Back to Journals » Nature and Science of Sleep » Volume 11
Sleep disturbances in patients with amyotrophic lateral sclerosis: current perspectives
Authors Boentert M ![]()
Received 1 May 2019
Accepted for publication 16 July 2019
Published 9 August 2019 Volume 2019:11 Pages 97—111
DOI https://doi.org/10.2147/NSS.S183504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sutapa Mukherjee
Matthias Boentert
Department of Neurology, University Hospital Muenster, Muenster, Germany
Abstract: Amyotrophic lateral sclerosis (ALS) is a progressive motor neuron disease inevitably leading to generalized muscle weakness and premature death. Sleep disturbances are extremely common in patients with ALS and substantially add to the burden of disease for both patients and caregivers. Disruption of sleep can be caused by physical symptoms, such as muscle cramps, pain, reduced mobility, spasticity, mucus retention, and restless legs syndrome. In addition, depression and anxiety may lead to significant insomnia. In a small subset of patients, rapid eye movement (REM) sleep behavioral disorder may be present, reflecting neurodegeneration of central nervous system pathways which are involved in REM sleep regulation. With regard to overall prognosis, sleep-disordered breathing (SDB) and nocturnal hypoventilation (NH) are of utmost importance, particularly because NH precedes respiratory failure. Timely mechanical ventilation is one of the most significant therapeutic measures to prolong life span in ALS, and transcutaneous capnometry is superior to pulse oxymetry to detect NH early. In addition, it has been shown that in patients on home ventilatory support, survival time depends on whether normocapnia, normoxia, and elimination of apneic events during sleep can be reliably achieved. Several studies have investigated sleep patterns and clinical determinants of sleep disruption in ALS, but exact prevalence numbers are unknown. Thus, constant awareness for sleep-related symptoms is appropriate. Since no curative treatment can be offered to affected patients, sleep complaints should be thoroughly investigated in order to identify any treatable etiology and improve or stabilize quality of life as much as possible. The use of hypnotics should be confined to palliation during the terminal phase and refractory insomnia in earlier stages of the disease, taking into account that most compounds potentially aggravate SDB.
Keywords: amyotrophic lateral sclerosis, sleep disorders, sleep-disordered breathing, non-invasive ventilation, health-related quality of life
Plain language summary
Amyotrophic lateral sclerosis (ALS) is a fatal neurological disease which causes advancing weakness of all muscles. Depending on the muscle involved, patients may suffer from reduced mobility, swallowing difficulties, impaired speech, and finally, respiratory muscle weakness. In patients with ALS, many different problems may cause sleep disturbances. For example, patients cannot turn around in bed any more, or they get pain from being severely immobilized. Many patients have difficulties to fall or stay asleep because of muscle cramps and restless legs. Respiratory muscle weakness is the most important condition which may disturb sleep because it leads to shallow breathing during the night and accumulation of carbon dioxide in the blood. If this is present, life span of ALS patients can be improved by starting non-invasive ventilation (NIV) using a facial mask. This can be even better achieved when NIV is started as early as it becomes necessary. In addition, regular follow-up appointments in a sleep lab help to ensure optimal home ventilation. Sleep disturbances are very common in patients with ALS, and constant awareness for sleep-related complaints is appropriate. Since there is no cure for ALS, it is even more important to systematically look for treatable problems and symptoms in order to improve or maintain quality of life as much as possible. The use of sleep medications should be confined to the last phase of the disease prior to death or to intractable insomnia in earlier stages.
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disorder affecting both the central and peripheral nervous system. The term ALS covers a broad clinical spectrum of different disease manifestations (or rather entities) which share the degeneration of both upper and lower motor neurons.1,2 Upper motor neuron involvement leads to increased muscle tone, spastic paresis and, if the corticobulbar tract is affected, to pseudobulbar palsy. Degeneration of lower motor neurons causes fasciculations, atrophy, and weakness of involved muscles. Virtually all skeletal muscles may be affected, including the extraocular and sphincter externi muscles in later stages of the disease.3,4 In a subset of patients, degeneration of the motor system is accompanied by either mild to moderate cognitive and behavioral abnormalities or overt frontotemporal dementia.5 The prevalence of ALS has been reported to be 5–8/100.000 in industrialized countries, with a peak of disease manifestation between 50 and 70 years of age.6–9 The lifetime risk for ALS may be as high as 1:300 for men and 1:400 for women.10,11
Although vast evidence has been collected on different pathomechanisms leading to motor neuron degeneration,12 no causative treatment is available to date. Only two compounds have been approved for the treatment of ALS, which include riluzole (possibly protecting motor neurons from glutamate excitotoxicity)13–15 and edaravone which has been postulated to scavenge free oxygen radicals.16,17 However, both medications can only be considered as disease-modifying but do not actually halt its progression. Thus, depending on the individual course of the disease, progressive muscle weakness is virtually inevitable in most patients and may finally lead to tetraplegia, chronic respiratory failure, anarthria, and aphagia. Mechanical ventilation, tube feeding, and technically assisted communication are required to prolong life and sustain participation.12,18 Median survival ranges between 2.5–3.5 years after symptom onset, and 1.5–2.5 years following diagnosis.19–21 Among all therapeutic measures, mechanical ventilation and enteral nutrition appear to have a particular impact on life span.21–23 Chronic respiratory failure and pulmonary infections comprise the major causes of death in ALS.24,25
ALS is devastating.26,27 The diagnosis itself confronts affected patients with the bitter prospect of foreseeable morbidity and mortality which can be prevented by no means. Therapeutic options are exclusively symptomatic, and cure is impossible. In the absence of any causative treatment, progression of motor impairment is inevitably associated with functional loss affecting virtually all activities of daily life, including ambulation, nutrition, autonomy, work, and social life. Affected patients get increasingly more dependent on caregivers and technical aids, rendering the entire situation a life-changing challenge for patients and families who constantly have to adapt to the intrinsic dynamics of the disease. For these reasons, clinical research on ALS has long focussed on the quality of life of both patients and caregivers.28–31 In the absence of causative treatment options, symptom alleviation is all that medicine can provide, and a systematic approach to all treatable aspects of the disease is desirable. Among these, sleep and sleep disturbances play a major role for health-related quality of life (HRQoL), psychological health, and everyday life of affected patients.32–37 The aim of this review is to systematically summarize how sleep is directly or indirectly altered in patients with ALS. Based on the current literature and following the International Classification of Sleep Disorders (ICSD-338), ALS-related sleep disturbances will be lined out with regard to clinical presentation, pathophysiology, appropriate diagnostic methods, and treatment options.
Sleep-disordered breathing (SDB)
According to the ICSD-3, SDB mainly comprises sleep apnea and sleep-related hypoventilation.38 Whereas central sleep apnea has only rarely been reported in ALS,39,40 obstructive sleep apnea (OSA) appears to be more common.41 Like in the general population, prevalence of OSA is particularly increased in male patients with ALS.41 OSA is less prevalent in patients with severe bulbar dysfunction than in patients with non-bulbar disease40,41 which possibly reflects the effect of tongue atrophy on upper airway patency. OSA has been proposed to predict survival when it is present prior to the onset of non-invasive ventilation (NIV),42 but this finding may not be independent from hypoventilation (or respiratory muscle weakness, respectively) since both subtypes of SDB often coincide.41–43 Sleep-related hypoventilation mainly relates to progressive weakness of the diaphragm which is caused by bilateral degeneration of phrenic nerve motor neurons. Hypoventilation begins during rapid eye movement (REM) sleep which is accompanied by active inhibition of skeletal muscle activity, including the external intercostal and accessory respiratory muscles.44 Muscle atonia during REM sleep spares the diaphragm, and if diaphragmatic weakness is present, alveolar ventilation is too low to sufficiently exhale carbon dioxide (CO2). In patients with neuromuscular disease or restrictive lung disorders, sleep-related hypoventilation is increasingly defined by capnographic rather than oxymetric measures, since about 30% of patients with manifest hypercapnia will be missed if sleep studies only comprise pulse oxymetry.41,45 As diaphragm weakness progresses, hypercapnia spreads to non-REM (NREM) sleep, and eventually leads to chronic hypercapnic respiratory failure as defined by a daytime CO2 tension exceeding 45 mmHg. Numerous studies have reported direct sequelae of SDB on sleep continuity and composition in patients with ALS. Both hypercapnia and hypoxia may cause awakening from sleep, sleep stage changes or intermittent arousals from sleep as defined by an EEG frequency shift for 3 s or greater in duration.46 In addition, apneas, hypopneas, and respiratory event-related arousals may disrupt sleep independent of impaired gas exchange. In non-ventilated ALS patients, SDB is associated with reduced sleep duration, sleep efficiency, slow-wave sleep, and REM sleep.39,41,47–51 Diaphragm weakness, which underlies nocturnal hypoventilation, is specifically associated with shorter REM sleep duration.51 It can be assumed that CO2 accumulation during REM sleep directly leads to either awakening or a sleep stage shift at least. Furthermore, compensation of diaphragm weakness requires that auxiliary respiratory muscles are recruited (eg, neck muscles or external intercostals), which is usually futile as long as REM sleep-associated muscle atonia persists. Interestingly, ALS patients with significant diaphragm paralysis may show persistent muscle tone during REM sleep in auxiliary respiratory muscles51 reflecting the brain’s attempt to maintain both ventilation and REM sleep. Impairment of objective sleep outcomes clearly relates to the presence of SDB and is less severe in patients in whom nocturnal ventilation is still normal.41,51,52
