Back to Journals » Journal of Pain Research » Volume 11
Single dose oral midazolam for minor emergency department procedures in children: a retrospective cohort study
Authors Neuman G, Swed Tobia R ![]() , Koren L, Leiba R, Shavit I
, Koren L, Leiba R, Shavit I ![]()
Received 4 November 2017
Accepted for publication 18 December 2017
Published 12 February 2018 Volume 2018:11 Pages 319—324
DOI https://doi.org/10.2147/JPR.S156080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Gal Neuman,1,* Rana Swed Tobia,2,* Liron Koren,3 Ronit Leiba,4 Itai Shavit5
1Clinical Pharmacology and Toxicology Unit, 2Department of Pediatrics, Ruth Children’s Hospital, Rambam Health Care Campus, 3Rappaport Faculty of Medicine, Technion – Institute of Technology, 4Quality of Care Unit, 5Emergency Department, Ruth Children’s Hospital, Rambam Health Care Campus, Haifa, Israel
*These authors contributed equally to this work
Background: In the pediatric emergency department, patients are commonly treated with a single dose of oral midazolam for minor procedures. We sought to evaluate the effect of this treatment on procedure completion rates.
Methods: We conducted a single-center retrospective cohort study of all patients who were treated with pre-procedure oral midazolam between January 2011 and June 2016. The primary outcome was the procedure completion rate.
Results: During the study period, 1,504 patients were treated with oral midazolam as per department protocol; 1,467 received midazolam and 37 declined midazolam. Oral midazolam was used in 14 different types of emergency department procedures. The procedure completion rates in the treatment and non-treatment groups were 1,402/1,467 (95.6%) and 24/37 (64.8%), respectively (difference 30.7%; 95% confidence interval [CI] 17.3%–46.8%); p<0.0001. Treatment group patients had procedure completion rates of 25/33 (75.8%), 165/188 (87.8%%), 1,154/1,187 (97.2%), and 58/59 (98.3%), in the less than 0.3 mg/kg group, 0.3 to less than 0.5 mg/kg group, 0.5 to less than 0.7 mg/kg group, and 0.7 to less than 0.9 mg/kg group, respectively. Multivariate regression did not demonstrate an association between sex, ethnicity, dosage of 0.5 mg/kg or greater, type of procedure, and failure to complete procedure. Severe adverse events were not recorded. A dose of less than 0.3 mg/kg was significantly associated with an increased risk of failure to complete a procedure (adjusted odds ratio 8.34, 95% CI 3.32–20.9; p<0.0001).
Conclusion: The findings suggest that oral midazolam in a single dose of 0.5 mg/kg or greater is associated with successful completion of minor pediatric procedures.
Keywords: midazolam, oral, procedures, child, emergency
Introduction
Procedure-related pain and distress are major challenges encountered when caring for sick and injured children in the emergency department (ED), and the use of sedation, a humanistic aspect of child care, has become common practice in pediatric emergency medicine worldwide.1–3 Painful procedures, such as fracture reduction, are usually treated with intravenous ketamine sedation.2,3 Despite the prevalent use of topical anesthetics, a large number of procedures, which are usually not painful, are associated with distress and suffering. Patients undergoing these minor stressful procedures are commonly treated with oral midazolam as a sole sedative agent.4–10 Currently, no study has evaluated the effect of midazolam on procedure completion rates in pediatric emergency medicine.10
In 2010, the Israeli Medical Association (IMA) issued guidelines recommending the administration of a single dose of oral midazolam prior to any distressful procedure in the pediatric ED.11 Consequently, in the ED of Ruth Children’s Hospital of Rambam Health Care Campus (RHCC) in Haifa, Israel, children receive this treatment relatively frequently.12,13
The objective of this study was to evaluate the effect of oral midazolam on procedure completion rates.
