Back to Journals » Nature and Science of Sleep » Volume 17

Sleep-Disordered Breathing as a Mediator Between Premature Birth and Behavior Problems in School-Aged Children: A Cross-Sectional Study of 6–10 Year Olds in Shanghai, China
Authors Hu Y ![]() , Jiang S, Yang S, Wang C, Zou J, Guan J, Liu Y
, Jiang S, Yang S, Wang C, Zou J, Guan J, Liu Y ![]() , Lu Q
, Lu Q
Received 19 May 2025
Accepted for publication 4 September 2025
Published 8 October 2025 Volume 2025:17 Pages 2599—2610
DOI https://doi.org/10.2147/NSS.S539617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yuli Hu,1,2,* Siqiong Jiang,1,* Shiyin Yang,3 Chunsheng Wang,4 Jianyin Zou,5 Jian Guan,5 Yupu Liu,5 Qunfeng Lu1,2
1Nursing Department of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Xuhui, Shanghai, 200233, People’s Republic of China; 2School of Nursing, Shanghai Jiaotong University, Shanghai, 200025, People’s Republic of China; 3Children’s Medical Center Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200127, People’s Republic of China; 4School of Medicine, Huzhou University, Zhejiang, 310000, People’s Republic of China; 5Department of Otolaryngology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yupu Liu, Email [email protected] Qunfeng Lu, Email [email protected]
Background: Premature birth poses a major challenge in global obstetric clinical practice. The relationship between preterm infants and behavioral problems in school-aged children remains debatable, and the mediating role of sleep-disordered breathing (SDB) in this connection has not been investigated. This study aimed to address these gaps through a large-scale cross-sectional survey.
Methods: We recruited 18,138 children aged 6– 10 from schools. Data on demographics, prematurity, SDB, and childhood behavioral problems were collected. The Paediatric Sleep Questionnaire (PSQ), a validated screening tool, assessed SDB symptoms, and the Conners’ Parent Rating Scale (CPRS) evaluated behavioral problems. Path analysis with bootstrap methods was used for statistical analysis.
Results: Among 18,138 participants, 8% (n = 1,450) were premature. After adjusting for age, gender, BMI z-score, maternal age, and maternal education level, prematurity showed a positive association with total PSQ score (B = 0.411, p < 0.01). Higher total PSQ scores were significantly associated with all six CPRS dimensions (all p < 0.05). While prematurity was not directly associated with Conduct, Psychosomatic, Impulsive-hyperactive, or Hyperactivity scores in CPRS (all p > 0.05), it demonstrated significant associations with Learning problems (β = 0.063, p = 0.005) and Anxiety scores (β = 0.076, p = 0.003). Mediation analysis showed PSQ accounted for a large proportion of associations between prematurity and Conduct, Psychosomatic, Impulsive – hyperactive, and Hyperactivity problems (95% Bootstrap CI excluded 0).
Conclusion: Premature infants may exhibit behavioral problems significantly associated with SDB, though our cross-sectional design precludes causal inference and parent-reported SDB severity may bias true associations. Future studies should utilize longitudinal cohorts to explore whether SDB is involved in the relationship between prematurity and behavioral problems (eg, anxiety). Additionally, they should conduct pilot randomized controlled trials of SDB interventions in preterm infants to assess neurodevelopmental benefits. Final conclusions require subsequent causal validation.
Keywords: premature birth, behavioral problems, sleep-disordered breathing
Introduction
Preterm birth (<37 + 0 weeks of gestation) disrupts the normal process of organogenesis in foetuses, resulting in a wide range of multisystem disorders and long-term consequences.1 In 2010, an estimated 14.9 million babies (with an uncertainty range of 12.3 to 18.1 million) were born preterm, accounting for 11.1% of all live births globally, with rates ranging from about 5% in several European countries to 18% in some African countries.2,3 Complications in premature infants include lung function impairments, such as altered airway mechanics and significant reductions in pulmonary function, growth disturbances including growth retardation, neurodevelopmental impairments characterized by cognitive dysfunction, behavioural issues, mental health problems, and motor disorders such as cerebral palsy and related conditions.4–7
Sleep-disordered breathing (SDB) affects approximately 4–11% of term-born infants.8 Premature infants, however, are 3–5 times more likely to develop SDB compared to term-born infants9. SDB, marked by upper airway collapse during sleep, mainly manifests as primary snoring (PS, a mild condition with loud snoring and minimal self-health impact) and obstructive sleep apnoea syndrome (OSAS, a severe one with recurrent apnea/hypopnea and multiple complications, diagnosed via polysomnography).10,11 Risk factors for SDB include adenoid and tonsil hypertrophy, allergic rhinitis, obesity, among others.12–14 Attaching importance to these factors is conducive to early screening, early treatment, and early recovery.
In recent years, internalizing and externalizing problems have garnered significant attention. Studies have indicated that children with SDB often exhibit behavioural challenges, including hyperactivity, inattention15,16 externalizing behaviours such as aggression and rule-breaking17,18 and internalizing issues such as anxiety, depression, somatic complaints, and social difficulties.19,20 These symptoms significantly impact children’s current and future social functioning. Regarding behavioral problems, premature infants are more likely to experience behavioral challenges and related issues during childhood.21,22 However, there were also studies that put forward different viewpoints. One study exploring the impact of different perinatal morbidity rates on the school performance of 12-year-old premature infants found that all premature infant groups performed comparably to the full-term infant group in terms of social skills and problematic behaviors, with no significant differences observed.23 Another study on the cognitive and behavioral outcomes of school-aged extremely preterm (EP) children revealed that, except for lower social maturity, there were no significant differences in behavioral problems between EP children and their full-term peers.24 These inconsistent findings emphasize the necessity of further exploring the relationship between premature infants and the behavior of school-aged children in large community samples, while utilizing standardized tools to assess behavior problems and taking into account necessary covariates. Therefore, this study hypothesized that SDB may act as a mediator in the relationship between prematurity and behavioral problems in school-aged children.
