Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Six months methylphenidate treatment improves emotion dysregulation in adolescents with attention deficit/hyperactivity disorder: a prospective study
Authors Suzer Gamli I ![]() , Tahiroglu AY
, Tahiroglu AY
Received 13 February 2018
Accepted for publication 6 April 2018
Published 22 May 2018 Volume 2018:14 Pages 1329—1337
DOI https://doi.org/10.2147/NDT.S164807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Ipek Suzer Gamli,1 Aysegul Yolga Tahiroglu2
1Sanliurfa Education and Research Hospital, Eyyubiye, Sanliurfa, Turkey; 2Child and Adolescent Psychiatry Department, Cukurova University School of Medicine, Saricam, Adana, Turkey
Purpose: Individuals with attention deficit/hyperactivity disorder (ADHD) may suffer from emotional dysregulation (ED), although this symptom is not listed among the diagnostic criteria. Methylphenidate (MPH) is useful in reducing emotional symptoms in ADHD. The aim of the present study was to determine both psychosocial risk factors and presence of ED in adolescents with ADHD before and after MPH treatment.
Participants and methods: Eighty-two patients aged 12–18 years with ADHD were included as participants. The Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime, the Difficulties in Emotion Regulation Scale (DERS), sociodemographic form, and the Inventory of Statements About Self-Injury were administered. Results were compared before and after 6 months MPH treatment.
Results: A significant improvement was detected on DERS for impulsivity (15.9±6.8 initial vs 14.2±6.5 final test, p<0.01) and total score (88.4±23.3 initial vs 82.4±2.7 final test, p<0.05) across all patients taking MPH regardless of subtype and sex. Despite treatment, a significant difference remained for impulsivity, strategies, and total score in patients with comorbid oppositional defiant disorder (ODD) compared with those without ODD, but no difference was detected for conduct disorder comorbidity. In patients who self-harm, scores for goals, impulsivity, strategies, clarity, and total score were higher before treatment: furthermore, impulsivity and total score remained high after treatment. In maltreated patients, goals, impulsivity, strategies, and total scores were significantly higher before treatment; however, their symptoms were ameliorated after treatment with MPH.
Conclusion: Individuals with severe ED may “self-medicate” by smoking and/or self-harming. MPH led to significant improvements in ED possibly owing, in part, to a decrease in impulsivity, so that individuals felt more able to supervise their emotions and engage in goal-directed behaviors. ED should be considered particularly in patients with additional psychosocial factors and ODD comorbidity, and included in the treatment plan.
Keywords: attention deficit, emotion, dysregulation, methylphenidate
Introduction
Attention deficit/hyperactivity disorder (ADHD) is characterized by inattention, hyperactivity, and/or impulsivity inappropriate for the individual’s age and the developmental stage. It is among the most common neuropsychiatric disorders worldwide.1,2
Untreated ADHD increases the risk of other psychiatric conditions and adverse life experiences such as smoking, substance misuse, suicidality, and/or non-suicidal self-injury (NSSI).3–7 ADHD has a significant adverse effect on an individual’s psychosocial functioning and quality of life, leading to more emotional and behavioral problems, lower self-esteem, and poorer outcomes in many domains.8
Executive function (EF) deficits play a major part in ADHD, affecting cognitive processes such as planning, problem-solving, and working memory.9 Problems with emotion regulation (ER) and/or modulating emotions also occur in individuals with EF deficits.10 ER is defined as the internal and external processes of observation, evaluation, and regulation of emotional reactions during goal-directed behaviors.11–13
Impairment in ER is referred to as emotional dysregulation (ED), and is gradually gaining recognition as a core deficit in patients with ADHD.14 Emotional inhibition, understanding of emotions, and empathy have been found to be lessened in individuals with ADHD.15,16 These individuals may have difficulties in understanding social clues and regulating affect appropriately and may have frequent emotional swings, with an adverse effect on their social functioning.15,17–19 A recent meta-analysis showed that individuals with ADHD mostly had emotional reactivity, negativity, and lability.20
Individuals with ADHD may also have difficulties in expressing appropriate emotional behaviors and may display negative emotionality.10 Regulating irritable and aggressive behaviors and/or emotions, in particular, are much more problematic in patients with ADHD.14,17,21 Moreover, individuals with persistent ADHD symptoms have higher rates of emotional lability, which is associated with poorer outcomes in many domains, adding support to the concept of emotional lability as another distinct dimension in ADHD.22
As ED is not specific to ADHD, it may be related to or may serve as a suitable marker for comorbid conditions that frequently present with ADHD. One study found that a deficit in ER was related to depressive symptoms later in life in patients with childhood ADHD.23 In addition, high rates of comorbid oppositional defiant disorder (ODD) may help to explain emotional symptoms in children with ADHD.24 It has been suggested that ODD should be assessed as a disorder of ER rather than a disruptive behavior disorder.25 Patients with non-episodic irritability and persistent negative mood may be diagnosed with disruptive mood dysregulation disorder (DMDD), which is a new diagnosis introduced in DSM-5.26 ED and recurrent temper outbursts are frequent in these individuals.27 Nearly 75% of patients with DMDD have comorbid ADHD.28 Borderline personality disorder is another psychopathology with intense ED, and symptoms may overlap with ADHD.29 Therefore, it should be kept in mind that ED may be linked to or raise the risk of comorbid conditions in ADHD.
