Back to Journals » Journal of Pain Research » Volume 12
Single shot ultrasound-guided thoracic paravertebral block for opioid-free radical mastectomy: a prospective observational study
Authors Santonastaso DP ![]() , de Chiara A
, de Chiara A ![]() , Russo E, Musetti G
, Russo E, Musetti G ![]() , Lucchi L, Sibilio A, Maltoni R
, Lucchi L, Sibilio A, Maltoni R ![]() , Gamberini E
, Gamberini E ![]() , Fusari M, Agnoletti V
, Fusari M, Agnoletti V
Received 11 April 2019
Accepted for publication 6 August 2019
Published 11 September 2019 Volume 2019:12 Pages 2701—2708
DOI https://doi.org/10.2147/JPR.S211944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Domenico P Santonastaso,1 Annabella de Chiara,1 Emanuele Russo,1 Giovanni Musetti,1 Leonardo Lucchi,2 Andrea Sibilio,3 Roberta Maltoni,4 Emiliano Gamberini,1 Maurizio Fusari,5 Vanni Agnoletti1
1Anesthesia and Intensive Care Unit, AUSL Romagna, M. Bufalini Hospital, Cesena 47521, Italy; 2Day Surgery – Breast Unit, AUSL Romagna, M. Bufalini Hospital, Cesena 47521, Italy; 3General Surgery Unit, AUSL Romagna, Santa Maria delle Croci Hospital, Ravenna 48121, Italy; 4Breast Cancer Unit, Department of Medical Oncology, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS, Meldola 47014, Italy; 5Anesthesia and Intensive Care Unit, AUSL Romagna, Santa Maria delle Croci Hospital, Ravenna 48121, Italy
Correspondence: Domenico P Santonastaso
Anesthesia and Intensive Care Unit, AUSL Romagna, M. Bufalini Hospital, Viale Ghirotti 286, Cesena, FC 47521, Italy
Tel +39 349 258 5491
Fax +39 54 735 2813
Email [email protected]
Background: General anesthesia (GA) is the most commonly used anesthesiological technique for radical mastectomy operations and can be associated with loco-regional anesthesia techniques. The aim of our study, carried out on 51 patients, was to assess the effectiveness of thoracic paravertebral block (TPVB) associated with GA, or as a sole anesthesiological technique for postoperative pain control and for the reduction of intra and postoperative opioids consumption.
Materials and methods: Fifty-one patients with neoplastic breast disease and elected as candidates for radical mastectomy were included in the study. The primary outcomes for this study were intra and postoperative opioid consumption and postoperative pain intensity. In 37 patients, TPVB was associated with GA while in 14 patients it was used as the sole anesthesiological technique. Data are reported as mean with standard deviation median with interquartile range, number, and percentage, depending on the underlying distribution.
Results: We did not use intra or postoperative opioids for any patient and the Numeric Rate Scale, assessed at time 0, at the end of the surgery, and 2, 6, 12, and 24 hrs after surgery, was >3 in seven patients only.
Conclusions: This study aims to show how TPVB can be used to carry out radical mastectomy procedures so that intra and postoperative opioids use can be avoided. In our study, TPVB was used in total mastectomy procedures in association with GA or as the sole anesthesiological technique, without the intra and postoperative use of opioids and with a significant reduction of local anesthetic dosages compared to those reported in the existing literature.
Keywords: thoracic paravertebral block, mastectomy, opioids free anesthesia, awake breast surgery
Introduction
Breast cancer is still the most common cancer among women and many affected women require breast surgery to remove the primary tumor as well as axillary staging or dissection.1 Approximately 40% of the women who undergo breast surgery, quadrantectomies and mastectomies, describe considerable postoperative pain (>5 on the Visual Analogue Scale) which is not always effectively controlled by standard postoperative therapies.2 Furthermore, acute postoperative pain is an important risk factor for the development of persistent chronic postoperative pain in women after breast surgery3 and occurs in almost 50% of the patients after breast surgery.4 Therefore, a therapeutic approach to pain after breast cancer surgery is necessary.