Symptoms of SDB comprise sleep fragmentation, non-restorative sleep, daytime fatigue, and excessive sleepiness. Morning headache may be present in some patients as a consequence of nocturnal hypercapnia or hypoxia, respectively. Although difficult to quantify in sleep studies, patients often start to compensate for diaphragm weakness and orthopnea during the night by adopting a more or less upright position in bed. Disease-specific tools for self-assessment of sleep quality and daytime performance have not yet been developed. Patient questionnaires covering symptoms suggesting significant fatigue, hypersomnolence, or sleep disruption may be used in conjunction with sleep studies but have not been evaluated with regard to prediction of SDB. Of note, mild OSA or intermittent hypercapnia during sleep may go unnoticed for quite a while which potentially hampers the sensitivity of patient-reported sleep outcomes. In contrast, signs and symptoms of respiratory muscle weakness may be more suitable to raise the suspicion of SDB. However, the Borg dyspnea scale only helps to identify patients with significant inspiratory muscle strength and evolving daytime hypercapnia but has not been used in conjunction with sleep studies.53 Bedside tests of respiratory muscle strength such as FVC, maximum inspiratory pressure (MIP), or sniff nasal inspiratory pressure (SNIP) have extensively been investigated as predictors of survival and disease progression,54–56 but only rarely for prediction of SDB.57,58 Interestingly, the latter two studies both revealed that SNIP might be most useful in this context. However, since indication criteria for NIV in patients with neuromuscular disease comprise reduction of FVC or MIP, these tests should be regularly performed as a screening procedure. For practical reasons, SNIP measurement (which is more laborious and variable in results) may be restricted to patients with weakness of mouth closure.59,60
Only in a small subset of patients respiratory muscle weakness and sleep-related hypoventilation may be the presenting symptom of ALS.61,62 In the vast majority of patients, respiratory muscle dysfunction slowly evolves during the course of the disease and then accompanies constant deterioration of motor function. Nocturnal hypercapnia may be detectable long before patients complain of sleep disruption or daytime dyspnea.63 Thus, routine evaluation of sleep-related breathing is recommendable even if subjective sleep quality is still unaffected. This holds true because NIV has been shown to have a substantial impact on overall prognosis, and there is growing evidence that early initiation of NIV is of particular importance (see below). In addition, NIV has been reported to improve or stabilize HRQoL in patients with ALS. In other words: from the moment on when indication criteria for NIV are met, and if the patient is willing to receive home ventilatory support, the initiation and long-term maintenance of mechanical ventilation is one of the most meaningful therapeutic measures which can ever be taken. Numerous retrospective studies and one randomized trial revealed that NIV improves life expectancy in patients with ALS.20,23,64–75 Moreover, prolongation of survival time is longer when NIV is started already in patients with only mild or near-normal vital capacity.76 Thus, constant awareness of treating physicians for the “respiratory issue” and low-threshold initiation of adequate diagnostic measures directly impact patients’ prognosis. In order to detect sleep-related hypoventilation with the highest sensitivity possible, sleep studies in ALS patients should preferably comprise transcutaneous capnometry which sufficiently substitutes for nighttime arterial blood gases77 and has been shown to be superior to pulse oximetry.41,45,78 In up to one-third of neuromuscular patients with definite hypoventilation (ie, nighttime hypercapnia), peripheral oxygen saturation is normal (Figure 1).
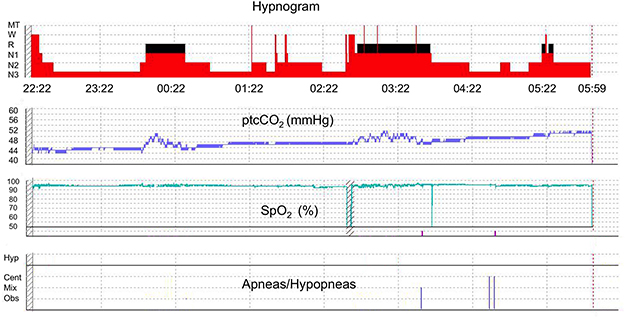 |
Figure 1 Polysomnography synopsis from a 67-year-old non-ventilated male patient with spinal onset ALS. The figure depicts four tracings representing hypnogram, transcutaneous capnometry, pulse oxymetry, and graphical presentation of apneas or hypopneas (from top to bottom). Whereas capnometry shows hypercapnia which begins during REM and persists during the last third of the night, peripheral oxygen saturation is normal throughout the entire recording.Abbreviations: ALS, amyotrophic lateral sclerosis, REM/R, rapid eye movement sleep, W, wake, N1 - N3, non-REM sleep stages, ptcCO2, transcutaneous carbon dioxide tension, SpO2, peripheral oxygen saturation, Hyp, hypopneas, Cent/Mix/Obs, central/mixed/obstructive apneas. |
Of note, for baseline evaluation of sleep and suspected SDB, full polysomnography (PSG) is generally recommended.79 In contrast to mere polygraphy, PSG allows to exactly assign transient hypercapnia to REM sleep, facilitating to detect sleep-related hypoventilation. In addition, only PSG reveals objective sleep quality and architecture, which is particularly important in early stages of the disease when SDB may not yet be present or does not yet predominate other causes of sleep disruption. Sleep fragmentation may not only render sleep non-restorative, but may also worsen SDB, and should be specifically sought for. Independent on ALS, sleep disruption is known to be an independent risk factor for cardiovascular mortality.80 Furthermore, patients with ALS may often be unaware of sleep problems in early stages of the condition,81 and low-threshold detection of evolving sleep disturbances by PSG may steer treatment planning and scheduling follow-up sleep studies.
Following initiation of NIV, objective sleep outcomes and nocturnal ventilation may rapidly enhance (Figure 2). Long-term NIV has been shown to improve not only prognosis but also sleep quality and HRQoL in patients with ALS and respiratory failure.47,49,82–84 This holds true despite the fact that ventilator-dependency constantly increases with time. Initiation of NIV requires optimal mask fitting, thorough titration of respirator settings, and education of both patients and caregivers, with all of these measures aiming to improve – and not to additionally worsen – the patient’s condition or quality of life. The choice of interface may substantially influence treatment adherence. Nasal masks are supposed to be less uncomfortable but may prove insufficient and sleep-disturbing when mouth leaks occur.85 This can be circumvented by oronasal interfaces, bearing in mind that they may promote pressure-induced upper airway obstruction.86 In this case, adjustment of the expiratory positive airway pressure (EPAP) or combining a nasal mask with a chin strap may solve the problem.86 One previous study suggests that EPAP itself may be associated with worse sleep quality in ALS patients87 but did not specifically address that effective treatment of OSA is likely to be more meaningful. Patient-ventilator asynchrony may also impair sleep quality and is probably common, but its impact on treatment adherence or clinical outcomes has not been investigated.88 For NIV, bi-level ventilation modes are used in order to ensure sufficient alveolar ventilation and compensation for air leaks. Preset volume support ventilation has been shown to be more effective in terms of gas exchange and symptom alleviation.89 Regular follow-up evaluation including polygraphy (at least) and capnometry is highly recommendable since several studies have shown that overall prognosis may be negatively affected in patients with ALS and other neuromuscular disorders when NIV fails to achieve its primary goals: normocapnia, normoxia, and normalization of the apnea-hypopnea index.90–92 Accordingly, ventilator settings should be adjusted if necessary. Education of patients and caregivers is a prerequisite of good treatment adherence.93 Both indication and aims of NIV should be discussed, along with handling issues, communicational and nutritional aspects. Once NIV has been started, extension of ventilator use during daytime will be inevitable over time, and tracheostomy as well as end-of-life scenarios should be addressed early.
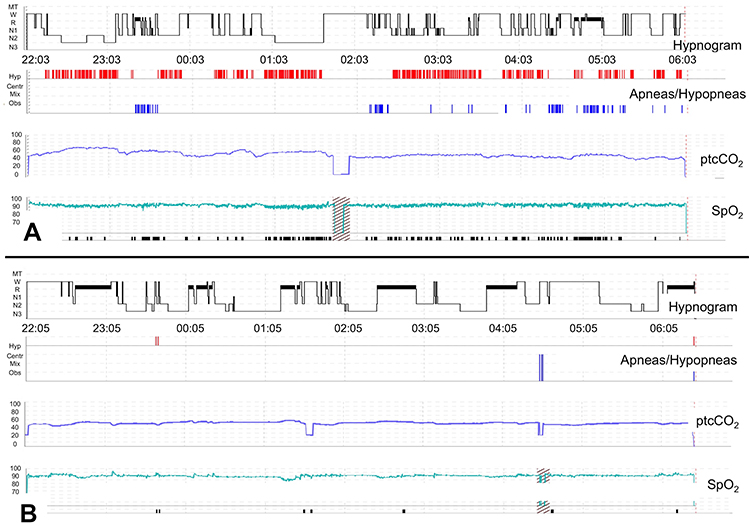 |
Figure 2 Polysomnography synopses from a 61-year-old non-ventilated patient with spinal onset ALS and clinically apparent respiratory muscle weakness before and after initiation of non-invasive ventilation (NIV). Both panels depict hypnogram, graphical presentation of apneas and hypopneas, transcutaneous capnometry, and pulse oxymetry (from top to bottom). (A) Sleep fragmentation with reduced sleep efficiency (65.6%), N3 percentage (13.3%), and REM percentage (6.1%). Sleep-disordered breathing is present, comprising severe obstructive sleep apnea (AHI 83.8/h, mean SpO2 88%) and nocturnal hypoventilation (mean ptcCO2 54.0 mmHg, maximum ptcCO2 63.7 mmHg). (B) Rapid improvement of objective sleep outcomes in the very first night of NIV treatment. Normalization of the AHI (0.3/h) and improvement of both CO2 elimination and oxygenation are evident (mean ptcCO2 52.0 mmHg, maximum ptcCO2 55.8 mmHg, mean SpO2 91%). In parallel, sleep architecture shows substantial increase of N3 and REM percentages (25.3% and 26.9%, respectively). Note that sleep-onset REM is present at the beginning of the night.Abbreviations: W, wake, R/REM, rapid eye movement sleep, N1-N3, non-REM sleep stages, ptcCO2, transcutaneous carbon dioxide tension, SpO2, peripheral oxygen saturation. |
There is conflicting evidence whether patients with bulbar ALS benefit from NIV or not, and formerly, initiation of NIV in this population was even discouraged considering a potential aspiration risk. Previous studies did not prove NIV to prolong survival in patients with bulbar dysfunction,69 which is contradicted by more recent evidence.94 In addition, several studies have reported improvement of HRQoL69 and sleep quality47,49 also in this subgroup, making it recommendable to generally offer NIV also to patients with bulbar ALS and respiratory failure, with a special focus on the individual situation and the extent of dysphagia.