Adults with ADHD exhibit similar deficits to children with the disorder. Items related to ED are well-defined in the Wender Utah Rating Scale for ADHD.30 Moreover, treatment with methylphenidate (MPH) has shown to be effective for core symptoms and additional emotional symptoms in adult patients with ADHD.31
In a minority of children with ADHD, stimulants may be associated with behavioral changes as side effects.32 In some patients, symptoms such as irritability, agitation, anxiety, and emotional lability may emerge with MPH usage.33 Stimulants led to irritability in 10% of children in one study, whereas the rate was 0% in the placebo group; this may cause confusion in clinical presentation.34 Moreover, clinicians should be aware of “rebound irritability”, which usually occurs alongside declining blood levels of MPH.35 However, based on the evidence, the association between MPH and changes in behavior is unclear. Further studies are needed to elucidate this association.33
Atomoxetine (ATX), another agent approved for treating ADHD, has been found to be useful, with moderate effect size, for reducing emotional lability in adults with ADHD.36 Moreover, ATX has a similar effect on ED as on other ADHD symptoms in adults.37 However, data on ED and the effects of ATX in children and adolescents with ADHD are insufficient, and further studies are required.
Other therapeutic approaches, such as psychosocial interventions, can also be used in the treatment of ED. In a study, cognitive behavioral therapy-based group therapy and parent training interventions were shown to be useful in reducing mood lability in children with ADHD and DMDD.38 Dialectical behavioral therapy is another therapeutic intervention that has been shown to be effective for ER in college students and adults with ADHD.39,40 In addition, mindfulness-based training was found to significantly reduce self-reported ED in adults with ADHD.41 Although data regarding children and adolescents are limited, these interventions appear to be useful in reducing emotional symptoms in patients with ADHD. Therefore, they may be evaluated as an adjunct treatment model for ADHD.42
The aim of this study was to determine the sociodemographic and clinical features and psychosocial risk factors of patients with untreated ADHD, thereby reflecting the early and problematic course of the disorder. An additional aim was to investigate difficulties with ER − especially in patients with additional adverse psychosocial risk factors − and measure the difference after MPH treatment for 6 months. Emotional lability and/or dysregulation in ADHD have been well-studied, generally using parental reports. To the best of our knowledge, there have been no follow-up studies regarding the effect of MPH on ED in adolescents with ADHD using a self-report scale, although this has been well-studied in adult patients.31,43
Participants and methods
Participants
Ethical approval for the study was provided by Cukurova University School of Medicine Non-Invasive Clinical Research Ethics Committee (8 May, 2015; reference number: 42/11). Written and informed consent was obtained from the parents and the participants who participated voluntarily in the study.
Eighty-two patients who presented to Cukurova University School of Medicine Child and Adolescent Psychiatry Department were included in the study. Patients were included if they: 1) were aged between 12 and 18 years, 2) were diagnosed as having ADHD based on the Turkish Version of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime (K-SADS-PL), 3) were treatment naïve, and 4) had no organic pathology. Mental Retardation and Autism Spectrum Disorders were used as exclusion criteria.
Routine tests including measurement of biochemical parameters and electrocardiogram were performed before starting the treatment. Participants were examined at baseline, and 1, 3, and 6 months of treatment. After the participants were examined, MPH treatment was started according to guidelines. The scales and tests described in the following section were administered both before starting the treatment and at the 6-month examination.
Measures
Initially, sociodemographic information was obtained including the participant’s age, birth history, developmental stages, medical history, academic history, peer relationships, familial characteristics, and any adverse events. The form was completed by the physician, using responses from the parents. Participants were interviewed by a child and adolescent psychiatrist using the K-SADS-PL, and psychiatric diagnoses were made in accordance with the text of the DSM-IV-TR.
K-SADS-PL
K-SADS-PL is a semi-structured interview technique performed by physicians, which detects former and existing Axis I psychopathologies according to the criteria of the DSM-III and DSM-IV-TR. First, questions are asked about fundamental symptoms, and the answers are scored between 0 and 3 based on severity and/or frequency. Psychopathologies associated with higher scoring symptoms are reassessed, evaluated, and diagnosed. K-SADS-PL has been shown to be a reliable and valid method for diagnosing psychopathologies in children and adolescents.44 The validity and reliability of the Turkish version were established by Gökler et al.45
Difficulties in Emotion Regulation Scale (DERS)
DERS is a brief, self-report questionnaire designed to assess ED, developed by Gratz and Roemer in 2004.46 It consists of 36 items, scored on a scale ranging from 1 (almost never) to 5 (almost always); higher scores reflect greater problems with ER. DERS has six subscales and a total score. Although DERS was composed for adults, research has shown that it is also an appropriate tool for measuring ED in adolescents.47 The validity and reliability of the Turkish version were established by Saritaş et al.48
Inventory of Statements About Self-Injury (ISAS)
ISAS is a self-report scale developed by Klonsky and Glenn in 2009. It consists of two parts: the frequency and accompanying features of NSSI behaviors are noted in the first part, and the function of self-harm is considered in the second.49 Only the first part was completed by the participants in the current study. The validity and reliability of the Turkish version were tested by Bildik et al.50
Statistical analysis
The Statistical Package for the Social Sciences (SPSS), version 16.00, was used for statistical analyses (SPSS Inc.; Chicago, IL, USA). Categorical variables were analyzed using the chi-square test. As DERS is composed of ordinal data, nonparametric tests were used: the Mann–Whitney U-test for independent variables, and the Wilcoxon signed-rank test for dependent variables. In all analyses, 0.05 was accepted as the level of statistical significance.
