Back to Journals » Nature and Science of Sleep » Volume 14
Sleep Disorders and Sleep Problems in Patients With Tourette Syndrome and Other Tic Disorders: Current Perspectives
Authors Jiménez-Jiménez FJ, Alonso-Navarro H ![]() , García-Martín E, Agúndez JAG
, García-Martín E, Agúndez JAG
Received 3 March 2022
Accepted for publication 1 July 2022
Published 25 July 2022 Volume 2022:14 Pages 1313—1331
DOI https://doi.org/10.2147/NSS.S340948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Félix Javier Jiménez-Jiménez,1 Hortensia Alonso-Navarro,1 Elena García-Martín,2 José AG Agúndez2
1Section of Neurology, Hospital Universitario Del Sureste, Arganda del Rey, Madrid, Spain; 2Universidad de Extremadura, University Institute of Molecular Pathology Biomarkers, ARADyAL, Cáceres, Spain
Correspondence: Félix Javier Jiménez-Jiménez, Section of Neurology, Hospital Universitario Del Sureste, Ronda del Sur 10, Arganda del Rey, Madrid, E28500, Spain, Email [email protected]
Abstract: Sleep disorders seem to be a frequent complaint of patients diagnosed with Tourette syndrome (TS) or chronic or persistent tic disorders (CTD or PTD). In this review, we expanded a previously used search using 4 well-known databases up to February 15, 2022, looking for the coexistence of global and/or specific sleep disorders and polysomnographic studies performed on patients with TS/CTD/PTD. The references of interest in the topic were selected by hand. Sleep disorders in general, insomnia, different arousal disorders, the persistence of tics during sleep, excessive daytime sleepiness, and periodic limb movements during sleep (PLMS) were very frequent in patients with TS, most of them being more frequent in patients with comorbid Attention Deficit Hyperactivity Disorder. The most frequent results from polysomnographic studies were decreased sleep efficiency and increased sleep onset latency. Many of these findings could be related to medication used for the treatment of tics and comorbid disorders.
Keywords: Tourette syndrome, sleep disorders, insomnia, hypersomnia, arousal disorders, periodic limb movements during sleep
Introduction
In 1884, Georges Gilles de la Tourette described 9 patients who presented with multiple tics, coprolalia, echolalia, and echopraxia. However in 1825, Itard had already made the first description of patients with a clinical picture consistent with what would nowadays be considered Tourette syndrome (TS).1,2 TS is defined as a neuropsychiatric disorder of genetic origin mainly characterized by the presence of motor and vocal tics. Both attention deficit hyperactivity disorder (ADHD) and obsessive-compulsive disorder (OCD) are very frequently associated with motor and vocal tics,1,3–5 other well-established comorbidities being learning problems, anxiety, depression, disruptive behaviour disorders, and substance abuse.1,5
In his seminal work, Gilles de la Tourette described one patient who showed confusional pictures of violence after a sudden awakening from a profound sleep, which is probably the first description of a sleep disorder in a patient with TS.6 Several recent reviews have shown that the presence of sleep disorders in TS should be considered as a frequent comorbidity of this condition.7–11
