Back to Journals » OncoTargets and Therapy » Volume 9
Single sternal metastasis due to malignant melanoma with unexpected long-term survival: a case report
Authors gogakos A, paliouras D, Asteriou C, Rallis T, Lazopoulos A, Chatzinikolaou F, Zissimopoulos A, Tsavlis D, Tsirgogianni K, Zarogoulidis K, Porpodis K, Tsakiridis K, pitsiou G, kioumis I, Karapantzos I, Karapantzou C, Sachpekidis N, Zarogoulidis P, Barbetakis N
Received 4 September 2015
Accepted for publication 19 November 2015
Published 18 January 2016 Volume 2016:9 Pages 321—323
DOI https://doi.org/10.2147/OTT.S95723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Daniele Santini
Apostolos S Gogakos,1 Dimitrios Paliouras,1 Christos Asteriou,1 Thomas Rallis,1 Achilleas Lazopoulos,1 Fotios Chatzinikolaou,2 Athanassios Zissimopoulos,3 Drosos Tsavlis,4 Katerina Tsirgogianni,4 Konstantinos Zarogoulidis,4 Konstantinos Porpodis,4 Kosmas Tsakiridis,5 Georgia Pitsiou,4 Ioannis Kioumis,4 Ilias Karapantzos,6 Chrysanthi Karapantzou,6 Nikos Sachpekidis,5 Paul Zarogoulidis,4 Nikolaos Barbetakis1
1Thoracic Surgery Department, 2Department of Pathology, Theagenio Cancer Hospital, Thessaloniki, 3Nuclear Medicine Department, University General Hospital of Alexandroupolis, Democritus University of Thrace, Alexandroupolis, 4Pulmonary Department – Oncology Unit, “G. Papanikolaou” General Hospital, Aristotle University of Thessaloniki, 5Cardiothoracic Surgery Department, 6Ear, Nose and Throat Department, “Saint Luke” Private Hospital, Panorama, Thessaloniki, Greece
Abstract: Metastases from melanoma have a very poor prognosis for the patient. Single metastatic lesions in the sternum due to melanoma are extremely rare. A rare case of a presternal mass in a 56-year-old patient who had undergone excision for malignant melanoma is presented. Review of the patient’s history and surgical resection of a single metastatic soft tissue lesion offer the best chance of long-term survival.
Keywords: melanoma, metastasis, chest wall, sternum
Introduction
Metastases from melanoma have a very poor prognosis for the patient. Soft tissue masses are quite hard to distinguish if they are secondary or primary lesions in a patient with a history of melanoma. In this case report, a 56-year-old male with a history of surgically removed malignant melanoma presented with a presternal lesion that proved to be metastasis from the primary site.
Case presentation
A 56-year-old male presented with a lesion in the right presternal space, growing progressively in size within 3 months. Apart from the mass, no symptoms or discomforts were present. The patient had undergone resection for malignant melanoma of the left tibia 4 years ago, rated Grade IV according to Clark, with 3 mm thickness according to Breslow.1 Sentinel lymph node dissection was negative for metastasis. Microscopic report indicated nevoid melanoma with tumor infiltrating lymphocytes “non-brisk” and a mitotic rate at 0–11 mm2. No ulceration or microsatellitosis was reported. Resection margin was free of neoplastic tissue. Two years later, the patient underwent a second resection for two new lesions at the left tibia, which turned out to be metastases of the original melanoma. Immunohistochemistry was positive for Melan A, S-100 protein, vimentin, and HMB45, while it was negative for PanCK and the epithelial membrane antigen (EMA).