Results
The study comprised 82 patients, including 39 (47.6%) girls and 43 (52.4%) boys. The mean age of the participants was 14.9±1.9 years. No significant differences were observed between girls and boys in terms of sociodemographic features such as parental education, occupational status, family structure, history of domestic violence, academic performance, and peer relationships.
All patients were treated with MPH. Psychometric measures were used both before and after treatment. A comparison of DERS scores for all patients before and after 6 months of treatment is given in Table 1.
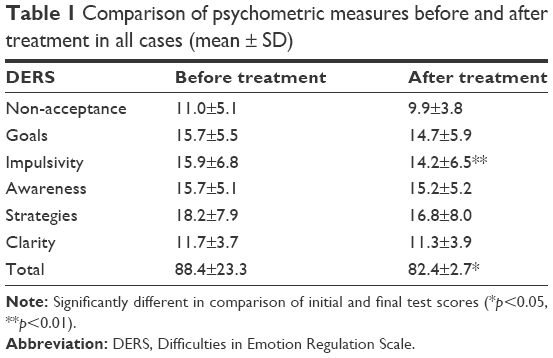 | Table 1 Comparison of psychometric measures before and after treatment in all cases (mean ± SD) |
Sixty-seven patients (81.7%) were diagnosed as having ADHD-combined subtype (ADHD-C), while 15 (18.3%) had the ADHD-inattention subtype (ADHD-I). The psychometric comparison of DERS among subtypes is shown in Table 2. There were no significant differences in initial and final test scores between patients with ADHD-C and those with ADHD-I subtypes.
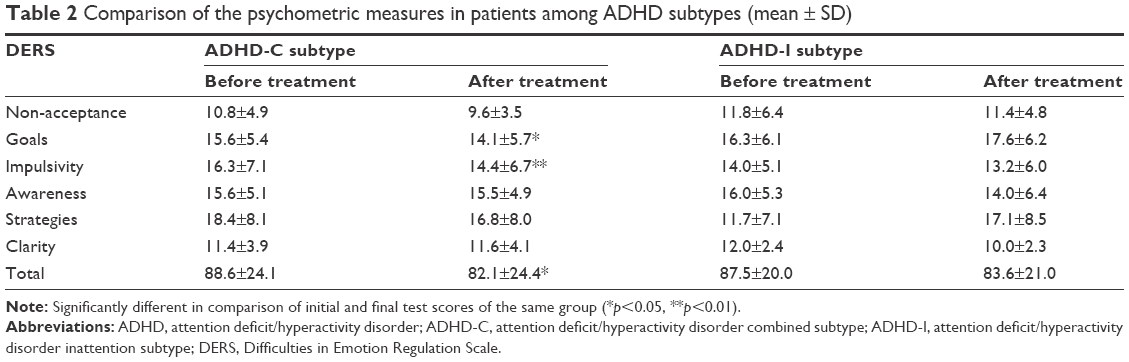 | Table 2 Comparison of the psychometric measures in patients among ADHD subtypes (mean ± SD) |
Sixteen patients (19.5%) were diagnosed as having comorbid ODD, and 12 (14.6%) had conduct disorder (CD). For patients with comorbid CD, initial total test scores were significantly higher than those of patients without comorbid CD (p<0.05). For patients with comorbid CD, there was no significant difference between the initial and final test scores. However, there was a significant decrease in scores in patients without comorbid CD (p<0.01). Psychometric measures (DERS scores) of patients with ODD are presented in Table 3.
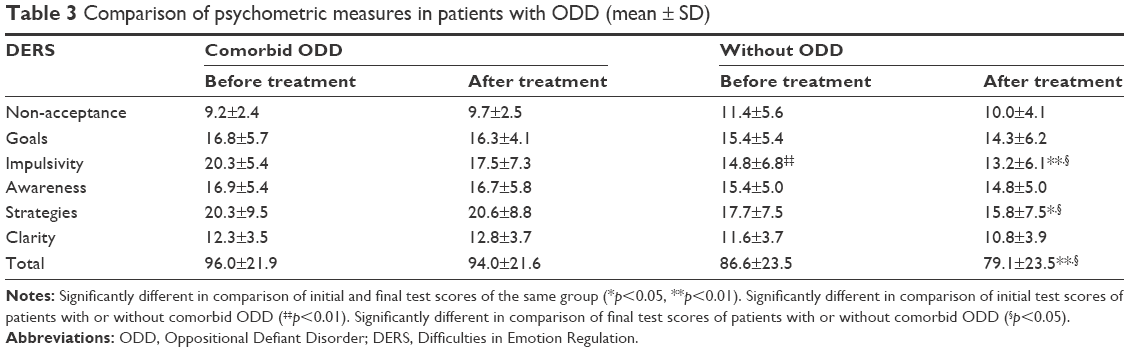 | Table 3 Comparison of psychometric measures in patients with ODD (mean ± SD) |
Twenty-three participants (28%) reported that they smoked regularly. Alcohol (n=9, 39.1%) and/or substance use (n=4, 100%) were significantly higher in smokers than in non-smokers (p<0.05). All smokers were diagnosed as having ADHD-C, and 16 of them (69.6%) had symptom onset before the age of 7 years. A comparison of psychometric properties in smokers and non-smokers is presented in Table 4.