The current review, which updates previously reported information,7–11 focuses on the main findings of studies addressing sleep features, including polysomnographic studies, of patients diagnosed with TS or persistent (chronic) tic disorder (CTD) according to the DSM-5,2 by describing and discussing the reported data on this issue. Our search strategy, which used the terms of the international classification of sleep disorders (3rd edition)13,14 and followed the methodology outlined in the PRISMA guidelines,15 has been reported in detail elsewhere.9 The time of the search was extended up to February 15, 2022.
Studies on the Prevalence of Sleep Disorders in Tourette Syndrome
Table 1 summarizes the studies reporting on the frequency of sleep disorders in patients diagnosed with TS or CTD. Most of the studies were hospital-based series,16–29 two were population-based studies,31,39 and one study was a prospective follow-up.31 The prevalence of sleep disorders described in these series ranges from 7.24% to 80%, although the definitions of sleep disorders, the age ranges, sex distribution, frequency of comorbidities, and the treatments used for TS and CTD show high variability between different studies. The lowest prevalence was found in a population study, although this was significantly higher than that found in a comparison control cohort, with a hazard ratio (95% confidence intervals) of 2.05 (1.43–2.95) (p < 0.01).30
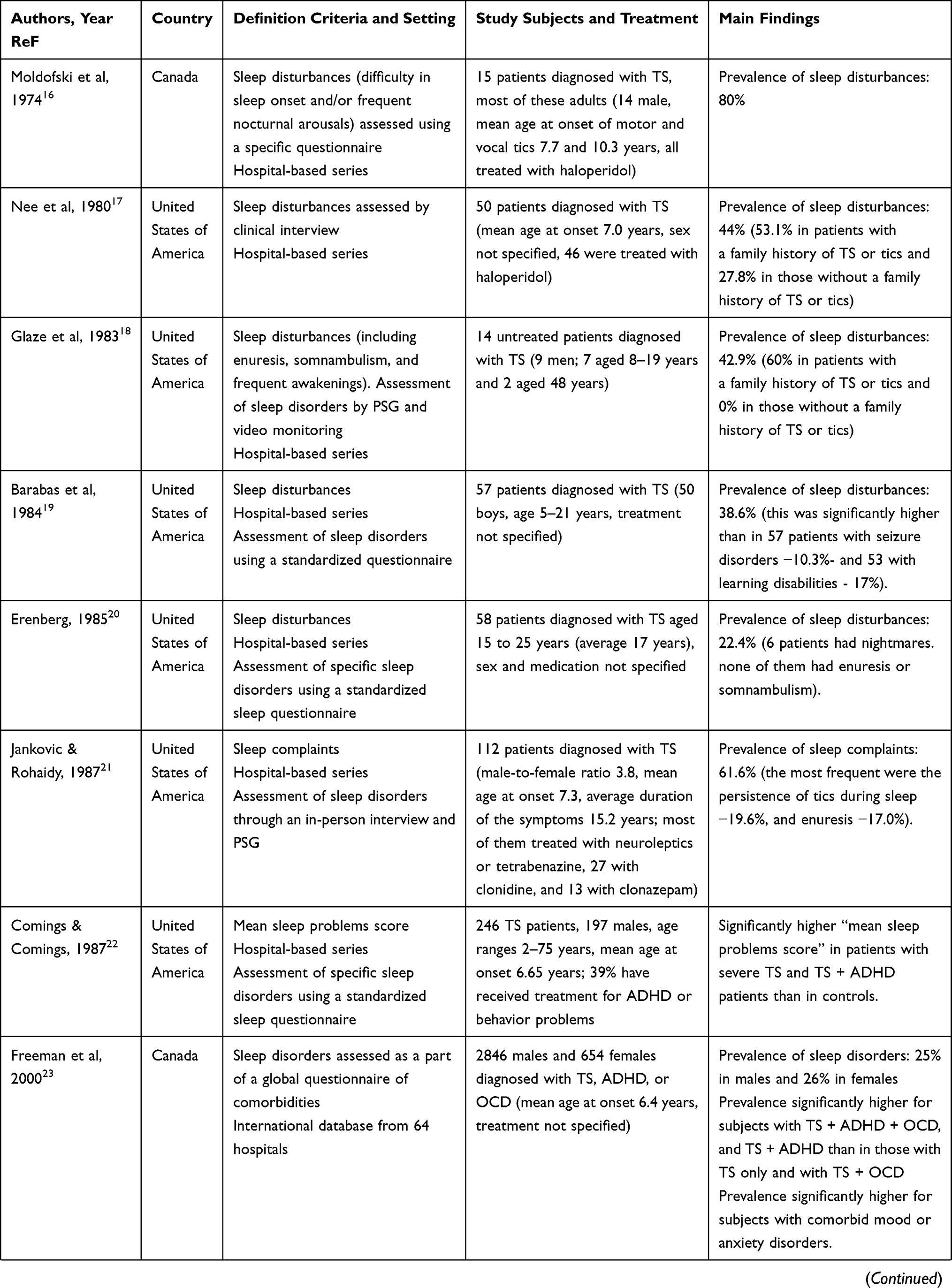 | 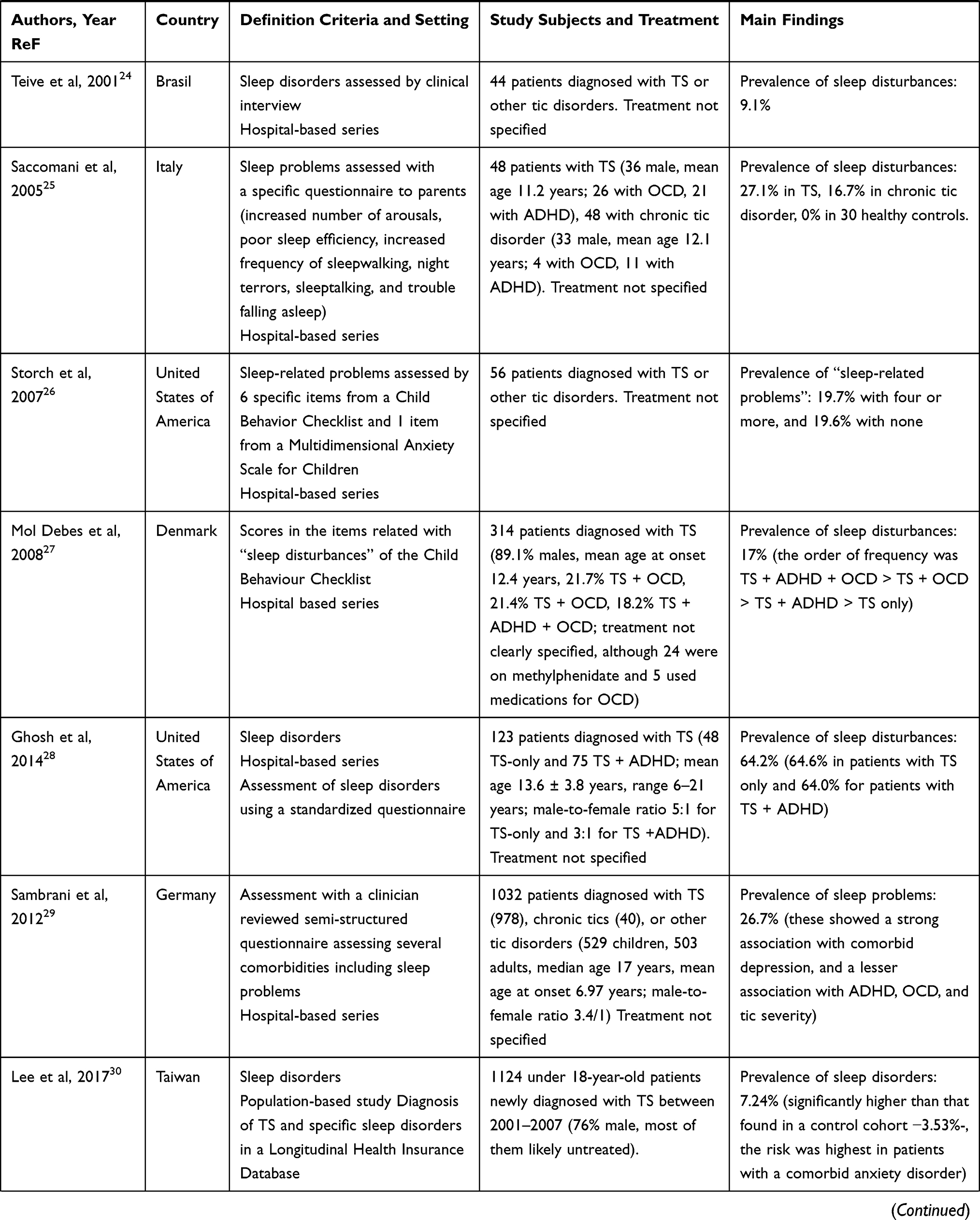 | 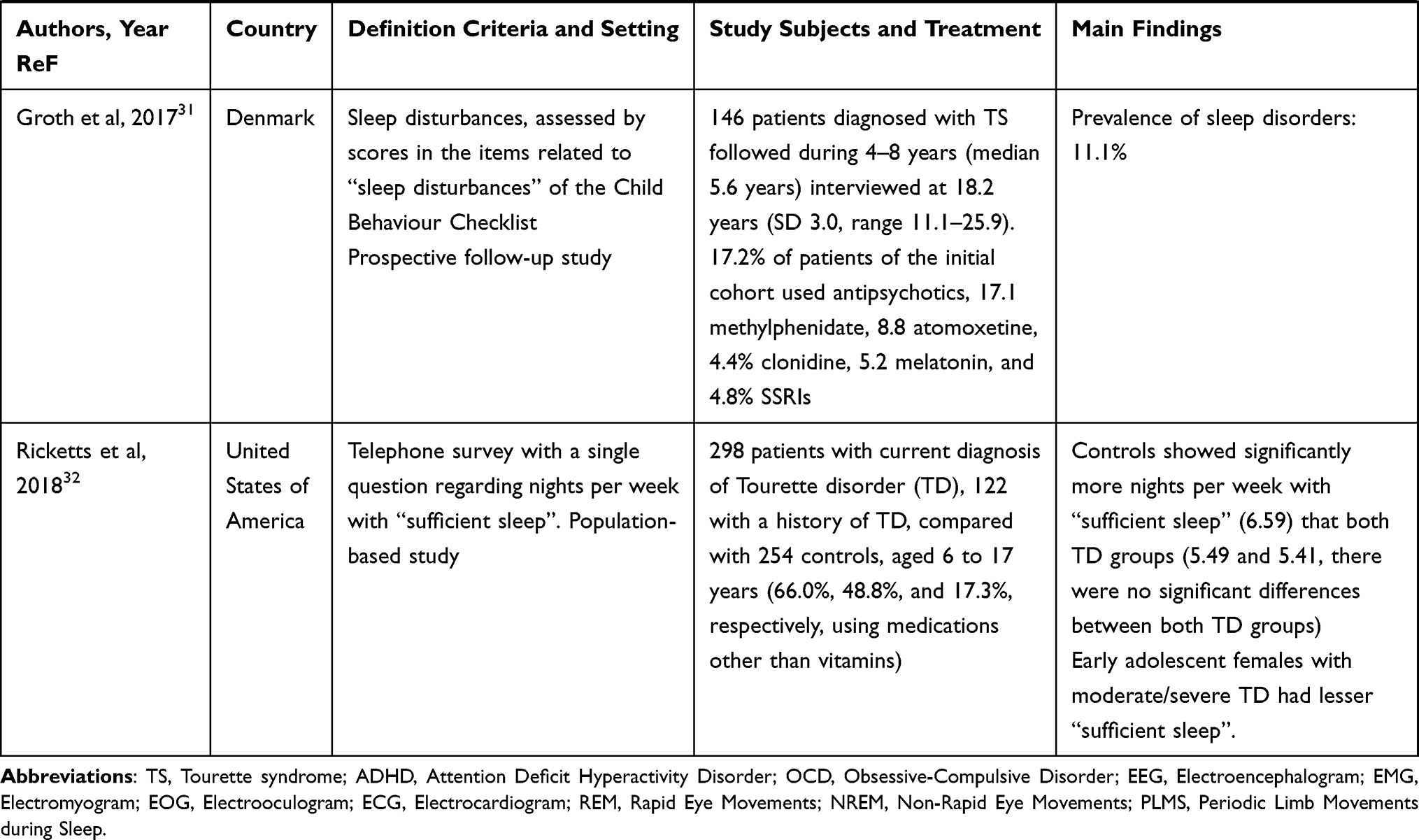 |
Table 1 Studies on the Prevalence of Sleep Disorders in Tourette Syndrome |
Some authors reported a significantly higher “mean sleep problems score” in patients diagnosed with severe TS or with TS + ADHD when compared with controls,22 and higher scores on the items related to “sleep disturbances” of the Child Behaviour Checklist in patients diagnosed with TS (especially if they had ADHD and/or OCD).27 In addition, patients with TS/TD showed fewer nights with “sufficient sleep” than controls in a population-based study.32
According to several studies, sleep disturbances were more frequent in TS patients with comorbidities, such as ADHD,22,23,27,29 OCD,22,27,29 mood disorders-depression,22,29 and anxiety disorders,22,30 and in those with a family history of TS or tics.17,18
Association Between Specific Sleep Disorders and Tourette Syndrome
Insomnia
Table 2 summarizes the results of studies addressing the prevalence of insomnia and related symptoms in patients with TS/CTD, which was a frequent complaint. As was described in the studies on the global prevalence of sleep disorders, most of the studies on the prevalence of insomnia in these disorders were hospital-based series,20–22,28,34–37 one was a population-based study30 and the other a total population cohort study.38 The prevalence of insomnia in these series ranged from 0.3% to 60%. The lowest prevalence, which was found in a population study in Taiwan, was similar to that found in a comparison control cohort (0.3 vs 0.2%).30 TS patients with coexistent ADHD were more prone to developing insomnia, according to several series.22,28,38
