Back to Journals » Journal of Pain Research » Volume 18
Single-Injection Adductor Canal Block Enhances Early Mobilization with Comparable Analgesia to Continuous Infusion in Unicompartmental Knee Arthroplasty: A Retrospective Cohort Study
Authors Lan F, Chong Y, Liu F, Wang T ![]()
Received 6 February 2025
Accepted for publication 26 July 2025
Published 1 August 2025 Volume 2025:18 Pages 3851—3858
DOI https://doi.org/10.2147/JPR.S512475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Karina Gritsenko
Fei Lan,* Yuhan Chong,* Fangyan Liu, Tianlong Wang
Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fangyan Liu, Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +86-18500372835, Email [email protected] Tianlong Wang, Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +86-13910525304, Email [email protected]
Objective: Adductor canal block (ACB) is commonly used for postoperative analgesia after unicompartmental knee arthroplasty (UKA). However, the comparative benefits of single-injection ACB (SACB) versus continuous ACB (CACB) remain unclear.
Methods: In our retrospective cohort study, patients undergoing unilateral, primary UKA were allocated to group CACB or group SACB from January 2016 to December 2023. The primary outcome was the visual analog scale (VAS) for pain. Secondary outcomes included the additional analgesic therapy, activity score, postoperative nausea and vomiting (PONV), complications, and length of stay (LOS).
Results: After 1:1 propensity score matching based on age, sex, body mass index (BMI), and preoperative pain score, 35 patients were included in each group (SACB and CACB). At 24 hours postoperatively, the SACB group had a slightly higher VAS pain score compared with the CACB group, though this difference was not statistically significant. The Post-Anesthesia Care Unit (PACU) activity score was significantly higher in the SACB group (p = 0.02), and the LOS was significantly shorter by approximately 3 days compared to the CACB group (p < 0.001). No significant differences were found between groups in terms of additional analgesic therapy, Oxford Knee Score (OKS), PONV, or complications.
Discussion: CACB did not significantly reduce postoperative pain or improve functional outcomes over three months after UKA compared to SACB. However, SACB was associated with improved immediate postoperative mobility and a shorter LOS, suggesting potential benefits for early recovery.
Keywords: unicompartmental knee arthroplasty, pain control, adductor canal block
Introduction
Unicompartmental knee arthroplasty (UKA) and total knee arthroplasty (TKA) are both widely accepted treatment options for patients with end-stage medial compartment osteoarthritis.1 UKA has several advantages over TKA, including more natural knee kinematics, a greater range of motion, higher patient satisfaction, lower complication and mortality rates, faster recovery, and improved patient-reported outcomes.2 While TKA has been the focus of extensive research on postoperative pain management strategies,2,3 the optimal analgesic protocol for UKA remains underexplored, despite its rising popularity.4 UKA, although less invasive, still induces considerable postoperative pain that may compromise early rehabilitation if not effectively managed.5,6 As a result of tourniquet-induced ischemia and surgical stress, inflammatory mediators are produced, leading to severe pain in most patients after knee arthroplasty.7
It is well established that nerve blocks are a crucial component of the multimodal analgesia regimen during the perioperative period after UKA,8 especially for adductor canal block (ACB).9 ACB provides effective analgesia to the anteromedial aspect of the knee by targeting the saphenous nerve while preserving quadriceps strength, making it particularly suitable for patients undergoing UKA who are expected to ambulate early.10 Both single-injection (SACB) and continuous infusion (CACB) adductor canal blocks are widely used as components of a multimodal analgesia regimen, each with its own benefits and limitations. Although SACB offers notable advantages in terms of technical simplicity, safety, and reliability, its relatively short duration of analgesia and the risk of rebound pain may limit its effectiveness compared to CACB. The potential for CACB to extend or amplify the clinically relevant analgesic effects of SACB has yet to be conclusively determined.11
Previous studies have compared SACB and CACB mainly in TKA patients, showing mixed results regarding duration of analgesia, opioid consumption, and functional recovery.12,13 However, direct comparative studies in UKA patients are scarce, and the generalizability of TKA findings to UKA remains uncertain due to differences in surgical invasiveness and rehabilitation protocols.