Exploring the relationships among prematurity, sleep-disordered breathing, and behavioral problems in school-age children was conducive to a deeper understanding of their connections, and this understanding could provide a foundation for targeted and diversified intervention strategies.
At the same time, it helped clinical personnel and families of affected children to recognize the need for attention when premature infants exhibited sleep-disordered breathing.
Methods
Study Design and Setting
This was a cross-sectional investigation conducted in Xuhui District, Shanghai, China.
Participants
Invitation letters were sent to the administrative offices of all 47 primary schools in the district. Of these, 13 schools declined to participate. As a result, the initial sample included 26,827 registered primary school students from 34 schools. Between September and December 2019, class teachers distributed informed consent forms and an online questionnaire with a QR code to the guardians of each student. A total of 19,033 guardians agreed to participate and completed the online survey, yielding a consent rate of 71.0%. For the purposes of this analysis, 18,138 children in grades one to five, aged 6–10 years, were selected as study participants. Missing data, such as incomplete body mass index (BMI) z-scores, maternal age, and maternal education level, were excluded from the analysis.
Class teachers distributed informed consent forms and online questionnaires, which included login codes, to the guardians of each student. The guardians provided demographic information, medical history, and responses to the PSQ and CPRS through the online survey. Anthropometric data, including height and weight, measured within the previous 3 months, were obtained from the physical examination database of the Shanghai Municipal Education Commission. Informed consent was obtained from all parents of the children through the online platform.
Ethics Approval
The study protocol was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University (Approval No: 2018–008). Class teachers distributed informed consent forms and online questionnaires, which included login codes, to the guardians of each student. Informed consent was obtained from all parents of the children through the online platform.
Measurement Tools and Research Variables
Demographic Characteristics
The questionnaire included items designed to assess demographic characteristics, such as age, sex, and maternal education level. WHO Anthro Plus software was used to calculate age- and sex-adjusted BMI z-scores (SD scores).25 The covariates included in this study are age, sex, BMI z-score, mother’s age, and education level. During data collection, we lacked procedures to capture potential unmeasured confounders like socioeconomic status and perinatal complications, but will consider including them in future research. Additionally, some parental health condition data were missing and unusable, so we did not incorporate them into the analysis.
Prematurity
In accordance with Chinese guidelines, preterm birth was defined as delivery occurring after 28 weeks, but before 37 completed weeks of gestation.26 Information regarding prematurity was collected via the online questionnaire. Guardians were asked, “Has your child been diagnosed with prematurity by a doctor?” If the response was affirmative, further details were gathered by asking, “Was the gestational age more than 28 weeks, but less than 37 weeks26?” If the guardian responded affirmatively, additional relevant information was collected.
Sleep Problems and High Risk of SDB Symptoms
The PSQ includes a sleep-related breathing disturbance (SRBD) scale and is widely used to screen for SDB in children aged 2–18 years.27 In this study, the presence or absence of each symptom was indicated by different scores, with “Yes” scored as 1, “No” scored as 0, and “Don’t Know” recorded as a missing value. The final score was derived by calculating the average score of non-missing items across all entries. A cut-off value of 0.33 was found to be most effective for screening and classifying children with SDB, specifically paediatric OSAS.28 The Chinese version of the PSQ demonstrated good sensitivity (77.6%) and specificity (86.7%).29 SDB screening was conducted using the PSQ, where a score of >7/22 symptoms indicated a higher risk of SDB diagnosis. In this study, a PSQ score of ≥8 was considered abnormal.29 We have obtained permission to use the Chinese version of the PSQ questionnaire. A systematic review30 shows that the PSQ exhibits higher sensitivity (0.76) compared to the OSA-18 (0.56) in identifying children with obstructive sleep apnea (OSA). This higher sensitivity reduces the likelihood of missed diagnoses during initial screening, rendering the PSQ an excellent choice for large-scale studies. The PSQ questionnaire takes relatively little time to complete and was well-received by parents, making it suitable for use in home or community settings. It encompasses respiratory symptoms, daytime sleepiness, and behavioral issues associated with SDB. We chose the PSQ questionnaire to evaluate OSA mainly because of its superior accuracy.
Behavioral Outcomes
The Conners’ Parent Rating Scale (CPRS) was used to assess common behavioral problems. The CPRS consists of 48 items encompassing six factors: conduct problems, learning problems, psychosocial problems, impulsive—hyperactive, hyperactivity, and anxiety.31 Each item is rated on a 4-point scale ranging from 0 to 3, with higher scores indicating more pronounced behavioral problems. The CPRS scale was used only for non-commercial academic research. For transparency and accountability, the original paper of the CPRS31 and the Chinese version used in the study were properly cited. To ensure homogeneity in the scale scores, the scores for each dimension of the scale were standardized, and these standardized scores were used as the dependent variable values for the analysis in this study. To standardize the CPRS scores, the mean (M) and standard deviation (SD) values for different sexes and age groups on the Chinese version of the CPRS were used to convert the actual scores (X) of each child across various dimensions into z-scores using the formula Z = (X − M)/SD. In this study, a z-score >2 was considered indicative of abnormal behavioral.32
Before data collection, informed consent was obtained from the families of all participating paediatric patients. The researcher provided a detailed oral explanation of the questionnaire completion process to the families. Families were instructed to scan a QR code on the paper form to access and complete the online questionnaire. For answers to any questions or clarifications, the families were encouraged to contact the researcher directly. Prior to finalizing the data collection process, the researcher thoroughly reviewed the data for completeness. In cases of uncertainty or ambiguity, the researcher contacted the families to verify the information provided.
Data Analysis
Data analysis utilized SPSS 24.0 and PROCESS 4.1.33 Categorical variables were presented as frequencies (%); continuous variables as M ± SD or median (P25–P75) based on distribution.
