Back to Journals » Drug Design, Development and Therapy » Volume 18
Sivelestat Sodium Alleviates Ischemia-Reperfusion-Induced Acute Kidney Injury via Suppressing TLR4/Myd88/NF-κB Signaling Pathway in Mice
Authors Wang J, Wu Y, Mao M, Bing H ![]() , Sun L, Xu W, Tian W, Xia Z, Jin X
, Sun L, Xu W, Tian W, Xia Z, Jin X ![]() , Chu Q
, Chu Q
Received 23 July 2024
Accepted for publication 27 September 2024
Published 5 October 2024 Volume 2024:18 Pages 4449—4458
DOI https://doi.org/10.2147/DDDT.S480148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jie Wang,1 Yuanbo Wu,2 Meng Mao,3 Hailong Bing,1 Liwei Sun,1 Wei Xu,1 Wangli Tian,1 Zhengyuan Xia,4,5 Xiaogao Jin,1,6 Qinjun Chu1
1Department of Anesthesiology and Perioperative Medicine, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, People’s Republic of China; 2Department of Anesthesiology, Hubei Cancer Hospital, Wuhan, Hubei, People’s Republic of China; 3Center for Advanced Medicine, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, 450007, People’s Republic of China; 4Department of Anesthesiology, The First Affiliated Hospital, Jinan University, Guangzhou, People’s Republic of China; 5Department of Anesthesiology, The University of Hong Kong, Hong Kong; 6Department of Anesthesiology, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, People’s Republic of China
Correspondence: Xiaogao Jin; Qinjun Chu, Email [email protected]; [email protected]
Purpose: We aim to detect the effects of sivelestat on renal ischemia-reperfusion associated with AKI and also explore the underlying mechanism.
Materials and Methods: Mice, aged between 8 and 12 weeks, were randomly allocated among four distinct groups, respectively normal saline sham group(C), normal saline surgery group(I), sivelestat (50 mg/kg) sham group(S), sivelestat (50 mg/kg) surgery group(SI) (n=6, each group). In the surgical groups, the renal pedicles of mice were clamped with non-traumatic micro-aneurysm clamps, resulting in ischemia of the kidneys for 45 minutes. This was followed by a period of reperfusion lasting 24 hours. Sham group mice underwent the identical surgery produced without clamping renal pedicles. Mice blood was obtained from eyeballs, and Serum creatinine and blood urea nitrogen levels were measured. After a 24-hour period of reperfusion, the mice were euthanized, and their kidneys were gathered for various analyses, including Western Blot (WB) analysis, RT-PCR, immunofluorescence (IF), hematoxylin and eosin (H&E) staining, and Tunel assay.
Results: Pretreatments with sivelestat decreased renal Neutrophil elastase (NE), serum creatinine, and blood urea nitrogen levels after renal ischemia-reperfusion. Sivelestat also reduced histological damage and cell apoptosis in kidneys following ischemia-reperfusion injury (IRI). In addition, the sivelestat administration diminished the levels of mRNA expression of interleukin 6 (IL-6), Macrophage inflammatory protein-2 (MIP-2), monocyte chemoattractant protein-1 (MCP-1), and tumor necrosis factor (TNF)-α in the kidneys during IRI. The kidney tissues of the SI group had significantly mitigated TLR4, Myd88, and NF-κB p-p65 protein expression levels compared to the I group (all P< 0.05).
Conclusion: We demonstrated a previously unidentified mechanism that sivelestat effectively attenuates AKI-induced renal dysfunction, possibly through suppressing the TLR4/Myd88/ NF-κB pathway.
Keywords: neutrophil elastase, ischemia reperfusion injury, renal dysfunction, inflammation
Introduction
Renal ischemia-reperfusion injury (IRI) is a serious medical disease that causes acute kidney injury (AKI), resulting in fast renal dysfunction and high death rates. These conditions, including kidney transplantation, shock, trauma, and urologic and cardiovascular surgery, are often seen and lack appropriate therapeutic options.1 Hence, it is imperative to explore the mechanism of AKI to facilitate the selection of treatment methods or the development of related drugs. The inflammatory response is essential in developing ischemic AKI. Neutrophils are the earliest leukocytes that gather in the kidney following ischemia damage, both in animal models and in humans with AKI,2 and are the main contributors to kidney injury.3,4
Neutrophil elastase (NE) is a serine protease that accelerates the synthesis of pro-inflammatory cytokines, hence intensifying the existing inflammation induced by neutrophils. NE can affect various substances, such as extracellular matrix (ECM) components, inactive enzymes, molecules involved in cell adhesion, receptors responsible for signaling, and cytokines.5 NE is the most abundant protease expressed by neutrophils.6
Sivelestat, a specific NE inhibitor, is currently approved for the treatment of acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). It was reported that sivelestat could downregulate the production of NE or proinflammatory cytokines and is help for improving pulmonary dysfunction. In addition, sivelestat has applications in the study of cancer. In recent years, it also was used for the treatment of COVID-19 in China. Additionally, studies have shown that sivelestat plays an important role in a variety of ischemic diseases, including cardiac IRI7 and cerebral IRI,8 Liver IRI,9,10 bladder IRI,11 and aortic IRI.12 Sivelestat has been shown to reduce AKI due to sepsis and acute pancreatitis.13,14 Hayama et al15 showed that sivelestat can attenuate kidney injury caused by renal IR in rats, but the mechanism is unclear. In this research work, we determined the sivelestat implications on renal IR-associated AKI in a mouse model and examined the underlying mechanism.