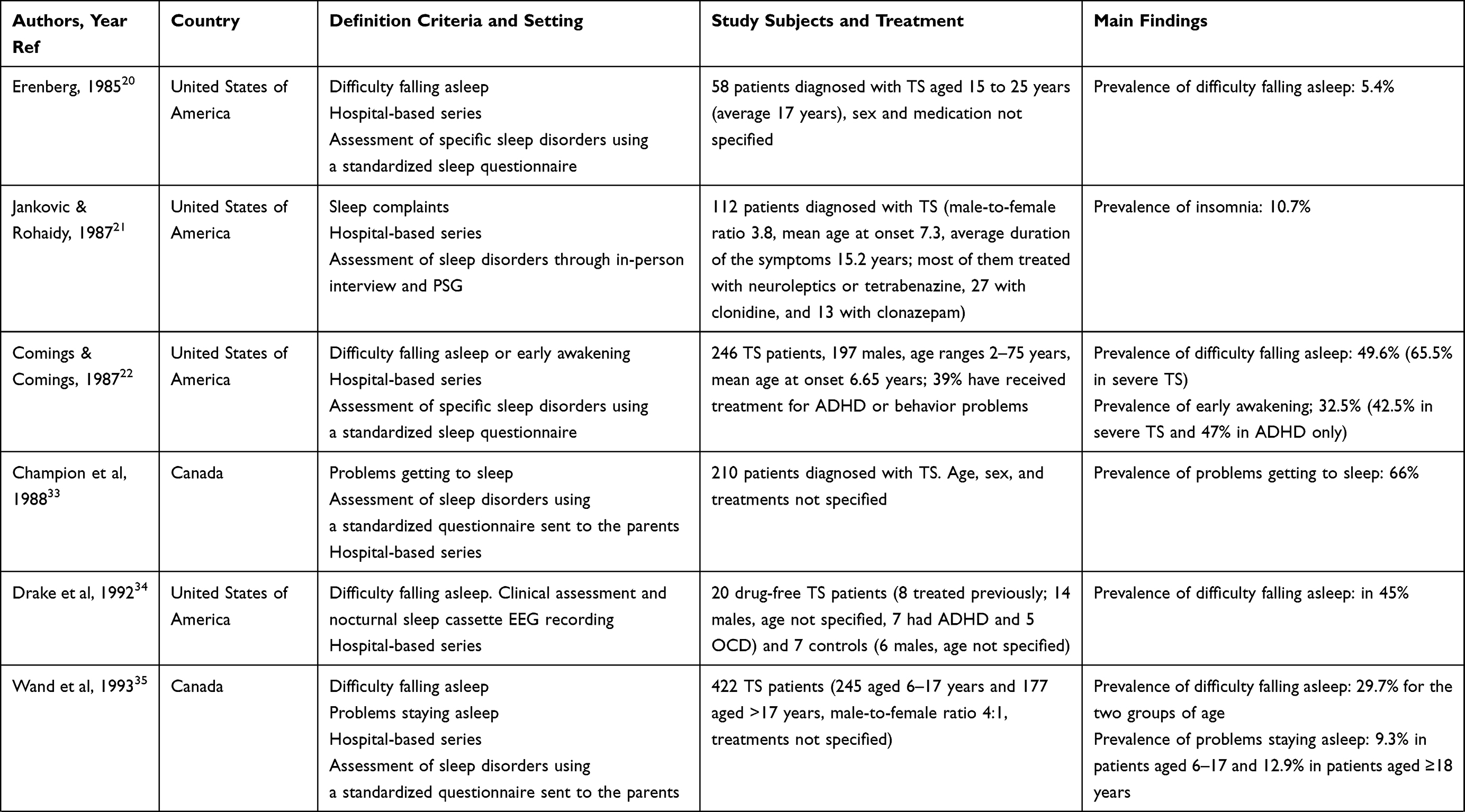 | 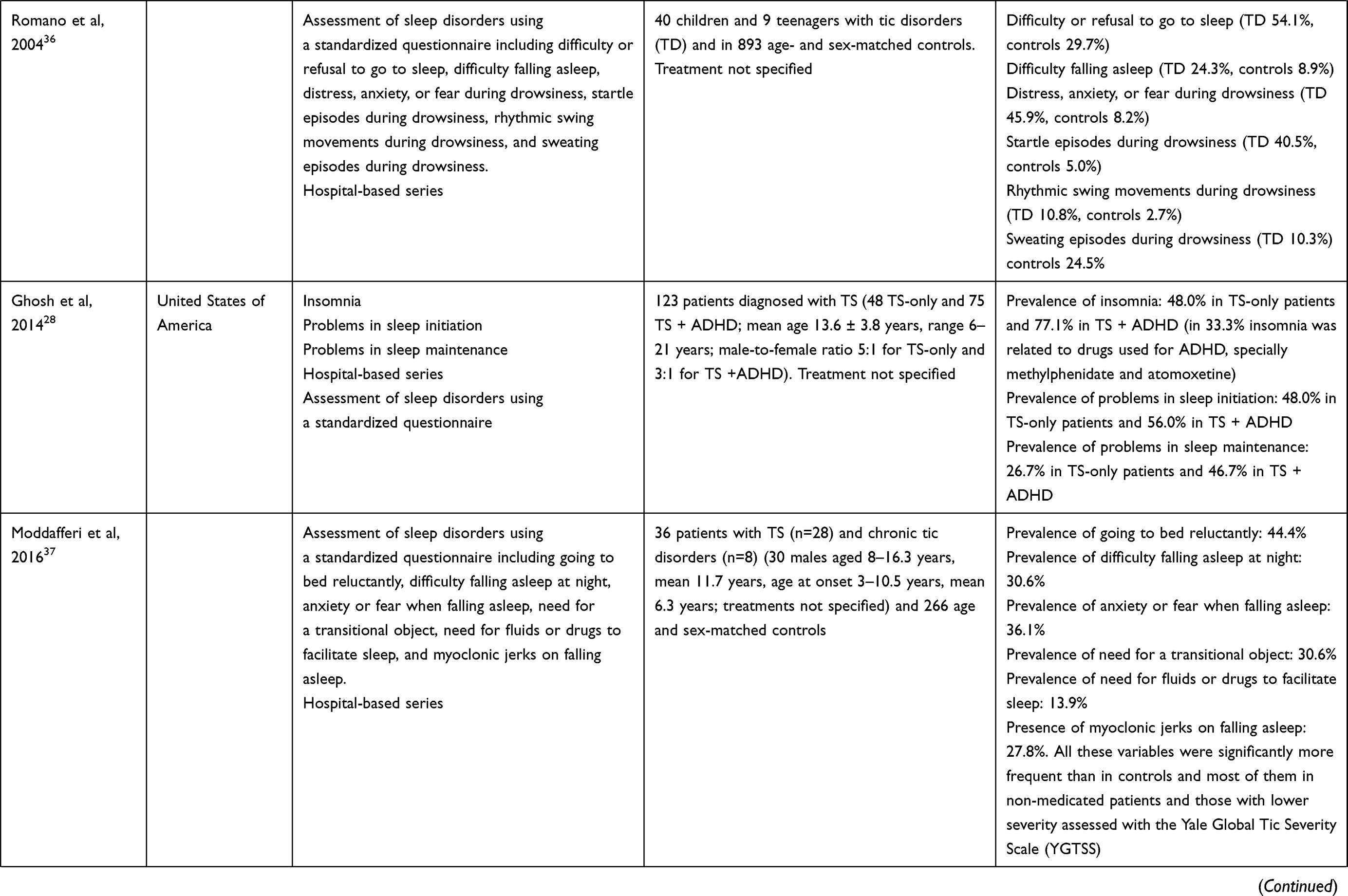 | 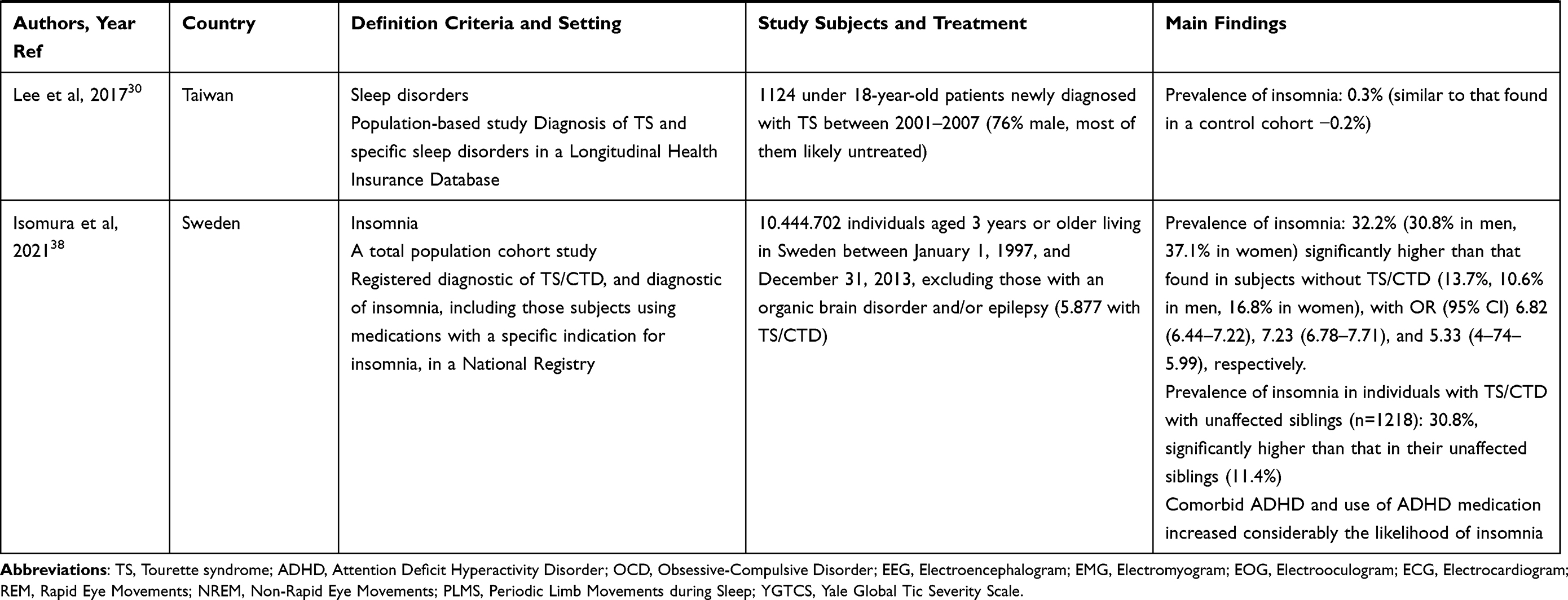 |
Table 2 Studies on the Prevalence of Insomnia in Tourette Syndrome |
The most consistent study, reported recently, was a total population cohort study carried out in Sweden38 which described a prevalence of insomnia of 32.2%, a 6.7-fold increase compared to the general population. Insomnia was more frequent in TS/CTD patients than in their asymptomatic siblings, and was more frequent in patients with coexistent ADHD or those taking ADHD medication.38
Sleep-Related Breathing Disorders
Literature references to the presence of sleep breathing disorders in patients with TS or CTD are scarce. Some authors reported an increased risk of life-threatening sleep apnea in children carrying TS gene variations and described sudden infant death related to obstructive sleep apnea in children from TS families.39 Apneic episodes with a relative increase in pCO2, which ceased after specific therapy, were reported in 3 out of 14 TS patients in a series.18
Other authors described the presence of obstructive sleep apnea confirmed by polysomnography, in 8 out of 34 TS patients.21 A population study carried out in Taiwan, involving newly diagnosed TS patients, showed an estimated prevalence of sleep apnea of 0.2%, which was similar to that found in a control cohort (0.4%).30
Seven of 31 TS-only patients (two of them with obstructive sleep apnea and 2 with central sleep apnea), and 3 out of 48 patients diagnosed with TS + ADHD, showed sleep-related breathing disorders in a study by Ghosh et al.28 Moddafferi et al37 reported a non-significant higher frequency of sleep breathing difficulties in patients with CTD than in controls (11.1% vs 4.9%), although the differences only reached statistical significance when unmedicated CTD patients (16%) were considered, but did not find any CTD patients with sleep apnea in their series.37
Finally, the frequency of snoring as a respiratory disturbance in sleep was found to be similar in TS-only patients (36.8%), TS + ADHD patients (46.6%), and in controls (43.7%) according to one study,40 while another described a significantly higher frequency in patients with CTD (32.0% in unmedicated patients, 27.8% in the whole sample) than in a control group (14.3%).37
Central Disorders of Hypersomnolence
According to Allen et al,40 patients with TS + ADHD showed significantly higher scores in items of “drowsiness during the day” and “irresistible daytime sleep”, and significantly higher frequencies of “drowsiness during the day” and “irresistible daytime sleep” than controls (33.3% and 23.0% of 89, and 3.0% and 3.0% of 146, respectively). However, the frequencies of these items in patients with TS-only (10.7% and 10.7% of 57) and ADHD-only (15.0% and 15.8% of 21) did not reach significant differences compared to controls.
