Back to Journals » International Journal of General Medicine » Volume 14
Single-Port Access Endoscopic Thyroidectomy via Axillary Approach for the Benign Thyroid Tumor: New Aspects from Vietnam
Authors Phan HH, Nguyen TH, Vo HL ![]() , Le NT, Tran NL
, Le NT, Tran NL
Received 1 March 2021
Accepted for publication 21 April 2021
Published 14 May 2021 Volume 2021:14 Pages 1853—1864
DOI https://doi.org/10.2147/IJGM.S308807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Single-port Access Endoscopic Thyroidectomy via Axillary Approach" [ID 308807].
Views: 15617
Hoang-Hiep Phan,1 Thai-Hoang Nguyen,1,2 Hoang-Long Vo,3 Ngoc-Thanh Le,2,4 Ngoc-Luong Tran1
1High-Tech Medical Treatment, National Hospital of Endocrinology, Hanoi, Vietnam; 2School of Medicine and Pharmacy, Vietnam National University, Hanoi, Vietnam; 3Institute for Preventive Medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam; 4Cardiovascular Center, E Hospital, Hanoi, 100000, Vietnam
Correspondence: Hoang-Long Vo Email [email protected]
Background: This study aims to describe our new experience with single-port totally endoscopic thyroidectomy via the axillary approach in patients with unilateral thyroid benign tumors. In parallel with that, we also discuss here the challenges and novelty highlights we have confronted and solved and the details of our operative technique.
Methods: Between August 2018 and May 2020, the study involved 54 patients who underwent a single-port single-incision endoscopic thyroidectomy via the axillary approach for benign thyroid tumor at the National Hospital of Endocrinology (Hanoi, Vietnam). Surgical patient indications were in working age, goiter classification of grade 1 or grade 2, the thyroid with mononuclear or multinucleated, lesion diameter of less than 4 cm, unilateral thyroid benign lesion and no previous history of neck surgery or irradiation.
Results: No mortality was observed. Morbidities included transient voice change in 8 patients, swallowing disorders in 2 patients, transient skin paresthesia in 2 patients and wound hematoma in 2 patients. Mean amount of postoperative drainage was 70.2 mL, mean duration of postoperative drainage was 2.7 days, and mean postoperative hospital day was 6.6 days. Mean total operation time was 66.0 minutes and mean blood loss was 13.3 mL. Regarding medium-term follow-up outcomes following surgery, we recorded the hypothyroidism in 3 patients (5.6%) and the hypocalcemia in 1 case (1.8%). Most patients felt normal neck movement and sensation (79.6%), 3 patients were painful (5.6%) and 8 those were numb (14.8%). We saw the soft incision scar in 35 patients (64.8%), convex scar in 14 patients (25.9%), and hard scar in 5 patients (9.3%).
Conclusion: Single-port endoscopic thyroidectomy via axillary approach is a safe and feasible treatment option for removing benign thyroid tumor, delivering favorable surgical outcomes with ideal cosmetic effect and reduction in injury to the anterior neck tissue.
Keywords: endoscopic thyroidectomy, endoscopic surgery, thyroidectomy, single-incision surgery, one-port surgery
Introduction
For endoscopic thyroidectomy, with good evidence of its safety and feasibility for both benign and malignant thyroid tumors, endoscopic thyroidectomy via the axillary, anterior, and breast approaches has been introduced in many individual surgical institutions around the world. There seems to be little doubt that endoscopic surgery with improved and modified techniques will continue to evolve. In particular, single-port access laparoscopic surgery has recently emerged as a less-invasive alternative to conventional laparoscopy in many fields.1 In the literature, most reports related to single-port single-incision endoscopic thyroidectomy were evaluated in developed countries,2,3 and it still remained the inconsistency among previous studies in the selection of study variables from different institutions. To the best of our knowledge, in resource-scarce settings like Vietnam, this is the first time for the surgeons to report a cohort of consecutive patients with benign thyroid tumors who underwent single-port endoscopic thyroidectomy via the axillary approach. Hence, the aim of this study was to present our new experience with single-port totally endoscopic thyroidectomy in patients with unilateral thyroid benign tumors. We also discuss here the challenges we confronted and the details of our operative technique.
Methods
Study Design and Study Population
This study was a prospective observational study. The study population consisted of 54 patients who underwent a single-port single-incision endoscopic thyroidectomy via the axillary approach for benign thyroid tumor at the National Hospital of Endocrinology (Hanoi, Vietnam) from August 2018 to May 2020. Single-incision endoscopic thyroidectomy via the axillary approach was indicated for the patients (i) in working age (male <60 years and female <55 years), (ii) goiter classification of grade 1 or grade 2, (iii) the thyroid with mononuclear or multinucleated, (iv) lesion diameter of less than 4 cm, (v) unilateral thyroid benign lesion and (vi) no previous history of neck surgery or irradiation. All patients provided written informed consent to participate in all the procedures. For women patients, breast physical examination and an ultrasonographic evaluation were performed beforehand.
Surgical Technique (Supplementary Video)
All the procedures were performed by the same team. The patient was placed in a supine position with the neck slightly extended under general anesthesia. By placing a pillow under your shoulder, the arm on the side of the lesion was maximized to expose the widest armpit area (Figure 1).
 |
Figure 1 Positioning the patient for surgery. |
For the position of the surgeon and physician assistant, surgeon stands right next to the armpit with the lesion. The first physician assistant stood on the same side of the surgeon. The first physician assistant stood above the surgeon on the right side of the patient and below the surgeon on the right side of the patient. The second physician assistant was the opposite of the surgeon.