General anesthesia (GA) is the most commonly used anesthesiological technique for radical mastectomy operations and can be associated with loco-regional anesthesia techniques. However, the side-effects and complications of GA, such as nausea, vomiting, and considerable postoperative pain, increase morbidity for most patients undergoing breast surgery.5 Over the last years, there has been an increase of research into loco-regional anesthesia techniques for use alongside or, in some cases, for replacement of GA, in breast surgery. Such techniques may reduce postoperative complications, such as nausea and vomiting (postoperative nausea and vomiting, PONV) and guarantee optimal postoperative pain control, by minimizing opioid use. Two meta-analyses of randomized controlled trials demonstrated that thoracic paravertebral block (TPVB) combined with GA or monitored anesthesia care has several advantages, such as better postoperative pain control, lower incidence of PONV, shorter recovery time, and higher patient satisfaction, compared to GA alone in breast surgery.6,7 Few studies have been published describing surgery without GA for breast cancer but all included the use of intra-operative opioids for sedation.8,9
In our study, TPVB was used in 14 cases as the only anesthesiological technique and in all 51 cases enabled us to avoid the use of opioids. Furthermore, TPVB is prophylactically effective in reducing the frequency and intensity of chronic postoperative pain10,11 and the incidence of cancer recurrence after breast cancer surgery.12 The aim of our study, which was carried out on 51 patients who underwent radical mastectomy, with or without axillary dissection, was to assess the effectiveness of TPVB associated with GA, or as a sole anesthesiological technique, in relation to opioid consumption, in intra and postoperative pain control, for the prevention of postoperative complications such as nausea and vomiting as well as of chronic pain 6 months after surgery.
Materials and methods
A prospective observational study was designed. The study was approved by the ethics committee of the AUSL (local health authority) of Romagna (ref. 7655/2016 I.5/212) and IRST and all data management adhered to the Declaration of Helsinki.13
Fifty-one patients with neoplastic breast disease, who simultaneously sought treatment at the M. Bufalini Hospital, Cesena, were included in the study and were elected as candidates for radical mastectomy, with or without axillary dissection, in a period spanning from July 2016 to January 2017, subject to their signing of informed consent for the study and the consent form for the processing of their personal data in anonymous form. Patients included in the study were aged from 18 to 92 years and presented an ASA risk ranging from I to IV, with no contra-indications for the execution of TPVB. Patients with allergies and/or contraindications for the administration of drugs used in the study were excluded from the study, as well as patients who presented chronic opioid use for therapeutic purposes, patients with coagulopathies and/or who used antiaggregant or anticoagulant drugs, with infections and lesions at puncture site or with a BMI ≥40.
The primary outcomes for this study were:
- Intra and postoperative opioid consumption.
- Postoperative pain intensity expressed as Numeric Rate Scale (NRS).
The secondary outcomes were:
- Patients who required rescue analgesic (nonsteroidal anti-inflammatory drugs – NSAIDs)
- Patients with PONV
- Patients with TPVB technique failure
- Days of hospitalization
- Patients with adverse events (accidental vascular puncture, accidental pneumothorax, nerve damage, and Horner’s/Harlequin’s syndrome).
- Postoperative chronic pain assessment (6 months).
All patients were admitted to hospital in the morning on the day of surgery and received premedication with midazolam 3 mg i.m. an hour before the operation, if requested by the patient. In all cases, the same two anesthesiologists performed the block and the same surgeon performed the surgery.
In the pre-anesthesia holding area, patients received routine monitoring (pulse oximeter, noninvasive blood pressure cuff, and electrocardiogram) and Bispectral Index System (BIS, Covidien Medtronic, Minneapolis, MN, USA) monitoring and were placed in the lateral position with the site of surgical interest uppermost. Ultrasound guidance (SonoSite M-Turbo, SonoSite Inc., Bothell, WA), with the transducer positioned into a longitudinal orientation to obtain a parasagittal view, was used to visualize the transverse process as a hyperechoic structure, with acoustic shadowing below it. The costotransverse ligament and the pleura were visualized as hyperechoic structures, and the paravertebral space appeared as a wedge-shaped hypoechoic layer between these structures. The skin and subcutaneous tissue of the puncture area were anesthetized with lidocaine (20 mg mL−1) 2 mL. The puncture area and the ultrasound probe were prepared in a sterile manner and the puncture was performed with a 22-G × 50-mm needle (Echoplex+, Vygon, Ecouen-France), using the “out-of-plane” technique. Hydrolocation using saline 0.9% was performed to help to show needle tip position. The patients received a ultrasound-guided TPVB at two thoracic (T) levels (T2–T3 and T4–T5 or T3–T4 and T5–T6) and for each level, 6 mL of Ropivacaine 0.7% was injected 40 mins before surgery. The spread of local anesthetic in the paravertebral space and a concomitant anterior movement of the parietal pleura were observed using real-time image guidance. (Figure 1)
 |
Figure 1 Ultrasound view of paravertebral space before (A) and after (B) administration of thoracic paravertebral block with 6 mL of ropivacaine 0.7%. Abbreviations: TP, transverse process; PP, parietal pleura. |
Forty minutes after TPVB administration, sensory blockage was assessed by cold sensation with an alcohol-soaked sponge and pin prick testing using a 22-G short bevel needle. The blocked area was tested from the T2 dermatome at the anterior axillary line in a cranial and caudal direction, and each dermatome on the blocked side was compared to the contralateral one. The test showed the diffusion of local anesthetic from T2 level up to T7 level over the posterior and anterolateral thorax.