Apart from hypoventilation and sleep apnea, nocturnal breathing in patients with ALS may be disturbed by recurrent laryngospasms which may occur either spontaneously or in response to gastro-oesophageal reflux.95,96 Another condition potentially causing nocturnal dyspnea is mucus retention which is particularly common in patients with poor bulbar function. Here, assisted coughing, mechanical insufflators/exsufflators, or suction of the upper airway may help alleviate the problem.
Sleep-related leg muscle cramps and fasciculations
Degeneration of the lower motoneurons causes fasciculations in skeletal muscles which may be reported to disrupt sleep by some patients.97 It may also lead to painful muscle cramps which often occur during the night and predominantly affect the lower limbs, then referred to as nocturnal leg muscle cramps. These have been reported to occur in the vast majority of ALS patients, causing substantial morbidity in affected individuals.98 Prevalence numbers range between 45% and 92%.35,99 Muscle cramps may also occur in intrinsic hand muscles or the abdominal wall musculature, but it is not known whether these are especially common during the night. Muscle cramps are likely to occur more frequently in patients with spinal disease manifestation.99 Electrophysiologically, muscle cramps result from anterior horn cells or motor units that discharge at a much higher frequency (>300 Hz) than with normal voluntary contraction.100 Discharge ceases spontaneously or after active stretching of the affected muscle group, but the latter maneuver may be hampered if limb weakness is present. Nocturnal or daytime muscle cramps should be actively asked for, and treatment options should be thoroughly discussed if significant symptom burden is obvious. For alleviation of muscle cramps, various measures may be considered. Electrolyte imbalances or lack of fluids should be treated adequately. Any medication possibly enhancing muscle cramps (eg, statins) should be critically checked and discontinued, if acceptable. Stretching of affected muscle groups is often recommended for prevention of muscle cramps, but the respective evidence is scarce even for otherwise healthy subjects101 and no ALS-specific studies have been published. For pharmacological treatment, mexiletine 150 mg twice daily may be considered since it has recently been shown to improve symptoms in a randomized controlled trial.102 Numerous other compounds including baclofen, memantine, vitamin E, and L-threonine have failed to show significant effects on muscle cramps in patients with ALS.103 The effects of quinidine (usually 200–300 mg at night) have been extensively evaluated in various non-ALS conditions, with moderate evidence that cramp intensity, and possibly frequency, are reduced.104 However, long-term quinidine is not recommended because of possible side effects and significant safety concerns.105
Immobilization
For healthy subjects, it is normal to repeatedly change position in bed during sleep. Under physiological conditions, this may occur up to 1.6 times per hour on average.106 If motor function declines in patients with ALS, it inevitably becomes more and more difficult to change position, perform comfort movements, or adjust bedclothes. These problems have rarely been evaluated systematically, but significant impact on sleep quality is both likely and comprehensible.36 Immobilization may promote nocturnal discomfort, pain, and dependency on caregivers. In addition, patients are at risk of skin lesions,107 which are possibly not less common in ALS than in other neurological conditions as previously thought (based on the observation that intradermal collagen density in the sacral region is increased in ALS patients).108,109
Nocturnal pain
In both health and disease, pain and sleep quality are closely related or rather mutually intertwined since pain disrupts sleep and impaired sleep promotes both the occurrence and exacerbation of pain.110,111 In patients with ALS, acute or recurrent pain may result from muscle cramps, spasticity, or immobilization, especially if bones and joints are rendered vulnerable to pressure because of progressive muscular atrophy. This kind of pain is often clearly localized by affected patients, nociceptive in nature and mostly secondary to a known cause or mechanism. In addition, ALS patients may experience neuropathic pain which is often more diffuse and “typically neuropathic” (eg, burning, tingling or lancinating if occurring spontaneously, and dysaesthetic if evoked by tactile stimuli). This type of pain usually cannot be attributed to a specific cause other than impairment of somatosensory pathways. However, neuropathic pain appears to be relatively uncommon in ALS112,113 although intraepidermal nerve fiber density is decreased in up to 75% of patients suggesting small fiber neuropathy as an immanent neuropathological feature of the disease.114 As in other conditions characterized by chronic pain, the concept of central sensitization may apply to a third kind of pain potentially occurring in ALS: diffuse, non-neuropathic, almost permanent and obviously inexplicable by nociceptive triggers.115 Central sensitization is characterized by an abnormally enhanced nociceptive response within the central nervous system. This results in pain perceptions triggered by central amplification of non-painful sensory inputs instead of clearly noxious stimuli.116 Little is known about the frequency and clinical determinants of central sensitization pain in ALS but some patients appear to be affected and are extremely difficult to treat. Studies specifically focussing on nocturnal pain in ALS are lacking, and treatment recommendations do not differentiate between daytime and sleep-related pain.117 In addition, real-life management of pain in patients with ALS is generally based on clinical experience rather than evidence-based guidelines. Nociceptive pain may respond to both adequate preventive measures (eg, positional aids, special mattresses) and non-steroidal anti-inflammatory drugs (eg, ibuprofen, metamizole) or acetaminophen, respectively. Opioids may be added in patients with otherwise intractable pain or advanced disease, especially if respiratory muscle weakness and dyspnea are present. Cannabis may also prove effective, with additional anxiolytic, sedating and appetite-enhancing features. If neuropathic or central sensitization pain is likely to be present, α2δ ligands (gabapentin, pregabalin) or tricyclic antidepressants should be considered. Pain resulting from spasticity may respond to central muscle relaxants, such as baclofen, tizanidine, or tolperisone. All of these compounds also have sedating effects, making it prudent to start with an evening dose.
In summary, pain of whatever etiology is a common complaint in ALS patients, and sleep disruption is likely to occur consecutively. Both pain and sleep disturbances substantially impair quality of life, which is underlined by the observation that in advanced disease, they predominantly determine the interest in assisted suicide if this is a legalized option.118 Thus, adequate pain relief is crucial in medical care for ALS patients throughout the course of the disease, and the impact of pain on sleep quality should be regarded with special interest.
Restless legs syndrome (RLS) and periodic limb movements (PLM) in sleep
The diagnosis of RLS is based on five essential criteria.38 These include: 1) an urge to move the legs (facultatively accompanied by unpleasant or even painful sensations in the lower extremities), 2) onset or exacerbation of these symptoms during rest or inactivity, 3) occurrence or worsening of symptoms in the evening or during the night, 4) symptom relief during voluntary movement such as walking or stretching, and 5), symptoms (1)–(4) cannot be explained by another medical or behavioral condition (eg neuropathic pain, leg muscle cramps, venous stasis, or habitual foot tapping). Prevalence of RLS in the general population is around 10%, with women more often affected than men,119 and clinical severity may considerably vary from mild or rare symptoms not causing any sleep disturbances to frequent and profound impairment of sleep and quality of life.120 Only few studies systematically investigated the prevalence and clinical determinants of RLS in patients with ALS.121–123 In all studies, RLS was significantly more common in ALS patients than in control subjects or the general population, respectively. Prevalence numbers ranged from 14.6% to 25%, and in one study, ALS patients with RLS reported a shorter history of complaints compared to control subjects with RLS.123 This finding may support the notion that progressive immobilization simply puts ALS patients at a greater risk to develop RLS. Indeed, the same study found that RLS severity was associated with motor impairment in affected patients, and Limousin et al reported that ALS patients with RLS had more difficulties to turn in bed than RLS-negative patients.121 It is not exactly known whether mild involvement of sensory nerve fibers or small fiber neuropathy – which may be present in a subset of patients114,124,125 – contribute to RLS in ALS.
Physicians should actively ask for RLS symptoms in order not to miss a condition for which effective treatment can be offered. With regard to pharmacological options, iron deficiency should be looked for and corrected according to standard recommendations.126 Long-term dopaminergic medication should only be established if the diagnosis of RLS can be ascertained by thorough distinction from myalgias, leg muscle cramps, calf edema, or neuropathic pain, and the risk of augmentation has always to be considered.127 If augmentation has occurred, or if symptoms appear to overlap with alternative etiologies, α2δ ligands are adequate for first-line treatment. In patients with severe RLS and concomitant chronic pain, opioids should be considered.