Patients and methods
Study design, subjects, and data collection
We conducted a retrospective cohort study of all children who were treated with pre-procedure oral midazolam between 1 January 2011 and 31 June 2016. Using a structured form, the electronic charts of the patients were reviewed independently by 2 abstractors (RST, LK). Chart review was conducted in accordance with published methods for retrospective studies, with the sole exception that abstraction of data was not done blindly with regard to the study objective.14 The medical charts were extracted from the ED electronic medical records system (“Prometheus”, RHCC integrated computer system). This computerized system was developed by the hospital’s department of Information Technology and is a mandatory working tool for all physicians and nursing staff. The following variables were extracted from the medical records of each patient: age, weight, sex, dosage, type of procedure, completion of procedure (yes/no), second sedative drug given and route of administration, any serious adverse event, and any ED return visit within 24 hours due to an adverse event. According to departmental policy, severe adverse reactions are recorded by the nurse responsible for the patient.15 Department protocol defines severe adverse event as hypoxia (saturation of 90% or less), apnea (discontinuation of breathing), aspiration (coughing or choking associated with observed gastric contents in the mouth), and laryngospasm (upper airway obstruction with oxygen desaturation caused by closure of the vocal cords).15 The patient records and information were anonymized and de-identified before analysis, and therefore the Institutional Review Board of RHCC (No. 0311-16) approved this study without the requirement of obtaining informed consent.
IMA protocol for pre-procedural oral midazolam in the ED
The recommended dosage of oral midazolam for ED procedures is 0.5–0.7 mg/kg.11 According to IMA guidelines, if a child aged 1 year or older is about to have a distressful procedure, such as laceration repair or urinary catheterization, the patient and his/her caregiver/s may be offered the option of oral midazolam.11 Only patients with an American Society of Anesthesiology score of ≤2 and a fasting time of 1 hour or more are eligible for this treatment.
ED protocol for administration of oral midazolam for minor procedures
The ED nursing staff of Ruth Children’s Hospital uses the pediatric Canadian Triage Acuity Scale (PedCTAS) to triage patients.16 The PedCTAS is a triage method that has been widely used in Canada and other countries since 2001. Using this method, patients are divided into 5 categories according to their medical condition: level 1 – patient requires immediate evaluation and care; level 2 – patient requires evaluation and care within 15 minutes; level 3 – patient requires evaluation and care within 30 minutes; level 4 – patient requires evaluation and care within 60 minutes; and level 5 – patient requires evaluation and care within 120 minutes.16 A nurse-driven protocol is used for the administration of oral midazolam prior to a procedure in children who have a PedCTAS level of 4 or 5. Any child who is 1 year old or older and is about to have a medical procedure involving a needle puncture is treated in the triage room with a topical analgesic agent; EMLA cream (Eutectic Mixture of Local Analgesics) applied to the intact skin, or LAT gel (4% lidocaine, 1:2000 adrenaline, 0.5% tetracaine) applied for laceration repair. Approximately 15 minutes before the procedure and at least 30 minutes after the LAT gel was applied (or 60 minutes after the EMLA cream was applied), the child and his/her parents are placed in one of the procedure rooms and a nurse provides an explanation of the procedure. Caregivers of children who are about to have a minor stressful procedure (such as laceration repair) are instructed by the nurse how to perform distraction of the child with the use of a mobile phone, and how to gently restrain the child on the bed. The caregivers are then offered oral midazolam and an explanation about the drug and possible adverse reactions is provided. The medication used is the intravenous solution mixed with an equal volume of raspberry juice, and the maximal single dose is 10 mg. If caregivers decline treatment for the child, the procedure is performed without midazolam. If a decision to treat with midazolam is made, an ED physician prescribes the drug and the parents are then asked to give the medication to their child. Approximately 30 minutes later, the procedure begins and the parents are asked to perform gentle restraint.17 If the procedure cannot be performed with gentle restraint (caregiver restraint), the procedure is discontinued. If a procedure is discontinued, the use of a second sedative is offered to the caregivers of patients who were treated with oral midazolam.