There were five phases in our operation. The first phase was placing trocar. After determining the skin incision in the armpit, we conducted a 3-cm skin incision along the skin crease of the axilla (Figure 2). A working space on the pectoralis major muscle and the subcutaneous tissue was dissected; then, the split was carried out in all directions to create a large enough cavity before placing the 3-cm one-port trocar (Figure 3). We maintained the insufflation using CO2 at 12 mmHg with flow rate of 6 L/min (Figure 4 and Figure 5). The second phase was forming the working space. The medial border of the sternocleidomastoid muscle was dissected from the strap muscle. We gradually separated toward the sternal pit and went the correct spongy layer, not passing through the mammary gland. The dissection area is usually above transverse to the thyroid cartilage and laterally to the outer border of the sternocleidomastoid muscle (Figure 6). The third phase was splitting the muscle to expose the thyroid gland. We separated the front border of the sternocleidomastoid muscle and omohyoid muscle (Figure 7). Then, we cut along sternothyfold muscle to enter the thyroid lobe (Figure 8). The fourth phase was evaluating the lesion and resecting the thyroid lobe. The lesion was assessed with the location, quantity, essence, and boundary. We freed the upper and lower extremities of the thyroid and separated the posterior part of the thyroid gland. From this step, we used the ultrasonic cutting knife in mode MIN = 3, MAX = 5, and the control pedal. Thyroid lobes were cut in order: the lower pole, the avascular space, the upper pole, the Berry’s ligament, and isthmus (Figure 9). The fifth phase was checking the lesion, retrieving the specimen and closing the trocar port. Recurrent laryngeal nerve and parathyroid gland were re-checked before rinsing and hemostasis (Figure 10). Then, the specimen was taken directly through the trocar port (Figure 11). Through the axillary incision, a single drain was placed in the cavity left after careful lavage. The wound was closed cosmetically. The small incision scar in the axilla was completely covered when the arm was in its natural position.
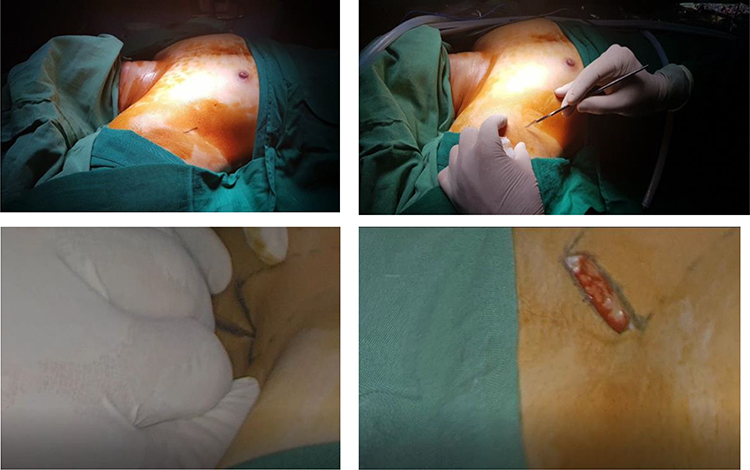 |
Figure 2 The 3-cm skin incision in right armpit of the patient. |