Materials and Methods
Animals
Male C57BL/6J mice, aged 8 to 12 weeks and weighing 22 to 25 grams, were acquired (Changsheng Biotech Co., Ltd. LiaoNing, China). The mice were housed in a controlled environment that ensured there were no disease-causing agents present. The circumstances were carefully regulated to maintain a consistent temperature of 20–22°C and humidity levels of 50–60%. Mice were exposed to a 12-hour alternating pattern of light and darkness and given unlimited access to food and drink. Mice experiments were followed the rules of guidelines for the care and use of laboratory animals. All experimental protocols strictly abide by the guidelines of Animal Experiment Ethics Committee of Zhengzhou Central Hospital Affiliated to Zhengzhou University (Ethics Batch Number: 202457). In this study, quantitative analysis experiments (eg, Assessment of Kidney Function, Quantitative Real-Time Reverse Transcriptase PCR) were biologically repeated six times. The semi-quantitative experiments were also repeated biologically four times, with each repeat being performed separately and independently.
Renal IR Procedure and Animal Grouping
Anesthesia was administered by intraperitoneal injection of esketamine (50 mg/kg) and Midazolam (40 mg/kg). These kidneys were subjected and underwent ischemia by applying non-traumatic micro-aneurysm clamps to the renal pedicles. The clamps were eliminated during a period of 45 minutes of ischemia. During the operation, the mice were maintained at a warm temperature using a heat pad. The sham-group mice experienced the identical surgical technique, with the exception of pedicle clamping. Mice blood was obtained from eyeballs, and serum creatinine and blood urea nitrogen levels were quantified. Twenty-four hours following the reperfusion, the mice were euthanized, and their kidneys were obtained for the purpose of conducting Western Blot (WB) analysis, RT-PCR, immunofluorescence (IF), Hematoxylin and Eosin (H&E) staining, and Tunel Assay.
Study Groups
The mice were allocated into 4 groups randomly (n=6/group) as follows:
- Group C: the sham-operated group was administered normal saline(NS) 0.9% sodium chloride (Sham+NS);
- Group I: the mice operated with IRI and were administered NS 0.9% sodium chloride (IRI+NS);
- Group S: the sham-operated group administered sivelestat (Sham+sivelestat);
- Group SI: the mice operated with IRI and were administered sivelestat (IRI+sivelestat);
After anesthesia, mice in the respective groups are administered 0.9% sodium chloride or 50mg/kg sivelestat (approximately 0.1mL) injected through the retro-orbital vein.16
Assessment of Kidney Function
The serum creatinine measurement was performed with an accessible creatinine test kit (Cat No.C011-2-1, Nanjing jiancheng Bioengineering Institute).Blood urea nitrogen (BUN) levels were quantified (Cat No. BC1535, Solarbio, China) (n=6/group).
Apoptosis Detection
The Apoptosis Detection Kit (Cat no. MK1025, Booster Biological Technology, Ltd. China) was applied for the purpose of apoptosis detection. The presence of apoptotic cells was assessed with a terminal transferase dUTP nick-end labeling (TUNEL) assay. The quantity of TUNEL-positive cells in five randomly chosen high-power fields (HPF) per sample was measured in a way where the observer was unaware of the sample identity (n=4/group).
WB Analysis
A mixture of protease inhibitors was implemented to isolate the proteins with RIPA buffer. The protein content was determined with a Bio-Rad protein assay. An SDS-polyacrylamide gel with a Tris/SDS buffer solution was typically loaded with 40 mg of protein. In the subsequent step, the proteins in the gels were placed onto nitrocellulose membranes. The membranes were incubated with primary antibodies at ambient temperature overnight following the blocking phase. The membranes were incubated with the secondary antibodies following the rinsing procedure. The proteins were determined with a WB imaging instrument (Amersham™ ImageQuant™ 800 biomolecular imager, MA, USA). The protein expression was ascertained utilizing the NIH Image/J program (the National Institutes of Health, Bethesda, MD, USA) (n=4/group).
H&E Staining
The kidney tissues that had been fixed using formaldehyde were embedded in paraffin and then sliced into sections that were 5 µm thick. These sections were subsequently treated with xylene to remove the paraffin and gradually rehydrated using ethanol. Hematoxylin (Solarbio, Beijing, China) and eosin (Sinopharm) were applied to stain these sections for morphological investigation.The tubular injury score was scored by the pathologists who were not aware of the group. Tubular damage score is based on the percentage of tubular damage, no damage, 0 point; 1–25% damage, 1 point; 25–50% damage, 2 points; 50–75% damage, 3points; 75–100% damage, 4 points (n=4/group).
IF Assay
IF was conducted on paraffin-embedded kidney slices. Tissue sections were dehydrated and dewaxed, and antigen retrieval was conducted. Antigen retrieval solution (0.01 M sodium citrate, Ph.6.0, Solarbio, Life Sciences, China). Endogenous peroxidase activity was blocked with 3% H2O2, and 0.5% 100×Triton was used to break the cell membrane, followed by Incubating the block with 5% donkey serum and incubating the slides with the primary antibody overnight in a humidified chamber. Following the process of washing, fluorescent secondary antibodies incubated kidney sections; the nuclei were stained with DAPI after further washing (n=4/group).