Study outcome measure
The primary outcome measure was the proportion of procedures completed with a single dose of oral midazolam. A failed procedure was defined as any case in which the procedure was not completed, or completed with the addition of a sedative agent after the procedure was discontinued.18
Statistical analysis
Descriptive statistics were used to describe the data and expressed in terms of frequency, percentage, mean, and standard deviation. Data were analyzed with SPSS 21 version (SPSS-IBM, Chicago, IL, USA). For the comparison of the proportion of completed procedures in the midazolam and non-midazolam groups, chi-square test was used. Multivariate regression was used to examine for potential confounders. The following variables were tested: sex, ethnicity, dosage of midazolam per weight, and type of procedure. p<0.05 was considered as significant.
Results
During the study period, 1,517 children who required a minor procedure were treated with oral midazolam as per department protocol; 13 cases were missed because of incomplete documentation, 1,467 received midazolam, and 37 declined it. Demographic characteristics are presented in Table 1. Oral midazolam was used in 14 different types of emergency procedures; the most common were urethral catheterization (33.6%), laceration repair (25.6%), and intravenous catheterization (23.6%) (Table 1). Of the 1,467 patients who received midazolam, 1,187 patients received the per protocol dose of 0.5–0.7 mg/kg, and 280 patients received higher or lower doses due to deviation from protocol (Table 1).
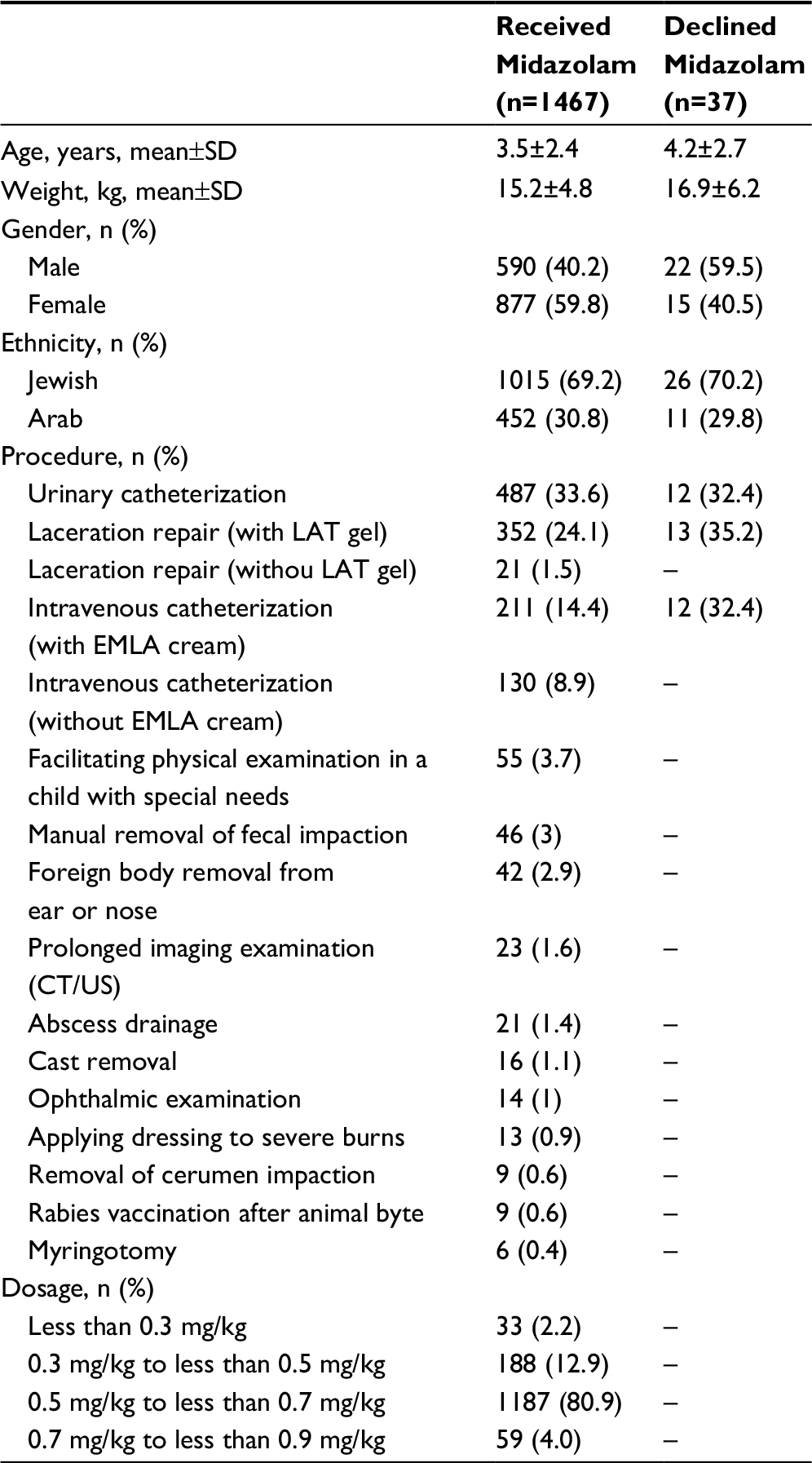 | Table 1 Patients’ characteristics Abbreviations: SD, standard deviation; CT, computerized tomography; US, ultrasound examination; LAT, lidocaine-adrenaline-tetracaine; EMLA, eutectic mixture of local analgesics. |