 |
Figure 3 A working space on the pectoralis major muscle and the subcutaneous tissue was dissected, then, the split was carried out in all directions to create a large enough cavity. |
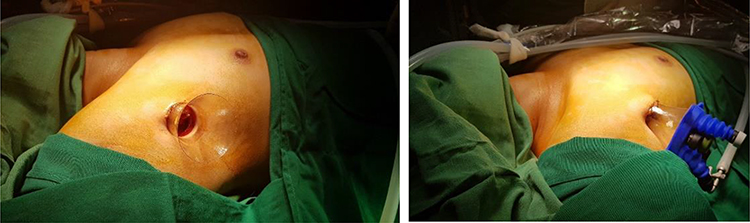 |
Figure 4 A port device with multiple channels was installed through the incision and CO2 was pumped into the cavity. |
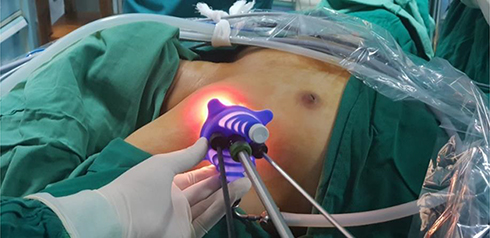 |
Figure 5 Insertion of endoscopic kit. |
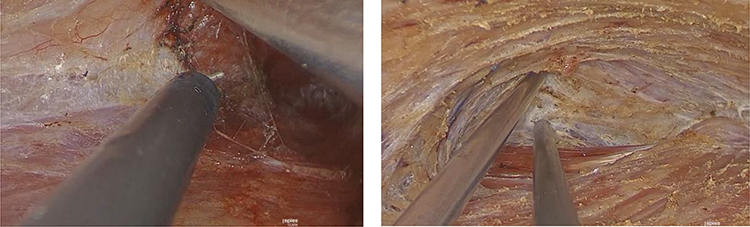 |
Figure 6 Muscle separation to create the working space. |
 |
Figure 7 To separate the front border of the sternocleidomastoid muscle and omohyoid muscle. |
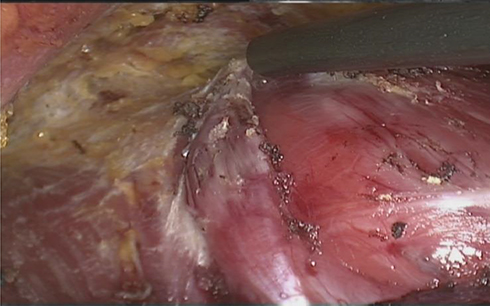 |
Figure 8 Sternothyfold muscle cut along to enter the thyroid lobe. |
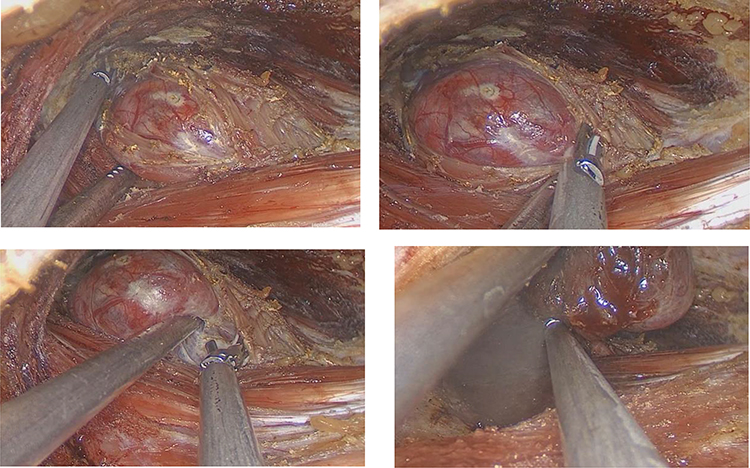 |
Figure 9 The upper and lower extremities of the thyroid gland removed and the posterior lateral part of the thyroid gland separated. |
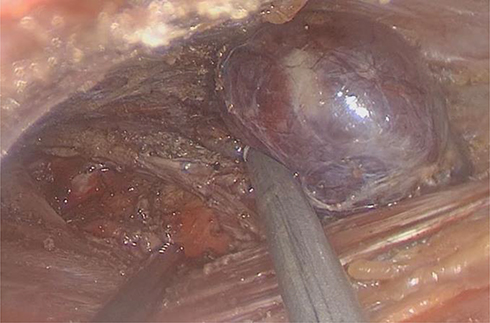 |
Figure 10 Recurrent laryngeal nerve and parathyroid gland carefully re-checked before rinsing and hemostasis. |
 |
Figure 11 The specimen was taken directly through the trocar port. |
Statistical Analysis
Statistical analysis was performed with the use of Stata® 15 (StataCorp LLC, USA) software. Categorical variables were presented as counts with percentage. Continuous variables were presented with mean, standard deviation (SD), and interquartile range.
Results
Preoperative Patient Characteristics
Of the 54 patients who underwent a single-incision endoscopic thyroidectomy via the axillary approach, the majority were female (n = 51, 94.4%). The mean age was 34.7 years (± 8.5, range 17–56). Thirty-one patients who suffered from dysphagia were detected with thyroid tumors (57.4%), while 23 patients were detected in periodic health examination (42.6%). The time from symptom onset to hospitalisation was mostly within 12 months (n = 43, 79.7%). On thyroid physical examination, the thyroid tumor was found in the left lobe with 22 patients (40.7%), in right lobe with 31 patients (57.4%), and in the isthmus with only 1 patient (1.9%). Most patients had hard consistency of the nodule (n = 51, 94.4%), well-defined margin of tumor (n = 45, 83.3%), and mobile tumor (n = 39, 72.2%) (Table 1).