Given the increasing emphasis on enhanced recovery protocols, identifying analgesic strategies that not only relieve pain but also support early ambulation is crucial.14 This study addresses a current evidence gap by directly comparing SACB and CACB in the context of UKA, with a focus on both immediate and longer-term outcomes.
Methods
Ethical Approval and Study Registration
The study was registered on the Chinese Clinical Trial Registry (ChiCTR2400092668), and due to its retrospective nature, the requirement for informed consent was waived. Ethical approval was granted by the ethics committee of Xuanwu Hospital, Capital Medical University ([2024]078–002).
Study Design and Patient Selection
This retrospective cohort study analyzed patients who underwent primary UKA with either SACB or CACB between January 2016 and December 2023. Patients diagnosed with osteoarthritis or inflammatory arthritis who went through unilateral condylar replacement surgery in Xuanwu Hospital were included in the study. This study enrolled adult patients aged over 18 years, with ASA classification of I–III. We excluded patients whose surgical plans were modified due to comorbidities or intraoperative findings, such as serious diseases affecting the heart, kidneys, liver, or other vital organs; inability to cooperate with pain scoring or early postoperative rehabilitation; or cases where bilateral unicondylar replacements were performed either separately or simultaneously during the study period. A total of 136 patients were initially assessed, and after propensity score matching, 70 patients were included in the final analysis, with 35 patients assigned to each group. A flow diagram of patient selection and group allocation is shown in Figure 1.
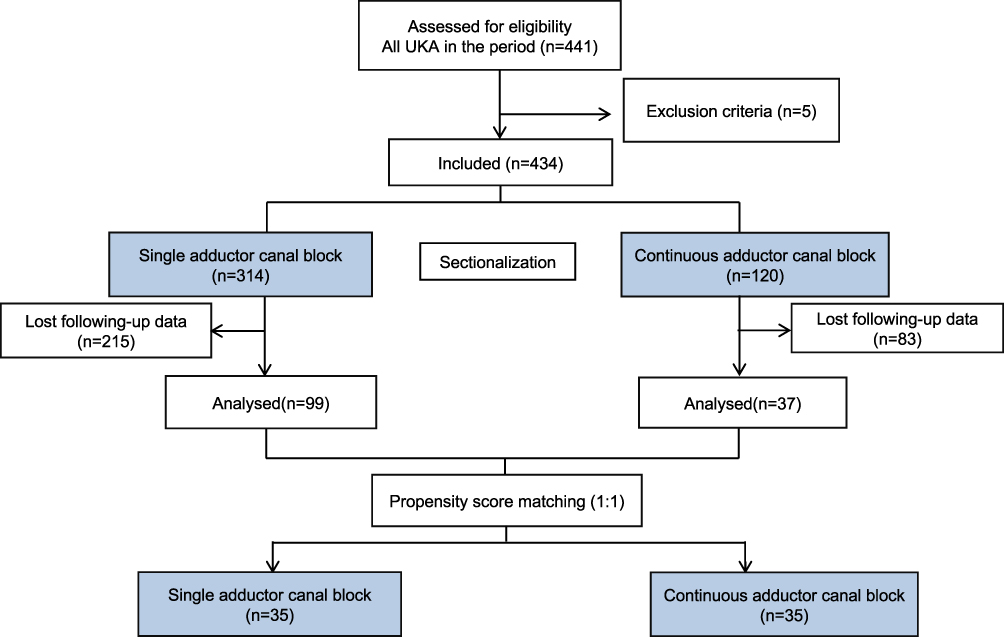 |
Figure 1 Flow chart of the study. |
Anesthesia and Analgesia Protocol
All patients received preoperative celecoxib as premedication. Spinal anesthesia was performed using 0.5% bupivacaine (Marcaine, Harvest, Shanghai) in all cases. Two experienced surgeons performed all knee surgeries using similar techniques. All patients underwent surgery with the use of a tourniquet, typically applied for less than 90 minutes. Prior to skin incision, 1 g of intravenous tranexamic acid (TXA) was administered. Intraoperatively, all patients received local infiltration analgesia (LIA) prepared under aseptic conditions, consisting of 100 mL of 0.2% ropivacaine, 10 mg of oxycodone, and 0.5 mg of epinephrine. The mixture was infiltrated into periarticular soft tissues—including the posterior and anterior capsule, ligaments, synovium, retinaculum, fat pad, and subcutaneous layers—at various stages of surgery, following a standardized protocol.15 For the nerve block administered immediately after the operation, patients were positioned supine with the hip externally rotated and the knee flexed. An 8-cm stimulating needle was inserted laterally to medially, positioning the tip deep to the sartorius muscle and lateral to the femoral artery at the apex of the femoral triangle. A total of 25 milliliters of 0.33% ropivacaine was administered gradually with intermittent aspiration. Patients in the CACB group received patient-controlled nerve block analgesia (PCNA) with 0.2% ropivacaine for 48 hours after a single injection. The PCNA settings included a background infusion rate of 5 mL/h, a bolus volume of 5 mL, and a lockout period of 30 minutes. Additional analgesic therapy refers to the administration of rescue analgesics in the PACU or ward when patients reported inadequate pain relief. In most cases, this included oral NSAIDs (celecoxib), intravenous parecoxib (40 mg), administered as needed.