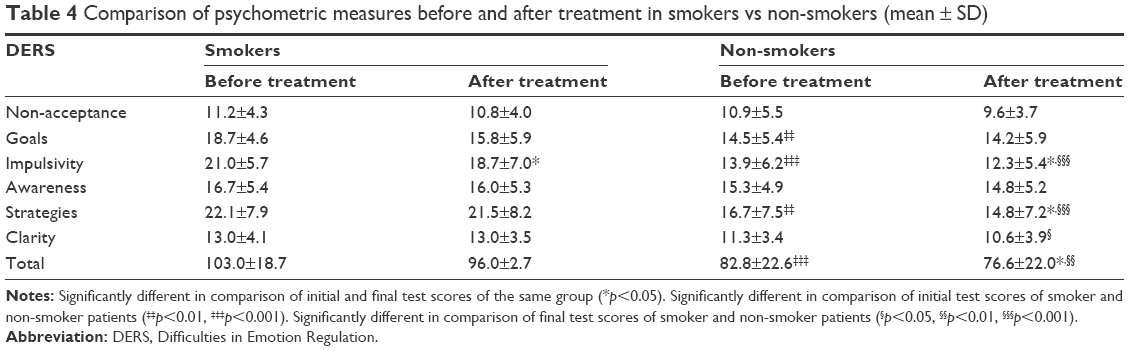 | Table 4 Comparison of psychometric measures before and after treatment in smokers vs non-smokers (mean ± SD) |
Forty-eight (58.5%) patients reported at least one NSSI on ISAS, 30 (62.5%) of whom were females. The average initial NSSI age was 11.4±3.4 years with wound picking, scraping letters/shapes in the skin, and tearing hair out being the most common behaviors. Twenty-one (53.8%) were alone when self-harming, and four (8.3%) were under the effect of drugs. Twenty-six (60.5%) committed NSSI after a stressful event, and 25 (83.3%) harmed themselves within an hour of the impulse. Eight (16.3%) reported that there was somebody with NSSI within their immediate family or among their close friends. The two ADHD subtypes did not differ with respect to presence of NSSI, except that pinpricking was more frequent in ADHD-C (p<0.05). DERS measures of patients with and without NSSI are given in Table 5.
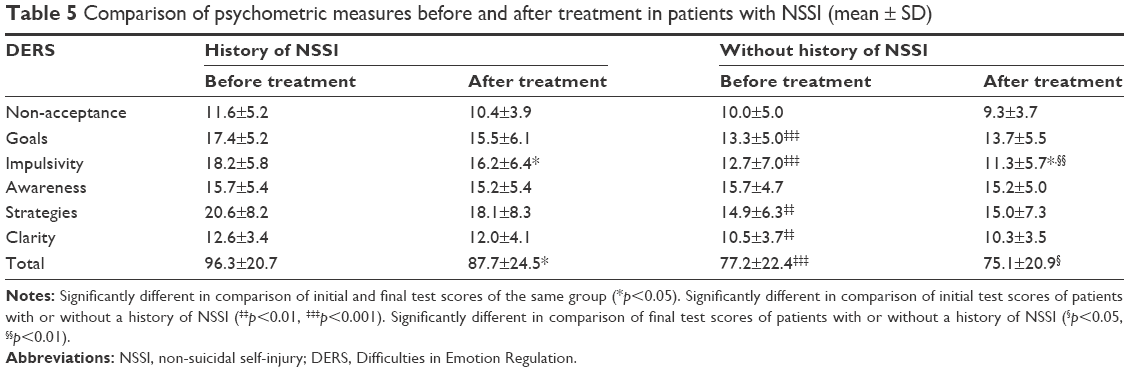 | Table 5 Comparison of psychometric measures before and after treatment in patients with NSSI (mean ± SD) |
Twenty-three (28%) participants had a history of maltreatment. Among children with maltreatment exposure, ADHD-C subtype diagnoses were significantly more common than ADHD-I subtype diagnoses (p<0.05). Comorbidities were not found to be associated with maltreatment (p>0.05). A comparison of psychometric properties in participants reporting maltreatment is shown in Table 6.
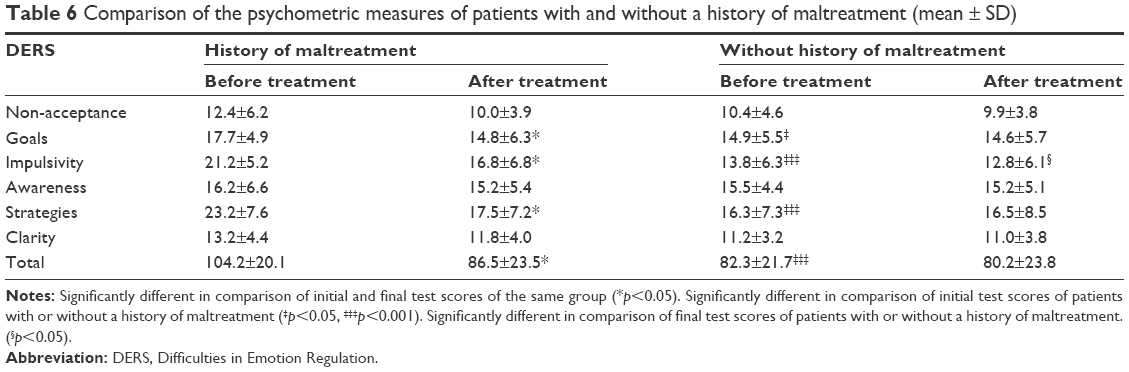 | Table 6 Comparison of the psychometric measures of patients with and without a history of maltreatment (mean ± SD) |
Discussion
ADHD may result in adverse consequences in many domains if undiagnosed or untreated.3,4,51 In this study, the participants were selected from patients who were treatment naïve and aged older than 12 years, in order to describe the sociodemographic and clinical features of untreated ADHD. We also aimed to investigate the difficulties in ER that these patients experienced and reveal changes with MPH treatment using a self-report scale for adolescents.