Mann–Whitney U-test assessed differences in CPRS dimensions. Spearman correlation analyzed relationships among variables. Multiple linear regression models examined the link between preterm birth and behavioral problems, stratified by PSQ scores. PROCESS Model 4 evaluated the mediation effect of PSQ score on prematurity-behavioral problems, controlling for age, sex, BMI z-score, mother’s age, and education. The association between preterm birth and behavioral problems in both the normal PSQ group and the abnormal PSQ group (two subgroups) was analyzed using multiple linear regression models. Bias-corrected bootstrap CI (5,000 samples) determined statistical significance for indirect effects. Partial mediation was indicated by significant direct and indirect effects; full mediation by significant indirect effect only. Missing values were excluded. The sensitivity analysis of the mediating effects was conducted using R version 4.0.5 software. Significance level was α = 0.05.
Results
Demographics and Clinical Characteristics
The mean age of primary school students was 7.86 years (SD = 1.388). The average age of their mothers was 37.54 years (SD = 3.73). The number of boys was 9,625, accounting for 53.1% (See Table 1). In our sample, the prematurity rate was 8% (1450/18,138). PSQ total scores and all six CPRS dimensions were non-normally distributed, so Mann–Whitney U-tests were used (Tables 2). When grouped by prematurity, all PSQ and CPRS dimension scores (conduct, learning, psychosomatic, impulsive-hyperactive, anxiety, hyperactivity) differed significantly (P < 0.05; see Table 2).
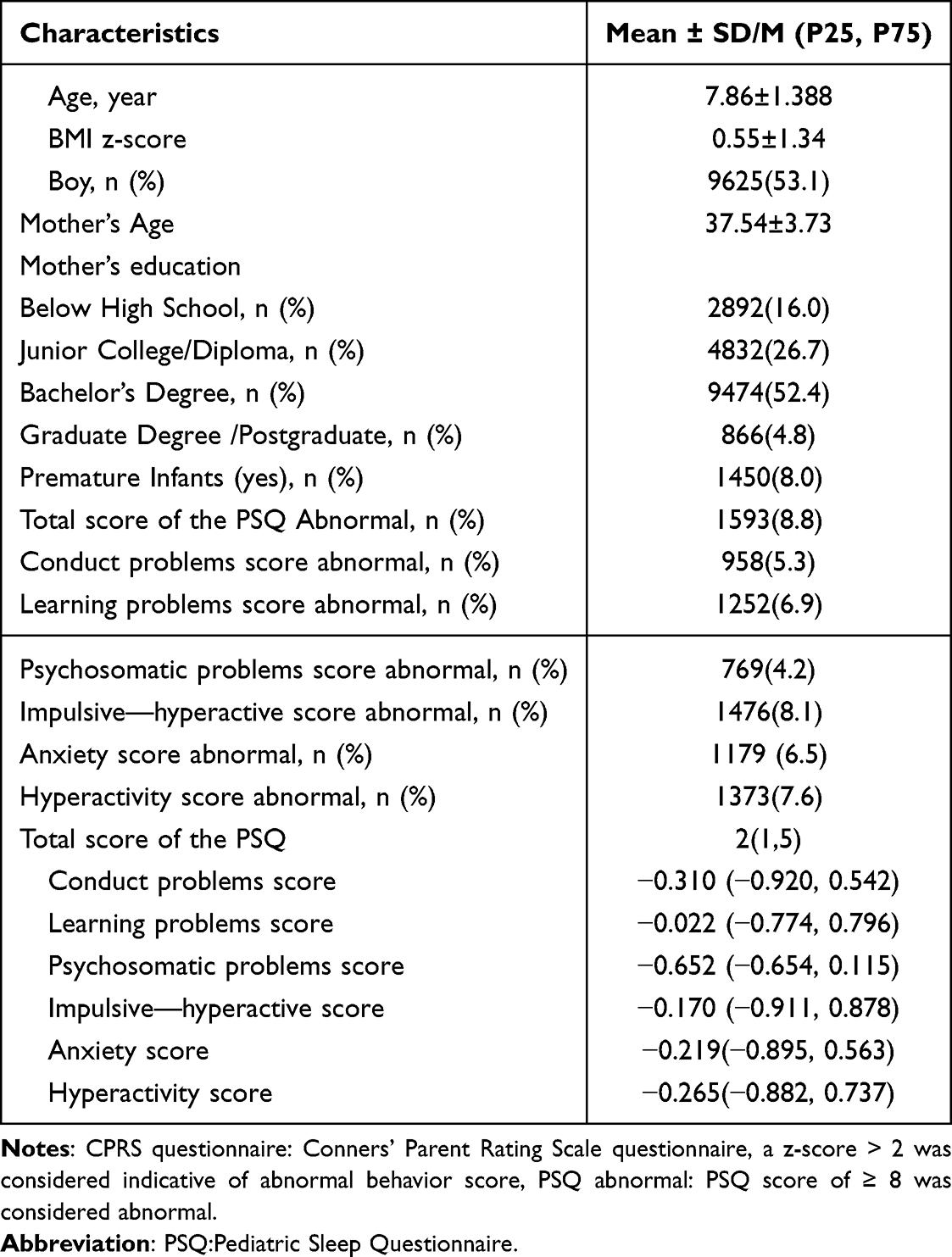 |
Table 1 Characteristics of Study Participants |
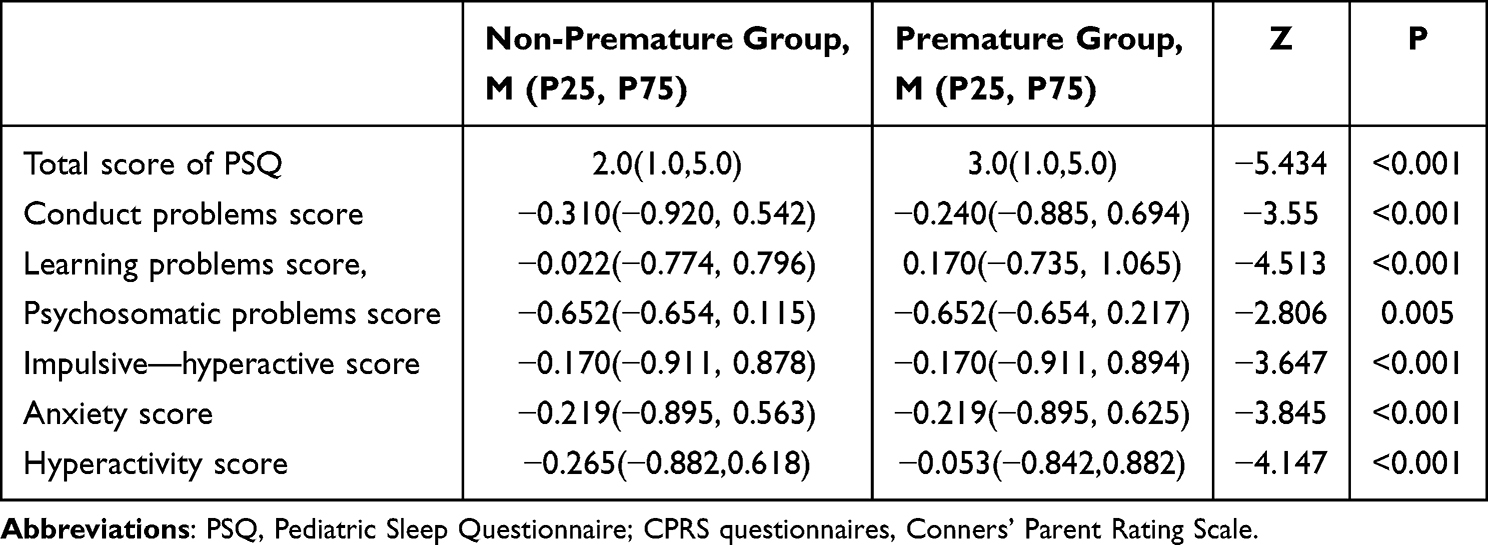 |
Table 2 Inter-Group Comparison Based on Dichotomous Variable Groupings of Prematurity Status, PSQ and the Six Dimensions of CPRS |