According to Ghosh et al,28 the frequencies of “excessive daytime sleepiness” and “unrefreshed after sleep” did not differ significantly between TS-only (52% and 65%, respectively) and TS + ADHD patients (52% and 64%, respectively). According to the same group, only 3 of 31 TS-only patients and 2 of 48 TS + ADHD patients showed primary hypersomnia (one in each group was diagnosed with concomitant sleep apnea).28
“Daytime somnolence” and “falling asleep at school” were significantly more frequent in patients diagnosed with tic disorders (19.4% and 5.6%, respectively) than in healthy controls (5.6% and 0.4%, respectively).37 In addition, in the tic disorder patient group, these two symptoms were more frequent in patients with higher severity of tics (according to the Yale Global Tic Severity Scale –YGTSS) and those medicated,37 and 2.8% of patients (all of them unmedicated and with low YGTSS scores) and 1.5% of the controls reported “sleep attacks”.37
Finally, a recent population-based study in a large cohort carried out in Taiwan showed a similar frequency of “hypersomnia” in patients with a recent diagnosis of TS (0.3%) than in healthy controls (0.1%).30
Ghosh et al28 reported the presence of narcolepsy in 2 of 31 patients diagnosed with TS-only and in 2 of 48 with TS + ADHD. One of 70 patients diagnosed with TS, 2 of 28 patients with narcolepsy, and none of 110 control individuals, carried mutations in a gene implicated in an animal model of narcolepsy and some sporadic cases of human narcolepsy, called orexin2/hypocretine2 receptor gene (HCRTR2, chromosome 6p12.1, gene ID 3062).41 In the literature search, we did not find any reports of co-occurrence of TS with Kleine-Levin syndrome.
Circadian Rhythm Sleep-Wake Disorders
Ghosh et al28 reported the presence of circadian rhythm sleep-wake disorders in 3 of 31 (9.7%) of their patients with TS-only and in 2 of 48 (4.2%) of the TS + ADHD patients in their series. We found no clinical descriptions of these disorders in TS.
Parasomnias
Data from studies addressing the frequency of both NREM-related parasomnias (confusional arousals, sleeptalking, sleepwalking or somnambulism, and sleep night terrors) and REM-related parasomnias in TS patients (REM sleep behaviour disorder, sleep paralysis, night terrors, and sleep enuresis) are summarized in Table 3.