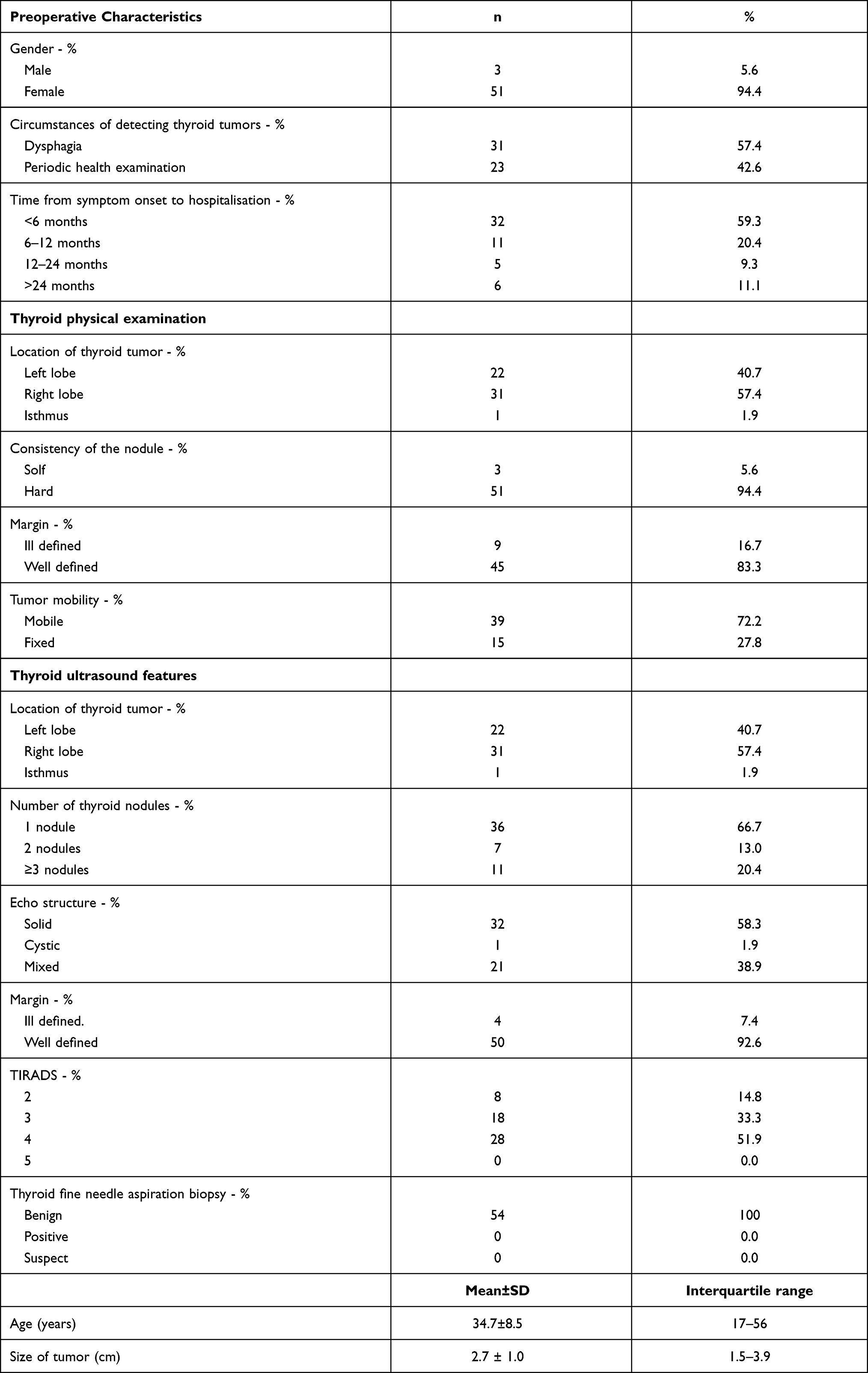 |
Table 1 Preoperative Characteristics |
Several preoperative thyroid ultrasound features are also shown in Table 1. The mean size of tumor was 2.7 cm (± 1.0, range 1.5–3.9). The location of the thyroid tumor on ultrasound was consistent with on physical examination. Thirty-six patients had one thyroid nodule (66.7%), 7 had two thyroid nodules (13.0%), and 11 had three thyroid nodules or over (20.4%). Echo structures of solid, mixed, and cystic were 58.3% patients, 38.9% patients and 1.9% patients, respectively. Fifty patients had a well-defined margin of tumor on ultrasound (92.6%). 8 patients were classified as TIRADS 2 (14.8%), when it was seen TIRADS 3 in 18 patients (33.3%) and TIRADS 4 in 28 patients (51.9%).
Operative and Postoperative Patient Characteristics
Table 2 shows operative patient characteristics. We performed the removal of the right lobe of the thyroid in 19 patients (35.2%), the right lobe of the thyroid in 34 patients (62.9%), and the isthmus of the thyroid in 1 patient (1.9%). The working space for this operation was easily created in 44 patients (81.5%). There were 9 patients experiencing difficult dissection (16.7%). Mean total operation time was 66.0 minutes (± 12.9, range 50–120) and mean blood loss was 13.3 mL (± 9.1, range 0–50).