Consistent with the literature, we found that MPH had a significant effect on ED, particularly in impulsivity and total scores. Symptoms such as poor inhibitory control, inattention, mood regulation, and working memory are thought to be associated with impaired prefrontal cortical “top-down” mechanisms.52 The prefrontal cortex and striatal regions can be targeted by stimulants that increase central dopamine and norepinephrine levels.53,54 Research has shown that medications that optimize catecholamine levels in these regions have positive effects on attention, behavior, and ER.52 In clinical presentation, this improvement may be partly connected to a decrease in impulsivity, so that individuals feel more successful in supervising their emotions and goal-directed behaviors, and are able to act in a more controlled way in general. Additionally, individuals with ADHD may experience improvements in terms of understanding, acceptance, monitoring negative emotions, planning adequate strategies, exhibiting appropriate behaviors, and controlling impulsivity as a result of the treatment process.
In our study, no significant associations were found between DERS scores and ADHD subtype. ED has been previously reported to be associated with ADHD, regardless of subtype, and hyperactive and/or impulsive behaviors decrease in individuals with ADHD during adolescence. Therefore, it has been postulated that clinical presentation of ED may be less similar to other domains in adolescents with both subtypes.55
A significant association was determined only in impulsivity score before treatment, although there were associations of clarity, strategies, impulsivity, and total DERS scores with comorbid ODD during treatment. In the literature, it has been shown that ED and ODD are closely related, with ED having an impact on both social impairment and comorbid ODD.56,57 The difference that we detected in individuals with and without ODD comorbidity both before and after treatment, may support an association between ED and ODD and point to treatment resistance or permanence. Additional interventions may be helpful for these patients. On the other hand, no significant association was found between CD and ED.
Among our participants, the rate of smoking was 28%, consistent with the fact that individuals with ADHD are at heightened risk for smoking.58 In addition, it is widely accepted that both inattention and hyperactivity/impulsivity raise the risk of an individual trying tobacco and switching to regular smoking.59,60 DERS scores were significantly higher in smokers compared with non-smokers, consistent with the finding that adolescents with more severe ED may use smoking for mood regulation or stabilization.61–63 Smoking may serve as a way of coping with difficulties and/or be a means of self-medication. It has been reported in the literature that approximately one third of patients with ADHD use cigarettes as self-medication.63 During treatment, ED tended to decrease in smokers, although a statistical difference remained.
Notably, more than half of the participants (58.5%) in our study reported NSSI at least once. In the literature, ADHD is accepted as a risk factor for NSSI, suicidal thoughts, and suicide attempts.6,7,64 Hyperactivity symptoms in childhood are associated with self-damaging behaviors such as self-cutting and self-hitting in adolescence, and a higher number of ADHD symptoms is closely associated with earlier onset of self-harm and suicide attempts.65,66 The average age of the first NSSI was reported as 11 years in our study. Given that we accepted patients aged over 12 years, this may support the idea that NSSI may be one of the adverse consequences of untreated ADHD. In our study, NSSI was detected more frequently in girls than in boys, which is in accordance with the literature.67,68
We did not find any significant association between NSSI and ADHD subtype. It has been previously reported that NSSI tends to occur in the ADHD-C subtype rather than ADHD-I, as NSSI is an impulsive behavior involving an urgent drive accompanied by poor inhibitory control.69 The majority of our patients who self-harmed (83.3%) did so immediately after experiencing the impulse to do so which supports the impulsive dimension. However, it has also been shown that having ADHD increases the risk of NSSI regardless of subtype, with ADHD-C having a greater risk compared with ADHD-I.70 Individuals with ADHD may perform NSSI owing to making frequent mistakes or, feeling unsuccessful and/or inefficient, hence NSSI can be a kind of help-seeking behavior. These findings support the idea that NSSI should be considered as both an impulsive behavior and a cognitive process.7,68
In patients with NSSI, goals, impulsivity, strategies, clarity, and total scores in DERS were significantly higher compared with patients without NSSI. Adolescents who lack emotional clarity and ER strategies in general are prone to NSSI.71 It has been suggested that individuals with NSSI have difficulties in understanding, regulating, and expressing their emotions. This may cause them to respond in an exaggerated or sentimental fashion and have problems in tolerating negative emotions, potentially resulting in NSSI as a way of coping or as self-punishment.49,72 These findings are compatible with our study; participants with NSSI had difficulties in coping with daily events or negative experiences. Problematic ER can be considered to be a predictive factor in addition to ADHD for future NSSI.73 On the other hand, the DERS impulsivity scores of individuals with and without NSSI did not differ during treatment. This supports the idea that treatment with MPH has a positive effect on coping with negative emotions and impulse control.