In 37 patients, anesthesia was induced with intravenous (IV) propofol 2 mg kg−1 and Rocuronium 0.6 mg kg−1 and I-Gel (Intersurgical, Berkshire, UK) was inserted according to the manufacturer’s instruction. Anesthesia was maintained by continuous IV infusion of propofol (6–9 mg kg−1 h−1) and the sedation level was monitored using BIS. Fentanyl 1 μg kg−1 in bolus doses was administered intravenously if mean blood pressure or heart rate exceeded 20% of the preoperative value. In 14 patients, for whom GA would have constituted a very high anesthesiological risk or required postoperative hospitalization in the intensive care unit, TPVB was used as the sole anesthesiological technique, associated with sedation. In these patients, IV propofol at 1–2 mg kg−1 h−1 was administered to target a BIS between 75 and 90 and an IV bolus of 1 μg kg−1 Fentanyl was administered intra-operatively if patients reported any discomfort. In patients requiring an axillary lymph node dissection, top-up local infiltration analgesia into the surgical field was performed by the surgeon using Lidocaine (20 mg mL−1) 6 mL. Ephedrine was administered when mean arterial pressure was <60 mmHg and atropine was administered when Heart Rate was 40–50 beats/min and all patients were administered 2 g of Cefazolin half an hour before the start of surgery. No prophylactic antiemetics were administered.
Surgery was completed within a time range of 70–110 mins. Acetaminophen 1 g IV was administered 30 mins before the end of the surgery, and then every 8 hrs. Postoperative pain was assessed using NRS, at time 0, at the end of the surgery, by the anesthetist and 2, 6, 12, and 24 hrs after surgery by ward nurses. Wherever pain exceeded 3 according to the NRS scale, 30 mg of Ketorolac was administered intravenously for a maximum of three times a day. The first-line treatment of PONV consisted of IV ondansetron 4 mg twice a day as needed and, if this proved ineffective, second-line therapy consisted of IV metoclopramide 10 mg as needed.
The quantity of opioids administered postoperatively, requests for rescue doses of NSAIDs, along with the presence and number of nausea and vomiting episodes, were all assessed. Lastly, patients were requested to fill out a pre-printed sheet on their judgment of the anesthesiological procedure, in which they could express a value from 0 to 5, where 0 indicates “entirely dissatisfied” and 5 indicates “very satisfied”. The patient was then discharged when deemed safe according to the Italian version of the Post Anesthesia Discharge Scoring System. Lastly, total days of hospitalization were also recorded.
After 6 months, patients received a telephone call to ascertain the presence of chronic pain during rest and in motion. Chronic postsurgical pain was evaluated with a NRS ranging from 0 (no pain) to 10 (worst pain imaginable). They were also asked to evaluate pain interference with: sleep, work activity, mood tone, possibility of entertainment.
Statistical analysis
Data are reported as mean with standard deviation (std. dev.), median with interquartile range (IQR), number and percentage, depending on underlying distribution.
Results
Fifty-one patients were included in the study and no patient was excluded for any reason.
Average patient age was 70.7 years (standard deviation was 14, 7, median was 74, IQR 22) and average BMI was 24.7 (standard deviation 4, 3, with a median of 23.6, IQR 4.8). In addition to the mastectomy, 11 patients (21.5%) also underwent a lymphadenectomy and 7 (13.7%) the positioning of a tissue expander (Table 1). ASA assessment was as follows: 6 ASA 1 patients (11.8%), 20 ASA 2 patients (39.2%), 24 ASA 3 patients (47%), and 1 ASA 4 patients (1.9%) (Table 1). GA associated with TPVB was carried out on 37 patients (72.5%) and in 14 patients we used TPVB as the sole anesthesiological technique (27.5%) (Table 1). During surgery opioid use has not been required for any patients and there were no cases of sympathetic block. No postoperative opioid was used for any patient. Ten patients (19,6%) required top-up local infiltration analgesia into the surgical field, with Lidocaine (20 mg mL−1) 3 mL, for axillary lymph node dissection. TPVB was carried out at two levels in all patients, at T2-T3/T4-T5 levels or T3-T4/T5-T6 levels, based on the best ultrasound image we were able to obtain Table 1.