Bivariate Correlation Descriptive Analyses
Table 3 shows bivariate correlation results. Mother’s age was negatively linked to the total PSQ score and all six CPRS dimensions (all rho < 0, P < 0.05). The total PSQ score was positively associated with conduct, psychosomatic, impulsive-hyperactive, anxiety, and hyperactivity problem scores (all rho > 0, P < 0.01). The six CPRS dimensions are also positively correlated with each other (all rho > 0, P < 0.01).
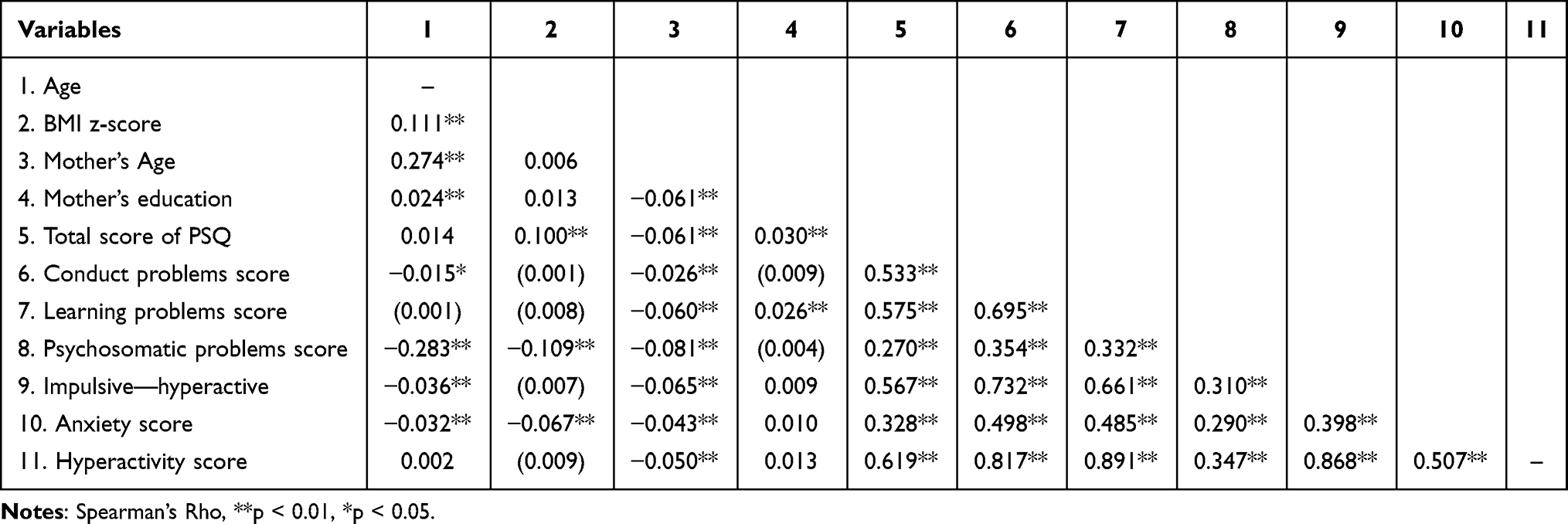 |
Table 3 Bivariate Correlation Coefficients of the Study Variables (N = 18,318) |
Mediation Models
Definitions of Direct, Indirect, and Total Effects
In the context of this study, the direct effect refers to the direct influence of the independent variable (prematurity) on the dependent variable (scores on the six dimensions of the CPRS questionnaire) without going through the mediator (the total PSQ score). The indirect effect represents the influence of prematurity on the CPRS scores that is transmitted via the total PSQ score. The total effect is the combined influence of prematurity on the CPRS scores, encompassing both the direct and indirect effects. When performing mediation analysis, the system automatically excludes missing values (Table 4).
 |
Table 4 Analysis of Preterm Birth’s Influence on PSQ Total Score and the Combined Effects on CPRS Dimensions |
The Relationship Between Prematurity, the Total PSQ Score, and Behavior Problems
After controlling for the effects of age, gender, BMI z-score, maternal age, and maternal education level, prematurity was found to be positively correlated with the total PSQ score (B = 0.411, P < 0.01). Furthermore, the total PSQ score had a significant direct impact on all six dimensions of the CPRS questionnaire (all P-values <0.05). See Table 4.