Outcome Measures
The primary outcome was postoperative pain assessed using the VAS. Pain at rest and during movement was assessed using a visual analog scale (VAS, 0–10). For movement pain at 0 hours in the PACU, patients were instructed to lift the operated leg approximately 15–20 cm off the bed while in the supine position, and the pain level during this action was recorded. As the effects of spinal anesthesia had not fully worn off at that time, nurses assisted patients in performing the movement, and patients reported their pain scores based on their subjective experience during the assisted motion. At 24 hours postoperatively, the movement pain score was recorded by asking patients to rate the pain they experienced during ambulation (ie, when getting out of bed and walking with assistance). Secondary outcomes included: OKS, additional analgesic therapy, activity score assessed by PACU, LOS, and complications after the surgery. The activity score which was assessed by PACU recorded the postoperative ambulation status in the first 24 hours. The frequency of postoperative nausea and vomiting (PONV) was observed. PONV was assessed through standardized follow-up by PACU nurses on postoperative day one and documented in the electronic medical records. Other complications, included dizziness, catheter site infection, prolonged motor block, and falls prior to discharge, were also evaluated based on clinical documentation. The data were collected retrospectively from existing medical records by a researcher (CYH) who was blinded to group allocation in order to minimize assessment bias.
Statistical Analyses
All measured parameters were summarized using descriptive statistics, including counts and percentages for categorical variables, means with standard deviations (SD) for normally distributed continuous variables, and medians with interquartile ranges (IQR) for non-normally distributed data. Propensity score matching between the SACB and CACB groups was based on preoperative visual analog scale (VAS) pain scores and patient characteristics such as age, sex, and BMI. The Student’s t-test was used to compare normally distributed continuous variables, including Oxford Knee Score (OKS) and length of hospital stay (LOS). The Mann–Whitney U-test was applied to compare perioperative pain scores, which did not follow a normal distribution. Categorical variables, such as use of additional analgesic therapy, activity score assessed by PACU, and incidence of postoperative complications, were compared using either the chi-square test or Fisher’s exact test, depending on the distribution and expected cell counts. All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). A P-value < 0.05 was considered statistically significant.
Results
Data were available for 70 subjects. Thirty-five subjects received intrathecal continuous 0.33% Ropivacaine infusion (CACB) and 35 received single-injection (SACB). Demographic information for the subjects is shown in Table 1. There was no statistical difference on preoperative pain score and OKS between these two groups.