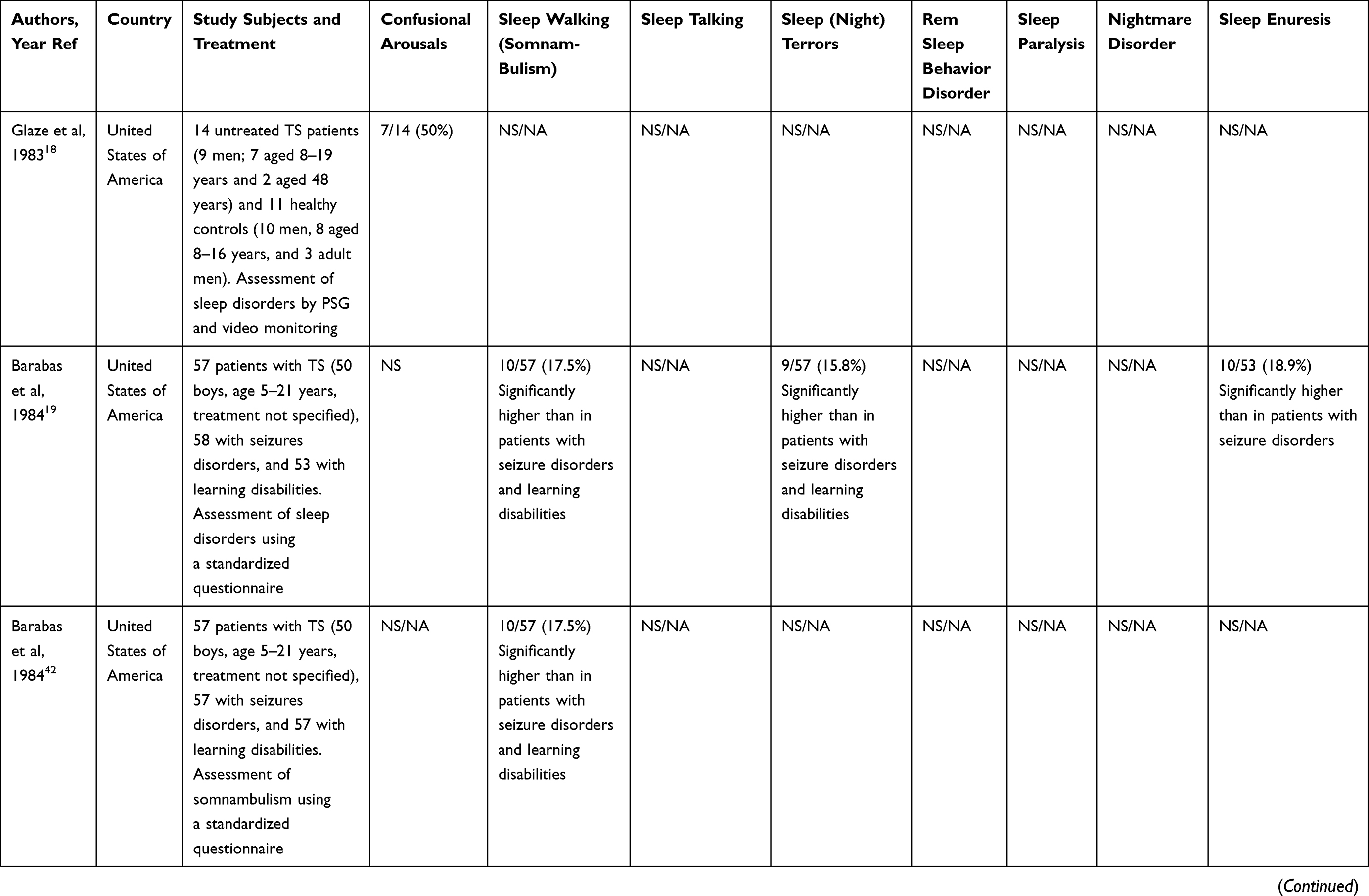 | 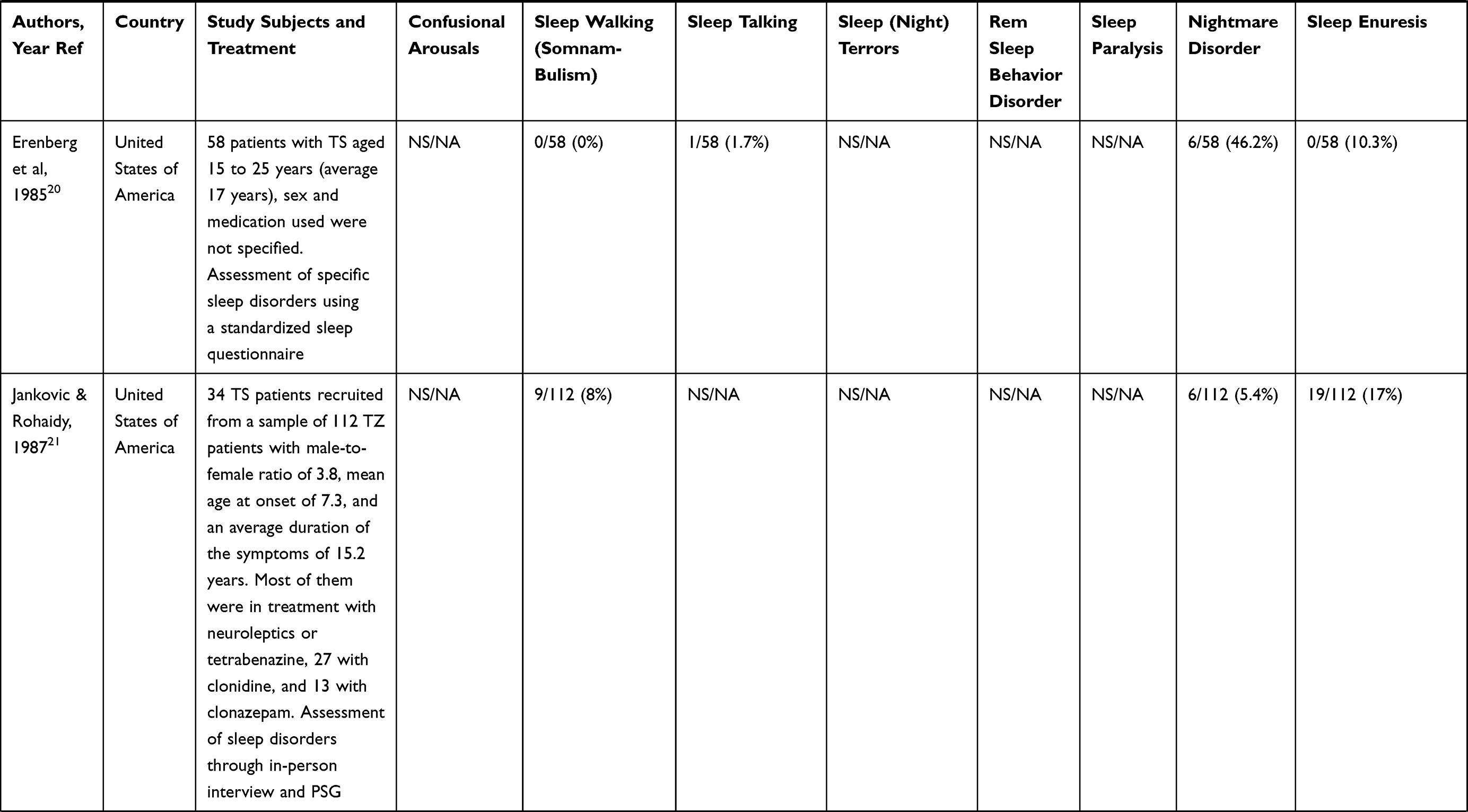 | 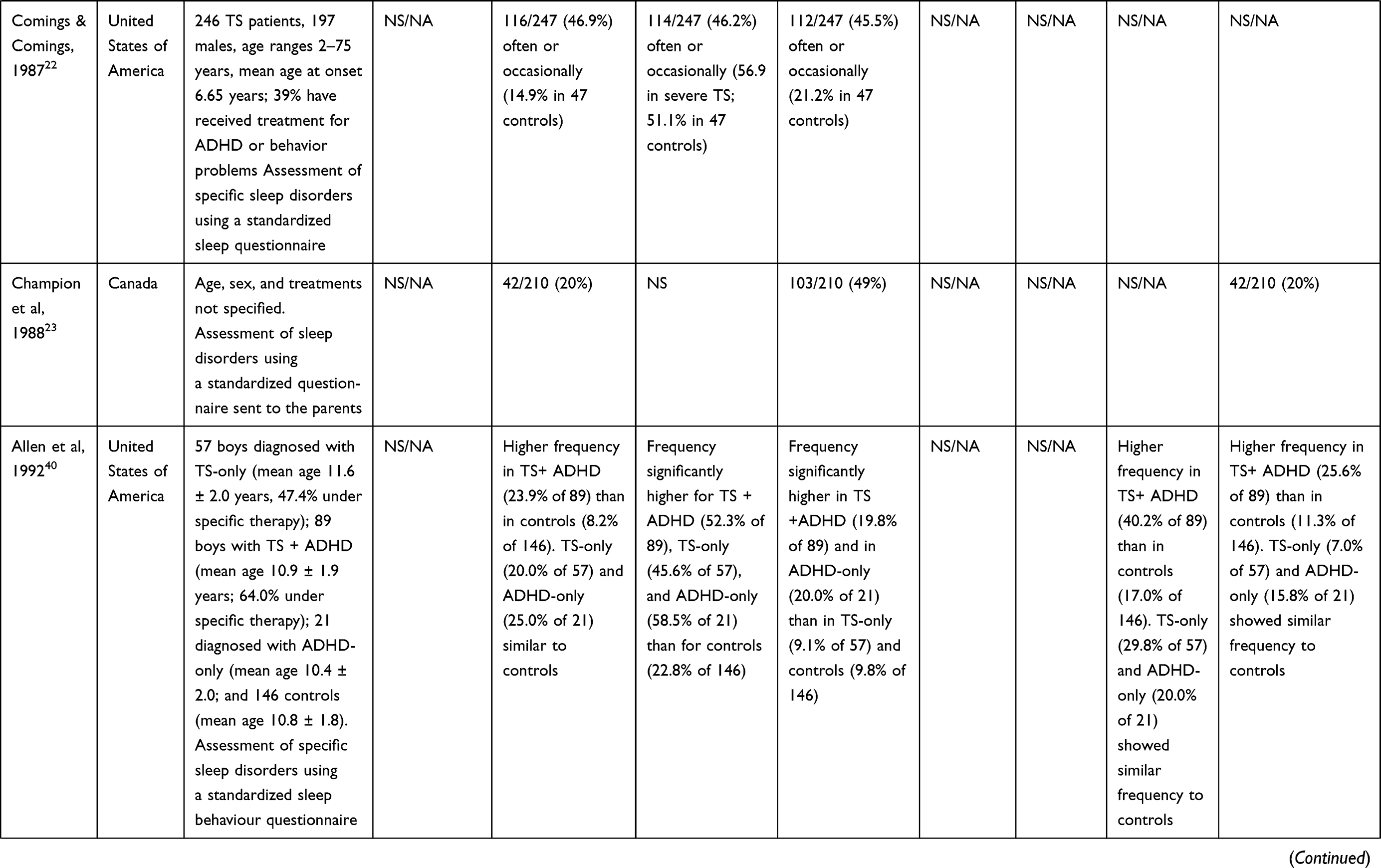 | 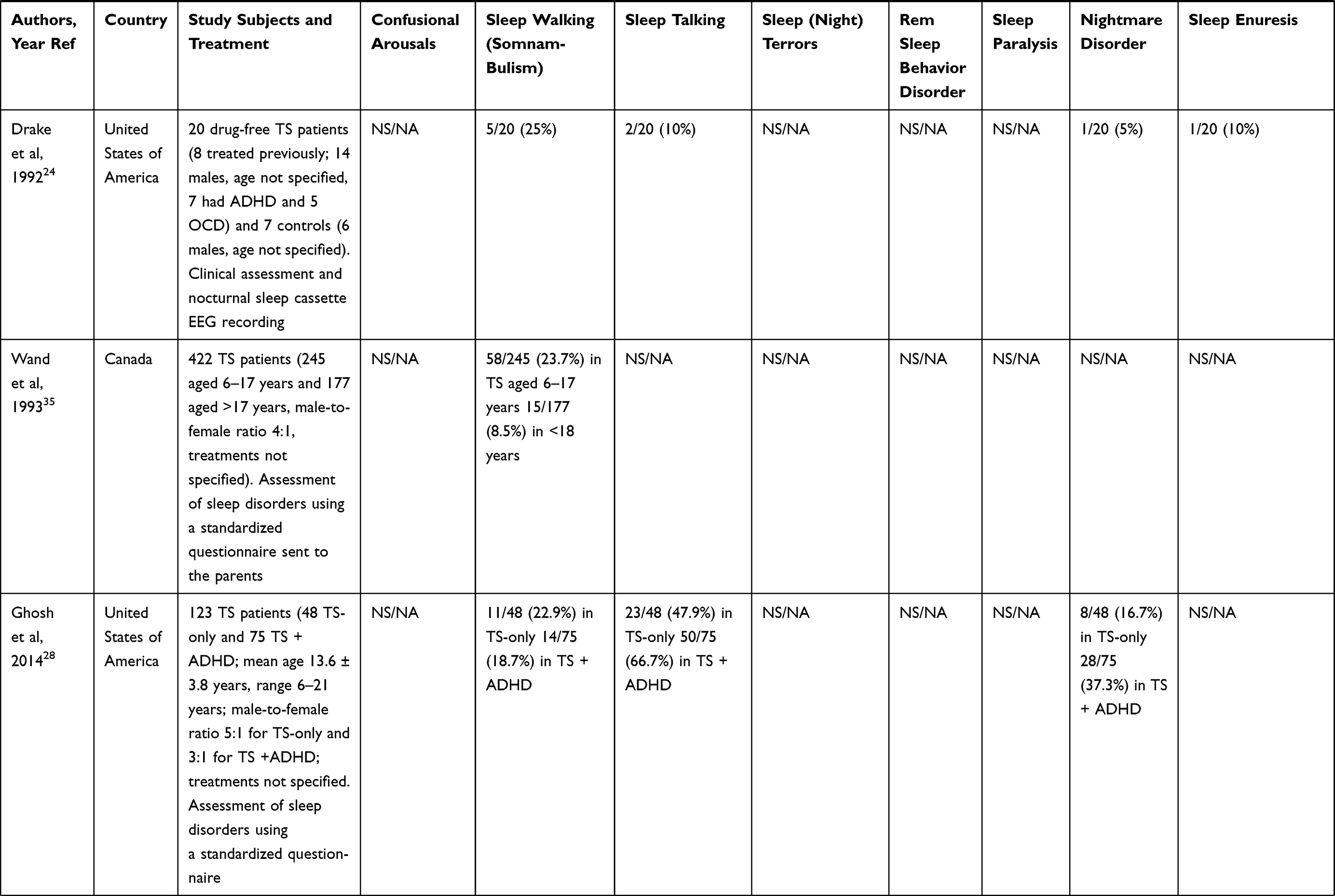 |
Table 3 Summary of Frequency of Parasomnias in Patients Diagnosed with Tourette Syndrome |
Confusional arousals, resembling those described in the seminal work by Gilles de la Tourette,6 have been described in 50% of TS patients in a short clinical series.18
The frequency of sleepwalking (somnambulism) in patients with TS found in several clinical series shows high variability, ranging from 8% to 46.0%.19,21–24,27,35,40,42 Moreover, Erenberg et al20 did not find any patients suffering from this parasomnia among 58 patients aged 15–25 years, and Modafferi et al37 reported a frequency of 5.6% in patients with tic disorders. Some authors report a 3-fold higher frequency of sleepwalking in TS patients compared with controls,22,52 and others report a significantly higher frequency in patients with TS + ADHD than in those with TS-only,28,40 in healthy controls,40 and in patients with co-occurrence migraine.43 Similarly, high variability was reported regarding the frequency of sleeptalking, which ranged from 1.7% to 47.9%,20,22,28,37,40 was significantly higher40 or did not differ significantly from that found in controls37 in two clinical series, and was higher in patients diagnosed with ADHD-only and TS + ADHD than in those with TS-only according to Allen et al.40 Finally, according to Storch et al,26 14.3% of 56 young patients with CTD or TS walked or talked during sleep.
The frequency of sleep terrors in patients with TS, which ranged from 15.8% to 49%,19,22,23,40 was significantly higher than that reported in controls37 and patients with learning disabilities or seizure disorders,19 and was even higher in patients with comorbid migraine43 and ADHD.40 Moddaferi et al37 described sleep terrors in 2.8% of patients with tic disorders and 1.1% of controls. To our knowledge, the association between sleep-related eating disorder and TS has not been reported to date.