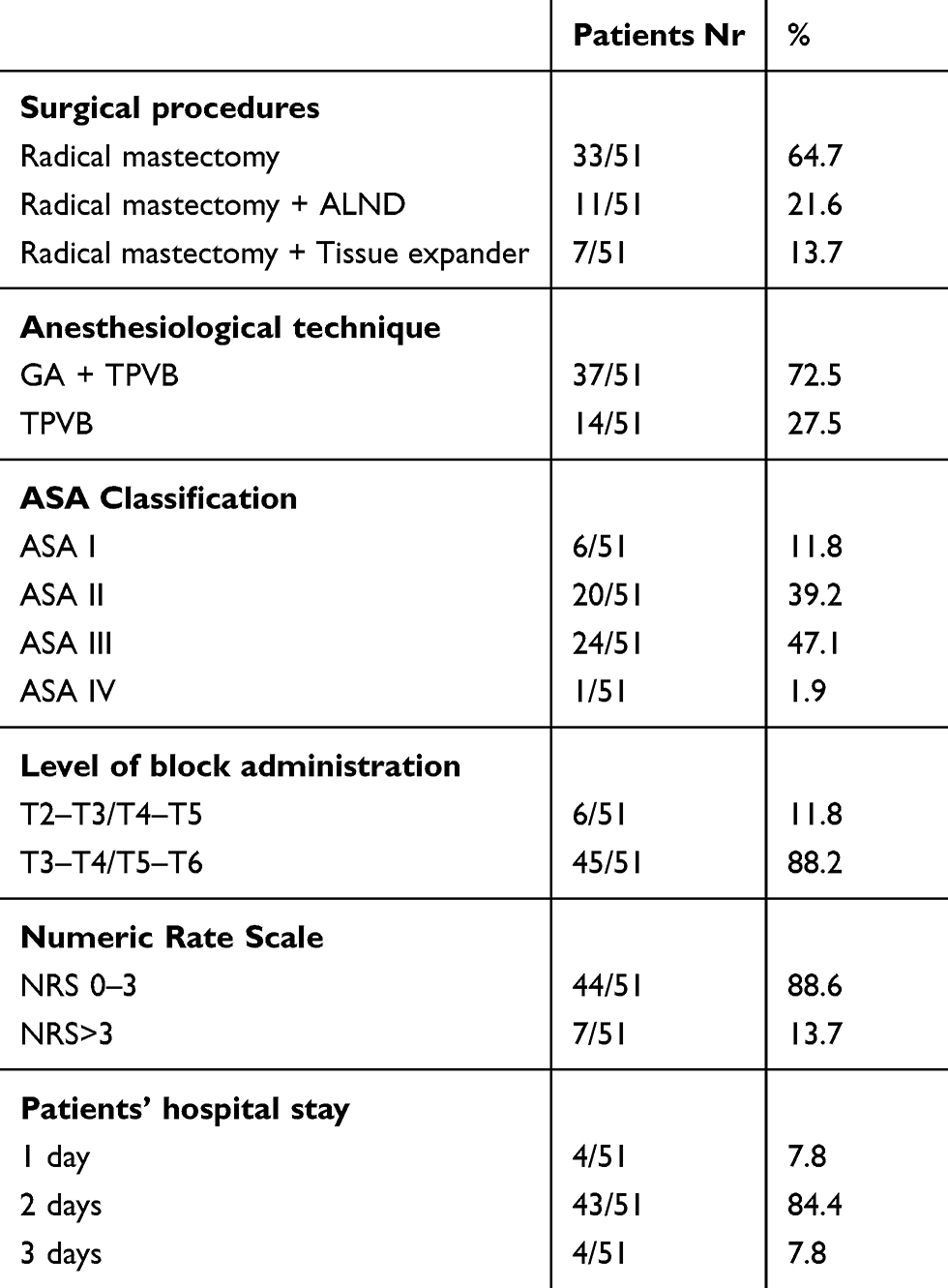 |
Table 1 Characteristics of patients, surgical procedures and anesthesiological technique |
The NRS, assessed at time (Tm) 0, and 2, 6, 12, and 24 hrs after the end of the surgery, was >3 in seven patients only (13, 7%) (Figure 2). Median NRS was 1 (iqr 2) at Tm 0, 1 (iqr 1) at 2 hrs, 1 (iqr 0) at 6 hrs, 1 (iqr 1) at 12 hrs, 1 (iqr 1) at 24 hrs. Seven patients (13.7%) who underwent a mastectomy with axillary dissection and tissue expander positioning, requested a supplementary dose of analgesic (30 mg Ketorolac) during the 24 hrs after surgery: four patients required supplementary dose of analgesic at Tm 2, two patients at Tm 6, and one patient at Tm 12 (Figure 3). Only a single episode (2%) of postoperative nausea was observed and resolved itself without the use of antiemetic drugs. No episodes of vomiting occurred. Average hospital stay was 1.98 days (std. dev. 0.3, median 2, IQR 0) (Table 1).