Quantitative Real-Time Reverse Transcriptase PCR
The extraction of total RNA from the kidney tissues was executed with a TRIzol reagent (Invitrogen, Carlsbad, CA). Subsequently, a quantity of 1 µg of mRNA was reverse transcribed using the NovoScriptPlus All-in-one 1st Strand cDNA Synthesis SuperMix (gDNA Purge) (Novoprotein, Suzhou, China). The Real-time PCR analysis was conducted using a Bio-Rad real-time PCR instrument with the NovoStartSYBR qPCR SuperMix Plus kit manufactured by Novoprotein. The measurement of target gene expression was calculated with the comparative Ct technique (ΔΔCt), and the relative measurement was provided as 2−ΔΔCt. The ratios of the target genes to the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH) were compared across various groups. The primer sequences for the target genes are shown in Table 1. (n=6/group).
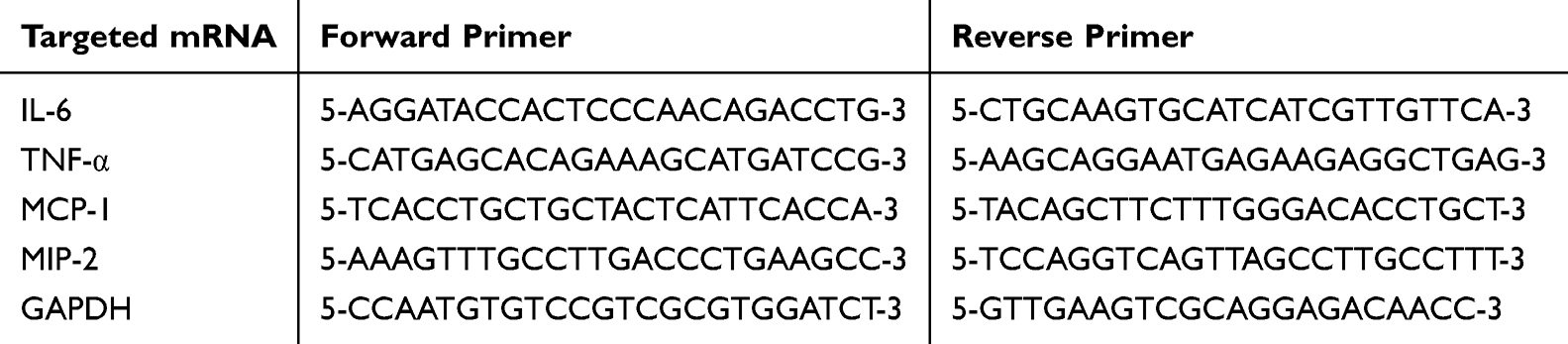 |
Table 1 The Primer Sequences Used in This Study |
Statistical Analysis
All data were expressed as mean ± SD. The ANOVA statistical test was applied to compare various groups, and subsequently, the Bonferroni process was implemented to compare the means. The Wilcoxon rank sum test was applied to examine the scores of renal tubular damage. P < 0.05 was deemed significant.
Results
Pretreatment with Sivelestat Decreases Renal NE Expression After Renal IR
To clarify the effectiveness of sivelestat on renal IRI in mice, we first examined the implications of sivelestat pretreatment on NE expression after renal IR. We emerged that contrasted with the control group (C), the elastase level was significantly raised after renal IRI (group I), while the elastase level was significantly decreased after sivelestat treatment (SI) (Figure 1A and B). In addition, administration of sivelestat alone in the absence of IRI did not impact the NE protein levels contrasted with the sham-operated mouse. Similarly, the results of IF staining of kidney sections also showed that the level of NE in renal tubular cells was significantly reduced after sivelestat treatment, indicating that sivelestat pretreatment could reduce the increase of NE expression after renal IRI (Figure 1C).
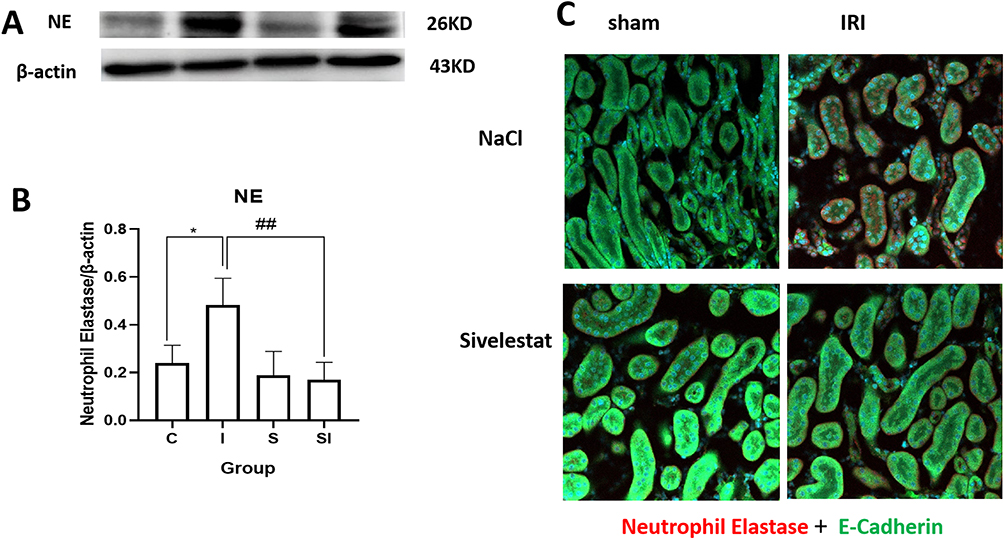 |
Figure 1 WB results of NE in the kidneys. (A) Illustrative outcomes of NE protein expression as assessed by WB in the four groups (Sham+NS, IRI +NS, Sham+sivelestat, IRI + sivelestat groups). (B) Quantitative assessment of NE protein expression. *P<0.05, I group vs C group. ##P<0.01, SI group vs I group. (C) IF results of NE expression in the kidneys. NE expression in the kidneys in the four. The NE region was labeled with the red Cy5.5, whereas the tubular epithelial cells cytoplasm exhibited green fluorescence due to the FITC staining of E-Cadherin. The nuclear material was dyed purple using DAPI. Sham surgery with NaCl injection group, Sham + NS group, C group. IRI surgery with NaCl injection group, IRI + NS group, I group; Sham surgery with sivelestat injection group, Sham + sivelestat group, S group; IRI surgery with sivelestat injection group, IRI + sivelestat group, SI group; Western blot, WB; Immunofluorescence, IF; Neutrophil elastase, NE; Ischemia reperfusion injury, IRI; normal saline, NS. |
Sivelestat Protected the Kidney from IRI
