen has received funding from the Finnish Parkinson Foundation and University of Helsinki. Ari Ylikoski has received funding from the Finnish Parkinson Foundation. Markku Partinen received fees from Bioprojet, Idorsia, Takeda, Orion-Pharma, Berlin Cures, Umecrine and Teva. The other authors have no conflict of interests to declare.
References
1. Barone P, Antonini A, Colosimo C, et al. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov Disord. 2009;24(11):1641–13. doi:10.1002/mds.22643
2. Ylikoski A, Martikainen K, Sieminski M, Partinen M. Parkinson’s disease and insomnia. Neurol Sci. 2015;36:2003–2010. doi:10.1007/s10072-015-2288-9
3. Havulinna AS, Tienari PJ, Marttila RJ, et al. Geographical variation of medicated parkinsonism in Finland during 1995 to 2000. Mov Disord. 2008;23(7):1024–1031. doi:10.1002/mds.22024
4. Lysen TS, Darweesh SKL, Ikram MK, Luik AI, Ikram MA. Sleep and risk of parkinsonism and Parkinson’s disease: a population-based study. Brain. 2019;142(7):2013–2022. doi:10.1093/brain/awz113
5. Postuma RB, Berg D. Advances in markers of prodromal Parkinson disease. Nat Rev Neurol. 2016;12:622. doi:10.1038/nrneurol.2016.152
6. Partinen E, Ylikoski A, Sieminski M, Partinen M. Impact of REM sleep behavior and sleep talking on mortality in Parkinson’s disease. Cureus. 2024;16(1):e52565. doi:10.7759/cureus.52565
7. Ferreira I, Guerra P, Pinto N, Alfaiate D, Pereira A. Evaluation of wakefulness electroencephalogram in OSA patients. Sleep Breathing. 2024;28(5):2037–2043. doi:10.1007/s11325-024-03116-y
8. Shen X, Wu Y, Zhang D. Nighttime sleep duration, 24-hour sleep duration and risk of all-cause mortality among adults: a meta-analysis of prospective cohort studies. Sci Rep. 2016;6(1):21480. doi:10.1038/srep21480
9. Kojima M, Wakai K, Kawamura T, et al. Sleep patterns and total mortality: a 12-year follow-up study in Japan. J Epidemiol. 2000;10(2):87–93. doi:10.2188/jea.10.87
10. Hublin C, Partinen M, Koskenvuo M, Kaprio J. Sleep and mortality: a population-based 22-year follow-up study. Sleep. 2007;30(10):1245–1253. doi:10.1093/sleep/30.10.1245
11. Kurina LM, McClintock MK, Chen JH, Waite LJ, Thisted RA, Lauderdale DS. Sleep duration and all-cause mortality: a critical review of measurement and associations. Ann Epidemiol. 2013;23(6):361–370. doi:10.1016/j.annepidem.2013.03.015
12. Sabia S, Fayosse A, Dumurgier J, et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun. 2021;12(1):2289. doi:10.1038/s41467-021-22354-2
13. Chen H, Schernhammer E, Schwarzschild MA, Ascherio A. A prospective study of night shift work, sleep duration, and risk of Parkinson’s disease. Am J Epidemiol. 2006;163(8):726–730. doi:10.1093/aje/kwj096
14. Otaiku AI. Association of sleep abnormalities in older adults with risk of developing Parkinson’s disease. Sleep. 2022;45(11). doi:10.1093/sleep/zsac206
15. Chen Y, Gao Y, Sun X, et al. Association between sleep factors and Parkinson’s disease: a prospective study based on 409,923 UK Biobank participants. Neuroepidemiology. 2023;57(5):293–303. doi:10.1159/000530982
16. Beydoun HA, Naughton MJ, Beydoun MA, et al. Association of sleep disturbance with Parkinson disease: evidence from the Women’s health initiative. Menopause. 2022;29(3):255–263. doi:10.1097/GME.0000000000001918
17. Clark CE, Gold J, Rigby BR. Sleep duration in middle-aged years of life predicts the age of diagnosis of Parkinson’s disease. Sleep Med. 2024;8:100123. doi:10.1016/j.sleepx.2024.100123
18. Westwood AJ, Beiser A, Jain N, et al. Prolonged sleep duration as a marker of early neurodegeneration predicting incident dementia. Neurology. 2017;88(12):1172–1179. doi:10.1212/wnl.0000000000003732
19. Yoon SH, Kim H-K, Lee J-H, et al. Association of sleep disturbances with brain amyloid and tau burden, cortical atrophy, and cognitive dysfunction across the AD Continuum. Neurology. 2023;101(21):e2162–e2171. doi:10.1212/WNL.0000000000207917
20. Roenneberg T, Merrow M. The Circadian clock and human health. Curr Biol. 2016;26(10):R432–R443. doi:10.1016/j.cub.2016.04.011
21. Li S, Wang Y, Wang F, Hu LF, Liu CF. A new perspective for Parkinson’s disease: circadian rhythm. Neurosci Bull. 2017;33(1):62–72. doi:10.1007/s12264-016-0089-7
22. Videnovic A, Willis GL. Circadian system - A novel diagnostic and therapeutic target in Parkinson’s disease? Mov Disord. 2016;31(3):260–269. doi:10.1002/mds.26509
23. Murphy S, Chibnik LB, Videnovic A. Chronotype, sleep, and sleepiness in Parkinson’s disease. Parkinsonism Related Disord. 2023;106:105189. doi:10.1016/j.parkreldis.2022.10.011
24. Leng Y, Blackwell T, Cawthon PM, Ancoli-Israel S, Stone KL, Yaffe K. Association of Circadian abnormalities in older adults with an increased risk of developing Parkinson disease. JAMA neurol. 2020;77(10):1270–1278. doi:10.1001/jamaneurol.2020.1623