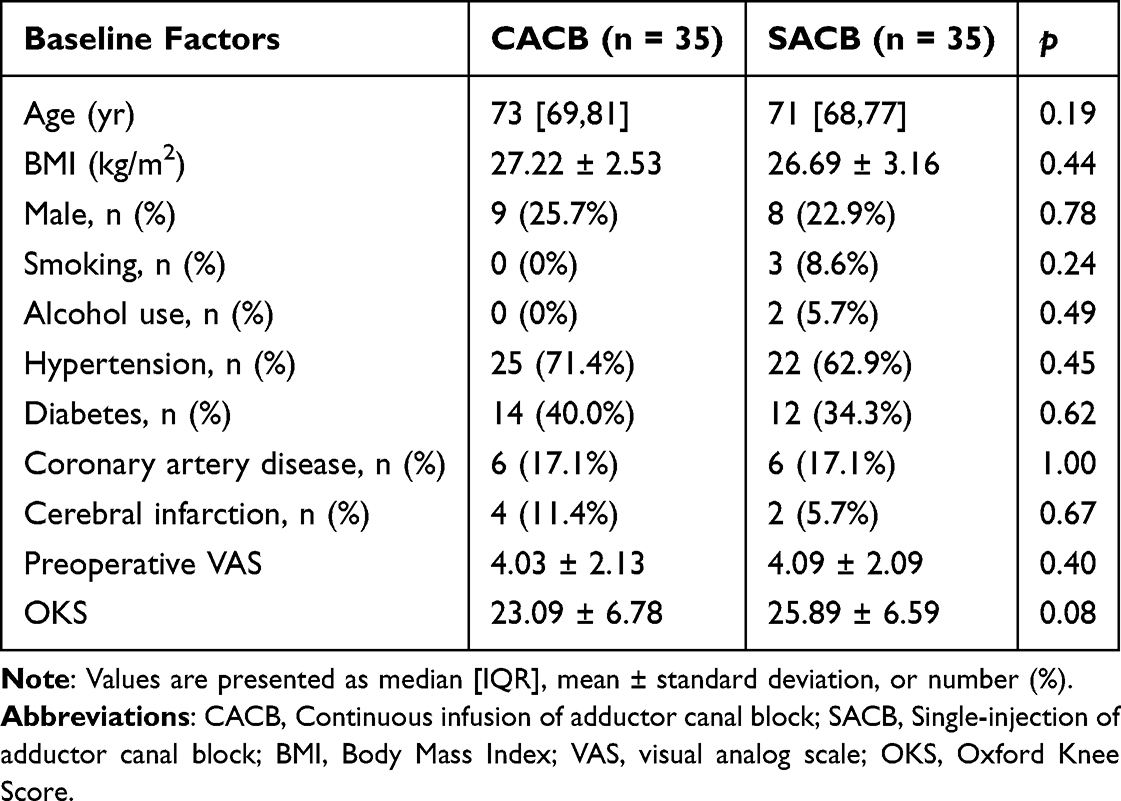 |
Table 1 Baseline Characteristics of the Patients Between Two Groups After Propensity Score Matching |
The VAS following UKA of CACB was comparable to SACB during the third month. However, VAS scores were slightly higher in SACB than CACB group at both 24 hours and three months postoperatively, but the differences were not statistically significant (p = 0.39 for rest, p = 0.18 for movement, and p = 0.15 at three months) (Figure 2). The activity Score assessed by PACU was significantly higher in SACB than CACB (p = 0.02). The OKS at both one month and three months postoperatively showed no significant difference between the SACB and CACB groups, as illustrated in Figure 3. The length of stay in SACB was 3 days shorter than that of CACB (p < 0.000). Other outcome measures including additional analgesic therapy, PONV and complications were not significantly different between the groups. No serious complications were observed in either group; only minor symptoms such as dizziness were reported. These details have been clarified in Table 2.
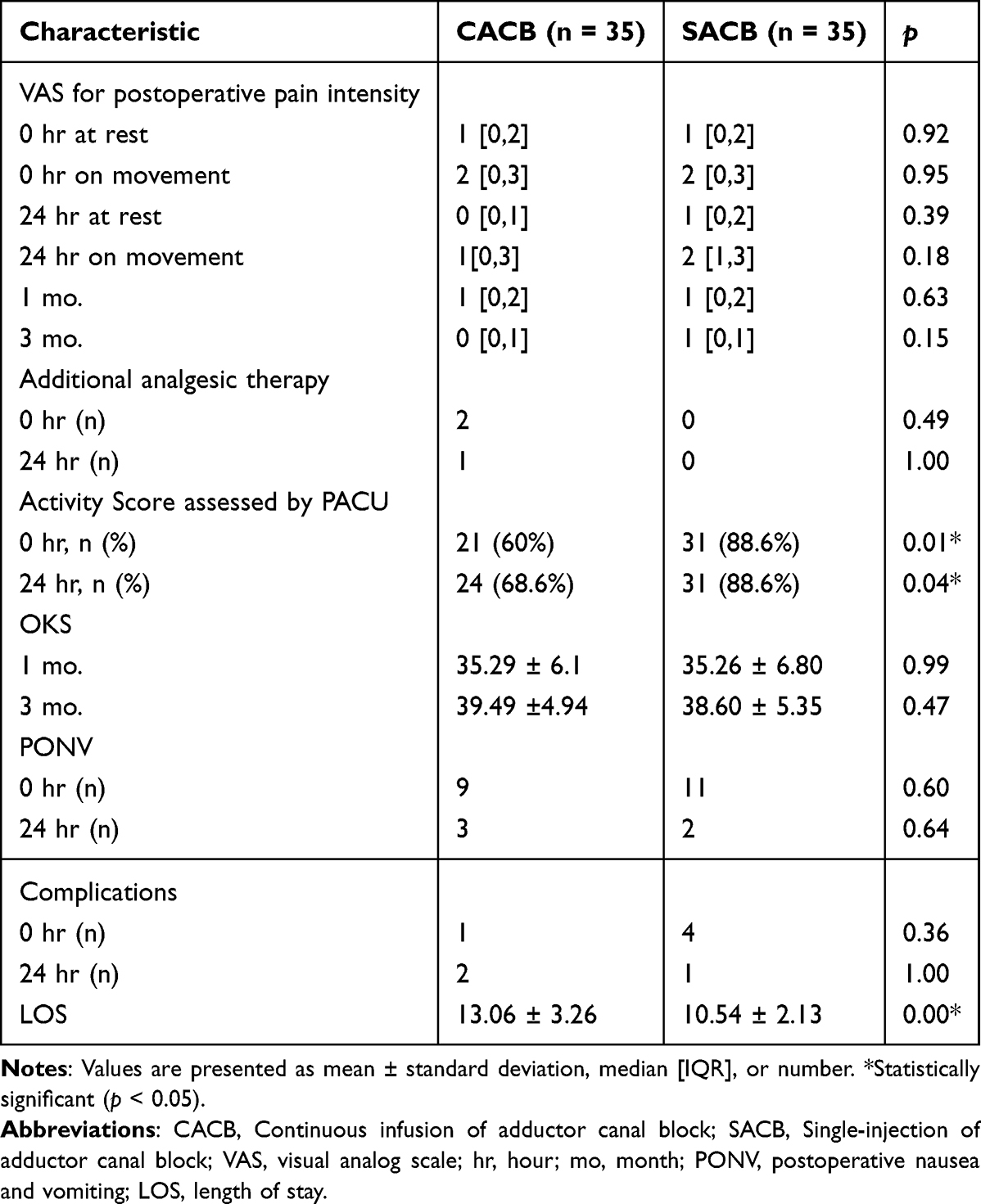 |
Table 2 Postoperative Outcome of the CACB and SACB After Propensity Score Matching |
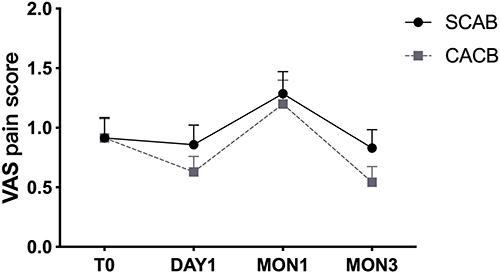 |