Subsequently, we investigated the impact of sivelestat on BUN and serum creatinine levels following renal ischemia. The findings indicated that the mice exposed to kidney IRI had impaired kidney function, as seen by significant elevations in BUN and serum creatinine levels (Figure 2A and B). The pathological investigation manifested that the renal injury in IRI was marked by the expansion of the tubules, shedding of the epithelial cells lining the tubules, development of casts, and brush boundary loss in the cells lining the tubules (Figure 2C). The tubular damage score was implemented to assess the renal injury extent. Pretreatment with sivelestat provided protection to the kidney against pathological damage caused by IRI, as shown by a hindrance in the tubular damage score (Figure 2D). To provide further evidence of sivelestat’s anti-apoptosis implication, the Tunel assay was applied to identify apoptosis in the kidney following IRI (Figure 2E). Sivelestat pretreatment significantly prevented the renal apoptosis induced by IRI (Figure 2F).
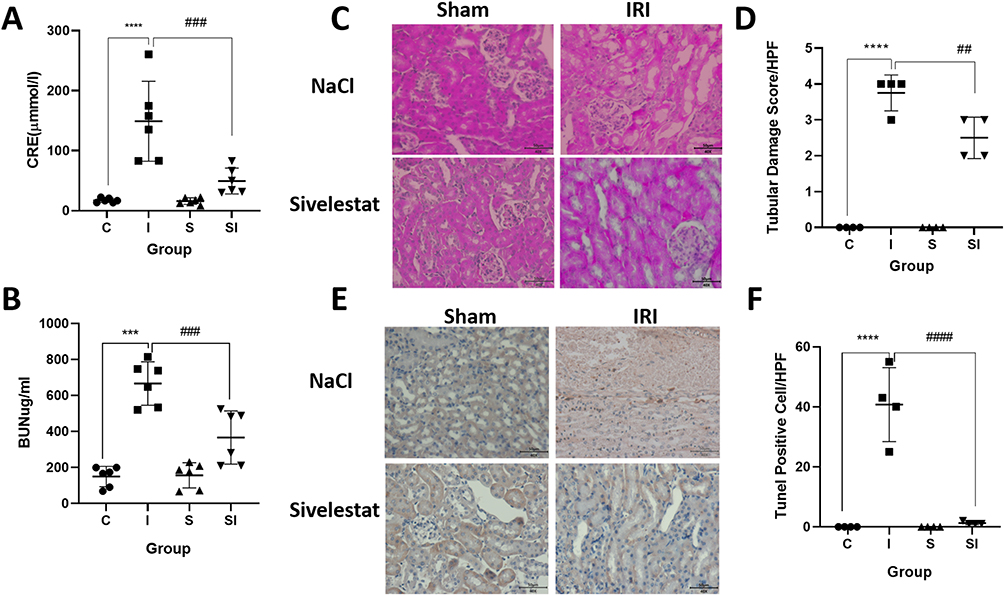 |
Figure 2 Pretreatment with sivelestat provided protection to the kidney against IRI. (A) Data summarizing the alterations in serum CRE levels in the four groups (Sham +NS, IRI+NS, Sham + sivelestat, IRI + sivelestat groups). ****P < 0.0001, vs sham group treated with NS. ###P < 0.001, vs IRI group treated with NS. (B) Data summarizing the variations in serum BUN level across mice in the four groups. ***P < 0.001, vs sham+ NS group. ###P < 0.001, vs IRI+NS group. (C) Renal H&E staining images demonstrating the four groups. (D) Summarized the tubular damage scores across the four groups/HPF. ****P < 0.0001, vs sham+NS group. ##P< 0.01, vs IRI+NS group. (E) Illustrative outcomes of apoptosis in the kidneys, as determined by the TUNEL assay, showing apoptotic cells (brown) and counterstaining with hematoxylin (blue) in the 4 groups (Pictures original magnification is 400×). (F) The quantitative assessment for apoptotic cells in the kidneys. ****P< 0.0001, vs sham group treated with NS. ####P < 0.0001, vs IRI group treated with NS.(n=4 per group). Sham surgery with NaCl injection group, Sham + NS group, C group; IRI surgery with NaCl injection group, IRI + NS group, I group; Sham surgery with sivelestat injection group, Sham + sivelestat group, S group; IRI surgery with sivelestat injection group, IRI + sivelestat group, SI group; HPF indicates a high power field. Ischemia reperfusion injury, IRI; normal saline, NS; creatinine, CRE; Blood urea nitrogen, BUN. |
Sivelestat Reduced Neutrophil Infiltration After IRI
Considering the fact that neutrophils act as the primary defense when renal IR occurs, we further examined the effect of Sivelestat treatment on neutrophil infiltration. Myeloperoxidase (MPO) serves as an indicator of neutrophil activation, with its quantity and functionality reflecting the performance and condition of polymorphonuclear leukocytes. The IF results showed that neutrophil infiltration levels increased dramatically after IR of renal tissue, whereas neutrophil aggregation decreased in the SI group pre-treated with sivelestat. (Figure 3)
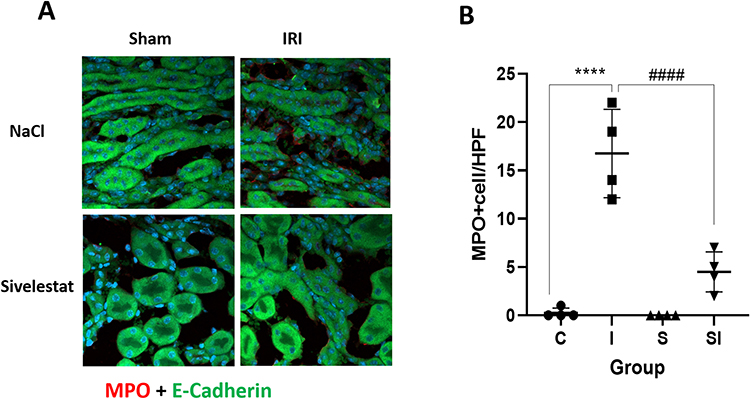 |