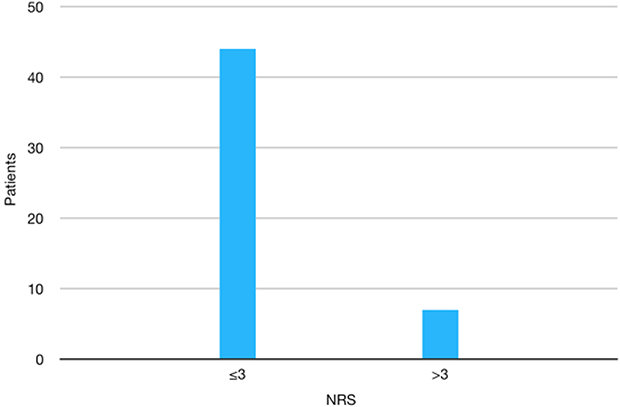 |
Figure 2 Number of patients with NRS ≤3 and >3, assessed at time 0, and 2, 6, 12, and 24 hrs after the end of the surgery. Abbreviation: NRS, Numeric Rate Scale. |
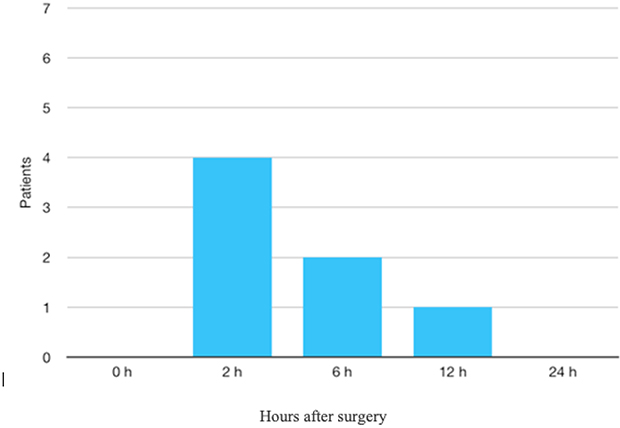 |
Figure 3 Time to request rescue dose in patients with NRS>3. Abbreviation: NRS, Numeric Rate Scale. |
All patients expressed a satisfaction level of 5 with the anesthesiological procedure (very satisfied), according to the scale mentioned in the materials and methods paragraph here above. No failures or complications occurred in the execution of this technique. None of the mastectomy patients reported any chronic pain at 6 months from surgery.
Discussion
This study aims to show how TPVB can be used, associated with GA or as a sole anesthesiological technique, to carry out radical mastectomy procedures, with or without axillary dissection, so that intra and postoperative opioid use can be avoided, while also ensuring perfect control of postoperative acute pain as well as any consequent onset of chronic pain.
Patients enrolled in our study received an ultrasound-guided TPVB, using the out-of-plane technique. The use of the ultrasound-guided technique enabled us to reduce the risk of complications, especially of pneumothorax and vascular puncture, indeed neither was observed in our study.14,15 Although postoperative chest X-rays looking for pneumothorax were not routinely performed, there were no patients in whom respiratory compromise was evident postoperatively. Therefore, no chest X-Rays were performed postoperatively. There are no significant differences in terms of safety and successful outcome in anesthesiological procedure using in-plane or out-of plane ultrasound-guided technique; our choice to use the out-of-plane technique was dictated by the fact our best experiences involved the use of this latter technique.16
As described in the literature, TPVB can be carried out on a single or several levels.17 We found it would be most appropriate to administer the block on two levels and exploit both cranial and caudal local anesthetic spread, to guarantee optimal anesthetic coverage.18,19
The total Ropivacaine dosage of 12 mL at 0.7%, divided equally between two selected levels, is lower than doses described in most studies found in the literature.8,20 In their work, Uppal et al,17 describe TPVB carried out on a single level with the administration of 25 mL of ropivacaine 0.5%, or on more than one level using 5 mL of ropivacaine 0.5% per level. Kulhari et al,20 also described block execution on a single level with the administration of 25 mL of ropivacaine 0.5%. Forty minutes after the execution of TPVB, all 51 patients presented anesthetic coverage from T2 to T7 levels.