Clinical examination upon admission demonstrated a swelling at the right presternal space, adjacent to the manubrium. On palpation, the lesion was hard and immobile, and there was no tenderness or pain of the sternum or the adjacent ribs. On percussion, there were no pathological findings. No lymphadenopathy was present and the findings from the examination of other organs and systems were normal. He was not under any medication. A plain chest radiograph and posterior–anterior and lateral views showed a lesion at the right side of the manubrium, at the height of sixth intercostals space. Findings from the lungs, the pleura, and the hilum lymph nodes were normal. Laboratory findings of the patient were within normal limits, except a slightly elevated serum calcium rate (10.26 mg/dL). A chest computed tomography (CT) demonstrated thickness of the pleura anteriorly, at the right side, near the heart (Figure 1). The patient underwent biopsy of the lesion, which was conclusive for a metastatic melanoma.
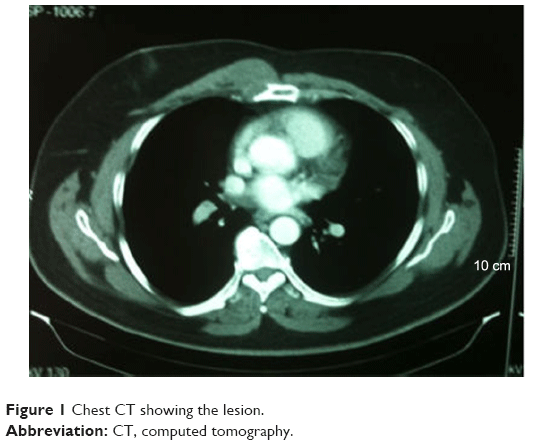 | Figure 1 Chest CT showing the lesion. |
Staging was completed with brain, abdomen, and a new thorax computed tomography scan prior to surgery, which showed no new findings. Surgical management required a median sternotomy with an extension to the right thoracic wall. The tumor was excised en-bloc with part of the manubrium and parts of the ribs and costochondral joints adjacent to it (fifth, sixth, seventh) (Figure 2A). The defect was covered with a mesh and the wound was closed in layers over two chest tubes (one in the mediastinum and the other in the right pleural cavity) connected to a thoracic drainage device (Bülau) (Figure 2B).
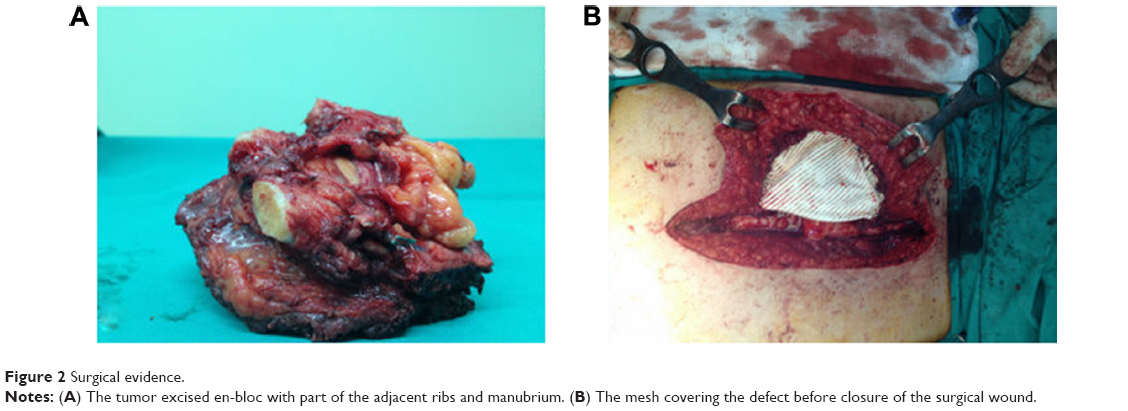 | Figure 2 Surgical evidence. |
The patient was hospitalized in our ICU for the first 24 hours post-surgery and was fully conscious. Three days post-surgery, the patient presented with pneumothorax at the right side, which was treated with placement of a new chest tube. He was discharged 14 days later after the removal of all tubes. Pathology was consistent with malignant melanoma, which infiltrated the muscles of the thoracic wall and sternum. Immunohistochemistry was positive for Melan A, S-100 protein, and HMB45, while it was negative for PanCK, CK-7, CK-20, TTF-1 and epithelial membrane antigen. The surgical margins were free of neoplastic tissue. During his follow-up 2 weeks later, the wound had healed well and the patient had no symptoms (Figure 3). Four years later, the patient was free of both local and distant recurrence.