Figure 3 Changes of MPO after IRI in the kidney. (A) IF findings of MPO expression in the kidneys. MPO expression in the kidneys in the 4 groups (Sham + NS, IRI+NS, Sham + sivelestat, IRI+sivelestat groups). MPO was stained red using Cy5.5, while E-Cadherin in the cytoplasm of tubular epithelial cells was stained green with FITC. The nuclei were stained purple with DAPI. (B) MPO+cell/HFP ****p < 0.0001 IRI + NS group vs.Sham + NS group; ####p < 0.0001 IRI + NS group vs.IRI + sivelestat group; Data are expressed as Mean ±SD, n = 4 per group. Sham surgery with NaCl injection group, Sham + NS group, C group; IRI surgery with NaCl injection group, IRI + NS group, I group; Sham surgery with sivelestat injection group, Sham + sivelestat group, S group; IRI surgery with sivelestat injection group, IRI + sivelestat group, SI group; Myeloperoxidase, MPO; Ischemia reperfusion injury, IRI; normal saline, NS; High power field, HPF. |
Sivelestat Inhibited the Release of Renal Pro-Inflammatory Mediators and Chemokines After IRI
In normal conditions, kidney injury usually stimulates the transcription, expression, and secretion of inflammatory cytokines. Next, we examined the effect of sivelestat on inflammatory cytokine levels. Figure 4 demonstrates that the mRNA expression levels of interleukin 6 (IL-6), tumor necrosis factor (TNF)-α, monocyte chemoattractant protein-1 (MCP-1), and Macrophage inflammatory protein-2 (MIP-2) were significantly elevated in the kidneys of mice following IRI contrasted with mice in the control group that had a sham operation, whereas decreased in the group treated with sivelestat treated IRI group. These results indicate that the application of sivelestat significantly ameliorated the inflammatory reaction after IRI.
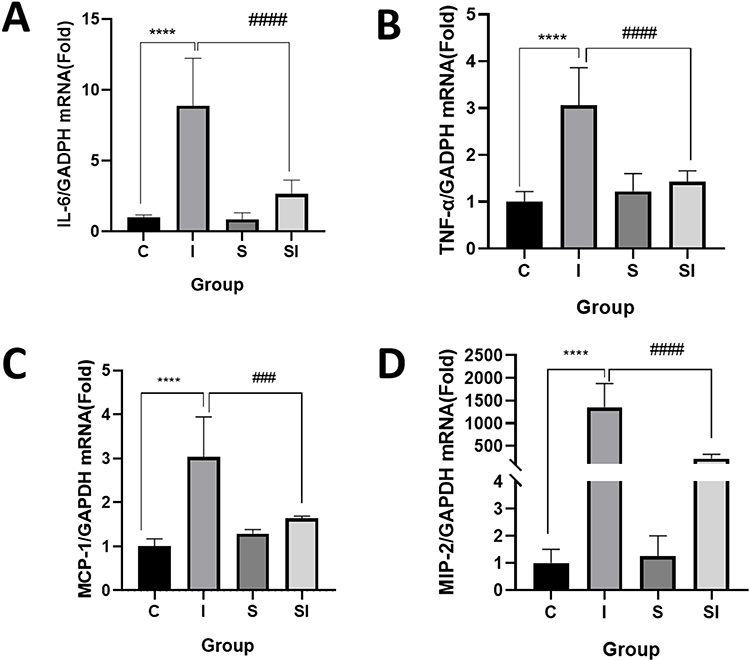 |
Figure 4 Effect of sivelestat on inflammatory cytokines expression in the IRI. (A–D) IL-6, TNF-αmRNA, MCP-1, and MIP-2 mRNA expressions were displayed in a dot plot. ****p < 0.0001 vs Sham + NS group; ####p < 0.0001 vs IRI + sivelestat group; n = 6 per group. Data are presented as Mean ± SD. Sham surgery with NaCl injection group, Sham + NS group, C group; IRI surgery with NaCl injection group, IRI + NS group, I group; Sham surgery with sivelestat injection group, Sham + sivelestat group, S group; IRI surgery with sivelestat injection group, IRI + sivelestat group, SI group; Ischemia reperfusion injury, IRI; normal saline, NS. |
Sivelestat Suppressed the TLR4/Myd88/NF-κB Pathway Activation After IRI
Numerous investigations have demonstrated that TLR4/Myd88/NF-κB signaling is involved in regulating inflammation. The results shown in Figure 4 indicated the potential of sivelestat to ameliorate inflammatory reactions after IRI. Based on this, we investigated the influence of sivelestat on activating the TLR4/Myd88/NF-κB signaling following IRI. The outcomes of WB analysis manifested that in the I group (IRI+NS), the renal tissues of mice had significantly elevated TLR4 (Figure 5B), Myd88 (Figure 5C), and NF-κB-pp65 (Figure 5D) protein levels compared to the C group (Sham+NS) (all P<0.05), while the kidney tissues of the SI group (IRI+sivelestat) exhibited significantly mitigated these levels contrasted with the untreated I group (IRI+NS) (all P<0.05). (Figure 5)
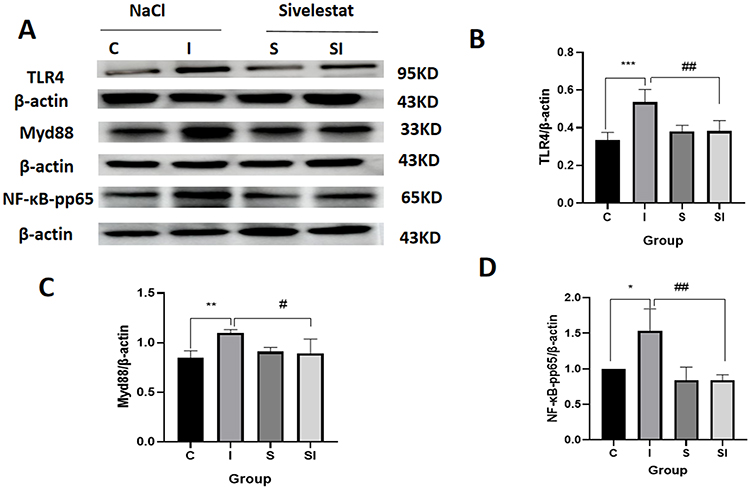 |