PLM in sleep have only rarely been investigated in patients with ALS. Whereas one study reported similar PLM parameters in ALS patients and healthy control subjects,128 another study showed that a PLM index above 15 per hour was significantly more common in ALS patients than in controls.129 Moszynski et al postulated that an increased PLM index above 5 per hour of total sleep time is associated with worse prognosis.130 However, all of these studies did not further report whether PLM had an impact on objective sleep. Unpublished data from a PSG-based cohort study in 150 ALS patients showed a mean PLM index of 24.0±41.7 (0–218.5), and one-third of patients had a PLM index above 15/h.41 However, the mean PLM arousal index was only 3.6±8.6 (0–58.2). PLM parameters showed no correlation with the ALS functional rating scale score,131 sleep efficiency, or the percentage of slow-wave sleep.41 More exact prevalence numbers have not been reported, the proportion of patients in whom PLM in sleep and RLS coincide is unknown, and in particular, it is unclear whether isolated PLM (ie, with no or few associated arousals) are clinically significant at all regarding the plethora of sleep-disrupting factors in ALS (Figure 3). From a pathophysiological rather than clinical perspective, it remains an interesting question whether PLM in ALS reflect spinal cord disinhibition and hyperexcitability caused by degeneration of inhibitory descending central pathways.132
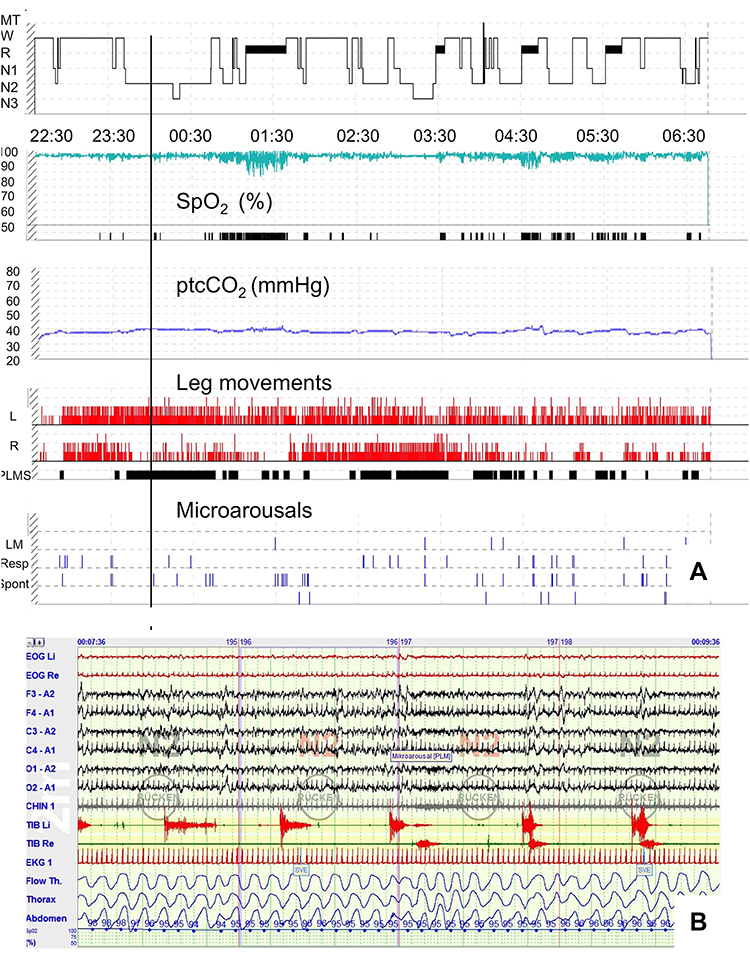 |
Figure 3 Periodic limb movements in sleep in a 62-year-old, non-ventilated patient with spinal onset ALS. (A) A polysomnography synopsis including hypnogram, oxygen saturation, transcutaneous ptcCO2, and graphical presentation of both leg movements (LM), and (micro)arousals from sleep (from top to bottom). Whereas capnometry is normal throughout the night, isolated obstructive sleep apnea is present leading to persistent desaturations (AHI 39.8/h). Almost permanent leg movements can be seen in both legs with long-lasting periodicity as reflected by the black bars within the fourth panel from above (PLMS). The PLM index was 117.1/h. However, only few PLM were associated with arousals from sleep, resulting in a PLM arousal index of no more than 5.4/h. (B) A 2-min excerpt from the same polysomnography with the timepoint according to the vertical black line in (A). Sleep stage is N2, and sleep-disordered breathing is absent. Only one of the 8 PLM which can be seen in the electromyography tracings (TIB L and TIB R, respectively) relates with an EEG arousal.Abbreviations: ALS, amyotrophic lateral sclerosis, PLM, periodic limb movemements, ptcCO2, transcutaneous carbon dioxide tension, SpO2, peripheral oxygen saturation, W, wake, R/REM, rapid eye movement sleep, N1-N3, non-REM sleep stages, LM, limb movements, L, left leg, R, right leg, TIB, tibialis anterior muscle, AHI, apnoea hypopnea index. |
Parasomnias
Parasomnias comprise abnormal movements, behaviors, perceptions or emotions, which arise from sleep, or occur on falling asleep or waking up, respectively. In fact, parasomnias can be regarded as dissociated sleep states characterized by partial arousals from either REM sleep or NREM sleep.38 There is no evidence supporting the notion that NREM parasomnia is a frequent finding in patients with ALS, and sleepwalking, pavor nocturnus or confusional arousals have not been specifically reported in this population.
REM behavioral disorder (RBD) is characterized by persistent phasic or tonic muscle activation during REM sleep that is detectable by means of surface electromyogram (EMG) and has been referred to as REM sleep without atonia. This reflects dysfunction or degeneration of the ponto-spinal pathway which physiologically blocks motor impulses during REM sleep.133 As a result, patients with manifest RBD show dream-enacting behavior which puts them at risk of bed falls and injuries.38 Furthermore, aggressive behavioral abnormalities may involve the bed partner. RBD is strongly associated with neurodegenerative disorders, including Parkinson’s disease, dementia with Lewy bodies, and multisystem atrophy. Idiopathic – or rather isolated – RBD is considered as an early manifestation of these conditions.134 Whereas the association between α-synucleinopathies and RBD has extensively been confirmed,135,136 neurodegenerative disorders with different neuropathological features seem to give a more inconsistent picture. RBD is an obligatory symptom in anti-IgLON5 disease which is a rare tauopathy recently described.137,138 In clinically diagnosed Alzheimer’s disease (AD), it appears to be rather uncommon,139 but a small proportion of patients with idiopathic RBD may develop AD or overlap dementia (122). These findings suggest that RBD is not exclusively restricted to α-synuclein pathology, and further evidence for this comes from several reports on patients with a “mixed“ pattern of either protein deposits or clinical presentation including individuals with anti-IgLON5 disease, parkinsonism-dementia-ALS complex, ALS due to one distinct SOD1 gene mutation, and frontotemporal dementia.140–143 In addition, one study including 344 RBD patients found two individuals carrying the C9orf72 repeat expansion, both showing parkinsonism but no signs of ALS or FTD.144 Only few studies have investigated EMG characteristics and behavior during REM sleep in larger cohorts of ALS patients. Puligheddu et al found the REM atonia index to be lower and the number of chin movements per hour of sleep to be higher in 29 ALS patients than in healthy controls.128 Both parameters showed significant correlation with the ALS-FRS-R score, suggesting that more severe motor impairment reflects more advanced neurodegeneration which also involves REM sleep-regulating pathways. However, this assumption remains unproven since only the chin EMG was quantitatively analyzed. Fasciculations, snoring and even artifacts triggered by NIV may impede interpretation of the chin EMG, and no information on sleep-related breathing or mask therapy was provided in this study. In addition, quantitative evaluation of motor activity during REM sleep requires standardized analysis of EMG tracings bilaterally recorded from distinct upper and lower extremity muscles.145 In a cohort of 41 ALS patients who underwent video PSG, Lo Coco et al found two individuals with manifest RBD and another two showing isolated REM sleep without atonia as defined by chin and leg muscle EMG recordings.129
The existing literature on RBD in ALS is still scarce, and further systematic studies are desirable. From the current evidence, it may be deduced that RBD can be present in a small subset of patients. This observation suggests that RBD, although more frequent in α-synucleinopathies, might comprise a pathologically distinct stage in different neurodegenerative disorders where neurodegeneration involves the pathways that regulate muscle tone during REM sleep.
If RBD is present in a patient with ALS and treatment is indicated, measures should be taken to prevent injuries and to decrease the probability of arousals from REM sleep. The latter approach may include that SDB should be treated first. If pharmacological treatment is considered necessary, clonazepam (0.25–2.0 mg) or melatonin (3–12 mg), both given at bedtime, are recommendable although high-quality evidence is still lacking.146
Insomnia
There are numerous reasons for which patients with ALS may suffer from persistent sleep disturbances. As a result, sleep often gets chronically non-restorative, which worsens daytime performance in addition to motor symptoms. SDB as a possible cause of sleep disruption has extensively been discussed further above. Also pain, muscle cramps, and RLS may significantly reduce patients’ ability to fall asleep in the evening or to maintain sleep throughout the night. Immobilization is very likely to impair sleep quality since it may hinder patients to turn around in bed, to adjust their bedclothes, or scratch themselves when they feel any pruritus. As long as these simple acts are naturally unimpaired one can only imagine how much the resulting sleep disturbances impact overall well-being. In addition, it has to be acknowledged that insomnia is extremely common in patients with ALS.33,147 However, only very few studies have investigated this in detail, and little is known about the exact prevalence of distinct sleep-disrupting factors. Furthermore, insomnia may be present not only because of physical complaints, but also due to stressful cognitions ranging from general solicitude to existential fears. Finally, the mutual relationship between depression and insomnia is likely to play a role, building an alternative basis for sleep quality impairment in ALS patients.148,149
Sedatives in patients with ALS
Sedatives, namely benzodiazepines and opioids, undoubtedly have their place among symptomatic treatment options that can be offered to ALS patients, and they are absolutely indispensable when it comes to palliative care in the terminal phase.150,151 This holds particularly true if respiratory failure is present and mechanical ventilation was either not consented for, is not feasible anymore, or is going to be terminated according to the patient’s will.152 However, it is important that sedatives are not considered as an “all-purpose medication” for insomnia earlier in the course of the disease when treating physicians or patients themselves might perceive the de facto situation as already palliative. This would bear the risk that sleep disturbances or pain (for which benzodiazepines or opioids are mostly prescribed prior to the terminal phase) are not retraced to the distinct etiology that is potentially underlying. Most importantly, SDB could unknowingly be aggravated.153 Thus, it is an ongoing challenge to regularly investigate the causes of sleep disruption and pain in every individual patient in order to identify conditions in which alternative treatments should be established first. If benzodiazepines can reasonably be considered to alleviate insomnia, short-acting compounds are strongly recommended to prevent carry-over effects that might add to daytime sleepiness.