Figure 2 Average postoperative visual analogue scale (VAS) pain scores at rest in the SACB and CACB groups. Error bars represent the standard error of the mean (SEM). Abbreviation: VAS, visual analogue scale. |
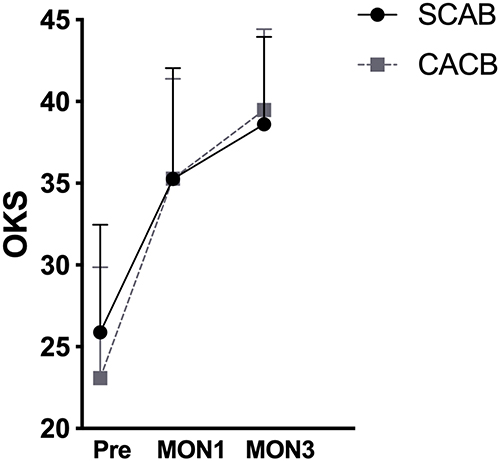 |
Figure 3 Comparison of average OKS between the SACB and CACB groups. Values are presented as mean ± standard deviation. Abbreviation: OKS, Oxford Knee Score. |
Discussion
In this retrospective cohort study, we investigated the differences in analgesic effects and other postoperative outcomes between SACB and CACB following UKA. Although CACB showed slightly better pain scores at rest on the first postoperative day and at three months postoperatively, the differences were not statistically significant (all P > 0.05). These findings suggest that CACB does not offer a clinically meaningful advantage in long-term or short-term pain relief compared to SACB. Furthermore, CACB did not reduce opioid consumption on the first postoperative day. The PACU activity score revealed that CACB was associated with limited ambulation during the first postoperative day (p < 0.05). However, no significant difference was found between the two groups in OKS at one and three months postoperatively. Other postoperative outcomes, including PONV and side effects, were not improved by CACB. In addition, the LOS was significantly greater in the CACB group (13.06 ±3.26 days) compared to the SACB group (10.54 ±2.13 days, p < 0.001).