Figure 5 Changes of protein levels of TLR4, Myd88, NF-κB-pp65 after IRI in the kidneys. (A) Representative results of TLR4, Myd88, NF-κB-pp65 expression in WB in the four groups (Sham +NS, IRI+NS, Sham + sivelestat, IRI+sivelestat groups). (B) Quantitative analysis of TLR4 expression in the WB. ***P<0.001, I group vs C group. ##P<0.01, SI group vs I group. (C) Quantitative analysis of Myd88 expression in the WB. **P<0.01, I group vs C group. #P<0.05, SI group vs I group. (D) Quantitative analysis of NF-κB-pp65 expression in the WB. *P<0.05, I group vs C group. ##P<0.01, SI group vs I group. Data are Mean ± SD. Sham surgery with NaCl injection group, Sham + NS group, C group; IRI surgery with NaCl injection group, IRI + NS group, I group; Sham surgery with sivelestat injection group, Sham + sivelestat group, S group; IRI surgery with sivelestat injection group, IRI + sivelestat group, SI group; Western Blot, WB; Ischemia reperfusion injury, IRI; normal saline, NS. |
Discussion
Herein, we have emerged that pre-treatment with sivelestat significantly attenuated IRI-induced kidney injury that was associated with concomitant reductions in pro-inflammatory cytokines and the related signaling pathway proteins TLR4, Myd88, and NF-κB. This is suggestive that inhibition of TLR4/Myd88/NF-κB signaling may represent a mechanism by which sivelestat confers protection against IRI-induced kidney injury.
In this study, an IRI mouse model was used to simulate AKI. The IRI model is one of the commonly used animal models to study AKI, and its operation method is simple and time-saving. IRI model mice have partial loss of renal function and renal tubular epithelial cell necrosis in the acute phase, presenting as AKI. This study uses a bilateral renal pedicle clipping IRI model, which is often used to induce ischemia in animals,17 because it has pathophysiological conditions similar to human AKI, and patients may have bilateral renal damage due to impaired blood flow.18
Sivelestat is a specific NE inhibitor with ideal clinical efficacy for systemic inflammatory response syndrome (SIRS), acute pulmonary edema, and ventilatory dysfunction.19 NE can cleave cell adhesion and junctional. In recent years, it has been found that sivelestat has an inhibitory effect on inflammatory cells, inhibits neutrophil aggregation, activation, and invasion, reduces the secretion of inflammatory factors, and alleviates inflammation.20,21 In this study, it was found that sivelestat could possess a protective impact on renal IRI-induced kidney injury in mice. Post-ischemic renal function was significantly preserved in mice administered with sivelestat, which was characterized by reduced histological damage and decreased serum creatinine and blood urea nitrogen levels after IRI injury, consistent with the results observed by T. Hayama et al in a rat renal IR model.15 Serum creatinine and blood urea nitrogen levels are one of the most commonly used indicators of renal function. In this study, the serum creatinine and blood urea nitrogen level in mice was significantly greater than that in the sham operation group following renal IRI, and the serum creatinine and blood urea nitrogen level in the SI group was significantly mitigated, which was aligned with the outcomes of histopathological HE staining for renal tubular injury. The appearance of the kidneys in the IRI group was swollen and gray, and the cutaneous medullary demarcation was not clear; the main manifestations were renal tubulointerstitial lesions under microscopy, with obvious tubular epithelial cell edema, vacuolar degeneration, basement membrane shrinkage, disappearance of brush margins, nuclear fragmentation, and intertubular capillary hyperemia and so on.