In our study, patients with a history of maltreatment were more severely affected by ER, particularly before treatment. Neglect and/or abuse may be associated with difficulties in recognizing, understanding, and expressing one’s emotional state; such difficulties could be included in the ED concept.74,75 Therefore, children who are exposed to inappropriate emotional interactions may suffer from problematic interpersonal relationships and social functioning. Individuals who are exposed to trauma have been shown to be at risk of further psychiatric disorders such as affective and personality disorders.76 Consequently, maltreatment appears to be an independent risk factor for ED and should be asked about. On the other hand, the difference before treatment largely diminished after MPH use in maltreated participants. This may be compatible with the fact that maltreatment exposure is an independent risk factor for ADHD, with a negative impact on the severity of symptoms.77 However, as demonstrated by our study, this difference may disappear during the treatment process.
Conclusion
In conclusion, as has been reported in follow-up studies, ADHD in childhood is associated with poor psychosocial functioning and additional psychiatric comorbidities. ED is among the main features of ADHD regardless of subtype and has a negative impact on individuals’ daily functioning, although it is not specific to ADHD. ED frequently occurs in patients with additional risk factors such as comorbid psychiatric conditions (ODD in particular), smoking, and a history of NSSI. Therefore, every individual with ADHD should be asked about ED and related problems such as irritability, temper outbursts, and mood swings. MPH is useful in reducing emotional symptoms in ADHD. The association between ED and ADHD determined here can be used to inform future studies with larger sample sizes.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th ed. Washington: American Psychiatric Association; 2013. | ||
Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–e1001. | ||
Rasmussen P, Gillberg C. Natural outcome of ADHD with developmental coordination disorder at age 22 years: a controlled, longitudinal, community-based study. J Am Acad Child Adolesc Psychiatry. 2000;39(11):1424–1431. | ||
Klein RG, Mannuzza S, Olazagasti MA, et al. Clinical and functional outcome of childhood attention-deficit/hyperactivity disorder 33 years later. Arch Gen Psychiatry. 2012;69(12):1295–1303. | ||
Modesto-Lowe V, Danforth JS, Neering C, Easton C. Can we prevent smoking in children with ADHD: a review of the literature. Conn Med. 2010;74(4):229–236. | ||
Allely CS. The association of ADHD symptoms to self-harm behaviours: a systematic PRISMA review. BMC Psychiatry. 2014;14:133. | ||
Hurtig T, Taanila A, Moilanen I, Nordström T, Ebeling H. Suicidal and self-harm behaviour associated with adolescent attention deficit hyperactivity disorder-a study in the Northern Finland Birth Cohort 1986. Nord J Psychiatry. 2012;66(5):320–328. | ||
Klassen AF, Miller A, Fine S. Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics. 2004;114(5):e541–e547. | ||
Chan RC, Shum D, Toulopoulou T, Chen EY. Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. 2008;23(2):201–216. | ||
Brown TE. Attention Deficit Disorder: The Unfocused Mind in Children and Adults. Yale University Press Health & Wellness; 2006. | ||
Shaw P, Stringaris A, Nigg J, Leibenluft E. Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry. 2014;171(3):276–293. | ||
Thompson RA. Emotion regulation: a theme in search of definition. Monogr Soc Res Child Dev. 1994;59(2–3):25–52. | ||
Zeman J, Cassano M, Perry-Parrish C, Stegall S. Emotion regulation in children and adolescents. J Dev Behav Pediatr. 2006;27(2):155–168. | ||
van Stralen J. Emotional dysregulation in children with attention-deficit/hyperactivity disorder. Atten Defic Hyperact Disord. 2016;8(4):175–187. | ||
Sjöwall D, Roth L, Lindqvist S, Thorell LB. Multiple deficits in ADHD: executive dysfunction, delay aversion, reaction time variability, and emotional deficits. J Child Psychol Psychiatry. 2013;54(6):619–627. | ||
Musser ED, Backs RW, Schmitt CF, et al. Emotion regulation via the autonomic nervous system in children with attention-deficit/hyperactivity disorder (ADHD). J Abnorm Child Psychol. 2011;39(6):841–852. | ||
Barkley RA. Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull. 1997;121(1):65–94. | ||
Walcott CM, Landau S. The relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol. 2004;33(4):772–782. | ||
Anastopoulos AD, Smith TF, Garrett ME, et al. Self-regulation of emotion, functional impairment, and comorbidity among children with AD/HD. J Atten Disord. 2011;15(7):583–592. | ||
Graziano PA, Garcia A. Attention-deficit hyperactivity disorder and children’s emotion dysregulation: a meta-analysis. Clin Psychol Rev. 2016;46:106–123. | ||
Stringaris A. Irritability in children and adolescents: a challenge for DSM-5. Eur Child Adolesc Psychiatry. 2011;20(2):61–66. | ||
Barkley RA, Fischer M. The unique contribution of emotional impulsiveness to impairment in major life activities in hyperactive children as adults. J Am Acad Child Adolesc Psychiatry. 2010;49(5):503–513. | ||