Conclusion
Sleep disturbances deserve to be recognized as a major aspect of morbidity in patients with ALS. In addition to progressive motor impairment, nutritional problems and loss of communication, sleep disruption and its sequelae substantially add to the burden of disease for patients and caregivers. Thus, treating physicians should regularly ask for sleep-related symptoms, thoroughly inquire potential causes, and initiate adequate treatment. With regard to both morbidity and mortality, SDB is the most important consequence of ALS for sleep. Its early recognition by adequate diagnostic measures is crucial in order to enable patients to benefit from mechanical ventilation as much as even possible. Beyond the obvious importance of SDB, sleep may be disrupted by a number of other causes, including immobilization, muscle cramps, pain, RLS, depression, and, at least occasionally, RBD. These conditions should be routinely taken into account since appropriate treatment may substantially improve sleep quality, mood, and HRQoL which are all crucial for patients’ ability to withstand the disease and maintain the will to live as long as they can or want to.154
Abbreviations
AHI, apnea hypopnea index; ALS, amyotrophic lateral sclerosis; ALS-FRS-R, ALS functional rating scale (revised); CO2, carbon dioxide; EMG, electromyography; EPAP, expiratory positive airway pressure; HRQoL, health-related quality of life; MIP, maximum inspiratory pressure; NIV, non-invasive ventilation; OSA, obstructive sleep apnea; PLM, periodic leg movements; PSG, polysomnography; RBD, REM sleep behavioral disorder; REM, rapid eye movement; RLS, restless legs syndrome; SDB, sleep-disordered breathing; SNIP, sniff nasal inspiratory pressure.
Disclosure
Dr Matthias Boentert reports grants from Sanofi-Genzyme GmbH and Loewenstein Medical GmbH, outside the submitted work, and no other conflicts of interest in this work.
References
1. Grad LI, Rouleau GA, Ravits J, Cashman NR. Clinical spectrum of amyotrophic lateral sclerosis (ALS). Cold Spring Harb Perspect Med. 2017;7:8. doi:10.1101/cshperspect.a024117
2. Hardiman O, Al-Chalabi A, Chio A, et al. Amyotrophic lateral sclerosis. Nat Rev Dis Primers. 2017;3:17071. doi:10.1038/nrdp.2017.71
3. Mizutani T, Aki M, Shiozawa R, et al. Development of ophthalmoplegia in amyotrophic lateral sclerosis during long-term use of respirators. J Neurol Sci. 1990;99(2–3):311–319.
4. Carvalho M, Schwartz MS, Swash M. Involvement of the external anal sphincter in amyotrophic lateral sclerosis. Muscle Nerve. 1995;18(8):848–853. doi:10.1002/mus.880180808
5. Hortobagyi T, Cairns NJ. Amyotrophic lateral sclerosis and non-tau frontotemporal lobar degeneration. Handb Clin Neurol. 2017;145:369–381. doi:10.1016/B978-0-12-802395-2.00026-2
6. Nakken O, Lindstrom JC, Tysnes OB, Holmoy T. Assessing amyotrophic lateral sclerosis prevalence in Norway from 2009 to 2015 from compulsory nationwide health registers. Amyotroph Lateral Scler Frontotemporal Degener. 2018;19(3–4):303–310. doi:10.1080/21678421.2017.1418004
7. Kab S, Moisan F, Preux PM, Marin B, Elbaz A. Nationwide incidence of motor neuron disease using the French health insurance information system database. Amyotroph Lateral Scler Frontotemporal Degener. 2017;18(5–6):426–433. doi:10.1080/21678421.2017.1306566
8. Rosenbohm A, Peter RS, Erhardt S, et al. Epidemiology of amyotrophic lateral sclerosis in Southern Germany. J Neurol. 2017;264(4):749–757. doi:10.1007/s00415-017-8413-3
9. Ragonese P, Cellura E, Aridon P, et al. Incidence of amyotrophic lateral sclerosis in Sicily: a population based study. Amyotroph Lateral Scler. 2012;13(3):284–287. doi:10.3109/17482968.2012.662689
10. Chio A, Mora G, Calvo A, Mazzini L, Bottacchi E, Mutani R. Epidemiology of ALS in Italy: a 10-year prospective population-based study. Neurology. 2009;72(8):725–731. doi:10.1212/01.wnl.0000343008.26874.d1
11. Alonso A, Logroscino G, Jick SS, Hernan MA. Incidence and lifetime risk of motor neuron disease in the United Kingdom: a population-based study. Eur J Neurol. 2009;16(6):745–751.
12. Foster LA, Salajegheh MK. Motor neuron disease: pathophysiology, diagnosis, and management. Am J Med. 2019;132(1):32–37. doi:10.1016/j.amjmed.2018.07.012
13. Lacomblez L, Bensimon G, Leigh PN, et al. A confirmatory dose-ranging study of riluzole in ALS. ALS/Riluzole Study Group-II. Neurology. 1996;47(6 Suppl 4):S242–S250. doi:10.1212/wnl.47.6_suppl_4.242s
14. Lacomblez L, Bensimon G, Leigh PN, Guillet P, Meininger V. Dose-ranging study of riluzole in amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis/Riluzole Study Group II. Lancet. 1996;347(9013):1425–1431. doi:10.1016/s0140-6736(96)91680-3
15. Bensimon G, Lacomblez L, Meininger V. A controlled trial of riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study Group. N Engl J Med. 1994;330(9):585–591. doi:10.1056/NEJM199403033300901
16. Writing Group On Behalf Of The Edaravone Als 18 Study G. Exploratory double-blind, parallel-group, placebo-controlled study of edaravone (MCI-186) in amyotrophic lateral sclerosis (Japan ALS severity classification: grade 3, requiring assistance for eating, excretion or ambulation). Amyotroph Lateral Scler Frontotemporal Degener. 2017;18(sup1):40–48. doi:10.1080/21678421.2017.1361441
17. Takei K, Takahashi F, Liu S, Tsuda K, Palumbo J. Post-hoc analysis of randomised, placebo-controlled, double-blind study (MCI186-19) of edaravone (MCI-186) in amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. 2017;18(sup1):49–54. doi:10.1080/21678421.2017.1361443
18. Andersen PM, Abrahams S, Borasio GD, et al. EFNS guidelines on the clinical management of amyotrophic lateral sclerosis (MALS)–revised report of an EFNS task force. Eur J Neurol. 2012;19(3):360–375. doi:10.1111/j.1468-1331.2011.03501.x
19. Traxinger K, Kelly C, Johnson BA, Lyles RH, Glass JD. Prognosis and epidemiology of amyotrophic lateral sclerosis: analysis of a clinic population, 1997–2011. Neurol Clin Pract. 2013;3(4):313–320. doi:10.1212/CPJ.0b013e3182a1b8ab
20. Zoccolella S, Beghi E, Palagano G, et al. Analysis of survival and prognostic factors in amyotrophic lateral sclerosis: a population based study. J Neurol Neurosurg Psychiatry. 2008;79(1):33–37. doi:10.1136/jnnp.2007.118018
21. Calvo A, Moglia C, Lunetta C, et al. Factors predicting survival in ALS: a multicenter Italian study. J Neurol. 2017;264(1):54–63. doi:10.1007/s00415-016-8313-y
22. Piepers S, van Den Berg JP, Kalmijn S, et al. Effect of non-invasive ventilation on survival, quality of life, respiratory function and cognition: a review of the literature. Amyotroph Lateral Scler. 2006;7(4):195–200. doi:10.1080/14660820500514974
23. Kleopa KA, Sherman M, Neal B, Romano GJ, Heiman-Patterson T. Bipap improves survival and rate of pulmonary function decline in patients with ALS. J Neurol Sci. 1999;164(1):82–88.
24. Spataro R, Re M L, Piccoli T, Piccoli F, La Bella V. Causes and place of death in Italian patients with amyotrophic lateral sclerosis. Acta Neurol Scand. 2010;122(3):217–223. doi:10.1111/j.1600-0404.2009.01290.x
25. Gil J, Funalot B, Verschueren A, et al. Causes of death amongst French patients with amyotrophic lateral sclerosis: a prospective study. Eur J Neurol. 2008;15(11):1245–1251. doi:10.1111/j.1468-1331.2008.02307.x
26. Oliveira AS, Pereira RD. Amyotrophic lateral sclerosis (ALS): three letters that change the people’s life. For Ever Arq Neuropsiquiatr. 2009;67(3A):750–782. doi:10.1590/S0004-282X2009000400040
27. Motor Neuron Disease Association, 2009. Available from: https://www.youtube.com/watch?v=4b-h_XBArC4. Accessed March 15, 2019.