At present, the clinical diagnosis of kidney damage mostly relies on monitoring modifications to urine output and renal function markers. However, it is important to note that urine output may be influenced by fluid replacement and diuretic medications. Although studies have shown that creatinine in renal function measures may not change significantly in the early stages of kidney injury and that blood urea nitrogen levels are susceptible to non-renal factors, the commonly used endpoints to measure kidney injury in animal models of IRI are creatinine and urea nitrogen levels (serum and blood).
The development and advancement of AKI are accompanied by the production and release of inflammatory factors, chemokines, infiltration of inflammatory cells, vascular endothelial cell injury, and renal tubular necrosis. In the present investigation, the IRI group exhibited significant elevation in the inflammatory factors and chemokines levels, which contrasted with group C, but they were significantly mitigated in the SI group, which contrasted with group I. Neutrophil infiltration exhibited a rise in the IRI group and a decline in the SI group, suggesting that Sivelestat inhibited the inflammatory response after renal IR. Research by Kumasaka et al showed that Sivelestat, a NE inhibitor, may mitigate tissue damage in rats with anti-Thy1.1 nephritis.22 Voisin et al used NE knockout mice to stimulate I/R injury in several organs, including the myocardium, kidneys, mesentery, and cremaster muscles. In all of these models, a significant hindrance in neutrophil infiltration into the tissue was seen, leading to a simultaneous prevention of acute tissue injury.5
Mammals have been shown to possess toll-like receptors that may detect pathogen-associated molecular patterns (PAMPs). Furthermore, PAMP is also considered to be a sentinel of tissue injury and a catalyst for the inflammatory cascade. TLR4, a member of the TLR family, has significant expression in several organs. It has a vital function in innate immunity by interacting with a wide range of exo- and endogenous ligands. This interaction triggers acute inflammatory reactions.23 When IRI occurs, the increase in TLR-4 expression subsequently activates the downstream NF-κB pathway, and the endogenous inflammatory pathway is activated, resulting in the generation of an extensive number of inflammatory factors, encompassing TNF-α and IL-6. Studies have shown that apoptosis of renal tubular cells is mediated by inflammatory damage. Adhesion factors in the ischemic region are also upregulated after renal IR, leading to an inflammatory cascade, which is induced by adhesion factors that mediate endothelial-neutrophil adhesion. In this work, in the kidney tissues of mice following IRI, the TLR4, Myd88, NF-κB-pp65, and NE proteins levels were significantly elevated. Additionally, these markers levels in the kidney tissues of the SI group were significantly mitigated contrasted with the I group. Combined with the outcomes of this study and the above analysis, it is speculated that sivelestat may alleviate the pathological changes of IR AKI in mice by controlling TLR4, Myd88, and NF-κB pathways, thereby inhibiting the TLR4 and Myd88 levels and downregulating the NF-κB pp65 and NE expression.
Through our study, we can see that sivelestat can significantly reduce IRI-induced AKI in mice. Therefore, in the future, sivelestat may be used as part of the effective treatment of patients with AKI in clinical practice, including AKI patients due to volume depletion in trauma patients, AKI patients undergoing cardiac surgery under cardiopulmonary bypass, and kidney transplant patients, etc. Our current study may have the following limitations: 1. The administration method of sivelestat is intravenous pumping, and the method of single intravenous administration is used in this study. Nevertheless, the total amount of administration is the same. 2. In this study, different drug concentration gradients were not set at different time points, but the protective effect of the drug was clearly seen. 3. The pathogenesis of AKI is complex and diverse; A variety of signaling pathways are involved in the occurrence and development of AKI, such as: Ras/MAPKs/PPAR-γ; AMPK/ SENP1/Sirt3; Hippo-YAP/MCP-1; JAK/STAT/SOCS; etc.This study only focused on the classical inflammatory TLR4/Myd88/NF-κB pathway and did not observe the phenomenon of inhibition of this signaling pathway protein at the animal and cellular levels. In the future, more studies such as gene sequencing and proteomics should be conducted to explore the relationship between sivelestat and AKI.
Conclusion
It is concluded that sivelestat can improve the renal function of AKI in mice, reduce the inflammatory response and pathological damage of kidney tissue, and that suppression of TLR4/Myd88/NF-κB signaling may represent a mechanism by which sivelestat confers protection against IRI-induced kidney injury. The insight gained from the current study may provide clues for the development of new therapies for clinical AKI patients.