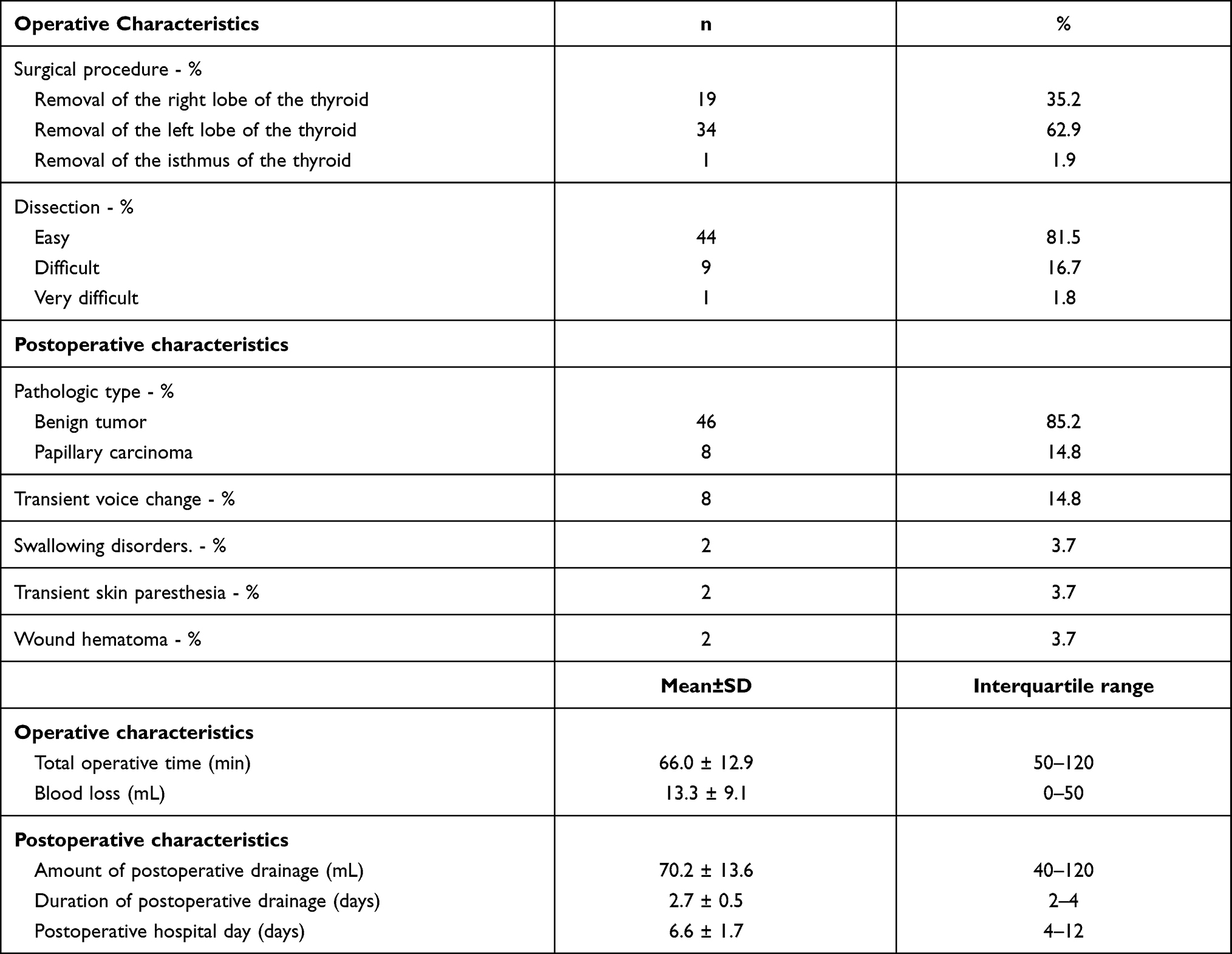 |
Table 2 Operative and Postoperative Characteristics |
Main postoperative patient characteristics are also shown in Table 2. No mortality was observed in the study cohort, and morbidities included transient voice change in 8 patients, swallowing disorders in 2 patients, transient skin paresthesia in 2 patients and wound hematoma in 2 patients. Mean amount of postoperative drainage was 70.2 mL (± 13.6, range 40–120), mean duration of postoperative drainage was 2.7 days (± 0.5, range 2–4), and mean postoperative hospital day was 6.6 days (± 1.7, range 4–12). Postoperative pathological examinations revealed 46 benign tumors (85.2%) and 8 papillary carcinomas (14.8%).
Medium-Term Follow-Up Outcomes After 3-Month Surgery
As was shown in Tables 3, 3 patients had hypothyroidism (5.6%) and 1 patient had hypocalcemia (1.8%). Most patients felt normal neck movement and sensation (79.6%), 3 patients were painful (5.6%) and 8 those were numb (14.8%). We assessed the soft incision scar in 35 patients (64.8%), convex scar in 14 patients (25.9%), and hard scar in 5 patients (9.3%). Overall, convenient surgical outcome was recorded for the whole cohort.
 |
Table 3 Medium-Term Follow-Up Outcomes After 3-Month Surgery |
Discussion
In this study, we selected the patients with benign thyroid nodules because this is a group whose thyroid nucleus is in the envelope and does not tend to invade out. In addition, since this is a newly developed technique combined with the first implementation in our center, the selection of patients with size of tumor below 4 cm with the exclusion of grade III tumors, thyroiditis, hyperthyroidism, and previous history of neck surgery or irradiation will be suitable for removing the entire thyroid lobe without tearing the sheath. In addition, the present indications enable the surgeons to perform the surgical procedure by the axillary approach thoroughly in the stages as well as safely in terms of oncology.
To date, endoscopic thyroidectomy has 5 main approaches to create the working space, including cervical approach, anterior chest approach, axillary approach, transoral approach, and postauricular facelift approach. Surgeons can use individual approaches, or they can also combine different approaches. Surgical manipulations can be performed with the robotic or endoscopic instruments.4 Each approach method to create a working space for thyroid endoscopy requires extensive training from the surgeon. The advantages and disadvantages of these approaches were recently reported by Kyung Tae et al 20195 (Table 4).
 |
Table 4 Comparison of the Approaches |
Currently in Vietnam, the endoscopic thyroid surgery of the Dr. Luong with 3 trocars was common, which were placed in the middle armpit, areola and in the delta-thoracic furrow. In the Dr. Luong’ technique, the trocar placement is directly on the patient's skin with the skin incisions being equal to the size of the trocar. In the current series of patients, in trocar insertion stage, we performed a 3 cm cut in the armpit position. Then, we dissectively create a split cavity in all directions to create a large enough cavity and place a one-port trocar. We find that there is a difference between the technique of placing one-port trocar compared to the previous technique of Dr. Luong. For the Dr. Luong’ technique, when the trocar was placed directly through the skin, the trocar leg was usually closed. Hence, gas will not be released during surgery. Meanwhile, our technique of keeping air in the surgical cavity was more difficult because the one-port trocar was placed through a trocar plastic tube, resulting in that the edges may be exposed during surgery. Compared to Dr. Luong’, it took more time for us to perform a working space between the pectoralis major muscle and the subcutaneous tissue, splitting wide in directions to create a large enough cavity before placing a single-port trocar, taking about 10–15 minutes to complete the set of one-port trocar.