28. Bourke SC, McColl E, Shaw PJ, Gibson GJ. Validation of quality of life instruments in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord. 2004;5(1):55–60. doi:10.1080/14660820310016066
29. Bromberg MB. Quality of life in amyotrophic lateral sclerosis. Phys Med Rehabil Clin N Am. 2008;19(3):
30. Epton J, Harris R, Jenkinson C. Quality of life in amyotrophic lateral sclerosis/motor neuron disease: a structured review. Amyotroph Lateral Scler. 2009;10(1):15–26. doi:10.1080/17482960802163721
31. Burke T, Galvin M, Pinto-Grau M, et al. Caregivers of patients with amyotrophic lateral sclerosis: investigating quality of life, caregiver burden, service engagement, and patient survival. J Neurol. 2017;264(5):898–904. doi:10.1007/s00415-017-8448-5
32. Raheja D, Stephens HE, Lehman E, Walsh S, Yang C, Simmons Z. Patient-reported problematic symptoms in an ALS treatment trial. Amyotroph Lateral Scler Frontotemporal Degener. 2016;17(3–4):198–205. doi:10.3109/21678421.2015.1131831
33. Panda S, Gourie-Devi M, Sharma A. Sleep disorders in amyotrophic lateral sclerosis: a questionnaire-based study from India. Neurol India. 2018;66(3):700–708. doi:10.4103/0028-3886.232327
34. Lo Coco D, La Bella V. Fatigue, sleep, and nocturnal complaints in patients with amyotrophic lateral sclerosis. Eur J Neurol. 2012;19(5):760–763. doi:10.1111/j.1468-1331.2011.03637.x
35. Lo Coco D, Mattaliano P, Spataro R, Mattaliano A, La Bella V. Sleep-wake disturbances in patients with amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2011;82(8):839–842. doi:10.1136/jnnp.2010.228007
36. Diaz-Abad M, Buczyner JR, Venza BR, et al. Poor sleep quality in patients with amyotrophic lateral sclerosis at the time of diagnosis. J Clin Neuromuscul Dis. 2018;20(2):60–68. doi:10.1097/CND.0000000000000234
37. Ahmed RM, Newcombe RE, Piper AJ, et al. Sleep disorders and respiratory function in amyotrophic lateral sclerosis. Sleep Med Rev. 2016;26:33–42. doi:10.1016/j.smrv.2015.05.007
38. American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd edition (ICSD-3). Westchester, IL. American Academy of Sleep Medicine; 2014.
39. Ferguson KA, Strong MJ, Ahmad D, George CF. Sleep-disordered breathing in amyotrophic lateral sclerosis. Chest. 1996;110(3):664–669. doi:10.1378/chest.110.3.664
40. Santos C, Braghiroli A, Mazzini L, Pratesi R, Oliveira LV, Mora G. Sleep-related breathing disorders in amyotrophic lateral sclerosis. Monaldi Arch Chest Dis. 2003;59(2):160–165.
41. Boentert M, Glatz C, Helmle C, Okegwo A, Young P. Prevalence of sleep apnoea and capnographic detection of nocturnal hypoventilation in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2018;89(4):418–424. doi:10.1136/jnnp-2017-316515
42. Quaranta VN, Carratu P, Damiani MF, et al. The prognostic role of obstructive sleep apnea at the onset of amyotrophic lateral sclerosis. Neurodegener Dis. 2017;17(1):14–21. doi:10.1159/000447560
43. Lyall RA, Donaldson N, Polkey MI, Leigh PN, Moxham J. Respiratory muscle strength and ventilatory failure in amyotrophic lateral sclerosis. Brain. 2001;124(Pt 10):2000–2013. doi:10.1093/brain/124.10.2000
44. Berger KIRDM, Ayappa I, Goldring RM. Pathophysiology of hypoventilation during sleep. Sleep Med Clin. 2014;9:289–300. doi:10.1016/j.jsmc.2014.05.014
45. Ogna A, Quera Salva MA, Prigent H, et al. Nocturnal hypoventilation in neuromuscular disease: prevalence according to different definitions issued from the literature. Sleep Breath. 2016;20(2):575–581. doi:10.1007/s11325-015-1247-2
46. Berry RBBR, Gamaldo CE, Harding SM, Lloyd RM, Marcus CL, Vaughn BV; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.2. Darien, Illinois: American Academy of Sleep Medicine; 2015. Available from: http://www.aasmnet.org.
47. Boentert M, Brenscheidt I, Glatz C, Young P. Effects of non-invasive ventilation on objective sleep and nocturnal respiration in patients with amyotrophic lateral sclerosis. J Neurol. 2015;262(9):2073–2082. doi:10.1007/s00415-015-7822-4
48. Katzberg HD, Selegiman A, Guion L, et al. Effects of noninvasive ventilation on sleep outcomes in amyotrophic lateral sclerosis. J Clin Sleep Med. 2013;9(4):345–351. doi:10.5664/jcsm.2586
49. Vrijsen B, Buyse B, Belge C, et al. Noninvasive ventilation improves sleep in amyotrophic lateral sclerosis: a prospective polysomnographic study. J Clin Sleep Med. 2015;11(5):559–566. doi:10.5664/jcsm.4704
50. David WS, Bundlie SR, Mahdavi Z. Polysomnographic studies in amyotrophic lateral sclerosis. J Neurol Sci. 1997;152(Suppl 1):S29–S35.
51. Arnulf I, Similowski T, Salachas F, et al. Sleep disorders and diaphragmatic function in patients with amyotrophic lateral sclerosis. Am J Respir Crit Care Med. 2000;161(3 Pt 1):849–856. doi:10.1164/ajrccm.161.3.9805008
52. Atalaia A, De Carvalho M, Evangelista T, Pinto A. Sleep characteristics of amyotrophic lateral sclerosis in patients with preserved diaphragmatic function. Amyotroph Lateral Scler. 2007;8(2):101–105. doi:10.1080/17482960601029883
53. Just N, Bautin N, Danel-Brunaud V, Debroucker V, Matran R, Perez T. The Borg dyspnoea score: a relevant clinical marker of inspiratory muscle weakness in amyotrophic lateral sclerosis. Eur Respir J. 2010;35(2):353–360. doi:10.1183/09031936.00184908
54. Fitting JW, Paillex R, Hirt L, Aebischer P, Schluep M. Sniff nasal pressure: a sensitive respiratory test to assess progression of amyotrophic lateral sclerosis. Ann Neurol. 1999;46(6):887–893.
55. Morgan RK, McNally S, Alexander M, Conroy R, Hardiman O, Costello RW. Use of Sniff nasal-inspiratory force to predict survival in amyotrophic lateral sclerosis. Am J Respir Crit Care Med. 2005;171(3):269–274. doi:10.1164/rccm.200403-314OC
56. Czaplinski A, Yen AA, Appel SH. Forced vital capacity (FVC) as an indicator of survival and disease progression in an ALS clinic population. J Neurol Neurosurg Psychiatry. 2006;77(3):390–392. doi:10.1136/jnnp.2005.072660
57. Tilanus TBM, Groothuis JT, TenBroek-Pastoor JMC, et al. The predictive value of respiratory function tests for non-invasive ventilation in amyotrophic lateral sclerosis. Respir Res. 2017;18(1):144. doi:10.1186/s12931-017-0624-8
58. Carratu P, Cassano A, Gadaleta F, et al. Association between low sniff nasal-inspiratory pressure (SNIP) and sleep disordered breathing in amyotrophic lateral sclerosis: preliminary results. Amyotroph Lateral Scler. 2011;12(6):458–463. doi:10.3109/17482968.2011.593038
59. AAHCP/AARC/AACP/AAP/ASDA/ATS/NAMDRC. Clinical indications for noninvasive positive pressure ventilation in chronic respiratory failure due to restrictive lung disease, COPD, and nocturnal hypoventilation – a consensus conference report. Chest. 1999;116(521–534):521-534.
60. American Thoracic Society/European Respiratory Society. ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624. doi:10.1164/rccm.166.4.518
61. de Carvalho M, Matias T, Coelho F, Evangelista T, Pinto A, Luis ML. Motor neuron disease presenting with respiratory failure. J Neurol Sci. 1996;139:
62. Gautier G, Verschueren A, Monnier A, Attarian S, Salort-Campana E, Pouget J. ALS with respiratory onset: clinical features and effects of non-invasive ventilation on the prognosis. Amyotroph Lateral Scler. 2010;11(4):379–382. doi:10.3109/17482960903426543
63. Barthlen GM, Lange DJ. Unexpectedly severe sleep and respiratory pathology in patients with amyotrophic lateral sclerosis. Eur J Neurol. 2000;7(3):299–302.
64. Aboussouan LS, Khan SU, Banerjee M, Arroliga AC, Mitsumoto H. Objective measures of the efficacy of noninvasive positive-pressure ventilation in amyotrophic lateral sclerosis. Muscle Nerve. 2001;24(3):403–409.
65. Aboussouan LS, Khan SU, Meeker DP, Stelmach K, Mitsumoto H. Effect of noninvasive positive-pressure ventilation on survival in amyotrophic lateral sclerosis. Ann Intern Med. 1997;127(6):450–453. doi:10.7326/0003-4819-127-6-199709150-00006
66. Bach JR. Amyotrophic lateral sclerosis: predictors for prolongation of life by noninvasive respiratory aids. Arch Phys Med Rehabil. 1995;76(9):828–832.
67. Bach JR. Amyotrophic lateral sclerosis: prolongation of life by noninvasive respiratory AIDS. Chest. 2002;122(1):92–98. doi:10.1378/chest.122.1.92
68. Bertella E, Banfi P, Paneroni M, et al. Early initiation of night-time NIV in an outpatient setting: a randomized non-inferiority study in ALS patients. Eur J Phys Rehabil Med. 2017;53(6):892–899. doi:10.23736/S1973-9087.17.04511-7
69. Bourke SC, Tomlinson M, Williams TL, Bullock RE, Shaw PJ, Gibson GJ. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Lancet Neurol. 2006;5(2):140–147. doi:10.1016/S1474-4422(05)70326-4
70. Burkhardt C, Neuwirth C, Sommacal A, Andersen PM, Weber M. Is survival improved by the use of NIV and PEG in amyotrophic lateral sclerosis (ALS)? A post-mortem study of 80 ALS patients. PLoS One. 2017;12(5):e0177555. doi:10.1371/journal.pone.0177555
71. Butz M, Wollinsky KH, Wiedemuth-Catrinescu U, et al. Longitudinal effects of noninvasive positive-pressure ventilation in patients with amyotrophic lateral sclerosis. Am J Phys Med Rehabil. 2003;82(8):597–604. doi:10.1097/01.PHM.0000078239.83545.D0
72. Chio A, Calvo A, Moglia C, et al. Non-invasive ventilation in amyotrophic lateral sclerosis: a 10 year population based study. J Neurol Neurosurg Psychiatry. 2012;83(4):377–381. doi:10.1136/jnnp-2011-300472
73. Elamin EM, Wilson CS, Sriaroon C, et al. Effects of early introduction of non-invasive positive pressure ventilation based on forced vital capacity rate of change: variation across amyotrophic lateral sclerosis clinical phenotypes. Int J Clin Pract. 2019;73(1):e13257. doi:10.1111/ijcp.13257
74. Pinto AC, Evangelista T, Carvalho M, Alves MA, Sales Luis ML. Respiratory assistance with a non-invasive ventilator (Bipap) in MND/ALS patients: survival rates in a controlled trial. J Neurol Sci. 1995;129:
75. Sivori M, Rodriguez GE, Pascansky D, Saenz C, Sica RE. Outcome of sporadic amyotrophic lateral sclerosis treated with non-invasive ventilation and riluzole. Medicina (B Aires). 2007;67(4):326–330.