Acknowledgments
The research was supported financially by grants from Henan Provincial Science and Technology Research Project (222102310019) and Provincial and ministerial joint construction project of Henan Provincial Department of Science and Technology (SBGJ202102209).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Thapa K, Singh T, Kaur A. Targeting ferroptosis in ischemia/reperfusion renal injury. Naunyn Schmiedebergs Arch Pharmacol. 2022;395(11):1331–1341. doi:10.1007/s00210-022-02277-5
2. Chen Q, Gu Q, Yin A, et al. Neutrophil percentage as a potential biomarker of acute kidney injury risk and short-term prognosis in patients with acute myocardial infarction in the elderly. Clin Interv Aging. 2024;19:503–515. doi:10.2147/CIA.S455588
3. Han S, Lee H, Practice C. Mechanisms and therapeutic targets of ischemic acute kidney injury. Kidney Res Clin Pract. 2019;38(4):427–440. doi:10.23876/j.krcp.19.062
4. Yang J, Chen C, Miao X, et al. Injury site specific xenon delivered by platelet membrane-mimicking hybrid microbubbles to protect against acute kidney injury via inhibition of cellular senescence. Adv Healthc Mater. 2023;12(20):e2203359. doi:10.1002/adhm.202203359
5. Voisin M, Leoni G, Woodfin A, et al. Neutrophil elastase plays a non-redundant role in remodeling the venular basement membrane and neutrophil diapedesis post-ischemia/reperfusion injury. J Pathol. 2019;248(1):88–102. doi:10.1002/path.5234
6. Häger M, Cowland J, Borregaard N. Neutrophil granules in health and disease. J Intern Med. 2010;268(1):25–34. doi:10.1111/j.1365-2796.2010.02237.x
7. Bidouard J, Duval N, Kapui Z, et al. SSR69071, an elastase inhibitor, reduces myocardial infarct size following ischemia-reperfusion injury. Eur J Pharmacol. 2003;461(1):49–52. doi:10.1016/S0014-2999(03)01298-6
8. Stowe A, Adair-Kirk T, Gonzales E, et al. Neutrophil elastase and neurovascular injury following focal stroke and reperfusion. Neurobiol Dis. 2009;35(1):82–90. doi:10.1016/j.nbd.2009.04.006
9. Uchida Y, Freitas M, Zhao D, et al. The protective function of neutrophil elastase inhibitor in liver ischemia/reperfusion injury. Transplantation. 2010;89(9):1050–1056. doi:10.1097/TP.0b013e3181d45a98
10. Yamaguchi Y, Akizuki E, Ichiguchi O, et al. Neutrophil elastase inhibitor reduces neutrophil chemoattractant production after ischemia-reperfusion in rat liver. Gastroenterology. 1997;112(2):551–560. doi:10.1053/gast.1997.v112.pm9024309
11. Kono T, Okada S, Saito MJM, et al. Neutrophil elastase inhibitor, sivelestat sodium hydrate prevents ischemia–reperfusion injury in the rat bladder. Mol Cell Biochem. 2008;311(1–2):87–92. doi:10.1007/s11010-007-9698-9
12. Fujimura N, Obara H, Suda K, et al. Neutrophil elastase inhibitor improves survival rate after ischemia reperfusion injury caused by supravisceral aortic clamping in rats. J Surg Res. 2013;180(1):e31–6. doi:10.1016/j.jss.2012.04.037
13. Li G, Jia J, Ji K, et al. The neutrophil elastase inhibitor, sivelestat, attenuates sepsis-related kidney injury in rats. Int J Mol Med. 2016;38(3):767–775. doi:10.3892/ijmm.2016.2665
14. Wang H, Tang A, Liu D, et al. Renoprotective activity of sivelestat in severe acute pancreatitis in rats. Exp Ther Med. 2013;6(1):29–32. doi:10.3892/etm.2013.1075
15. Hayama T, Matsuyama M, Funao K, et al. Benefical effect of neutrophil elastase inhibitor on renal warm ischemia-reperfusion injury in the rat. Transplant Proc. 2006;38(7):2201–2202. doi:10.1016/j.transproceed.2006.06.094
16. Yardeni T, Eckhaus M, Morris H, et al. Retro-orbital injections in mice. Lab Anim NY. 2011;40(5):155–160. doi:10.1038/laban0511-155
17. Gao S, Zhu Y, Li H, et al. Remote ischemic postconditioning protects against renal ischemia/reperfusion injury by activation of T-LAK-cell-originated protein kinase (TOPK)/PTEN/Akt signaling pathway mediated anti-oxidation and anti-inflammation. Int Immunopharmacol. 2016;38:395–401. doi:10.1016/j.intimp.2016.06.020
18. Fu Y, Tang C, Cai J, et al. Rodent models of AKI-CKD transition. Am J Physiol Renal Physiol. 2018;315(4):F1098–f1106. doi:10.1152/ajprenal.00199.2018
19. Togo S, Matsuo K, Ishibe A, et al. Usefulness of a selective neutrophil elastase inhibitor (sivelestat) in septic ARDS patients after gastrointestinal surgery. Hepatogastroenterology. 2008;55(84):967–973.
20. Champagne B, Tremblay P, Cantin A, et al. Proteolytic cleavage of ICAM-1 by human neutrophil elastase. J Immunol. 1998;161(11):6398–6405. doi:10.4049/jimmunol.161.11.6398
21. Colom B, Bodkin J, Beyrau M, et al. Leukotriene B4-neutrophil elastase axis drives neutrophil reverse transendothelial cell migration in vivo. Immunity. 2015;42(6):1075–1086. doi:10.1016/j.immuni.2015.05.010
22. Undefined U, Undefined U, Undefined U, et al. Beneficial effect of neutrophil elastase inhibitor on anti-Thy1.1 nephritis in rats. Nephrology. 2008;2008:13.
23. Yang J, Liu H, Han S, et al. Melatonin pretreatment alleviates renal ischemia-reperfusion injury by promoting autophagic flux via TLR4/MyD88/MEK/ERK/mTORC1 signaling. FASEB J. 2020;34(9):12324–12337. doi:10.1096/fj.202001252R
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Malnutrition, Inflammatory Biomarkers, and Stress-Induced Hyperglycemia on the Glomerular Filtration Rate in Renal Dysfunction
Jang W, Fujii N, Fujii T, Choi JW
International Journal of General Medicine 2025, 18:4481-4494
Published Date: 14 August 2025