We also create a CO2 pump surgical cavity like many of the authors used earlier. The air cavity not only lifts the stripped skin but also takes advantage of the organizational separation effect of CO2. When pumping CO2, the gas creeps into the associated organizational area to extract this part, the observation of the organization is clearer and the ablation of the organization is also much more convenient. We did not see any patients with CO2 poisoning or mediastinal airflow. One advantage of CO2 for creating a working cavity is that it is easy to perform in surgery, does not have to equipment, does not require time-consuming operations in surgery and leaves no scars on the neck area, although it has very small scars. While the organizational ablation creates a lot of smoke during the surgery, the inflow of air also has the effect of expelling the gas to clarify the anatomy, because in the surgery, there is a valve of the trocar that must be open to discharge air. We splitted slowly toward the snout, on the correct porous layer. The dissection area is usually above transverse to the thyroid cartilage and laterally to the outer edge of the sternum. With the cavity-forming technique in the existing one-port approach, it is difficult for the surgeon to place the trocar first, as the one-port trocar must be made sure to fit into the anatomical inlet in the armpit. Since the instruments are almost parallel to each other during surgery, collisions between surgical instruments cannot be avoided, and to avoid this we have to use the 30 degrees for a wider field of view.
In addition, once performing the dissection of the upper and lower extremities of the thyroid gland, we must use a suitable curved kit together with straight kit. During cavity creation, when we want to move up or down, it will directly affect the bronchoscope, as well as possibly collide with the trocar leg leading to air leakage. Therefore, to limit the above disadvantages, it is required that surgeons have enough experience with laparoscopic surgery in general, as well as previous experience in endoscopic thyroid surgery in particular. The important thing with this technique is that we still have to make sure the cavity is large enough to be able to separate the thyroid from a single lateral line. In addition to having to keep the gas in the cavity, at some time we need a second physician assistant to hold the trocar close to the skin wall so as not to allow entry and CO2 loss out.
Up to now, most surgical centers in Vietnam have commonly performed the technique of Dr. Luong, laparoscopic surgery with the axillary-breast approach to enter the thyroid lobe. Following the Dr. Luong’ approach, the authors found that the thymus-thyroid muscle covers the front of the thyroid gland and when this longitudinal separation does not cause damage to any muscle groups during surgery, then the hump protrudes itself and is fully exposed to the front. In addition, surgeon also easily reveals the superior vascular, recurrent laryngeal nerve and parathyroid gland in the side wall.6 With our unique approach, surgeons need to enter the thyroid laterally up the thyroid without damaging the mammary gland. Since the level of effectiveness and invasiveness is not much different from the previous technique, along with the aesthetic advantage of the patient right after surgery, this technique we gradually selected more common in surgical treatment for benign single-lobe nuclear goiter, with only a 3-cm incision in the patient’ armpit. The current single-incision axillary approach is fundamentally improved on the basis of laparoscopic surgical techniques and lateral thyroid laparoscopic access by Dr. Luong. We also approached the thyroid by the lateral line after creating the working cavity, so we inherited the advantages and previous experience from the 3-port approach of Dr. Luong. In the Dr. Luong’ approach, the 3 lateral approach lines are located in 3 different planes, so it is convenient for the surgeon to detach the upper and lower extremities of the thyroid gland. Meanwhile, all three of our instruments are almost parallel, so the use of a 30-degree lens combined with endoscopic experience in visualizing different planes during surgery is necessary to have a more favorable field of view in determining anatomical landmarks around the thyroid gland as well as during dissection. The endoscopy was performed through a single port and the insertion trocars were basically parallel, so we could not avoid collisions between instruments. Especially when dissection, we cannot avoid trauma to recurrent laryngeal nerve in some cases, manifested that, postoperatively, there were 8 patients suffered from transient voice change. In particular, we found the dissection of the thyroid gland would be more difficult and more prolonging in the cases with limited tumor mobility or solid echo structure. Due to the above limitations, the current lateral single-port laparoscopy by the axillary approach requires smooth coordination between the main surgeon and the camera assistant, as well as the previous 3-port laparoscopic surgery experience of the surgeons. In addition, we also suggest the need to improve the curvature kit for laparoscopic surgery based on the experience of the surgeon, thereby, to facilitate the separation of parathyroid glands and recurrent laryngeal nerve. To prevent the spread and spillage of thyroid cells during the removal of the specimen, the samples taken out are usually stored in a plastic bag and taken out directly through trocar port.7 This procedure requires a tough bag, along with a tool that is not too sharp to grip the specimen. Specimens inside the bag are removed by suction, forceps or both. However, in order to pass the specimen through the trocar port with small size, some authors have to tear the thyroid nucleus to remove it many times.8 Importantly, if the surgeons are not careful in the process of collecting samples out through the trocar port, you may puncture the bag, tear your bag and spill the thyroid cells along the way. In the present cohort, we did not use plastic bags, which was different from previous studies. We have completely removed the entire thyroid lobe in all cases and put the sample directly out quickly and intact in just 5–10 seconds through the trocar port. In our approach, in addition to the surgeons having to avoid key components during surgery, it’s also important to fully remove the goiter. Patient samples are drawn quickly through the trocar port, thereby shortening the sampling time much more than the sampling time compared to previous used techniques.