76. Vitacca M, Montini A, Lunetta C, et al. Impact of an early respiratory care programme with non-invasive ventilation adaptation in patients with amyotrophic lateral sclerosis. Eur J Neurol. 2018;25(3):556–e533. doi:10.1111/ene.13547
77. Storre JH, Magnet FS, Dreher M, Windisch W. Transcutaneous monitoring as a replacement for arterial PCO(2) monitoring during nocturnal non-invasive ventilation. Respir Med. 2011;105(1):143–150. doi:10.1016/j.rmed.2010.10.007
78. Georges M, Nguyen-Baranoff D, Griffon L, et al. Usefulness of transcutaneous PCO2 to assess nocturnal hypoventilation in restrictive lung disorders. Respirology. 2016;21(7):1300–1306. doi:10.1111/resp.12812
79. Kushida CA, Littner MR, Morgenthaler T, et al. Practice parameters for the indications for polysomnography and related procedures: an update for 2005. Sleep. 2005;28(4):499–521. doi:10.1093/sleep/28.4.499
80. Rod NH, Kumari M, Lange T, Kivimaki M, Shipley M, Ferrie J. The joint effect of sleep duration and disturbed sleep on cause-specific mortality: results from the Whitehall II cohort study. PLoS One. 2014;9(4):e91965. doi:10.1371/journal.pone.0091965
81. Congiu PT, Milioli G, Borghero G, Puligheddu M. Sleep, sleep structure and sleep disorders in a cohort of patients affected by ALS. Ann Community Med Pract. 2018;4(1):1028.
82. Vandoorne E, Vrijsen B, Belge C, Testelmans D, Buyse B. Noninvasive ventilation in amyotrophic lateral sclerosis: effects on sleep quality and quality of life. Acta Clin Belg. 2016;71(6):389–394. doi:10.1080/17843286.2016.1173941
83. Mustfa N, Walsh E, Bryant V, et al. The effect of noninvasive ventilation on ALS patients and their caregivers. Neurology. 2006;66(8):1211–1217. doi:10.1212/01.wnl.0000208957.88534.11
84. Lyall RA, Donaldson N, Fleming T, et al. A prospective study of quality of life in ALS patients treated with noninvasive ventilation. Neurology. 2001;57(1):153–156. doi:10.1212/wnl.57.1.153
85. Teschler H, Stampa J, Ragette R, Konietzko N, Berthon-Jones M. Effect of mouth leak on effectiveness of nasal bilevel ventilatory assistance and sleep architecture. Eur Respir J. 1999;14(6):1251–1257.
86. Schellhas V, Glatz C, Beecken I, et al. Upper airway obstruction induced by non-invasive ventilation using an oronasal interface. Sleep Breath. 2018;22(3):781–788. doi:10.1007/s11325-018-1640-8
87. Crescimanno G, Greco F, Arrisicato S, Morana N, Marrone O. Effects of positive end expiratory pressure administration during non-invasive ventilation in patients affected by amyotrophic lateral sclerosis: a randomized crossover study. Respirology. 2016;21(7):1307–1313. doi:10.1111/resp.12836
88. Atkeson AD, RoyChoudhury A, Harrington-Moroney G, Shah B, Mitsumoto H, Basner RC. Patient-ventilator asynchrony with nocturnal noninvasive ventilation in ALS. Neurology. 2011;77(6):549–555. doi:10.1212/WNL.0b013e318228c0fb
89. Sancho J, Servera E, Morelot-Panzini C, Salachas F, Similowski T, Gonzalez-Bermejo J. Non-invasive ventilation effectiveness and the effect of ventilatory mode on survival in ALS patients. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15(1–2):55–61. doi:10.3109/21678421.2013.855790
90. Georges M, Attali V, Golmard JL, et al. Reduced survival in patients with ALS with upper airway obstructive events on non-invasive ventilation. J Neurol Neurosurg Psychiatry. 2016;87(10):1045–1050. doi:10.1136/jnnp-2015-312606
91. Gonzalez-Bermejo J, Morelot-Panzini C, Arnol N, et al. Prognostic value of efficiently correcting nocturnal desaturations after one month of non-invasive ventilation in amyotrophic lateral sclerosis: a retrospective monocentre observational cohort study. Amyotroph Lateral Scler Frontotemporal Degener. 2013;14(5–6):373–379. doi:10.3109/21678421.2013.776086
92. Ogna A, Nardi J, Prigent H, et al. Prognostic value of initial assessment of residual hypoventilation using nocturnal capnography in mechanically ventilated neuromuscular patients: a 5-year follow-up study. Front Med (Lausanne). 2016;3:40.
93. Volanti P, Cibella F, Sarva M, et al. Predictors of non-invasive ventilation tolerance in amyotrophic lateral sclerosis. J Neurol Sci. 2011;303(1–2):114–118. doi:10.1016/j.jns.2010.12.021
94. Sancho J, Martinez D, Bures E, Diaz JL, Ponz A, Servera E. Bulbar impairment score and survival of stable amyotrophic lateral sclerosis patients after noninvasive ventilation initiation. ERJ Open Res. 2018;4:2. doi:10.1183/23120541.00159-2017
95. Bortolotti M. Laryngospasm and reflex central apnoea caused by aspiration of refluxed gastric content in adults. Gut. 1989;30(2):233–238. doi:10.1136/gut.30.2.233
96. Kuhnlein P, Gdynia HJ, Sperfeld AD, et al. Diagnosis and treatment of bulbar symptoms in amyotrophic lateral sclerosis. Nat Clin Pract Neurol. 2008;4(7):366–374. doi:10.1038/ncpneuro0853
97. Montagna P, Liguori R, Zucconi M, Lugaresi A, Cirignotta F, Lugaresi E. Fasciculations during wakefulness and sleep. Acta Neurol Scand. 1987;76(2):152–154.
98. Stephens HE, Joyce NC, Oskarsson B. National study of muscle cramps in ALS in the USA. Amyotroph Lateral Scler Frontotemporal Degener. 2017;18(1–2):32–36. doi:10.1080/21678421.2016.1245755
99. Caress JB, Ciarlone SL, Sullivan EA, Griffin LP, Cartwright MS. Natural history of muscle cramps in amyotrophic lateral sclerosis. Muscle Nerve. 2016;53(4):513–517. doi:10.1002/mus.24892
100. Baldissera F, Cavallari P, Dworzak F. Motor neuron ‘bistability’. A pathogenetic mechanism for cramps and myokymia. Brain. 1994;117(Pt 5):929–939. doi:10.1093/brain/117.5.929
101. Hallegraeff JM, van der Schans CP, de Ruiter R, de Greef MH. Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in older adults: a randomised trial. J Physiother. 2012;58(1):17–22. doi:10.1016/S1836-9553(12)70068-1
102. Oskarsson B, Moore D, Mozaffar T, et al. Mexiletine for muscle cramps in amyotrophic lateral sclerosis: a randomized, double-blind crossover trial. Muscle Nerve. 2018. doi:10.1002/mus.26117
103. Baldinger R, Katzberg HD, Weber M. Treatment for cramps in amyotrophic lateral sclerosis/motor neuron disease. Cochrane Database Syst Rev. 2012;(4):CD004157. doi: 10.1002/14651858.
104. El-Tawil S, Al Musa T, Valli H, et al. Quinine for muscle cramps. Cochrane Database Syst Rev. 2015;(4):CD005044. doi: 10.1002/14651858.CD005044.pub3
105. Hogan DB. Quinine: not a safe drug for treating nocturnal leg cramps. CMAJ. 2015;187(4):237–238. doi:10.1503/cmaj.150044
106. Skarpsno ES, Mork PJ, Nilsen TIL, Holtermann A. Sleep positions and nocturnal body movements based on free-living accelerometer recordings: association with demographics, lifestyle, and insomnia symptoms. Nat Sci Sleep. 2017;9:267–275. doi:10.2147/NSS.S145777
107. Chen JH, Wu SC, Chen HJ, Kao CH, Tseng CH, Tsai CH. Risk of developing pressure sore in amyotrophic lateral sclerosis patients - a nationwide cohort study. J Eur Acad Dermatol Venereol. 2018;32(9):1589–1596. doi:10.1111/jdv.14911
108. Hayashi T, Narita Y, Okugawa N, Hamaguchi E, Shibahara M, Kuzuhara S. Pressure ulcers in ALS patients on admission at a university hospital in Japan. Amyotroph Lateral Scler. 2007;8(5):310–313. doi:10.1080/17482960701538825
109. Ono S, Toyokura Y, Mannen T, Ishibashi Y. Increased dermal collagen density in amyotrophic lateral sclerosis. J Neurol Sci. 1988;83(1):81–92.
110. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–1552. doi:10.1016/j.jpain.2013.08.007
111. Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and managing sleep disturbance in patients with chronic pain. Sleep Med Clin. 2016;11(4):531–541. doi:10.1016/j.jsmc.2016.08.004
112. Moisset X, Cornut-Chauvinc C, Clavelou P, Pereira B, Dallel R, Guy N. Is there pain with neuropathic characteristics in patients with amyotrophic lateral sclerosis? A cross-sectional study. Palliat Med. 2016;30(5):486–494. doi:10.1177/0269216315600332
113. Wallace VC, Ellis CM, Burman R, Knights C, Shaw CE, Al-Chalabi A. The evaluation of pain in amyotrophic lateral sclerosis: a case controlled observational study. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15(7–8):520–527. doi:10.3109/21678421.2014.951944
114. Dalla Bella E, Lombardi R, Porretta-Serapiglia C, et al. Amyotrophic lateral sclerosis causes small fiber pathology. Eur J Neurol. 2016;23(2):416–420. doi:10.1111/ene.12936
115. Nijs J, Torres-Cueco R, van Wilgen CP, et al. Applying modern pain neuroscience in clinical practice: criteria for the classification of central sensitization pain. Pain Physician. 2014;17(5):447–457.
116. Ziegler EA, Magerl W, Meyer RA, Treede RD. Secondary hyperalgesia to punctate mechanical stimuli. Central sensitization to A-fibre nociceptor input. Brain. 1999;122(Pt 12):2245–2257. doi:10.1093/brain/122.12.2245
117. Chio A, Mora G, Lauria G. Pain in amyotrophic lateral sclerosis. Lancet Neurol. 2017;16(2):144–157. doi:10.1016/S1474-4422(16)30358-1
118. Ganzini L, Silveira MJ, Johnston WS. Predictors and correlates of interest in assisted suicide in the final month of life among ALS patients in Oregon and Washington. J Pain Symptom Manage. 2002;24(3):312–317.
119. Hogl B, Kiechl S, Willeit J, et al. Restless legs syndrome: a community-based study of prevalence, severity, and risk factors. Neurology. 2005;64(11):1920–1924. doi:10.1212/01.WNL.0000163996.64461.A3
120. Abetz L, Allen R, Follet A, et al. Evaluating the quality of life of patients with restless legs syndrome. Clin Ther. 2004;26(6):925–935.
121. Limousin N, Blasco H, Corcia P, Arnulf I, Praline J. The high frequency of restless legs syndrome in patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2011;12(4):303–306. doi:10.3109/17482968.2011.557736
122. Liu S, Shen D, Tai H, et al. Restless legs syndrome in Chinese patients with sporadic amyotrophic lateral sclerosis. Front Neurol. 2018;9:735. doi:10.3389/fneur.2018.00735
123. Lo Coco D, Piccoli F, La Bella V. Restless legs syndrome in patients with amyotrophic lateral sclerosis. Mov Disord. 2010;25(15):2658–2661. doi:10.1002/mds.23261
124. Weis J, Katona I, Muller-Newen G, et al. Small-fiber neuropathy in patients with ALS. Neurology. 2011;76(23):2024–2029. doi:10.1212/WNL.0b013e31821e553a
125. Isak B, Tankisi H, Johnsen B, et al. Involvement of distal sensory nerves in amyotrophic lateral sclerosis. Muscle Nerve. 2016;54(6):1086–1092. doi:10.1002/mus.25157
126. Wijemanne S, Ondo W. Restless legs syndrome: clinical features, diagnosis and a practical approach to management. Pract Neurol. 2017;17(6):444–452. doi:10.1136/practneurol-2017-001762
127. Garcia-Borreguero D, Silber MH, Winkelman JW, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation. Sleep Med. 2016;21:1–11. doi:10.1016/j.sleep.2016.01.017
128. Puligheddu M, Congiu P, Arico D, et al. Isolated rapid eye movement sleep without atonia in amyotrophic lateral sclerosis. Sleep Med. 2016;26:16–22. doi:10.1016/j.sleep.2016.05.016
129. Lo Coco D, Puligheddu M, Mattaliano P, et al. REM sleep behavior disorder and periodic leg movements during sleep in ALS. Acta Neurol Scand. 2017;135(2):219–224. doi:10.1111/ane.12593
130. Moszczynski AJ, Tandon A, Coelho FM, Zinman L, Murray B. Mortality associated with periodic limb movements during sleep in amyotrophic lateral sclerosis patients. Einstein (Sao Paulo). 2012;10(4):428–432.
131. Cedarbaum JM, Stambler N, Malta E, et al. The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (Phase III). J Neurol Sci. 1999;169(1–2):13–21.
132. Bara-Jimenez W, Aksu M, Graham B, Sato S, Hallett M. Periodic limb movements in sleep: state-dependent excitability of the spinal flexor reflex. Neurology. 2000;54(8):1609–1616. doi:10.1212/wnl.54.8.1609
133. Luppi PH, Clement O, Sapin E, et al. The neuronal network responsible for paradoxical sleep and its dysfunctions causing narcolepsy and rapid eye movement (REM) behavior disorder. Sleep Med Rev. 2011;15(3):153–163. doi:10.1016/j.smrv.2010.08.002
134. Hogl B, Stefani A, Videnovic A. Idiopathic REM sleep behaviour disorder and neurodegeneration - an update. Nat Rev Neurol. 2018;14(1):40–55. doi:10.1038/nrneurol.2017.157
135. Iranzo A, Fernandez-Arcos A, Tolosa E, et al. Neurodegenerative disorder risk in idiopathic REM sleep behavior disorder: study in 174 patients. PLoS One. 2014;9(2):e89741. doi:10.1371/journal.pone.0089741
136. Boeve BF, Silber MH, Ferman TJ, et al. Clinicopathologic correlations in 172 cases of rapid eye movement sleep behavior disorder with or without a coexisting neurologic disorder. Sleep Med. 2013;14(8):754–762. doi:10.1016/j.sleep.2012.10.015
137. Sabater L, Gaig C, Gelpi E, et al. A novel non-rapid-eye movement and rapid-eye-movement parasomnia with sleep breathing disorder associated with antibodies to IgLON5: a case series, characterisation of the antigen, and post-mortem study. Lancet Neurol. 2014;13(6):575–586. doi:10.1016/S1474-4422(14)70051-1
138. Gelpi E, Hoftberger R, Graus F, et al. Neuropathological criteria of anti-IgLON5-related tauopathy. Acta Neuropathol. 2016;132(4):531–543. doi:10.1007/s00401-016-1591-8
139. Wang P, Wing YK, Xing J, et al. Rapid eye movement sleep behavior disorder in patients with probable Alzheimer’s disease. Aging Clin Exp Res. 2016;28(5):951–957. doi:10.1007/s40520-015-0382-8
140. Cagnin A, Mariotto S, Fiorini M, et al. Microglial and neuronal TDP-43 pathology in Anti-IgLON5-related tauopathy. J Alzheimers Dis. 2017;59(1):13–20. doi:10.3233/JAD-170189
141. Lo Coco D, Caruso G, Mattaliano A. REM sleep behavior disorder in patients with DJ-1 mutations and parkinsonism-dementia-ALS complex. Mov Disord. 2009;24(10):1555–1556. doi:10.1002/mds.22629
142. Lo Coco D, Cupidi C, Mattaliano A, Baiamonte V, Realmuto S, Cannizzaro E. REM sleep behavior disorder in a patient with frontotemporal dementia. Neurol Sci. 2012;33(2):371–373. doi:10.1007/s10072-011-0702-5
143. Ebben MR, Shahbazi M, Lange DJ, Krieger AC. REM behavior disorder associated with familial amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2012;13(5):473–474. doi:10.3109/17482968.2012.673172
144. Daoud H, Postuma RB, Bourassa CV, et al. C9orf72 repeat expansions in rapid eye movement sleep behaviour disorder. Can J Neurol Sci. 2014;41(6):759–762. doi:10.1017/cjn.2014.39
145. Frauscher B, Iranzo A, Gaig C, et al. Normative EMG values during REM sleep for the diagnosis of REM sleep behavior disorder. Sleep. 2012;35(6):835–847. doi:10.5665/sleep.1886
146. Jung Y, St Louis EK. Treatment of REM sleep behavior disorder. Curr Treat Options Neurol. 2016;18(11):50. doi:10.1007/s11940-016-0433-2
147. Gunther R, Richter N, Sauerbier A, et al. Non-motor symptoms in patients suffering from motor neuron diseases. Front Neurol. 2016;7:117. doi:10.3389/fneur.2016.00117
148. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
149. Skapinakis P, Rai D, Anagnostopoulos F, Harrison S, Araya R, Lewis G. Sleep disturbances and depressive symptoms: an investigation of their longitudinal association in a representative sample of the UK general population. Psychol Med. 2013;43(2):329–339. doi:10.1017/S0033291712001055
150. Borasio GD, Voltz R. Palliative care in amyotrophic lateral sclerosis. J Neurol. 1997;244(Suppl 4):S11–S17.
151. Neudert C, Oliver D, Wasner M, Borasio GD. The course of the terminal phase in patients with amyotrophic lateral sclerosis. J Neurol. 2001;248(7):612–616.
152. Kettemann D, Funke A, Maier A, et al. Clinical characteristics and course of dying in patients with amyotrophic lateral sclerosis withdrawing from long-term ventilation. Amyotroph Lateral Scler Frontotemporal Degener. 2017;18(1–2):53–59. doi:10.1080/21678421.2016.1214734
153. Takekawa H, Kubo J, Miyamoto T, Miyamoto M, Hirata K. Amyotrophic lateral sclerosis associated with insomnia and the aggravation of sleep-disordered breathing. Psychiatry Clin Neurosci. 2001;55(3):263–264. doi:10.1046/j.1440-1819.2001.00852.x
154. Verschueren A, Kianimehr G, Belingher C, et al. Wish to die and reasons for living among patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. 2018.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.