Seymour KE, Chronis-Tuscano A, Iwamoto DK, Kurdziel G, MacPherson L. Emotion regulation mediates the association between ADHD and depressive symptoms in a community sample of youth. J Abnorm Child Psychol. 2014;42(4):611–621. | ||
Villemonteix T, Purper-Ouakil D, Romo L. [Is emotional dysregulation a component of attention-deficit/hyperactivity disorder (ADHD)?]. Encephale. 2015;41(2):108–114. French. | ||
Cavanagh M, Quinn D, Duncan D, Graham T, Balbuena L. Oppositional defiant disorder is better conceptualized as a disorder of emotional regulation. J Atten Disord. 2017;21(5):381–389. | ||
Baweja R, Mayes SD, Hameed U, Waxmonsky JG. Disruptive mood dysregulation disorder: current insights. Neuropsychiatr Dis Treat. 2016;12:2115–2124. | ||
Roy AK, Klein RG, Angelosante A, et al. Clinical features of young children referred for impairing temper outbursts. J Child Adolesc Psychopharmacol. 2013;23(9):588–596. | ||
Leibenluft E. Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129–142. | ||
Cavelti M, Corbisiero S, Bitto H, et al. A comparison of self-reported emotional regulation skills in adults with attention-deficit/hyperactivity disorder and borderline personality disorder. J Atten Disord. 2017:1087054717698814. | ||
Wender PH, Wolf LE, Wasserstein J. Adults with ADHD. An overview. Ann N Y Acad Sci. 2001;931:1–16. | ||
Rösler M, Retz W, Fischer R, et al. Twenty-four-week treatment with extended release methylphenidate improves emotional symptoms in adult ADHD. World J Biol Psychiatry. 2010;11(5):709–718. | ||
Posner J, Kass E, Hulvershorn L. Using stimulants to treat ADHD-related emotional lability. Curr Psychiatry Rep. 2014;16(10):478. | ||
Konrad-Bindl DS, Gresser U, Richartz BM. Changes in behavior as side effects in methylphenidate treatment: review of the literature. Neuropsychiatr Dis Treat. 2016;12:2635–2647. | ||
Biederman J, Krishnan S, Zhang Y, McGough JJ, Findling RL. Efficacy and tolerability of lisdexamfetamine dimesylate (NRP-104) in children with attention-deficit/hyperactivity disorder: a phase III, multicenter, randomized, double-blind, forced-dose, parallel-group study. Clin Ther. 2007;29(3):450–463. | ||
Blader JC, Pliszka SR, Jensen PS, Schooler NR, Kafantaris V. Stimulant-responsive and stimulant-refractory aggressive behavior among children with ADHD. Pediatrics. 2010;126(4):e796–e806. | ||
Moukhtarian TR, Cooper RE, Vassos E, Moran P, Asherson P. Effects of stimulants and atomoxetine on emotional lability in adults: a systematic review and meta-analysis. Eur Psychiatry. 2017;44:198–207. | ||
Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry. 2005;58(2):125–131. | ||
Waxmonsky JG, Wymbs F, Pariseau ME, et al. A novel group therapy for children with ADHD and severe mood dysregulation. J Atten Disord. 2013;17(6):527–541. | ||
Philipsen A, Richter H, Peters J, et al. Structured group psychotherapy in adults with attention deficit hyperactivity disorder: results of an open multicentre study. J Nerv Ment Dis. 2007;195(12):1013–1019. | ||
Fleming AP, McMahon RJ, Moran LR, Peterson AP, Dreessen A. Pilot randomized controlled trial of dialectical behavior therapy group skills training for ADHD among college students. J Atten Disord. 2015;19(3):260–271. | ||
Mitchell JT, McIntyre EM, English JS, et al. A pilot trial of mindfulness meditation training for ADHD in adulthood: impact on core symptoms, executive functioning, and emotion dysregulation. J Atten Disord. 2017;21(13):1105–1120. | ||
Aadil M, Cosme RM, Chernaik J. Mindfulness-based cognitive behavioral therapy as an adjunct treatment of attention deficit hyperactivity disorder in young adults: a literature review. Cureus. 2017;9(5):e1269. | ||
Reimherr FW, Williams ED, Strong RE, et al. A double-blind, placebo-controlled, crossover study of osmotic release oral system methylphenidate in adults with ADHD with assessment of oppositional and emotional dimensions of the disorder. J Clin Psychiatry. 2007;68(1):93–101. | ||
Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980–988. | ||
Gökler B, Ünal F, Pehlivantürk B, Kültür EÇ, Akdemir D, Taner Y. Reliability and Validity of Schedule for Affective Disorders and Schizophrenia for School Age Children-Present and Lifetime Version-Turkish Version (K-SADS-PL-T). Turkish Journal of Child and Adolescent Mental Health. 2004;11(3):109–116. | ||
Gratz KL, Roemer L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J Psychopathol Behav Assess. 2004;26(1):41–54. | ||
Weinberg A, Klonsky ED. Measurement of emotion dysregulation in adolescents. Psychol Assess. 2009;21(4):616–621. | ||
Saritaş DA, Gençöz T, Özen A. Confirmatory factor analyses of the Difficulties in Emotion Regulation Scale (DERS) in a Turkish adolescent sample. Eur J Psychol Assess. 2015;31(1):12–19. | ||
Klonsky ED, Glenn CR. Assessing the functions of non-suicidal self-injury: psychometric properties of the inventory of Statements About Self-injury (ISAS). J Psychopathol Behav Assess. 2009;31(3):215–219. | ||
Bildik T, Somer O, Başay BK, Başay Ö, Özbaran B. Kendine Zarar Verme Davranişi Değerlendirme Envanteri’nin Türkçe Formunun Geçerlik ve Güvenilirlik Çalişmasi [The validity and reliability of the Turkish version of the inventory of statements about self-injury]. Turk Psikiyatri Derg. 2013;24(1):49–57. Turkish. | ||