The average surgery time was recorded to be 66.02 minutes (± 12.94, range 50–120), which seems to be reasonable compared to the results of previous studies, which reported a mean operative time of 66–93 min for an anterior approach with neck incision.9–13 Considering each stage separately, we spent more time in creating surgical cavities, but the time to take samples out of the patient was significantly shortened. Given the previous experience of surgeons with the current one-port approach, we believe that endoscopic thyroidectomy time will be even shorter in future cases. In fact, the time of endoscopic thyroidectomy varies among studies because the total time depends on the time at each surgery stage, the experience of the surgeon, processing methods, as well as technical adjustments of each institution. Previously, a surgeon’s competency with an operation has been measured on the basis of various parameters, including operative time,14 operative time plus incidence of postoperative complications,15,16 or operative time plus intraoperative volume of blood loss.17 Nevertheless, in our experience, there were no serious complications occurring postoperatively during our study period, and intraoperative blood loss was negligible. Postoperative bleeding is also of concern due to the requirement of reoperation, even if detected in time can cause apnea due to compression of the trachea. The results of our study had no cases of bleeding during surgery, showing that if the bleeding was carefully stopped, this complication was not worrying, as well as the safety of the single-incision endoscopic thyroidectomy by the axillary approach. Our results were consistent with previous reports of Jinbeom Cho,2 David J,18 Shizuonakano19 and Tran Ngoc Luong.20
Since thyroid disease occurred more commonly in women, cosmetic outcome was an important postoperative output parameter in thyroid surgery. A verbal response scale was used to estimate the patients’ satisfaction with the postoperative wound. Although this method has been consistently used in previous studies9–11,13 since its introduction by Miccoli et al,12 we consider this as an important limitation regarding the level of evidence and think that a quantitative grading system for estimating wound satisfaction is required for the purpose of scientific and objective research. We recommend that such a grading system should take into account the degree of scarring, length of incision, incidence of postoperative surgical wound complications, and patients’ subjective estimation. In terms of cosmoses in general, all the patients were satisfied with good cosmetic results and 14 patients with hypertrophic scars (25.9%). This is probably due to the reduced length of incision and the double-ring wound retraction, which protected the wound from maceration and contamination.
Thyroid surgeons’ expectations for surgical outcomes evolve over time. Single-port access endoscopic thyroidectomy via axillary approach differs from the conventional thyroidectomy not only in terms of its incision length and better cosmesis but also with advantages galore which includes decreased tissue trauma, less hospital stay, less postoperative pain and increased postoperative comfort.2,3,21–23 To overcome the pain and invasiveness, we decided the 3-cm incision size and applied single-incision endoscopic surgery so as to narrow the dissection area approaching the operation site. Several port-access techniques have been developed in various institutions to carry out single-incision laparoscopic surgery;24–26 however, there is still no commercial single-port access in Vietnam, and single-port devices have problems with medical insurance coverage. Thus, we used commonly available devices in laparoendoscopic surgery using an axillary approach for our patient cohort.
Several limitations should be acknowledged in our study. Our sample size was relatively small, partially due to the restriction to patients’ hospital visits during the Covid-19 pandemic, suggesting that a larger number of patients in the many-year cohort may enable a better understanding of the advantages and disadvantages of single-incision endoscopic thyroidectomy using the axillary approach. Also, like most similar reports, our study had single-center results that may not reflect current practice at other surgical centers. Since it is our initial experience in the National Hospital of Endocrinology, the colleagues need careful consideration in extending other indications with the best development of suitable single-port devices once introducing this technique.
Conclusions
Our results showed reasonable surgical outcomes compared to previous studies on endoscopic thyroidectomy. A single-port endoscopic thyroidectomy via axillary approach is a safe and feasible treatment option for removing benign thyroid tumor, delivering favorable surgical outcomes with ideal cosmetic effect and reduction in injury to the anterior neck tissue. Since this is our initial experience in Vietnam with new aspects of single-port access surgery via axillary route, its further development can be considered with expanded patient indications.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Board of Hanoi Medical University.
Acknowledgments
We would like to thank Assoc. Prof. Dr. Quoc-Hung Doan (Hanoi Medical University) for critical reading and checking to improve the manuscript. Assoc. Prof. Dr. Quoc-Hung Doan partially supported the authors in the sections of methodology, data curation, and writing—review and editing. Hoang-Hiep Phan and Thai-Hoang Nguyen are co-first authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Tsai AY, Selzer DJ. Single-port laparoscopic surgery. Adv Surg. 2010;44(1):1–27.
2. Cho J, Lee D, Baek J, Lee J, Park Y, Sung K. Single-incision endoscopic thyroidectomy by the axillary approach with gas inflation for the benign thyroid tumor: retrospective analysis for a single surgeon’s experience. Surg Endosc. 2017;31(1):437–444.