Despite the fact that REM behaviour disorder is a very infrequent condition in children,44 Trajanovic et al45 described a boy diagnosed with TS who developed a clinical picture compatible with this disease aged 7 years. Modafferi et al37 reported a frequency of 5.6% of sleep paralysis in patients with tic disorders and 2.6% in controls, although the difference did not reach statistical significance. The frequency of nightmare disorders in TS or tic disorders, which was higher in patients with TS + ADHD,28,40 ranged from 5.4% to 46.2%.20,21,24,28,37,40 Finally, although sleep enuresis was not found in any of the 58 TS patients of a clinical series,20 other authors have reported this comorbidity in 10–20% of patients with TS or tic disorders,19,21,23,24,40 being more frequent in patients with TS + ADHD.40
Sleep-Related Movement Disorders
Alonso-Navarro et al46 recently reviewed the relationship between TS and restless legs syndrome (RLS), which were first described as coexistent disorders, together with akathisia, in a German family.47 Walters et al48 found a frequency of TS of 1.7% (similar to that described in the general population) in 118 adult patients referred with a diagnosis of RLS to a Sleep Disorders Unit. On the other hand, 10% of 144 probands diagnosed with TS or CTD chronic tics, and 23% of their parents, fulfilled diagnostic criteria for RLS, most of them being linked to paternal RLS.49 A recent study found an association between TS without concomitant OCD and 3 intronic variants in the BTB domain containing 9 gene (BTB9, chromosome 6p21.2, gene ID 114781, MIM 611237; related to the risk for RLS according to Genome-Wide Association Studies).50
Periodic limb movements during sleep (PLMS) have been reported as a frequent finding in TS patients (even more frequent in patients with TS + ADHD −32.0% than in patients with TS-only – 20.8%) in a clinical series.28 In addition, PLMS have been a frequent finding in polysomnographic studies in patients with TS,51–54 especially in those with comorbid ADHD,53 are most frequently seen in sleep stages I/II,51,52 and in many cases cause arousals.41
Restless sleep was reported in 10.7% of patients with TS21 and 38.9% of patients with tic disorders,35 this frequency being significantly higher than that found in controls.35 Another group described a significantly higher frequency of the presence of continuous movements of legs in TS patients (40.5%) than in controls (5.9%).36 Finally, according to another clinical series, “moving a lot during sleep”, which was a very frequent finding in patients with TS-only (47.4%) and in controls (44.4%), was significantly more frequent in patients with ADHD-only (84.1%) and with TS + ADHD (62.1%).40
The reported frequency of sleep-induced bruxism in TS was 2.7–10% in two clinical series,21,34 while other authors reported this symptom in 19.4% of patients with tic disorders (most of them with lower severity), a frequency that was significantly higher than that found in controls (4.1%).37 Jankovic & Rohaidy21 reported sleep-induced myoclonus in 5.4% of their patients diagnosed with TS.
Several authors reported the persistence of tics during sleep in patients with TS, with wide variability in frequency that ranged from 13.8% to 100%.18,20,21,34,52,54–56 The presence of tics during sleep has been documented in all sleep stages, having a predominance in I and II stages,52,55,56 and in the REM stage.42
Other symptoms, such as “rocking during sleep”20 and “unusual movements during sleep”,37 have been reported, respectively, in 1.72% of patients with TS and 22.2% of patients with tic disorders.
Polysomnographic Features of Sleep in Tourette Syndrome
The results of studies addressing the polysomnographic features of TS18,21,34,51–62 have been one of the aims of a recently reported review.9 In summary, the data reported with the highest consistency regarding this issue were the following:9
- Total sleep time51,56 and sleep efficiency51,53,56,61 were found to be decreased.
- Percentage in REM sleep was found to be decreased in 3 studies,18,53,56 whereas another study reported an increase of this value.54
- Four studies described a decrease in the percentage of delta sleep,34,52,57,60 while the other two studies found this value to be increased.18,56
- Six studies described an increase in nocturnal awakenings,18,34,52,53,56,61 while another involving 2 patients did not report this finding.59
- Patients with TS showed an increase in periodic limb movements during sleep (PLMS),51,52 periodic limb movements index (PLMI),51,52 and PLMS with arousal,51 this finding being more marked in patients with comorbid ADHD.54
Keenan et al10 performed a meta-analysis of 20 studies combining data from polysomnographic studies of patients with persistent tic disorders (PTD)-only (n = 198), persistent tic disorders + ADHD (n = 79), ADHD-only (n = 316), and controls (n = 336), and found the following results in comparison with controls:
- Patients with PTD + ADHD showed significantly increased time in bed, increased total sleep time, decreased sleep efficiency, increased sleep onset latency, and similar REM sleep and slow-wave sleep percentages.
- Patients with PTD-only showed significantly decreased sleep efficiency, increased sleep onset latency, and similar time in bed, total sleep time, and similar REM sleep and slow-wave sleep percentages.
- Patients with ADHD-only showed similar time in bed, total sleep time, sleep efficiency, sleep onset latency, and REM sleep and slow-wave sleep percentages.
However, the results from many of these studies could be related to the medications used.
Discussion and Conclusions
This and other reviews regarding sleep disorders7–11 and polysomnographic studies9,66 in patients with TS have important limitations due to the relatively small size of the samples studied, differences in comorbid conditions, the age of the patients included, and the medications used by the patients. While in several studies the patients were not taking any drugs for the treatment of TS at the time of evaluation,18,34,51,53,55–57,61,62 in other studies many patients used stimulants or other specific therapies for tics, which could have an important influence on the results,21,23,27,28,37,52 and in others, the treatment was not clearly specified.19,20,24–26,30,32,33,35–37,59
Patients diagnosed with TS or CTD, especially children, and those who have comorbidities such as ADHD or ADHD + OCD, suffer from one or more types of sleep disorders with a high frequency. Although the frequency of sleep disorders in patients with TS is widely variable among different studies, the most frequently reported are insomnia, excessive daytime sleepiness, the persistence of tics during sleep, different disorders of arousal, and the presence of PLMS.9 Decreased sleep efficiency and increased sleep onset latency are the most frequent findings in TS patients with or without comorbid ADHD according to a recent meta-analysis.10
While the severity of TS or tic disorders has been assessed by several of the studies included in this review,12,23,26,27,32,35,37,53,62 the possible relationship between sleep disorders and the severity of the disease has been addressed by few of them.22,25,27,32,37 A negative correlation between the number of sleep-related problems and the severity of motor tics, assessed with the YGTSS, was reported by Storch et al.26 Other authors reported that the interaction between age, sex, and severity of tic disorders could be a reliable predictor of the presence of sleep insufficiency.32 Two reports described that patients with higher severity of TS have shown both higher total sleep scores,22,27 and higher frequency of sleep problems according to Comings & Commings,22 while another found that patients with lower severity of tic disorders, assessed by the YGTSS, showed more frequent difficulty in initiating sleep, nightmares, night awakenings, sleeptalking, bruxism, and unusual movement disorders compared with patients with higher severity of tics.
The contribution of anxiety to sleep disorders in TS has been addressed by 3 studies,26,30,37 despite the fact that these and many others have shown a high frequency of anxiety as a comorbid condition in TS (11%–70%).22–24,26,27,30,32,33,35–37 Patients with CTD with comorbid anxiety have shown a higher frequency of sleep-related problems when compared with those without this comorbidity, according to Storch et al.26 TS or CTD patients with higher scores on an anxiety scale were more prone to present abnormal movements during or before sleep, according to Modafferi et al.37 Finally, in a population-based study, patients recently diagnosed with TS showed a significant association between anxiety disorders and sleep disorders.30
Although it is beyond the scope of this review to analyze sleep disorders in patients with ADHD-only, and taking into account that ADHD is a frequent comorbidity of TS and CTD, it is reasonable to think that ADHD could contribute to sleep disorders/problems in TS/CTD. According to sleep questionnaires, patients with ADHD-only showed a wide range of frequent sleep disturbances.40,63,64 Several case–control studies reported a higher frequency of PLMS in patients with ADHD than in controls,65,66 a finding that was not confirmed by others,67 and patients with RLS have shown a higher frequency of ADHD symptoms using DSM-IV ADHD scores.68 Bioulac et al69 described higher ESS and Maintenance of Wakefulness Test scores in patients with ADHD-only. Large population studies have shown that patients with ADHD symptoms report slower sleep duration, longer sleep latency and nocturnal wake time, longer sleep efficiency,70 increased odds of insomnia,70,71 poorer sleep quality,72 and higher odds of suffering probable obstructive sleep apnea syndrome, RLS, and PLMS.71 Despite the fact that many PSG and actigraphy studies have shown different alterations in patients with ADHD-only,53,54,64–66,73–75 other studies do not show significant alterations.63,67,76 Moreover, a meta-analysis of studies using PSG or actigraphy showed that ADHD-only patients spent more time in stage 1 than controls as the only finding,77 while another found no differences in PSG parameters between the two groups.10
To our knowledge, neither formal specific studies nor guidelines on the approach to the treatment of sleep disorders/problems exist for TS. As was suggested in a recent review, treatment of tics and comorbid conditions that can worsen sleep in patients with TS/CTD, such as obstructive sleep apnea syndrome, ADHD, RLS, and so on, could result in an improvement of sleep complaints, and several drugs used for the improvement of tics such as clonidine, clonazepam, topiramate, aripiprazole, risperidone, or others could potentially improve sleep.11
To our knowledge, despite the fact that Modafferi et al40 used a validated global sleep questionnaire, studies addressing the quality of sleep (which could be assessed with the Pittsburgh sleep quality index –PSQI-,78 or other well-validated scales), and/or looking for the presence of excessive daytime somnolence (for example, the Epworth Sleepiness Scale or ESS79) in patients diagnosed with TS or CTD, are still lacking.
Future assessments of sleep disorders in TS/CTD should ideally be multicenter, prospective, with long-term follow-up and multicenter studies, involving large samples of drug-free TS/CTD patients (at least at the time of recruitment) and age- and sex-matched controls without a family history of tics, using multiple sleep disorders screening questionnaires,80–83 the PSQI,78 the ESS,79 and questionnaires on the presence of RLS84 and REM sleep behaviour disorders,85 together with objective assessment using nocturnal polysomnographic studies and/or actigraphy.