Procedure completion rates
Procedure completion rates in the treatment and non-treatment groups were 1,402/1,467 (95.6%) and 24/37 (64.8%), respectively (difference 30.7%; 95% confidence interval [CI] 17.3%–46.8%), p<0.0001.
Treatment group patients had procedure completion rates of 25/33 (75.8%), 165/188 (87.8%%), 1,154/1,187 (97.2%), and 58/59 (98.3%), in the less than 0.3 mg/kg group, 0.3 to less than 0.5 mg/kg group, 0.5 to less than 0.7 mg/kg group, and 0.7 to less than 0.9 mg/kg group, respectively.
Of the 1,467 patients who received midazolam, 65 (4.4%) did not complete the procedure. Five underwent urethral catheterization, 23 had a laceration repair, 16 underwent intravenous catheterization, 6 had abscess drainage, 12 had foreign body removal, 2 underwent manual removal of fecal impaction, and 1 patient had cast removal. In 59 patients, a second sedative was required to complete the procedure; intranasal midazolam in 34, intramuscular ketamine in 9, intravenous propofol in 14, and nitrous oxide inhalation in 2. In 6 cases, patients refused a second sedative (4 patients who had urethral catheterization and 2 patients who had limb lacerations).
Variables associated with failure to complete a procedure
Multivariate regression did not demonstrate an association between sex, ethnicity, midazolam dosage of 0.5 mg/kg or greater, type of procedure, and failure to complete procedure (Table 2). Midazolam in a dose of 0.3 mg/kg to less than 0.5 mg/kg was associated with an increased risk of failure to complete a procedure (adjusted odds ratio [AOR] 1.88, 95% CI 0.83–4.27; p<0.013). Midazolam in a dose of less than 0.3 mg/kg was significantly associated with an increased risk of failure to complete a procedure (AOR 8.34, 95% CI 3.32–20.9; p<0.0001) (Table 2).