Steiner H, Remsing L; Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(1):126–141. | ||
Arnsten AF, Pliszka SR. Catecholamine influences on prefrontal cortical function: relevance to treatment of attention deficit/hyperactivity disorder and related disorders. Pharmacol Biochem Behav. 2011;99(2):211–216. | ||
Wilens TE. Effects of methylphenidate on the catecholaminergic system in attention-deficit/hyperactivity disorder. J Clin Psychopharmacol. 2008;28(3 Suppl 2):S46–S53. | ||
Faraone SV. The pharmacology of amphetamine and methylphenidate: relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci Biobehav Rev. 2018;87:255–270. | ||
Bunford N, Evans SW, Langberg JM. Emotion dysregulation is associated with social impairment among young adolescents with ADHD. J Atten Disord. 2018;22(1):66–82. | ||
Sobanski E, Banaschewski T, Asherson P, et al. Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): clinical correlates and familial prevalence. J Child Psychol Psychiatry. 2010;51(8):915–923. | ||
Bunford N, Evans SW, Wymbs F. ADHD and emotion dysregulation among children and adolescents. Clin Child Fam Psychol Rev. 2015;18(3):185–217. | ||
Matthies S, Holzner S, Feige B, et al. ADHD as a serious risk factor for early smoking and nicotine dependence in adulthood. J Atten Disord. 2013;17(3):176–186. | ||
Kollins SH, McClernon FJ, Fuemmeler BF. Association between smoking and attention-deficit/hyperactivity disorder symptoms in a population-based sample of young adults. Arch Gen Psychiatry. 2005;62(10):1142–1147. | ||
Rhodes JD, Pelham WE, Gnagy EM, et al. Cigarette smoking and ADHD: an examination of prognostically relevant smoking behaviors among adolescents and young adults. Psychol Addict Behav. 2016;30(5):588–600. | ||
Wilens TE, Martelon M, Anderson JP, Shelley-Abrahamson R, Biederman J. Difficulties in emotional regulation and substance use disorders: a controlled family study of bipolar adolescents. Drug Alcohol Depend. 2013;132(1–2):114–121. | ||
Dinn WM, Aycicegi A, Harris CL. Cigarette smoking in a student sample: neurocognitive and clinical correlates. Addict Behav. 2004;29(1):107–126. | ||
Wilens TE, Adamson J, Sgambati S, et al. Do individuals with ADHD self-medicate with cigarettes and substances of abuse? Results from a controlled family study of ADHD. Am J Addict. 2007;16 Suppl 1:14–21. | ||
Taylor MR, Boden JM, Rucklidge JJ. The relationship between ADHD symptomatology and self-harm, suicidal ideation, and suicidal behaviours in adults: a pilot study. Atten Defic Hyperact Disord. 2014;6(4):303–312. | ||
Izutsu T, Shimotsu S, Matsumoto T, et al. Deliberate self-harm and childhood hyperactivity in junior high school students. Eur Child Adolesc Psychiatry. 2006;15(3):172–176. | ||
Semiz UB, Basoglu C, Oner O, et al. Effects of diagnostic comorbidity and dimensional symptoms of attention-deficit-hyperactivity disorder in men with antisocial personality disorder. Aust N Z J Psychiatry. 2008;42(5):405–413. | ||
Whitlock J, Muehlenkamp J, Purington A, et al. Nonsuicidal self-injury in a college population: general trends and sex differences. J Am Coll Health. 2011;59(8):691–698. | ||
Kirkcaldy BD, Brown J, Siefen RG. Disruptive behavioural disorders, self harm and suicidal ideation among German adolescents in psychiatric care. Int J Adolesc Med Health. 2006;18(4):597–614. | ||
Chronis-Tuscano A, Molina BS, Pelham WE, et al. Very early predictors of adolescent depression and suicide attempts in children with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry. 2010;67(10):1044–1051. | ||
Swanson EN, Owens EB, Hinshaw SP. Pathways to self-harmful behaviors in young women with and without ADHD: a longitudinal examination of mediating factors. J Child Psychol Psychiatry. 2014;55(5):505–515. | ||
Turner BJ, Chapman AL, Layden BK. Intrapersonal and interpersonal functions of non suicidal self-injury: associations with emotional and social functioning. Suicide Life Threat Behav. 2012;42(1):36–55. | ||
Gratz KL. Targeting emotion dysregulation in the treatment of self-injury. J Clin Psychol. 2007;63(11):1091–1103. | ||
Wilcox HC, Arria AM, Caldeira KM, et al. Longitudinal predictors of past-year non-suicidal self-injury and motives among college students. Psychol Med. 2012;42(4):717–726. | ||
Kim J, Cicchetti D. Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. J Child Psychol Psychiatry. 2010;51(6):706–716. | ||
Camras LA, Sachs-Alter E, Ribordy SC. Emotion understanding in maltreated children: Recognition of facial expressions and integration with other emotion cues. In: Lewis M, Sullivan MW, editors. Emotional development in atypical children. Hillsdale, NJ: Lawrence Erlbaum Associates; 1996:203–225. | ||
Dvir Y, Ford JD, Hill M, Frazier JA. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harv Rev Psychiatry. 2014;22(3):149–161. | ||
Prayez F, Wodon I, Van Hyfte S, Linkowski P. [Attention-deficit/hyperactivity disorder (ADHD) and child maltreatment: a review]. Rev Med Brux. 2012;33(2):75–86. French. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.