Direct Effects
Prematurity had no direct link to Conduct, Psychosomatic, Impulsive – hyperactive, or hyperactivity scores (all P > 0.05). But it was directly correlated with Learning problems (β = 0.063, p = 0.005) and Anxiety scores (β = 0.076, p = 0.003) (Table 5 and Figure 1).
 |
Table 5 Mediating Role of PSQ Total Score in the Scores of Six CPRS Dimensions Among Premature Infants |
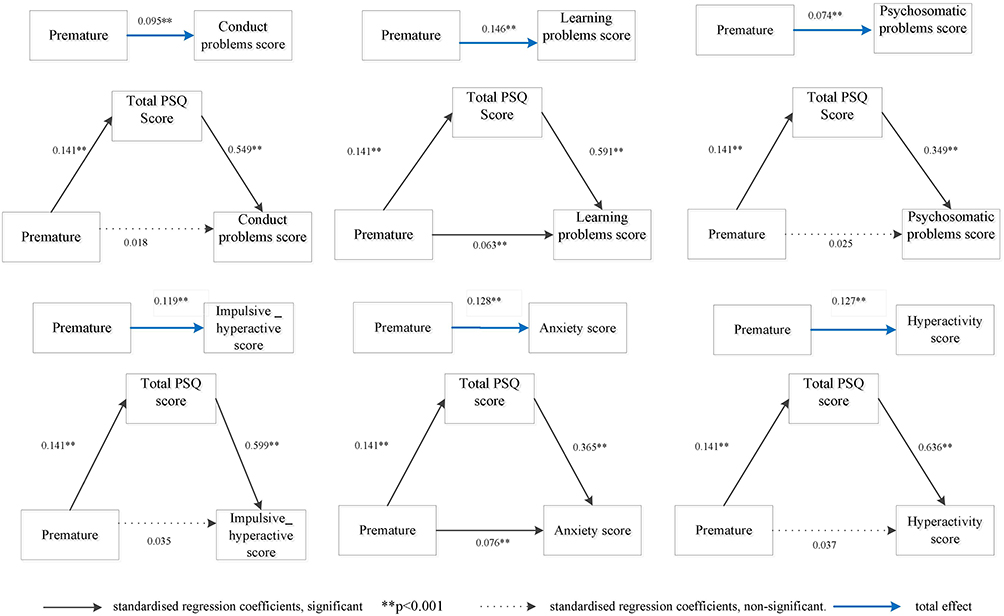 |
Figure 1 Mediating effect of total PSQ score on the association between the six dimensions of CPRS and premature infant development. |
Mediated Effects
The correlations between prematurity and the Z-scores of Conduct, Psychosomatic, Impulsive – Hyperactive, and Hyperactivity problems scores across six CPRS dimensions, mediated by total PSQ score, were significant (95% Bootstrap CI excluded 0) (Table 5 and Figure 1). Prematurity correlated with all six CPRS dimensions, with significant total effects (p < 0.001), and all mediated correlations via PSQ were significant.
Partial Mediation
In an exploratory analysis, there was a pattern suggesting that prematurity had a direct association with Learning problems (β = 0.063, p = 0.005) and Anxiety scores (β = 0.076, p = 0.003) in CPRS, and the total PSQ score seemed to play a partial role in the relationship pattern (Table 5 and Figure 1).
Full Mediation
In an exploratory analysis, no significant direct association was observed between prematurity and the following CPRS dimensions: Conduct problems: direct effect (β = 0.018, p = 0.438), Psychosomatic problems: direct effect (β = 0.025, p = 0.345), Impulsive-hyperactive problems: direct effect (β = 0.035, p = 0.121), Hyperactivity: direct effect (β = 0.037, p = 0.836). These findings suggest that the total PSQ score fully mediated the relationships between prematurity and these CPRS dimensions (Table 5 and Figure 1).
Overall Significance
The mediated correlation between prematurity and six CPRS dimensions by total PSQ score was significant (95% Bootstrap CI excluded 0) (Table 5 and Figure 1). Prematurity showed significant overall correlations with Z-scores of all six CPRS dimensions (all P < 0.05).
Sensitivity Analyses
Based on Table 6, the sensitivity analysis of mediating effects revealed that the mediating effect of the total PSQ score on the Z-scores of Conduct, Learning problems, Impulsive-hyperactive, and Hyperactivity problems scores in preterm infants had been quite robust (ρ critical value >0.4). The mediating effect of the total PSQ score on the Z-scores of Psychosomatic and Anxiety scores in preterm infants had been relatively robust (ρ critical value <0.4). It was advisable to incorporate additional confounding variables (such as family history) in future research focusing on these two variables.
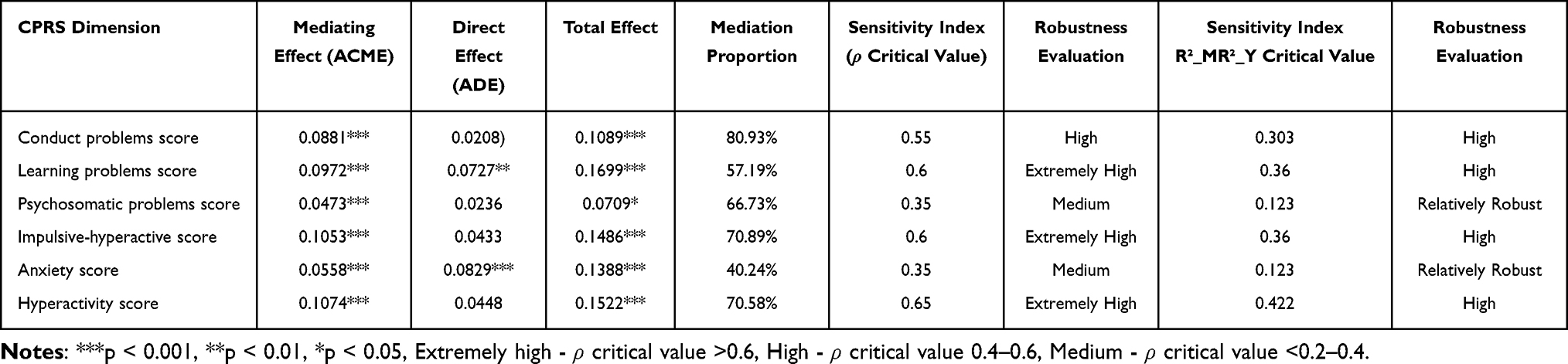 |
Table 6 Sensitivity Analysis Results of Mediating Effect of Preterm Birth & PSQ Total Score on CPRS 6 Dimensions |
Discussion
The results of this cross-sectional study reveal the relationship between premature birth, sleep-disordered breathing (total score of PSQ), and behavioral problems (CPRS questionnaire) in children. After controlling for confounding factors such as age, gender, BMI z-score, mother’s age, and mother’s education, our main research findings indicate that sleep-disordered breathing (total score of PSQ) in premature infants partially or fully mediates children’s behavioral problems. It is important to highlight that the mediation effect observed in this cross-sectional study merely suggests a statistical association and does not imply any causal relationships among the variables.