25. Hublin C, Kaprio J. Chronotype and mortality-a 37-year follow-up study in Finnish adults. Chronobiol Int. 2023;40(7):841–849. doi:10.1080/07420528.2023.2215342
26. Arora N, Richmond RC, Brumpton B, et al. Self-reported insomnia symptoms, sleep duration, chronotype and the risk of acute myocardial infarction (AMI): a prospective study in the UK Biobank and the HUNT Study. Eur J Epidemiol. 2023;38(6):643–656. doi:10.1007/s10654-023-00981-x
27. Partinen M, Gislason T. Basic Nordic Sleep Questionnaire (BNSQ): a quantitated measure of subjective sleep complaints. J Sleep Res. 1995;4:150–155. doi:10.1111/j.1365-2869.1995.tb00205.x
28. Ylikoski A, Martikainen K, Partinen M. Parasomnias and isolated sleep symptoms in Parkinson’s disease: a questionnaire study on 661 patients. J Neurol Sci. 2014;346(1):204–208. doi:10.1016/j.jns.2014.08.025
29. Danielsson K, Sakarya A, Jansson-Fröjmark M. The reduced morningness–eveningness questionnaire: psychometric properties and related factors in a young Swedish population. Chronobiol Int. 2019;36(4):530–540. doi:10.1080/07420528.2018.1564322
30. Merikanto I, Dauvilliers Y, Chung F, et al. Disturbances in sleep, circadian rhythms and daytime functioning in relation to coronavirus infection and Long-COVID - A multinational ICOSS study. J Sleep Res. 2022;31(4):e13542. doi:10.1111/jsr.13542
31. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812–821. doi:10.1097/ALN.0b013e31816d83e4
32. Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord. 2010;25(15):2649–2653. doi:10.1002/mds.23429
33. Krieger T, Zimmermann J, Huffziger S, et al. Measuring depression with a well-being index: further evidence for the validity of the WHO well-being index (WHO-5) as a measure of the severity of depression. J Affect Disord. 2014;156:240–244. doi:10.1016/j.jad.2013.12.015
34. Schneider CB, Pilhatsch M, Rifati M, et al. Utility of the WHO-five well-being index as a screening tool for depression in Parkinson’s disease. Mov Disord. 2010;25(6):777–783. doi:10.1002/mds.22985
35. Ferri R, Lanuzza B, Cosentino FI, et al. A single question for the rapid screening of restless legs syndrome in the neurological clinical practice. Eur J Neurol. 2007;14(9):1016–1021. doi:10.1111/j.1468-1331.2007.01862.x
36. Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance. Sleep Med. 2014;15(8):860–873. doi:10.1016/j.sleep.2014.03.025
37. Ainsworth BE, Herrmann SD, Meckes N, et al. The Compendium of Physical Activities Tracking Guide. Healthy Lifestyles Research Center, College of Nursing & Health Innovation, Arizona State University. Available from: https://sites.google.com/site/compendiumofphysicalactivities/.
38. World Health Organization GRC. Global Recommendations on Physical Activity for Health. WHO Press; 2010.
39. Adan A, Almirall H. Horne & Östberg morningness-eveningness questionnaire: a reduced scale. Pers Individ Dif. 1991;12(3):241–253. doi:10.1016/0191-8869(91)90110-W
40. Korman M, Zarina D, Tkachev V, et al. Estimation bias and agreement limits between two common self-report methods of habitual sleep duration in epidemiological surveys. Sci Rep. 2024;14(1):3420. doi:10.1038/s41598-024-53174-1
41. Li J, Chang Y-P, Riegel B, et al. Intermediate, but not extended, afternoon naps may preserve cognition in chinese older adults. J Gerontol Ser A. 2017;73(3):360–366. doi:10.1093/gerona/glx069
42. Gao J, Huang X, Park Y, et al. Daytime napping, nighttime sleeping, and Parkinson disease. Am J Epidemiol. 2011;173(9):1032–1038. doi:10.1093/aje/kwq478
43. Sohail S, Yu L, Schneider JA, Bennett DA, Buchman AS, Lim ASP. Sleep fragmentation and Parkinson’s disease pathology in older adults without Parkinson’s disease. Mov Disord. 2017;32(12):1729–1737. doi:10.1002/mds.27200
44. Tall P, Qamar MA, Rosenzweig I, et al. The Park Sleep subtype in Parkinson’s disease: from concept to clinic. Expert Opin Pharmacother. 2023;24(15):1725–1736. doi:10.1080/14656566.2023.2242786
45. Paul KC, Chuang Y-H, Shih I-F, et al. The association between lifestyle factors and Parkinson’s disease progression and mortality. Mov Disord. 2019;34(1):58–66. doi:10.1002/mds.27577
46. Fonseca MCM, Sansone D, Farah D, Fiorini AC, Scorza CA, Scorza FA. Seasonality as a risk factor for deaths in Parkinson’s disease. Clinics. 2024;79:100506. doi:10.1016/j.clinsp.2024.100506
47. Jackson CL, Patel SR, Jackson WB II, Lutsey PL, Redline S. Agreement between self-reported and objectively measured sleep duration among white, black, Hispanic, and Chinese adults in the United States: multi-ethnic study of atherosclerosis. Sleep. 2018;41(6). doi:10.1093/sleep/zsy057
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.