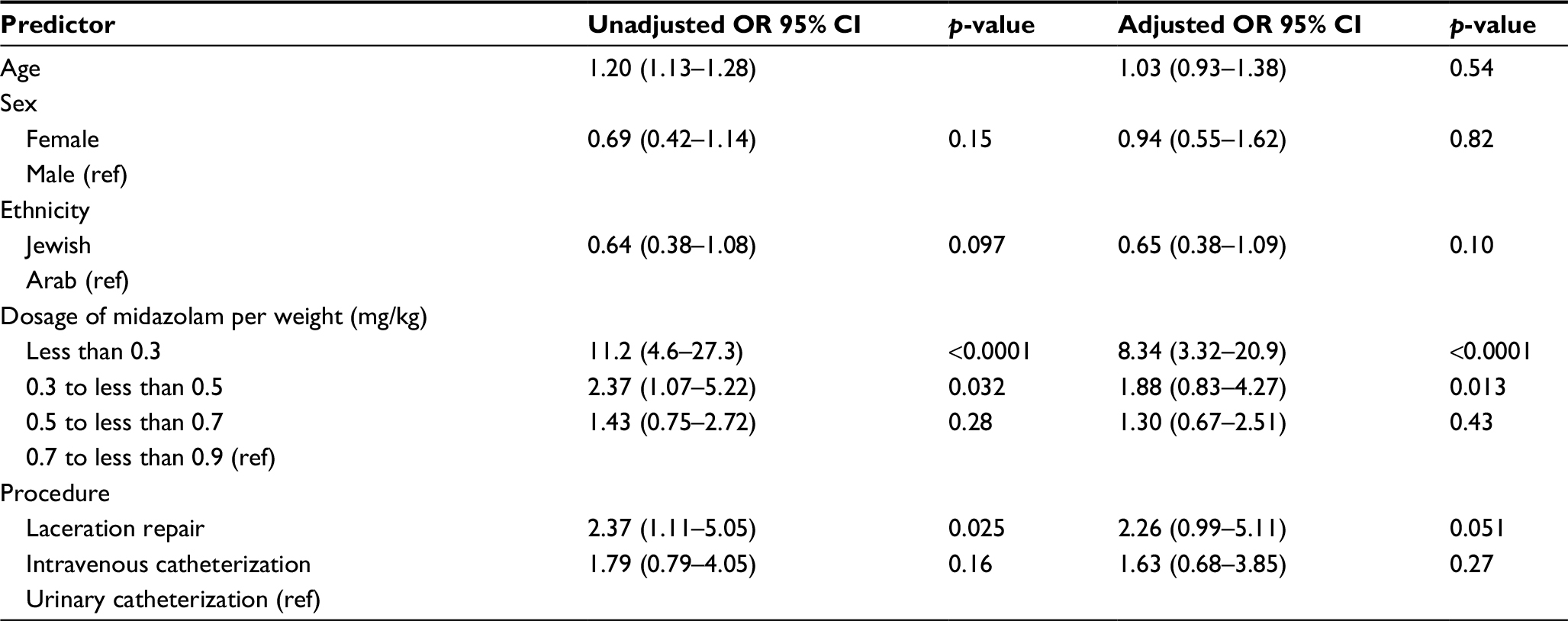 | Table 2 Results of univariate and multivariate regression of predictors of failure to complete a procedure with a single dose of oral midazolam (n=1,467) Abbreviations: OR, odds ratio; CI, confidence interval; ref, reference. |
Adverse events related to oral midazolam
Midazolam-related severe adverse events were not recorded during the study period. No patient was admitted to hospital due to an adverse event related to midazolam, and no patient returned to the ED within 24 hours due to an adverse event.
Discussion
In our cohort, oral midazolam was used in a wide variety of minor stressful procedures (Table 1). Almost all the patients in the midazolam group completed the procedures (95.6%), as opposed to approximately two-thirds of the patients who were not treated with midazolam (64.8%). These findings suggest that oral midazolam helps to facilitate the completion of stressful procedures in the ED.
Laceration repair, urethral catheterization, and intravenous catheterization accounted for 83% of the procedures. With regard to laceration repair, our search yielded only 1 study that examined the effectiveness of oral midazolam.19 In a randomized controlled trial that compared oral midazolam with oral ketamine, only 2 (6%) of the children in the midazolam arm required the addition of a second sedative to complete the procedure, as compared to 12 (32%) of the children in the ketamine arm.19 This finding supports our results as it indicates that midazolam helps to facilitate completion of this procedure. Previous studies on urethral catheterization have reported that the procedure is associated with a significant level of stress, and that oral midazolam can be helpful in these patients.13,20–23 A quasi-experimental study that assessed the effectiveness of midazolam in febrile infants undergoing urethral catheterization found that premedication with midazolam reduced the distress associated with the procedure. Patients receiving midazolam had a 53% decrease in mean visual analog scale (VAS) score when parents assessed distress (from 71.7 to 33.6) and a 48% decrease in the mean VAS score when nurses assessed distress (from 55.5 to 28.7).13 Outside the ED, most of the data on the effectiveness of oral midazolam in urethral catheterization are from the field of voiding cystourethrogram. Studies that compared 0.5–0.6 mg/kg of oral midazolam against placebo reported that midazolam was effectively used; children who received midazolam were more cooperative and tolerant than those treated with placebo.20–23 There is also a growing body of evidence suggesting that oral midazolam is effective in facilitating dental procedures in children.24,25 All together, these reports suggest that oral midazolam has the potential to facilitate completion of stressful procedures, and support our finding of a high rate of procedure completion using oral midazolam.