The mechanism of sleep is closely related to the sleep centre and the activity status of the cerebral cortex.34 Premature infants, due to insufficient neurophysiological development, may experience various sleep abnormalities, including a high incidence of SDB.35 Potential biological pathways may involve prematurity-related neurodevelopmental vulnerabilities and SDB-induced intermittent hypoxia/inflammation collectively impacting neural circuits and neurotransmitter systems regulating behavior. The indications of externalizing,17,18,36 and internalizing symptoms37-39 are manifested often through parental behavior ratings in SDB cases. Those studies suggest an association between sleep disorders in premature infants and various behavioral problems in children, indicating that sleep - disordered breathing may be related to the relationship between premature infants and childhood behavior in an exploratory sense.37–40 Those were consistent with our research hypothesis. Our study offered an in-depth analysis and explanation of the correlations, showing how SDB in premature infants had been associated with the emergence of internalizing and externalizing behavioral problems in children, suggesting its mediating role in this relationship.
Studies have shown that group cognitive-behavioral therapy can be successfully applied in urban schools to reduce the increasing risk for externalizing and internalizing disorders.41 The literature on the effectiveness of mental health interventions in low-income urban schools has mostly reported disappointing results,41 which suggests that interventions for children’s behavioral issues require schools with adequate resources and high-quality intervention measures. This highlights the need for health management departments to pay close attention to behavioral problems among children in remote areas and intervene promptly.
Regarding the relationship between SDB and behavioral problems in children, our results indicated that the total PSQ score correlated positively with the six dimensions of the CPRS questionnaire (Table 3). Previous studies had also reported findings consistent with ours, indicating that behavioral issues were more common in children with SDB among primary school students.42 Sleep quality played an important role in children’s academic performance and healthy development. Studies had shown that SDB was associated with poor academic performance, particularly in language, art, math, science, and learning problems.43 A recent high-quality meta-analysis had reported that children with SDB exhibited deficiencies in multiple cognitive domains, particularly in full-scale intelligence quotient as well as subdomains, such as problem-solving, working memory, processing speed, and language.44 This indicated that prioritizing screening for SDB and actively treating it could reduce undesirable behavioral in children. The aforementioned studies had indicated that prioritizing screening and treatment for SDB was extremely important. OSAS was a common clinical manifestation of SDB. Adenotonsillectomy was widely considered the primary treatment for OSAS in children.45 A systematic review had demonstrated enhanced quality of life following adenotonsillectomy, with no significant postoperative complications.46 Future cohort or intervention studies are necessary to figure out the causal relationships among prematurity, SDB, and how children behave. Specifically, longitudinal studies should track SDB development trajectories in premature infants using polysomnography, combined with neuroimaging biomarkers to explore neural mechanisms. Multi-center trials could also validate whether early adenotonsillectomy for SDB intervention alters behavioral outcomes in former preterm children.
Limitations
Assessment Bias: The evaluation of children’s SDB and behavioral issues relied on parent-completed questionnaires using parent-reported instruments, which may introduce subjective bias. The absence of objective diagnostic methods like polysomnography impeded the verification of clinical severity, potentially masking true associations. To reduce this bias, relevant explanations, materials were given to guardians before questionnaire completion, and contact information for consultation was provided. The robustness of findings was partly shown by consistent strong associations in subgroup analysis.
Sample Limitation: The sample was restricted to Xuhui District, Shanghai, limiting the generalizability of results. Future research should gather data from different cities or regions for a more diverse sample.
Causality Establishment Issue: As a cross - sectional study with data collected at a single time point, it is impossible to determine the temporal sequence of variables, making it hard to distinguish causes from effects. For instance, although an association between SDB and children’s behavioral problems was found, it is unclear whether SDB caused the problems, behavioral issues triggered sleep disturbances, or both were influenced by unmeasured factors such as the family environment.
Unmeasured Confounders: Potential unmeasured confounders like socioeconomic status, perinatal complications, or parental health conditions may affect the observed associations.
Despite these limitations, the study has a large sample size. There are relatively few studies on the mediation analysis of prematurity, SDB, and child behavior. The findings offer early warning knowledge for future research and inform clinical staff and parents of premature infants to pay attention to SDB and conduct screening.
Conclusion
This cross-sectional study reveals an association between prematurity and children’s behavioral problems, suggesting SDB may act as a partial or full mediator. However, the findings are limited by parental-reported data bias and the cross-sectional design’s inability to infer causality. Future cohort or intervention studies are needed to explore causal relationships among prematurity, SDB, and behavioral problems.
The Clinical Implications
While preliminary data hinted at possible links between sleep - disordered breathing (SDB) and behavioral problems in premature infants, these observations did not establish causality and required validation through longitudinal or interventional studies. Current practice may have included monitoring SDB symptoms and tracking behavioral outcomes over time, but any interventions for behavioral issues should not attribute causation to SDB alone without comprehensive multidisciplinary assessment. Future research needs to clarify whether these associations reflect direct pathways, shared vulnerabilities, or confounding factors to guide evidence - based care.