It is important to note that in five patients there were difficulties in needle penetration of the paravertebral space, at a depth of 4.5 cm, and we administered local anesthetic posteriorly to superior costotransverse ligament (SCTL).21 We observed pleural displacement with the needle tip and local anesthetic injection clearly posterior to the SCTL. Onset time and anesthetic coverage of the block were overlapped with the TPVB carried out in a conventional manner.
Lee et al, showed that both AG and postoperative opioid administration increase PONV.22 The avoidance of opioids, thanks to the execution of TPVB, enabled a reduction in the incidence of PONV, which together with postoperative pain, constitutes the most common cause of prolonged hospitalization after breast surgery. PONV prophylaxis was not administered to any of the patients, not even to those with an APFEL score >2.
We also assessed the onset of chronic pain in patients, 6 months after surgery. Persistent postoperative pain, defined as the presence of pain 3 months after surgery, is quite common in breast surgery, indeed 25% to 53% of the patients experience symptoms.23 Persistent pain negatively impacts patients’ quality of life and constitutes a significant economic burden on the health care system.24 Several studies support the notion that TPVB effectively decreases pain scores in the early postoperative period and increases patient satisfaction;6,25,26 furthermore TPVB may also decrease chronic pain.27,28 None of the patients included in our study developed chronic pain 6 months after surgery. Ten patients, who implanted a tissue expander, reported a sensation of tension in the area surrounding the tissue expander, which in any case did not limit their normal activities in any way. Furthermore, these patients reported a pain level that never exceeded 2 on the NRS scale.
As highlighted above, in 14 of the 51 patients, for whom general anesthesia would have constituted a very high anesthesiological risk or required postoperative hospitalization in intensive care unit, TPVB was used as the sole anesthesiological technique, associated with sedation. Few studies have been published describing GA-free surgery for breast cancer. One reports a case series using TPVB and sedation for breast surgery.8 The authors performed either single or multilevel injections, the range LA volume used was 20–30 mL Bupivacaine 0.5% or bupivacaine 0.5% with lignocaine 2% (50:50) and Clonidine 150 mcg, with the use of propofol or remifentanil TCI for sedation with prilocaine top-ups administered by the surgical team as needed. Another study compared GA to monitored anesthesia care (sedation using propofol and remifentanil TCI) coupled with multilevel TPVB and intra-operative surgical local anesthetic infiltration for breast cancer surgery.9 Deep levels of sedation were targeted (BIS 50–70) and respiratory depression was observed in some patients, including one patient who required airway instrumentation. In contrast to these studies, and similar to our previous experience,29 all our patients received double-level TPVB with a total dosage of 12 mL Ropivacaine 0.7%, no intra-operative opioid infusion and only propofol sedation with BIS between 75 and 90.
We have demonstrated that it is feasible to perform major breast surgery with double injection TPVB and under sedation. This is particularly relevant in the context of breast cancer surgery, as the majority of these patients are elderly and may have comorbidities, making GA either undesirable or unsafe.
The total lack of complications and/or collateral postoperative effects, associated with optimal pain control, guaranteed excellent comfort for patients. Indeed, already 3 hrs after surgery patients were able to eat and move freely and were rapidly discharged. Surgeons were extremely satisfied with the use of TPVB due to excellent pain control and the reduction of adverse effects linked to anesthesia, thus facilitating postoperative patient management.