Abbreviations
ADHD, attention deficit hyperactivity disorder; BTBD9, BTB domain containing 9 gene; HCRTR2, orexin2/hypocretine 2 receptor gene; ECG, electrocardiogram; EEG, electroencephalogram; EMG, electromyogram; EOG, electrooculogram; NREM, non-rapid eye movements; OCD, obsessive-compulsive disorder; PLMI, periodic limb movements index; PLMS, periodic limb movements during sleep; REM, rapid eye movements; RLS, restless legs syndrome; TD, Tourette disorder; TS, Tourette syndrome; YGTSS, Yale global tic severity scale.
Acknowledgments
We thank Prof. James McCue for revising the English language. We appreciate the efforts of the staff of the Library of Hospital Universitario del Sureste, Arganda del Rey (Madrid, SPAIN), who obtained an important number of papers for us.
Funding
This authors’ laboratory work was supported in part by Grants RETICS RD16/0006/0004 (ARADyAL), PI18/00540, and PI21/01683 from Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Madrid, Spain and IB20134 and GR21073 from Junta de Extremadura, Mérida, Spain. Partially funded with FEDER funds.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Jiménez-Jiménez FJ, Alonso-Navarro H, Plaza-Nieto JF, Pilo de la Fuente B, Síndrome de T. Tratado de los Trastornos del Movimiento.
2. Walusinski O. Georges Gilles de la Tourette: Beyond the Eponym. Oxford: Oxford University Press; 2018.
3. Novotny M, Valis M, Klimova B. Tourette syndrome: a mini-review. Front Neurol. 2018;9:139. doi:10.3389/fneur.2018.00139
4. Robertson MM, Eapen V, Singer HS, et al. Gilles de la Tourette syndrome. Nat Rev Dis Primers. 2017;3:16097. doi:10.1038/nrdp.2016.97
5. Robertson MM. A personal 35 year perspective on Gilles de la Tourette syndrome: prevalence, phenomenology, comorbidities, and coexistent psychopathologies. Lancet Psychiatry. 2015;2:68–87. doi:10.1038/nrdp.2016.97
6. Lajonchere C, Nortz M, Finger S. Gilles de la Tourette and the discovery of Tourette syndrome. Includes a translation of his 1884 article. Arch Neurol. 1996;53:567–574. doi:10.1001/archneur.1996.00550060111024
7. Kirov R, Becker A, Rothenberger A. Sleep in Tourette syndrome. Curr Dev Disord Rep. 2014;1:252–259. doi:10.1007/s40474-014-0028-0
8. Hibberd C, Charman T, Bhatoa RS, et al. Sleep difficulties in children with Tourette syndrome and chronic tic disorders: a systematic review of characteristics and associated factors. Sleep. 2020;43(6):zsz308. doi:10.1093/sleep/zsz308
9. Jiménez-Jiménez FJ, Alonso-Navarro H, García-Martín E, Agúndez JAG. Sleep disorders in Tourette syndrome. Sleep Med Rev. 2020;53:101335. doi:10.1016/j.smrv.2020.101335
10. Keenan L, Sherlock C, Bramham J, Downes M. Overlapping sleep disturbances in persistent tic disorders and attention-deficit hyperactivity disorder: a systematic review and meta-analysis of polysomnographic findings. Neurosci Biobehav Rev. 2021;126:194–212. doi:10.1016/j.neubiorev.2021.03.018
11. Blaty JL, DelRosso LM. Tourette disorder and sleep. Biomed J. 2022;45(22):240–249. doi:10.1016/j.bj.2022.01.002
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
13. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
14. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146:1387–1394. doi:10.1378/chest.14-0970
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi:10.1371/journal.pmed.1000097
16. Moldofsky H, Tullis C, Lamon R. Multiple tic syndrome (Giles de la Tourette’s syndrome). J Nerv Ment Dis. 1974;159:282–292. doi:10.1097/00005053-197410000-00007
17. Nee LE, Caine ED, Polinsky RJ, Eldridge R, Ebert MH. Gilles de la Tourette syndrome: clinical and family study of 50 cases. Ann Neurol. 1980;7:41–49. doi:10.1002/ana.410070109
18. Glaze DG, Frost JD
19. Barabas G, Matthews WS, Ferrari M. Disorders of arousal in Gilles de la Tourette’s syndrome. Neurology. 1984;34:815–817. doi:10.1212/wnl.34.6.815
20. Erenberg G. Sleep disorders in Gilles de la Tourette’s syndrome. Neurology. 1985;35:1397. doi:10.1212/wnl.35.9.1397-a
21. Jankovic J, Rohaidy H. Motor, behavioral and pharmacologic findings in Tourette’s syndrome. Can J Neurol Sci. 1987;14(3 Suppl):541–546. doi:10.1017/s0317167100038087
22. Comings DE, Comings BG. A controlled study of Tourette syndrome. VI. Early development, sleep problems, allergies, and handedness. Am J Hum Genet. 1987;41:822–828.
23. Freeman RD, Fast DK, Burd L, Kerbeshian J, Robertson MM, Sandor P. An international perspective on Tourette syndrome: selected findings from 3500 individuals in 22 countries. Dev Med Child Neurol. 2000;42:436–447. doi:10.1017/s0012162200000839
24. Teive HA, Germiniani FM, Della Coletta MV, Werneck LC. Tics and Tourette syndrome: clinical evaluation of 44 cases. Arq Neuropsiquiatr. 2001;59:725–728. doi:10.1590/s0004-282x2001000500014
25. Saccomani L, Fabiana V, Manuela B, Giambattista R. Tourette syndrome and chronic tics in a sample of children and adolescents. Brain Dev. 2005;27:349–352. doi:10.1016/j.braindev.2004.09.007
26. Storch EA, Merlo LJ, Lack C, et al. Quality of life in youth with Tourette’s syndrome and chronic tic disorder. J Clin Child Adolesc Psychol. 2007;36:217–227. doi:10.1080/15374410701279545
27. Mol Debes NM, Hjalgrim H, Skov L. Validation of the presence of comorbidities in a Danish clinical cohort of children with Tourette syndrome. J Child Neurol. 2008;23:1017–1027. doi:10.1177/0883073808316370
28. Ghosh D, Rajan PV, Das D, Datta P, Rothner AD, Erenberg G. Sleep disorders in children with Tourette syndrome. Pediatr Neurol. 2014;51:31–35. doi:10.1016/j.pediatrneurol.2014.03.017
29. Sambrani T, Jakubovski E, Müller-Vahl KR. New insights into clinical characteristics of Gilles de la Tourette syndrome: findings in 1032 patients from a single German center. Front Neurosci. 2016;10:415. doi:10.3389/fnins.2016.00415
30. Lee WT, Huang HL, Wong LC, et al. Tourette syndrome as an independent risk factor for subsequent sleep disorders in children: a nationwide population-based case-control study. Sleep. 2017;40(3). doi:10.1093/sleep/zsw072
31. Groth C, Mol Debes N, Rask CU, Lange T, Skov L. Course of Tourette syndrome and comorbidities in a large prospective clinical study. J Am Acad Child Adolesc Psychiatry. 2017;56(4):304–312. doi:10.1016/j.jaac.2017.01.010
32. Ricketts EJ, Rozenman MR, Choi C, et al. Sleep sufficiency in pediatric and adolescent Tourette’s disorder: national survey of Children’s Health. J Dev Behav Pediatr. 2018;39:72–76. doi:10.1097/DBP.0000000000000518
33. Champion LM, Fulton WA, Shady GA. Tourette syndrome and social functioning in a Canadian population. Neurosci Biobehav Rev. 1988;12:255–257. doi:10.1016/s0149-7634(88)80054-x
34. Drake ME
35. Wand RR, Matazow GS, Shady GA, Furer P, Staley D. Tourette syndrome: associated symptoms and most disabling features. Neurosci Biobehav Rev. 1993;17:271–275. doi:10.1016/s0149-7634(05)80010-7
36. Romano A, Cundari G, Bruni O, et al. Disturbe de tic e disturbi dell’arousal. Valutazione clinica di 49 bambini e adolescenti. Minerva Pediatr. 2004;56:327–334.