Recent research into regional analgesia techniques has shown that ACB provides effective analgesia while maintaining quadriceps motor strength for physical performance.10,16 According to previous concepts, especially continuous infusion ACB could be theoretically superior analgesic option, as the larger volume of local anesthetic delivered may spread within the adductor canal, potentially blocking nerves in both its proximal and distal regions, thereby enhancing pain relief.13,17 Wang et al conducted a meta-analysis which enrolled 8 RCTs with 642 patients recommended CACB as an analgesic method for early postoperative pain treatment after TKA.13 Conversely, Hussain et al, after reanalyzing eleven trials, concluded that CACB does not improve or extend analgesic benefits compared to SACB for TKA in the first 48 hours postoperatively.9 The most recent study by Kim et al found that CACB and Patient-Controlled Analgesia (PCA) + SACB did not differ significantly in analgesic efficacy or opioid-related side effects.18 Our study also indicated that CACB was not statistically superior to SACB in postoperative analgesia following UKA. As CACB presents greater technical challenges and higher failure rates, its application may be constrained.19 We also applied additional analgesic therapy to assess analgesia effect between these two groups and got consistent results. Additionally, many studies found similar morphine consumption after TKA with the SACB and CACB techniques.20,21 However, multimodal preoperative treatments, such as COX inhibitors, local infiltration, or peripheral nerve blocks, can provide sufficient analgesia and support rehabilitation.22 In this study, we opted for preoperative COX inhibitors, periarticular injections, and ACB blocks. Overall, our findings suggest that a multimodal analgesic approach combined with SACB offers comparable pain control to continuous CACB.
Our results showed that ambulatory rate ambulation rate immediately and at 24 hours postoperatively was significantly higher in SACB than CACB. There was no difference of function recovery on long-term follow up between the two groups. In a study by Canbek et al, although no statistically significant difference was found, the CACB group performed better than the SACB group in ambulation tests, such as mean time to ambulation and mean time to walk upstairs.23 In contrast, Shah et al found no evidence to support the idea that CACB results in superior ambulation and early functional recovery compared to the findings of the present study.24 As we all know that better functional recovery results from better and longer pain prevention. In our study the immediate and short-term pain score were the same in the two groups. The lower PACU activity score in the CACB group may reflect delayed early ambulation, potentially resulting from quadriceps inhibition or increased patient caution. However, direct assessment of muscle strength was not performed in this study.
Moreover, PONV and side effects were not significantly different between the groups. The most common side effects in the present study were dizziness. No cases of catheter site infection or prolonged nerve block were observed in any patient during the study. The length of hospitalization was significantly longer in CACB group, which may result from the lower rate of ambulatory.
Limitations
This study has several limitations. One major limitation is the relatively small sample size (35 patients per group), which may reduce the statistical power to detect minor but potentially meaningful differences between CACB and SACB. In addition, since the choice between SACB and CACB was made based on the attending anesthesiologist’s clinical judgment rather than a standardized protocol, the possibility of confounding by indication cannot be entirely ruled out, despite our use of propensity score matching to minimize bias. Moreover, although the study spanned over seven years, perioperative analgesic protocols at our institution remained largely consistent. Nonetheless, we acknowledge that subtle changes in clinical practice over time may have introduced variability into the outcomes. Finally, most of the referenced studies were conducted in the context of total knee arthroplasty (TKA). However, unicompartmental knee arthroplasty (UKA) is associated with several advantages over TKA, including fewer major complications, lower mortality, faster recovery, and better functional outcomes. Further randomized controlled trials are needed to provide stronger evidence on the non-inferiority of SACB compared to CACB specifically in the UKA population.