We found a procedure success rate of 97.2% among the 1187 patients who received a dose of 0.5 to less than 0.7 mg/kg, and a success rate of 98.3% among the 59 patients who were treated with a dose of 0.7 to less than 0.9 mg/kg. According to the multivariate regression analysis, midazolam dosage of 0.5 mg/kg or greater was not associated with procedure failure. These results seem to indicate that oral midazolam in a dose of 0.5 mg/kg or more is associated with procedure completion. Two previous studies also reported successful completion of procedures with similar doses of oral midazolam.19,25
Another important finding is that our multivariate regression revealed that a dosage of less than 0.3 mg/kg was associated with failure to complete a procedure. These results are in line with a previous study that reported that anxiety scores were no different in children receiving placebo or oral midazolam in a dose of 0.3 mg/kg.26 These findings suggest that the IMA protocol is not suited for children who weigh more than 30 kg, because the maximal dose of 10 mg (per protocol) results in a dosage of less than 0.3 mg/kg.
Midazolam-related severe adverse events were not found in our study. Future large prospective studies are warranted to confirm the safety of this treatment.
This study has several limitations. Firstly, this is a single-center study; therefore, the results may not be generalizable. Secondly, the study has limitations inherent in a retrospective chart review, including dependence on the quality of documentation; thus, we had no data regarding the sedative state of the child during the procedure or the length of each procedure because these parameters were not recorded. In children who were more cooperative, it is possible that using nitrous oxide would have yielded a shorter procedure time. Thirdly, only patients who required evaluation and care within 60 minutes or more (triage category 4 or 5) were included in the study. Our results may not apply to patients who require more urgent care. Fourthly, we were not able to provide information on non-severe adverse events, such as paradoxical reaction, vomiting, or over-sedation because these data were not recorded systematically in patients’ charts. Finally, midazolam was offered to all caregivers of the patients based on department protocol. We do not believe that declining midazolam represents a bias toward decision to discontinue procedures.
Conclusion
The results of this cohort study suggest that oral midazolam helps to facilitate completion of stressful procedures in the ED. Our findings show that midazolam in a single dose of 0.5 mg/kg or greater is associated with successful completion of ED procedures in children.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
American Academy of Paediatrics. Committee on Psychosocial Aspects of Child and Family Health; Task Force on Pain in Infants, Children and Adolescents. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001;108(3):793–797. | ||
Godwin SA, Burton JH, Gerardo CJ, et al; American College of Emergency Physicians. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63(2):247–258. | ||
Pacheco GS, Ferayorni A. Paediatric procedural sedation and analgesia. Emerg Med Clin North Am. 2013;31(3):831–852. | ||
Brosius KK, Bannister CF. Midazolam premedication in children: a comparison of two oral dosage formulations on sedation score and plasma midazolam levels. Anesth Analg. 2003;96(2):392–395. | ||
Khalil SN, Vije HN, Kee SS, Farag A, Hanna E, Chuang AZ. A paediatric trial comparing midazolam/Syrpalta mixture with premixed midazolam syrup (Roche). Paediatr Anaesth. 2003;13(3):205–209. | ||
Srivastava B, Mittal N, Mittal P. Acceptability and efficacy of commercial oral preparation of midazolam for brief painful procedure: a randomised double blind clinical trial. Int J Clin Pediatr Dent. 2014;7(3):153–156. | ||