Data Sharing Statement
As per IRB application and permission, research data will not be made available in the public. However, the relevant data can be obtained from the corresponding authors upon qualified request and with the consent of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine.
Acknowledgments
Thanks to all participants for completing this large cross-sectional study.
Author Contributions
Yuli Hu: Writing – original draft, Writing – review & editing, Methodology, Formal analysis, Data curation, Validation, Visualization, Funding acquisition. Siqiong Jiang: Writing – review & editing, Methodology, Resources, Supervision. Shiyin Yang: Writing – review & editing, Investigation, Data curation. Chunsheng Wang: Software, Validation, Visualization, Formal analysis, Data curation, Writing – review and editing. Jianyin Zou: Methodology, Writing – review and editing, Jian Guan: Conceptualization, Writing – review & editing, Project administration and Supervision. Yupu Liu: Writing – review & editing, Project administration, Data curation and Supervision. Qunfeng Lu: Writing – review & editing, Methodology, Resources, Funding acquisition, Conceptualization and Supervision.
All authors have made substantial contributions to the research presented in this work, spanning key stages such as conceptual framing, research methodology formulation, practical implementation, data collection, in-depth analysis, and result interpretation, with some contributing across multiple or all of these domains. They have actively participated in the writing process, either by drafting initial versions, refining content through revisions, or providing critical feedback to enhance the article’s quality. Furthermore, all authors have collectively endorsed the final paper for publication, reached a consensus on the target journal for submission, and committed to taking full responsibility for the integrity and accuracy of every aspect of the research.
Funding
This study was funded by the Shanghai Jiao Tong University School of Medicine: Nursing Development Program (SJTUHLXK2022 and SJTUHLXK2024), Clinical Research Plan of SHDC (grant number SHDC2022CRS016B), 2024 Hospital-level Retrospective Clinical Research Project (ynhg202439), Nursing Department of Shanghai Sixth People’s Hospital (SSHebn2024-09) and SHLYHLXK-2025-03.
Disclosure
The authors declare no conflicts of interest.
References
1. Roggero P, Giannì ML, Garbarino F, et al. Consequences of prematurity on adult morbidities. Eur J Internal Med. 2013;24(7):624–626. doi:10.1016/j.ejim.2013.01.011
2. WHO. March of dimes, partnership for maternal, newborn & child health, save the children. born too soon: the global action report on preterm birth. Available from: http://www.who.int/maternal_child_adolescent/documents/born_too_soon/en/.
3. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. doi:10.1016/S0140-6736(12)60820-4
4. Thunqvist P, Tufvesson E, Bjermer L, et al. Lung function after extremely preterm birth-A population-based cohort study (EXPRESS). Pediatric Pulmonology. 2018;53(1):64–72. doi:10.1002/ppul.23919
5. Bocca-Tjeertes IF, Kerstjens JM, Reijneveld SA, et al. Growth and predictors of growth restraint in moderately preterm children aged 0 to 4 years. Pediatrics. 2011;128(5):e1187–e1194. doi:10.1542/peds.2010-3781
6. Caesar R, Colditz PB, Cioni G, Boyd RN. Clinical tools used in young infants born very preterm to predict motor and cognitive delay (not cerebral palsy): a systematic review. Dev Med Child Neurol. 2021;63(4):387–395. doi:10.1111/dmcn.14730
7. Stein RE, Siegel MJ, Bauman LJ. Are children of moderately low birth weight at increased risk for poor health? A new look at an old question. Pediatrics. 2006;118(1):217–223. doi:10.1542/peds.2005-2836
8. Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242–252. doi:10.1513/pats.200708-135MG
9. Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: association with race and prematurity. J Pediatr. 2003;142(4):383–389. doi:10.1067/mpd.2003.28
10. Guilleminault C, Akhtar F. Pediatric sleep-disordered breathing: new evidence on its development. Sleep Med Rev. 2015;24:46–56. doi:10.1016/j.smrv.2014.11.008
11. Pietropaoli N, Supino MC, Vitelli O, et al. Cognitive function in preschool children with sleep-disordered breathing. Sleep Breath. 2015;19(4):1431–1437. doi:10.1007/s11325-015-1157-3
12. Bjork S, Jain D, Marliere MH, Predescu SA, Mokhlesi B. Obstructive sleep apnea, obesity hypoventilation syndrome, and pulmonary hypertension: a state-of-the-art review. Sleep Med Clin. 2024;19(2):307–325. doi:10.1016/j.jsmc.2024.02.009
13. Li Y, Tong X, Wang S, et al. Pediatric sleep-disordered breathing in Shanghai: characteristics, independent risk factors and its association with malocclusion. BMC Oral Health. 2023;23(1):130. doi:10.1186/s12903-023-02810-9
14. Li HY, Lee LA. Sleep-disordered breathing in children. Chang Gung Med J. 2009;32(3):247–257.
15. Ting H, Wong RH, Yang HJ, et al. Sleep-disordered breathing, behavior, and academic performance in Taiwan schoolchildren. Sleep Breath. 2011;15(1):91–98. doi:10.1007/s11325-010-0329-4
16. Sedky K, Bennett DS, Carvalho KS. Attention deficit hyperactive disorder and sleep disordered breathing in pediatric populations: a meta-analysis. Sleep Med Rev. 2014;18(4):349–356. doi:10.1016/j.smrv.2013.12.003
17. Mulvaney SA, Goodwin J, Morgan WJ, et al. Behavior problems associated with sleep disordered breathing in school-aged children--the Tucson children’s assessment of sleep apnea study. J Pediatr Psychol. 2006;31(3):322–330. doi:10.1093/jpepsy/jsj035
18. Bourke RS, Anderson V, Yang JSC, et al. Neurobehavioral function is impaired in children with all severities of sleep disordered breathing. Sleep Med. 2011;12(3):222–229. doi:10.1016/j.sleep.2010.08.011
19. Csábi E, Gaál V, Hallgató E, et al. Increased behavioral problems in children with sleep-disordered breathing. Ital J Pediatr. 2022;48(1):173. doi:10.1186/s13052-022-01364-w
20. Wei X, Lü W. Childhood trauma and internalizing and externalizing behavior problems among adolescents: role of executive function and life events stress. J Adolesc. 2023;95(4):740–750. doi:10.1002/jad.12150
21. Bröring T, Oostrom KJ, van Dijk-Lokkart EM, et al. Attention deficit hyperactivity disorder and autism spectrum disorder symptoms in school-age children born very preterm. Res Dev Disabil. 2018;74:103–112. doi:10.1016/j.ridd.2018.01.001
22. Chiorean A, Savoy C, Beattie K, et al. Childhood and adolescent mental health of NICU graduates: an observational study. Arch Dis Child. 2020;105(7):684–689. doi:10.1136/archdischild-2019-318284
23. Winchester SB, Sullivan MC, Marks AK, et al. Academic, social, and behavioral outcomes at age 12 of infants born preterm. West J Nurs Res. 2009;31(7):853–871. doi:10.1177/0193945909339321
24. Kim ES, Kim EK, Kim SY, et al. Cognitive and behavioral outcomes of school-aged children born extremely preterm: a korean single-center study with long-term follow-up. J Korean Med Sci. 2021;36(39):e260. doi:10.3346/jkms.2021.36.e260
25. World Health Organization. Growth reference data for 5-19 years. Geneva, Switzerland: WHO; 2009. Available from: http://www.who.int/growthref/tools/en/.