Conclusion
SACB was associated with improved immediate postoperative mobility and a shorter hospital stay compared to CACB. However, CACB did not demonstrate superior outcomes in terms of postoperative pain at three months, OKS, incidence of PONV, or side effects. Given its comparable analgesic effect and advantages in early mobilization and shorter hospitalization, SACB may be considered the preferred option for perioperative pain management in UKA.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The protocol was approved by the ethics committee of Xuanwu Hospital, Capital Medical University (Approval number: [2024]078-002). Patient consent for the review of medical records was waived by the Ethics Committee due to the retrospective nature of the study. All patient data were anonymized and handled with strict confidentiality. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Funding
This work was supported by Post-subsidy funds for National Clinical Research Center, Ministry of Science and Technology of China (303-01-001-0272-03).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Wilson HA, Middleton R, Abram SGF, et al. Patient relevant outcomes of unicompartmental versus total knee replacement: systematic review and meta-analysis. BMJ. 2019;364:l352. doi:10.1136/bmj.l352
2. Janssen SJ, van Oost I, Breugem SJM, van Geenen RCI. A structured evaluation of the symptomatic medial Oxford unicompartmental knee arthroplasty (UKA). EFORT Open Rev. 2021;6(10):850–860. doi:10.1302/2058-5241.6.200105
3. Leiss F, Götz JS, Maderbacher G, et al. Pain management of unicompartmental (UKA) vs. total knee arthroplasty (TKA) based on a matched pair analysis of 4144 cases. Sci Rep. 2020;10(1):17660. doi:10.1038/s41598-020-74986-x
4. Bolognesi MP, Greiner MA, Attarian DE, et al. Unicompartmental knee arthroplasty and total knee arthroplasty among medicare beneficiaries, 2000 to 2009. J Bone Joint Surg Am. 2013;95(22):e174. doi:10.2106/JBJS.L.00652
5. D’Ambrosi R, Ursino C, Setti S, Scelsi M, Ursino N. Pulsed electromagnetic fields improve pain management and clinical outcomes after medial unicompartmental knee arthroplasty: a prospective randomised controlled trial. J ISAKOS. 2022;7(5):105–112. doi:10.1016/j.jisako.2022.05.002
6. Baker PN, Petheram T, Avery PJ, Gregg PJ, Deehan DJ. Revision for unexplained pain following unicompartmental and total knee replacement. J Bone Joint Surg Am. 2012;94(17):e126. doi:10.2106/JBJS.K.00791
7. Li Q, Nie H, Wang Z, et al. The effects of perineural dexamethasone on rebound pain after nerve block in patients with unicompartmental knee arthroplasty: a randomized controlled trial. Clin J Pain. 2024;40(7):409–414. doi:10.1097/AJP.0000000000001220
8. Singh NP, Makkar JK, Chawla JK, Sondekoppam RV, Singh PM. Prophylactic dexamethasone for rebound pain after peripheral nerve block in adult surgical patients: systematic review, meta-analysis, and trial sequential analysis of randomised controlled trials. Br J Anaesth. 2024;132(5):1112–1121. doi:10.1016/j.bja.2023.09.022
9. Hussain N, Brull R, Zhou S, et al. Analgesic benefits of single-shot versus continuous adductor canal block for total knee arthroplasty: a systemic review and meta-analysis of randomized trials. Reg Anesth Pain Med. 2023;48(2):49–60. doi:10.1136/rapm-2022-103756
10. Henshaw DS, Jaffe JD, Reynolds JW, Dobson S, Russell GB, Weller RS. An evaluation of ultrasound-guided adductor canal blockade for postoperative analgesia after medial unicondylar knee arthroplasty. Anesth Analg. 2016;122(4):1192–1201. doi:10.1213/ANE.0000000000001162
11. Sun C, Zhang X, Song F, et al. Is continuous catheter adductor canal block better than single-shot canal adductor canal block in primary total knee arthroplasty?: a GRADE analysis of the evidence through a systematic review and meta-analysis. Medicine. 2020;99(20):e20320. doi:10.1097/MD.0000000000020320