TPVB was originally developed for thoracic surgery and has also been extensively used in breast surgery with numerous advantages for patients. Regional anesthesia could reduce the incidence of cancer recurrence by attenuating the neuroendocrine stress response during surgery and reducing opioid requirements, thus reducing their immunosuppressive effects and providing antitumor and anti-inflammatory effects directly through the systemic local anesthetic action.30,31 An increasing number of laboratory and animal studies suggest that opioids cause immunosuppression and stimulate tumor cells in vitro. Buckley et al.32 found that the serum of women with breast cancer who were randomized to receive propofol-paravertebral anesthesia for primary breast cancer surgery maintained a healthy activity of anticancer natural killer cells compared to the serum of women undergoing an anesthetic technique with sevoflurane-opioid. Several studies have shown that patients who receive TPVB experience reduced levels of postoperative pain, a decreased need for opioids after surgery, therefore suffer less nausea and vomiting, which ultimately results in shorter hospital stays, compared to patients who receive GA alone.
Conclusion
In our study, TPVB was used in total mastectomy procedures in association with GA or, in a few cases, as the sole anesthesiological technique, without the intra or postoperative use of opioids and with a significant reduction of local anesthetic dosages compared to those reported in the existing literature. Our experience with TPVB in radical mastectomies has convinced us to use this technique routinely for this type of procedure insofar as it provides maximum patient satisfaction. Future trials are necessary in order to compare TPVB with other loco-regional anesthesia techniques used in breast surgery, such as PECS1, PECS2, and the Erector spinae plane block.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work. In addition, Domenico P Santonastaso and Annabella de Chiara performed the anesthesiological procedures and followed the patients in the postoperative period, Emanuele Russo and Emiliano Gamberini followed the patients in the postoperative period, and Leonardo Lucchi and Andrea Sibilio performed surgical procedures.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tyczynski JE, Bray F, Parkin DM. Breast cancer in Europe - ENCR cancer fact sheet. Eur Network Cancer Registries. 2002;2:1–4.
2. Cheng GS, Ilfeld BM. A review of postoperative analgesia for breast cancer surgery. Pain Manag. 2016;6(6):603–618. doi:10.2217/pmt-2015-0008
3. Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 2011;12:725–746. doi:10.1016/j.jpain.2010.12.005
4. Okamoto A, Yamasaki M, Yokota I, et al. Classification of acute pain trajectory after breast cancer surgery identifies patients at risk for persistent pain: a prospective observational study. J Pain Res. 2018;11:2197–2206. doi:10.2147/JPR.S171680
5. Jokela RM, Kangas-Saarela TA, Valanne JV, Koivuranta MK, Ranta PO, Alahuhta SM. Postoperative nausea and vomiting after sevoflurane with or without ondansetron compared with propofol in female patients undergoing breast surgery. Anesth Analg. 2000;91:1062–1065.
6. Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105:842–852. doi:10.1093/bja/aeq198
7. Tahiri Y, Tran de QH, Bouteaud J, et al. General anaesthesia versus thoracic paravertebral block for breast surgery: a meta- analysis. J Plast Reconstr Aesthet Surg. 2011;64:1261–1269. doi:10.1016/j.bjps.2011.03.025
8. Simpson J, Ariyarathenam A, Dunn J, Ford P. Breast surgery using thoracic paravertebral blockade and sedation alone. Anesthesiol Res Pract. 2014;2014:127467. doi:10.1155/2014/127467
9. Sato M, Shirakami G, Fukuda K. Comparison of general anesthesia and monitored anesthesia care in patients undergoing breast cancer surgery using a combination of ultrasound- guided thoracic paravertebral block and local infiltration anesthesia: a retrospective study. J Anesth. 2016;30:244–251. doi:10.1007/s00540-016-2183-4
10. Heesen M, Klimek M, Rossaint R, Imberger G, Straube S. Paravertebral block and persistent postoperative pain after breast surgery: meta-analysis and trial sequential analysis. Anaesthesia. 2016;71:1471–1481. doi:10.1111/anae.2016.71.issue-12