37. Modafferi S, Stornelli M, Chiarotti F, Cardona F, Bruni O. Sleep, anxiety and psychiatric symptoms in children with Tourette syndrome and tic disorders. Eur J Paediatr Neurol. 2016;20:696–703. doi:10.1016/j.ejpn.2016.05.003
38. Isomura K, Sidorchuk A, Sevilla-Cermeño L, et al. Insomnia in Tourette syndrome and chronic tic disorder. Mov Disord. 2022;37:392–400. doi:10.1002/mds.28842
39. Sverd J, Montero G. Is Tourette syndrome a cause of sudden infant death syndrome and childhood obstructive sleep apnea? Am J Med Genet. 1993;46:494–496. doi:10.1002/ajmg.1320460506
40. Allen RP, Singer HS, Brown JE, Salam MM. Sleep disorders in Tourette syndrome: a primary or unrelated problem? Pediatr Neurol. 1992;8:275–280. doi:10.1016/0887-8994(92)90365-6
41. Thompson MD, Comings DE, Abu-Ghazalah R, et al. Variants of the orexin2/hcrt2 receptor gene identified in patients with excessive daytime sleepiness and patients with Tourette’s syndrome comorbidity. Am J Med Genet B Neuropsychiatr Genet. 2004;129B:69–75. doi:10.1002/ajmg.b.30047
42. Barabas G, Matthews WS, Ferrari M. Somnambulism in children with Tourette syndrome. Dev Med Child Neurol. 1984;26:457–460. doi:10.1111/j.1469-8749.1984.tb04471.x
43. Barabas G, Matthews WS. Homogeneous clinical subgroups in children with Tourette syndrome. Pediatrics. 1985;75:73–75. doi:10.1542/peds.75.1.73
44. Jiménez-Jiménez FJ, Alonso-Navarro H, García-Martín E, Agúndez JAG. Neurochemical features of rem sleep behaviour disorder. J Pers Med. 2021;11(9):880. doi:10.3390/jpm11090880
45. Trajanovic NN, Voloh I, Shapiro CM, Sandor P. REM sleep behaviour disorder in a child with Tourette’s syndrome. Can J Neurol Sci. 2004;31:572–575. doi:10.1017/s031716710000384x
46. Alonso-Navarro H, García-Martín E, Agúndez JAG, Jiménez-Jiménez FJ. Association between restless legs syndrome and other movement disorders. Neurology. 2019;92:948–964. doi:10.1212/WNL.0000000000007500
47. Müller N, Voderholzer U, Kurtz G, Straube A. Tourette’s syndrome associated with restless legs syndrome and akathisia in a family. Acta Neurol Scand. 1994;89:429–432. doi:10.1111/j.1600-0404.1994.tb02661.x
48. Walters AS, LeBrocq C, Passi V, et al. A preliminary look at the percentage of patients with restless legs syndrome who also have Parkinson's disease, essential tremor or Tourette syndrome in a single practice. J Sleep Res. 2003;12:343–345. doi:10.1046/j.0962-1105.2003.00368.x
49. Lespérance P, Djerroud N, Diaz Anzaldua A, Rouleau GA, Chouinard S, Richer F; Montréal Tourette Study Group. Restless legs in Tourette syndrome. Mov Disord. 2004;19:1084–1087. doi:10.1002/mds.20100
50. Rivière JB, Xiong L, Levchenko A, et al. Association of intronic variants of the BTBD9 gene with Tourette syndrome. Arch Neurol. 2009;66:1267–1272. doi:10.1001/archneurol.2009.213
51. Voderholzer U, Müller N, Haag C, Riemann D, Straube A. Periodic limb movements during sleep are a frequent finding in patients with Gilles de la Tourette’s syndrome. J Neurol. 1997;244:521–526. doi:10.1007/s004150050136
52. Cohrs S, Rasch T, Altmeyer S, et al. Decreased sleep quality and increased sleep related movements in patients with Tourette’s syndrome. J Neurol Neurosurg Psychiatry. 2001;70:192–197. doi:10.1136/jnnp.70.2.192
53. Kirov R, Kinkelbur J, Banaschewski T, Rothenberger A. Sleep patterns in children with attention-deficit/hyperactivity disorder, tic disorder, and comorbidity. J Child Psychol Psychiatry. 2007;48:561–570. doi:10.1111/j.1469-7610.2007.01729.x
54. Stephens RJ, Chung SA, Jovanovic D, et al. Relationship between polysomnographic sleep architecture and behavior in medication-free children with TS, ADHD, TS and ADHD, and controls. J Dev Behav Pediatr. 2013;34:688–696. doi:10.1097/DBP.0000000000000012
55. Silvestri R, De Domenico P, Di Rosa AE, Bramanti P, Serra S, Di Perri R. The effect of nocturnal physiological sleep on various movement disorders. Mov Disord. 1990;5:8–14. doi:10.1002/mds.870050104
56. Silvestri R, Raffaele M, De Domenico P, et al. Sleep features in Tourette’s syndrome, neuroacanthocytosis and Huntington’s chorea. Neurophysiol Clin. 1995;25:66–77. doi:10.1016/0987-7053(96)81034-3
57. Mendelson WB, Caine ED, Goyer P, Ebert M, Gillin JC. Sleep in Gilles de la Tourette syndrome. Biol Psychiatry. 1980;15:339–343.
58. Hashimoto T, Endo S, Fukuda K, et al. Increased body movements during sleep in Gilles de la Tourette syndrome. Brain Dev. 1981;3:31–35. doi:10.1016/s0387-7604(81)80003-4
59. Fish DR, Sawyers D, Allen PJ, Blackie JD, Lees AJ, Marsden CD. The effect of sleep on the dyskinetic movements of Parkinson’s disease, Gilles de la Tourette syndrome, Huntington’s disease, and torsion dystonia. Arch Neurol. 1991;48:210–214. doi:10.1001/archneur.1991.00530140106023
60. Moeller AA, Krieg JC. Sleep EEG in Gilles de la Tourette’s syndrome. J Neurol. 1992;239:113. doi:10.1007/BF00862987
61. Kostanecka-Endress T, Banaschewski T, Kinkelbur J, et al. Disturbed sleep in children with Tourette syndrome: a polysomnographic study. J Psychosom Res. 2003;55:23–29. doi:10.1016/s0022-3999(02)00602-5
62. Kirov R, Brand S, Banaschewski T, Rothenberger A. Opposite impact of REM sleep on neurobehavioral functioning in children with common psychiatric disorders compared to typically developing children. Front Psychol. 2017;7:2059. doi:10.3389/fpsyg.2016.02059
63. Wiggs L, Montgomery P, Stores G. Actigraphic and parent reports of sleep patterns and sleep disorders in children with subtypes of attention-deficit hyperactivity disorder. Sleep. 2005;28(11):1437–1445. doi:10.1093/sleep/28.11.1437
64. Moreau V, Rouleau N, Morin CM. Sleep of children with attention deficit hyperactivity disorder: actigraphic and parental reports. Behav Sleep Med. 2014;12(1):69–83. doi:10.1080/15402002.2013.764526
65. Picchietti DL, England SJ, Walters AS, Willis K, Verrico T. Periodic limb movement disorder and restless legs syndrome in children with attention-deficit hyperactivity disorder. J Child Neurol. 1998;13(12):588–594. doi:10.1177/088307389801301202
66. Philipsen A, Feige B, Hesslinger B, et al. Sleep in adults with attention-deficit/hyperactivity disorder: a controlled polysomnographic study including spectral analysis of the sleep EEG. Sleep. 2005;28(7):877–884. doi:10.1093/sleep/28.7.877
67. Sangal RB, Owens JA, Sangal J. Patients with attention-deficit/hyperactivity disorder without observed apneic episodes in sleep or daytime sleepiness have normal sleep on polysomnography. Sleep. 2005;28(9):1143–1148.
68. Wagner ML, Walters AS, Fisher BC. Symptoms of attention-deficit/hyperactivity disorder in adults with restless legs syndrome. Sleep. 2004;27(8):1499–1504. doi:10.1093/sleep/27.8.1499
69. Bioulac S, Chaufton C, Taillard J, et al. Excessive daytime sleepiness in adult patients with ADHD as measured by the maintenance of wakefulness test, an electrophysiologic measure. J Clin Psychiatry. 2015;76(7):943–948. doi:10.4088/JCP.14m09087
70. Hysing M, Lundervold AJ, Posserud MB, Sivertsen B. Association between sleep problems and symptoms of attention deficit hyperactivity disorder in adolescence: results from a large population-based study. Behav Sleep Med. 2016;14(5):550–564. doi:10.1080/15402002.2015.1048448
71. Vogel SWN, Bijlenga D, Benjamins JS, Beekman ATF, Kooij JJS, Van Someren EJW. Attention deficit hyperactivity disorder symptom severity and sleep problems in adult participants of the Netherlands sleep registry. Sleep Med. 2017;40:94–102. doi:10.1016/j.sleep.2017.09.027
72. Gregory AM, Agnew-Blais JC, Matthews T, Moffitt TE, Arseneault L. ADHD and sleep quality: longitudinal analyses from childhood to early adulthood in a Twin Cohort. J Clin Child Adolesc Psychol. 2017;46(2):284–294. doi:10.1080/15374416.2016.1183499
73. Kirov R, Uebel H, Albrecht B, Banaschewski T, Yordanova J, Rothenberger A. Attention-deficit/hyperactivity disorder (ADHD) and adaptation night as determinants of sleep patterns in children. Eur Child Adolesc Psychiatry. 2012;21(12):681–690. doi:10.1007/s00787-012-0308-3
74. Miano S, Amato N, Foderaro G, et al. Sleep phenotypes in attention deficit hyperactivity disorder. Sleep Med. 2019;60:123–131. doi:10.1016/j.sleep.2018.08.026
75. Kapoor V, Ferri R, Stein MA, Ruth C, Reed J, DelRosso LM. Restless sleep disorder in children with attention-deficit/hyperactivity disorder. J Clin Sleep Med. 2021;17(4):639–643. doi:10.5664/jcsm.8984
76. Prihodova I, Paclt I, Kemlink D, Skibova J, Ptacek R, Nevsimalova S. Sleep disorders and daytime sleepiness in children with attention-deficit/hyperactivity disorder: a two-night polysomnographic study with a multiple sleep latency test. Sleep Med. 2010;11(9):922–928. doi:10.1016/j.sleep.2010.03.017
77. Díaz-Román A, Hita-Yáñez E, Buela-Casal G. Sleep characteristics in children with attention deficit hyperactivity disorder: systematic review and meta-analyses. J Clin Sleep Med. 2016;12(5):747–756. doi:10.5664/jcsm.5810
78. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
79. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–545. doi:10.1093/sleep/14.6.540
80. Kerkhof GA, Geuke MEH, Brouwer A, Rijsman RM, Schimsheimer RJ, Van Kasteel V. Holland sleep disorders questionnaire: a new sleep disorders questionnaire based on the international classification of sleep disorders-2. J Sleep Res. 2013;22:104–107. doi:10.1111/j.1365-2869.2012.01041.x
81. Spoormaker VI, Verbeek I, van den Bout J, Klip EC. Initial validation of the SLEEP-50 questionnaire. Behav Sleep Med. 2005;3(4):227–246. doi:10.1207/s15402010bsm0304_4
82. Roth T, Zammit G, Kushida C, et al. A new questionnaire to detect sleep disorders. Sleep Med. 2002;3:99–108. doi:10.1016/s1389-9457(01)00131-9
83. Klingman KJ, Jungquist CR, Perlis ML. Questionnaires that screen for multiple sleep disorders. Sleep Med Rev. 2017;32:37–44. doi:10.1016/j.smrv.2016.02.004
84. Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria–history, rationale, description, and significance. Sleep Med. 2014;15:860–873. doi:10.1016/j.sleep.2014.03.025
85. Stiasny-Kolster K, Mayer G, Schäfer S, Möller JC, Heinzel-Gutenbrunner M, Oertel WH. The REM sleep behavior disorder screening questionnaire: a new diagnostic instrument. Mov Disord. 2007;22:2386–2393. doi:10.1002/mds.21740
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.