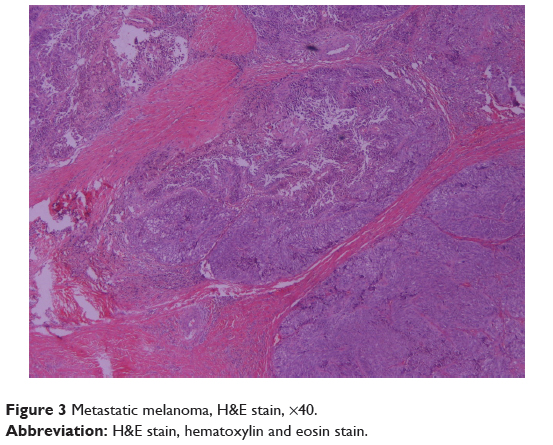 | Figure 3 Metastatic melanoma, H&E stain, ×40. |
Discussion
Metastatic melanoma has a very poor prognosis, with a median survival of only 6–8 months.2 Today, the use of newer and more effective therapeutic regimens help in the early detection of metastatic melanoma.3
In this case report, a 56-year-old male with a history of surgically removed malignant melanoma was presented with a presternal lesion that proved to be a metastasis from the primary site. It is quite common for the metastases of cutaneous malignant melanoma of ordinary type to resemble various types of soft tissue sarcoma. However, thorough immunohistological analysis should be performed to detect the presence of melanin, melanosomes, S-100 protein, Melan A, and HMB45 in order to categorize such tumors as melanoma metastases rather than soft tissue sarcomas.4–7
This case study emphasizes the rarity of such occurrence, with a single soft tissue metastasis from malignant melanoma. Although prognosis in such cases is poor, review of the literature indicates that surgical removal of a single metastatic lesion results in a better survival rate compared to other therapeutic approaches, such as immunotherapy or radiation.4,5
Based on this study, we concluded that patients with oligometastatic disease do benefit if the lesions are surgically removed. Preoperative evaluation of the number of lesions though remains crucial. A careful review of the patient’s history, along with early diagnosis and radical surgery, is essential for a favorable outcome, offering the best chance of long-term survival.
Acknowledgment
We thank the patient who provided written informed consent to publish this paper and the accompanying images. A copy of the written consent is available for review by the Editor-in-chief of this journal. Ethical approval for this study was obtained from the review board of the Theagenio Cancer Hospital.
Disclosure
The authors declare no conflict of interest.
References
Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of 17,600 melanoma patients: Validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001; 19(16):3622–3634. | ||
Tafra L, Dale PS, Wanek LA, Ramming KP, Morton DL. Resection and adjuvant immunotherapy for melanoma metastatic to the lung and thorax. J Thorac Cardiovasc Surg. 1995;110(1):119–128. | ||
Chen JT, Dahmash NS, Ravin CE, et al. Metastatic melanoma in the thorax: report of 130 patients. Am J Roentgenol. 1981;137(2):293–298. | ||
Barth A, Wanek LA, Morton DL. Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg. 1995;181:193–201. | ||
Fletcher WS, Pommier RF, Lum S, et al. Surgical treatment of metastatic melanoma. Am J Surg. 1998;175:413–417. | ||
Dewan M, Malatani TS, Ansari MA. Lessons to be learned: a case study approach. Malignant melanoma of soft tissue. J R Soc Promot Health. 2005;125(1):42–46. | ||
Lodding P, Kindblom LG, Angervall L. Metastases of malignant melanoma simulating soft tissue sarcoma. A clinico-pathological, light- and electron microscopic and immunohistochemical study of 21 cases. Virchows Arch A Pathol Anat Histopathol. 1990;417(5):377–388. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.