12. Zhang L-K, Zhang B-Y, Quan R-F, Xu H, Sun Y-J, Zhou J-H. Single shot versus continuous technique adductor canal block for analgesia following total knee arthroplasty: a PRISMA-compliant meta-analysis. Medicine. 2019;98(20):e15539. doi:10.1097/MD.0000000000015539
13. Wang C, Chen Z, Ma X. Continuous adductor canal block is a better choice compared to single shot after primary total knee arthroplasty: a meta-analysis of randomized controlled trials. Int J Surg. 2019;72:16–24. doi:10.1016/j.ijsu.2019.10.012
14. Barrington JW, Lovald ST, Ong KL, Watson HN, Emerson RH. How do demographic, surgical, patient, and cultural factors affect pain control after unicompartmental knee arthroplasty? A multivariable regression analysis. J Arthroplasty. 2016;31(9 Suppl):97–101. doi:10.1016/j.arth.2016.03.038
15. Lan F, Shen Y, Ma Y, et al. Continuous adductor canal block used for postoperative pain relief after medial unicondylar knee arthroplasty: a randomized, double-blind, placebo-controlled trial. BMC Anesthesiol. 2019;19(1):114. doi:10.1186/s12871-019-0787-6
16. Patterson ME, Vitter J, Bland K, Nossaman BD, Thomas LC, Chimento GF. The effect of the IPACK block on pain after primary TKA: a Double-blinded, prospective, randomized trial. J Arthroplasty. 2020;35(6S):S173–S177. doi:10.1016/j.arth.2020.01.014
17. Kim MK, Moon HY, Ryu CG, Kang H, Lee HJ, Shin HY. The analgesic efficacy of the continuous adductor canal block compared to continuous intravenous fentanyl infusion with a single-shot adductor canal block in total knee arthroplasty: a randomized controlled trial. Korean J Pain. 2019;32(1):30–38. doi:10.3344/kjp.2019.32.1.30
18. Kim SE, Han H-S, Lee MC, Ro DH. Single shot adductor canal block combined with intravenous patient-controlled analgesia can be effective as continuous adductor canal block in reducing opioid consumption and breakthrough pain after total knee arthroplasty. J Exp Orthop. 2022;9(1):84. doi:10.1186/s40634-022-00523-6
19. Hauritz RW, Hannig KE, Balocco AL, et al. Peripheral nerve catheters: a critical review of the efficacy. Best Pract Res Clin Anaesthesiol. 2019;33(3):325–339. doi:10.1016/j.bpa.2019.07.015
20. Elkassabany NM, Cai LF, Badiola I, et al. A prospective randomized open-label study of single injection versus continuous adductor canal block for postoperative analgesia after total knee arthroplasty. Bone Joint J. 2019;101-B(3):340–347. doi:10.1302/0301-620X.101B3.BJJ-2018-0852.R2
21. Turner JD, Dobson SW, Henshaw DS, et al. Single-injection adductor canal block with multiple adjuvants provides equivalent analgesia when compared with continuous adductor canal blockade for primary total knee arthroplasty: a double-blinded, randomized, controlled, equivalency trial. J Arthroplasty. 2018;33(10):3160–3166.e1. doi:10.1016/j.arth.2018.05.026
22. Terkawi AS, Mavridis D, Sessler DI, et al. Pain management modalities after total knee arthroplasty: a network meta-analysis of 170 randomized controlled trials. Anesthesiology. 2017;126(5):923–937. doi:10.1097/ALN.0000000000001607
23. Canbek U, Akgun U, Aydogan NH, Kilinc CY, Uysal AI. Continuous adductor canal block following total knee arthroplasty provides a better analgesia compared to single shot: a prospective randomized controlled trial. Acta Orthop Traumatol Turc. 2019;53(5):334–339. doi:10.1016/j.aott.2019.04.001
24. Shah NA, Jain NP, Panchal KA. Adductor canal blockade following total knee arthroplasty-continuous or single shot technique? Role in postoperative analgesia, ambulation ability and early functional recovery: a randomized controlled trial. J Arthroplasty. 2015;30(8):1476–1481. doi:10.1016/j.arth.2015.03.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.