11. Woodworth GE, Ivie RMJ, Nelson SM, Walker CM, Maniker RB. Perioperative breast analgesia: a qualitative review of anatomy and regional techniques. Reg Anesth Pain Med. 2017;42(5):609–631. doi:10.1097/AAP.0000000000000641
12. Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. 2006;105:660–664. doi:10.1097/00000542-200610000-00008
13. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involv- ing human subjects. JAMA. 2013;310:2191–2194. doi:10.1001/jama.2013.281053
14. Pace MM
15. Naja Z, Lönnqvist PA. Somatic paravertebral nerve blockade. Incidence of failed block and complications. Anaesthesia. 2001;56:1184–1188. doi:10.1046/j.1365-2044.2001.02084-2.x
16. Krediet AC, Moayeri N, van Geffen GJ. Different approaches to ultrasound-guided thoracic paravertebral block: an illustrated review. Anesthesiology. 2015;123(2):459–474. doi:10.1097/ALN.0000000000000747
17. Uppal V, Sondekoppam RV, Sodhi P, Johnston D, Ganapathy S. Single-injection versus multiple-injection technique of ultrasound-guided paravertebral blocks: a randomized controlled study comparing deramtomal spread. RTeg Anesth Pain Med. 2017;42(5):575–581. doi:10.1097/AAP.0000000000000631
18. Santonastaso DP, de Chiara A, Rispoli M, Musetti G, Agnoletti V. Real-time view of anesthetic solution spread during an ultrasound-guided thoracic paravertebral block. Tumori. 2018;104:NP50–NP52. [Epub ahead of print]. doi:10.1177/0300891618763212
19. Agnoletti V, Piraccini E, Corso R, et al. Methylene blue diffusion after multilevel thoracic paravertebral blocks. J Cardiothorac Vasc Anesth. 2011;25(2):e5–e6. doi:10.1053/j.jvca.2010.07.023
20. Kulhari S, Bharti N, Bala I, Arora S, Singh G. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: a randomized controlled trial. Br J Anaesth. 2016;117(3):382–386. doi:10.1093/bja/aew223
21. Costache I, Sinclair J, Farrash FA, et al. Does paravertebral block require access to the paravertebral space? Anaesthesia. 2016;71(7):858–859. doi:10.1111/anae.13527
22. Lee YZ, Lee RQ, Thinn KK, Poon KH, Liu EH. How patients fare after anaesthesia for elective surgery: asurvey of postoperative nausea andvomiting, pain and confusion. Singapore Med J. 2015;56(1):40–46. doi:10.11622/smedj.2015008
23. Mejdahl MK, Andersen KG, Gärtner R, Kroman N, Kehlet H. Persistent pain and sensory disturbances after treatment for breast cancer: six year nationwide follow-up study. Br Med J. 2013;346:f1865–f1865. doi:10.1136/bmj.f1865
24. Wu J, Buggy D, Fleischmann E, et al. Thoracic paravertebral regional anesthesia improves analgesia after breast cancer surgery: a randomized controlled multicentre clinical trial. Can J Anaesth. 2015;62(3):241–251. doi:10.1007/s12630-015-0340-0
25. Terkawi AS, Tsang S, Sessler DI, et al. Improving analgesic efficacy and safety of thoracic paravertebral block for breast surgery: a mixed-effects meta-analysis. Pain Physician. 2015;18(5):E757–E780.
26. Thavaneswaran P, Rudkin GE, Cooter RD, Moyes DG, Perera CL, Maddern GJ. Brief reports: paravertebral block for anesthesia: a systematic review. Anesth Analg. 2010;110:1740–1744. doi:10.1213/ANE.0b013e3181da82c8
27. Hussain N, Shastri U, McCartney CJL, et al. Should thoracic paravertebral blocks be used to prevent chronic postsurgical pain after breast cancer surgery? A systematic analysis of evidence in light of IMMPACT recommendations. Pain. 2018;159(10):1955–1971. doi:10.1097/j.pain.0000000000001292
28. Andreae MH, Andreae DA. Regional anaesthesia to prevent chronic pain after surgery: a cochrane systematic review and meta-analysis. Br J Anaesth. 2013;111:711–720. doi:10.1093/bja/aet213
29. Santonastaso DP, de Chiara A, Piccioni F, Tognù A, Agnoletti V. Awake mastectomy under ultrasoundguided thoracic paravertebral block inelderly patients. J Clin Anesth. 2018;47:50–51. doi:10.1016/j.jclinane.2018.03.014
30. Kim R. Anesthetic technique and cancer recurrence in oncologic surgery: unraveling the puzzle. Cancer Metastasis Rev. 2017;36(1):159–177. doi:10.1007/s10555-016-9647-8
31. Votta-Velis EG, Piegeler T, Minshall RD, et al. Regional anaesthesia and cancer metastases: the implication of local anaesthetics. Acta Anaesthesiol Scand. 2013;57(10):1211–1229. doi:10.1111/aas.12210
32. Buckley A, McQuaid S, Johnson P, Buggy DJ. Effect of the anesthetic technique on the antitumor activity of natural serum killer cells of women undergoing breast cancer surgery: a pilot study. Br J Anesth. 2014;113(1):i56–i62. doi:10.1093/bja/aeu200
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.