Salem K, Khoshrang H, Kousha M, et al. Efficacy and safety of orally administered intravenous midazolam versus a commercially prepared syrup. Iran J Pediatr. 2015;25(3):e494. | ||
Somri M, Parisinos CA, Kharouba J, et al. Optimising the dose of oral midazolam sedation for dental procedures in children: a prospective, randomised, and controlled study. Int J Paediatr Dent. 2012;22(4):271–279. | ||
Salem K, Kamranzadeh S, Kousha M, Shaeghi S, AbdollahGorgi F. Two oral midazolam preparations in paediatric dental patients: a prospective randomised clinical trial. Int J Pediatr. 2015;2015:349795. | ||
Conway A, Rolley J, Sutherland JR. Midazolam for sedation before procedures. Cochrane Database Syst Rev. 2016;5:CD009491. | ||
Shavit I, Augarten A, Efrat R, Hershman E, Zimerman D, Kozer E, et al. Approach to pain and anxiety in the pediatric emergency department (Hebrew). 2010 Israel Medical Association. Available from: http://www.ima.org.il/Ima/FormStorage/Type7/clinical_52_pain.pdf. Accessed October 19, 2017. | ||
Shavit I, Feraru L, Miron D, Weiser G. Midazolam for urethral catheterisation in female infants with suspected urinary tract infection: a case-control study. Emerg Med J. 2014;31(4):278–280. | ||
Weiser G, Cohen D, Krauss B, Galbraith R, Shavit I. Premedication with midazolam for urethral catheterisation of febrile infants. Eur J Emerg Med. 2014;21(4):314–318. | ||
Kaji AH, Schriger D, Green S. Looking through the retrospectoscope: reducing bias in emergency medicine chart review studies. Ann Emerg Med. 2014;64(3):292–298. | ||
Shavit I, Bar-Yaakov N, Grossman L, Weiser G, Edry R, Steiner IP. Sedation for children with intraoral injuries in the emergency department: a case-control study. Pediatr Emerg Care. 2014;30(11):805–807. | ||
Gravel J, Fitzpatrick E, Gouin S, et al. Performance of the Canadian Triage and Acuity Scale for children: a multicentre database study. Ann Emerg Med. 2013;61(1):27–32. | ||
Feld LH, Negus JB, White PF. Oral midazolam preanesthetic medication in paediatric outpatients. Anesthesiology. 1990;73(5):831–834. | ||
Lane RD, Schunk JE. Atomized intranasal midazolam use for minor procedures in the paediatric emergency department. Pediatr Emerg Care. 2008;24(5):300–303. | ||
Rubinstein O, Barkan S, Breitbart R, et al. Efficacy of oral ketamine compared to midazolam for sedation of children undergoing laceration repair: a double-blind, randomised, controlled trial. Medicine (Baltimore). 2016;95(26):e3984. | ||
Ferguson GG, Chen C, Yan Y, et al. The efficacy of oral midazolam for decreasing anxiety in children undergoing voiding cystourethrogram: a randomised, double-blind, placebo controlled study. J Urol. 2011;185:2542–2546. | ||
Herd DW, McAnulty KA, Keene NA, Sommerville DE. Conscious sedation reduces distress in children undergoing voiding cystourethrography and does not interfere with the diagnosis of vesicoureteric reflux: a randomised controlled study. AJR Am J Roentgenol. 2006;187(6):1621–1626. | ||
Sorkhi H, Bakhshandeh-Bali MK, Nooreddini HG. Randomised clinical trial of sedation with oral midazolam for voiding cystourethrography in children. Med J Isl Rep Iran. 2010;24:67–71. | ||
Azarfar A, Esmaeeili M, Farrokh A, et al. Oral midazolam for voiding dysfunction in children undergoing voiding cystourethrography: a controlled randomised clinical trial. Nephrourol Mon. 2014;6(3):e17168. | ||
Lourenço-Matharu L, Ashley PF, Furness S. Sedation of children undergoing dental treatment. Cochrane Database Syst Rev. 2012;3:CD003877. | ||
Peretz B, Kharouba J, Somri M. A comparison of two different dosages of oral midazolam in the same paediatric dental patients. Pediatr Dent. 2014;36(3):228–232. | ||
Anderson BJ, Exarchos H, Lee K, Brown TC. Oral premedication in children: a comparison of chloral hydrate, diazepam, alprazolam, midazolam and placebo for day surgery. Anaesth Intensive Care. 1990;18(2):185–193. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.