3. Cho J, Park Y, Baek J, Sung K. Single-incision endoscopic thyroidectomy for papillary thyroid cancer: a pilot study. Int J Surg. 2017;43:1–6.
4. Berber E, Bernet V, Fahey III TJ, et al. American Thyroid Association statement on remote-access thyroid surgery. Thyroid. 2016;26(3):331–337.
5. Tae K, Ji YB, Song CM, Ryu J. Robotic and endoscopic thyroid surgery: evolution and advances. Clin Exp Otorhinolaryngol. 2019;12(1):1.
6. Lương TN. Cắt toàn bộ tuyến giáp nội soi để điều trị ung thư. T?p Chí Y H?c Vi?t Nam. 2012;2:57–60.
7. Slotema ET, Sebag F, Henry J. What is the evidence for endoscopic thyroidectomy in the management of benign thyroid disease? World J Surg. 2008;32(7):1325–1332.
8. Inabnet Iii W, Jacob B, Gagner M. Minimally invasive endoscopic thyroidectomy by a cervical approach. Surg Endoscopy Other Interventional Tech. 2003;17(11):1808–1811.
9. Bellantone R, Lombardi CP, Bossola M, et al. Video-assisted vs conventional thyroid lobectomy: a randomized trial. Arch Surg. 2002;137(3):301–305.
10. Hegazy MA, Khater AA, Setit AE, et al. Minimally invasive video-assisted thyroidectomy for small follicular thyroid nodules. World J Surg. 2007;31(9):1743–1750.
11. Lombardi CP, Raffaelli M, Princi P, et al. Safety of video‐assisted thyroidectomy versus conventional surgery. Head Neck. 2005;27(1):58–64.
12. Miccoli P, Berti P, Raffaelli M, Materazzi G, Baldacci S, Rossi G. Comparison between minimally invasive video-assisted thyroidectomy and conventional thyroidectomy: a prospective randomized study. Surgery. 2001;130(6):1039–1043.
13. Dobrinja C, Trevisan G, Makovac P, Liguori G. Minimally invasive video-assisted thyroidectomy compared with conventional thyroidectomy in a general surgery department. Surg Endosc. 2009;23(10):2263–2267.
14. Liao H-J, Dong C, Kong F-J, Zhang Z-P, Huang P, Chang S. The CUSUM analysis of the learning curve for endoscopic thyroidectomy by the breast approach. Surg Innov. 2014;21(2):221–228.
15. Kwak HY, Kim SH, Chae BJ, Song BJ, Jung SS, Bae JS. Learning curve for gasless endoscopic thyroidectomy using the trans-axillary approach: CUSUM analysis of a single surgeon’s experience. Int J Surg. 2014;12(12):1273–1277.
16. Maguire T, Mayne CJ, Terry T, Tincello DG. Analysis of the surgical learning curve using the cumulative sum (CUSUM) method. Neurourol Urodyn. 2013;32(7):964–967.
17. Liu S, Qiu M, Jiang D-Z, et al. The learning curve for endoscopic thyroidectomy: a single surgeon’s experience. Surg Endosc. 2009;23(8):1802–1806.
18. Terris DJ, Angelos P, Steward DL, Simental AA. Minimally invasive video-assisted thyroidectomy: a multi-institutional North American experience. Arch Otolaryngol Head Neck Surg. 2008;134(1):81–84.
19. Ikeda Y, Takami H, Niimi M, Kan S, Sasaki Y, Takayama J. Endoscopic total parathyroidectomy by the anterior chest approach for renal hyperparathyroidism. Surg Endoscopy Other Interventional Tech. 2002;16(2):320–322.
20. Lương TN. Nghiên Cứu Ứng Dụng Phẫu Thuật Nội Soi Điều Trị Bướu Giáp Thể Nhân Lành Tính. Hà Nội: Đại học Y Hà Nội; 2006.
21. Calò PG, Medas F, Conzo G, et al. Intraoperative neuromonitoring in thyroid surgery: is the two-staged thyroidectomy justified? Int J Surg. 2017;41:S13–S20.
22. Conzo G, Docimo G, Mauriello C, et al. The current status of lymph node dissection in the treatment of papillary thyroid cancer. A Literature Review Clin Ter. 2013;164(4):e343–6.
23. Docimo G, Tolone S, Ruggiero R, et al. Total thyroidectomy without prophylactic central neck dissection combined with routine oral calcium and vitamin D supplements: is it a good option to achieve a low recurrence rate avoiding hypocalcemia? A retrospective study. Minerva Chir. 2013;68(3):321–328.
24. Sakr MF. Thyroidectomy Techniques. Thyroid Disease. Springer; 2020:505–597.
25. Kim Y-S, Joo K-H, Park S-C, Kim K-H, Ahn C-H, Kim J-S. Endoscopic thyroid surgery via a breast approach: a single institution’s experiences. BMC Surg. 2014;14(1):1–6.
26. Fan S, Liang F-Y, Chen W-L, et al. Minimally Invasive selective neck dissection: a prospective study of endoscopically assisted dissection via a small submandibular approach in cT 1–2 N 0 oral squamous cell carcinoma. Ann Surg Oncol. 2014;21(12):3876–3881.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.