26. Obstetrics Group. Obstetrics and gynecology branch of chinese medical association. guidelines for clinical diagnosis and treatment of preterm birth (2014). Chin J Perinat Med. 2015;18(4):241–245. 10.3760/cma.j.issn.0529-567x.2014.07.001.
27. Chervin RD, Hedger K, Dillon JE, et al. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21–32. doi:10.1016/s1389-9457(99)00009-x
28. Traeger N, Schultz B, Pollock AN, et al. Polysomnographic values in children 2-9 years old: additional data and review of the literature. Pediatr Pulmonol. 2005;40(1):22–30. doi:10.1002/ppul.20236
29. Li XD, Tai J, Xu ZF, et al. Analysis of polysomnography in children with obstructive sleep apnea hypopnea syndrome. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016;51(11):812–818. doi:10.3760/cma.j.issn.1673-0860.2016.11.003
30. Incerti Parenti S, Fiordelli A, Bartolucci ML, et al. Diagnostic accuracy of screening questionnaires for obstructive sleep apnea in children: a systematic review and meta-analysis. Sleep Med Rev. 2021;57:101464. doi:10.1016/j.smrv.2021.101464
31. Huiqin T, Ren’e X. Xu Taoyuan. Applied research on the Conners Parent Symptom Questionnaire (revised version). Shanghai Arch Psychiatry. 1993;04:246–248.
32. Fan J, Da Y, Li W. The norm and reliability of the Conners parent symptom questionnaire in Chinese urban children. Shanghai Arch Psychiatry. 2005;17(6):321–323. doi:10.3969/j.issn.1002-0829.2005.06.001 Chinese.
33. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
34. Carskadon MA, Acebo C, Jenni OG. Regulation of adolescent sleep: implications for behavior. Ann N Y Acad Sci. 2004;1021(1):276–291. doi:10.1196/annals.1308.032
35. Stangenes KM, Fevang SK, Grundt J, et al. Children born extremely preterm had different sleeping habits at 11 years of age and more childhood sleep problems than term-born children. Acta Paediatr. 2017;106(12):1966–1972. doi:10.1111/apa.13991
36. Beebe DW, Ris MD, Kramer ME, et al. The association between sleep disordered breathing, academic grades, and cognitive and behavioral functioning among overweight subjects during middle to late childhood. Sleep. 2010;33(11):1447–1456. doi:10.1093/sleep/33.11.1447
37. Rosen CL, Storfer-Isser A, Taylor HG, et al. Increased behavioral morbidity in school-aged children with sleep-disordered breathing. Pediatrics. 2004;114(6):1640–1648. doi:10.1542/peds.2004-0103
38. Giordani B, Hodges EK, Guire KE, et al. Changes in neuropsychological and behavioral functioning in children with and without obstructive sleep apnea following tonsillectomy. J Int Neuropsychol Soc. 2012;18(2):212–222. doi:10.1017/S1355617711001743
39. Montoya-Castilla I, Postigo S, Prado-Gascó V, et al. Relationships between affective states and childhood internalizing disorders. Arch Psychiatr Nurs. 2018;32(4):591–598. doi:10.1016/j.apnu.2018.03.013
40. Johnson S, Marlow N. Preterm birth and childhood psychiatric disorders. Pediatr Res. 2011;69(5):0b013e318212faa0. doi:10.1203/PDR.
41. Eiraldi R, Power TJ, Schwartz BS, et al. Examining effectiveness of group cognitive-behavioral therapy for externalizing and internalizing disorders in urban schools. Behav Modif. 2016;40(4):611–639. doi:10.1177/0145445516631093
42. Sakamoto N, Gozal D, Smith DL, et al. Sleep duration, snoring prevalence, obesity, and behavioral problems in a large cohort of primary school students in Japan. Sleep. 2017;40(3):zsw082. doi:10.1093/sleep/zsw082
43. Galland B, Spruyt K, Dawes P, et al. Sleep disordered breathing and academic performance: a meta-analysis. Pediatrics. 2015;136(4):e934–e946. doi:10.1542/peds.2015-1677
44. Menzies B, Teng A, Burns M, et al. Neurocognitive outcomes of children with sleep disordered breathing: a systematic review with meta-analysis. Sleep Med Rev. 2022;63:101629. doi:10.1016/j.smrv.2022.101629
45. Connolly HV, Tomaselli LT, McKenna Benoit MK, et al. Adenotonsillectomy for pediatric obstructive sleep apnea: how to predict those at risk for postoperative complications. J Clin Sleep Med. 2020;16(1):3–4. doi:10.5664/jcsm.8150
46. Todd CA, Bareiss AK, McCoul ED, et al. Adenotonsillectomy for obstructive sleep apnea and quality of life: systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2017;157(5):767–773. doi:10.1177/0194599817717480
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.