Back to Journals » Infection and Drug Resistance » Volume 19
Single Daily versus Multiple-Daily Sputum Cultures for Guiding Antibiotic Therapy in ICU Patients with Pulmonary Infections: A Retrospective Cohort Study
Authors Wang JY, Liu Z, Xia QC, Chu WW ![]() , Liang DY, Huang YM, Jia XL, Yu WL
, Liang DY, Huang YM, Jia XL, Yu WL ![]() , Xia FP, Sun Y, Lu ZH
, Xia FP, Sun Y, Lu ZH
Received 30 September 2025
Accepted for publication 19 January 2026
Published 22 January 2026 Volume 2026:19 567559
DOI https://doi.org/10.2147/IDR.S567559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Ji-Yun Wang,1,2,* Zhi Liu,1,* Qian-Cheng Xia,1 Wen-Wen Chu,3 Dai-Yun Liang,1 You-Ming Huang,2 Xue-Li Jia,1 Wei-Li Yu,1 Fei-Ping Xia,4 Yun Sun,1 Zhong-Hua Lu1,*
1The First Department of Critical Care Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Wannan Medical College, Wuhu, Anhui Province, People’s Republic of China; 3Department of Clinical Laboratory, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 4Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhong-Hua Lu, The First Department of Critical Care Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China, Email [email protected] Yun Sun, The First Department of Critical Care Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China, Email [email protected]
Background: Effective antibiotic management is crucial for ICU patients with pulmonary infections. However, guidelines are unclear whether the optimal strategy is multiple cultures on the infection onset day or a single daily culture to guide antibiotic therapy.
Methods: This study involved 362 ICU patients with confirmed pulmonary infections, categorized into a “multiple-daily” group (≥ 2 cultures within 24 hours) and a “once-daily” group (1 culture per 24 hours). Propensity score matching was used to balance baseline characteristics. Primary outcome was antibiotic adjustment rate. Secondary outcomes included mechanical ventilation duration, ICU and total hospital length of stay, hospitalization costs, and mortality.
Results: The multiple-daily group had more frequent antibiotic adjustments both before and after matching (76.88% vs 67.33%, p = 0.048 pre-matching; p = 0.076 post-matching). The once-daily group experienced significantly shorter durations of mechanical ventilation (pre: 119.50 vs 159.50 hours; post: 116.00 vs 156.00 hours; both p < 0.001), ICU stay (pre: 10.00 vs 13.00 days; post: 9.00 vs 13.00 days; both p < 0.001), and lower hospitalization costs (pre: 138,150 vs 167,910 CNY, p = 0.011; post: 136,870 vs 167,780 CNY, p = 0.004). The hospital stay was also shorter in the once-daily group, with similar mortality rates between groups. Common multidrug-resistant pathogens included CRAB (32.52%), MRSA (24.39%), ESBL (18.70%), CRPA (15.45%), and CRE (12.00%). The multiple-daily group had higher detection rates of CRAB (38.46% vs 25.86%, p= 0.050) and MRSA (30.77% vs 17.24%, p= 0.048), with more frequent antibiotic adjustments, especially in multidrug-resistant cases (87.69% vs 70.69%, p= 0.019).
Conclusion: In ICU patients with pulmonary infections, multiple-daily sputum cultures lead to more frequent antibiotic adjustments and better detection of multidrug-resistant pathogens. However, a once-daily culture strategy is associated with reduced healthcare resource utilization and comparable mortality. Further randomized trials are needed to determine the optimal sputum culture frequency in the ICU setting.
Trial Registration: This study was registered with the Chinese Clinical Trial Registry under the registration number ChiCTR2400091085.
Keywords: antibiotic management, pulmonary infections, sputum culture frequency, multidrug-resistant, propensity score matching
Introduction
Pulmonary infections are a leading cause of ICU mortality, causing 20% of deaths.1 In intensive care unit (ICU) patients, these infections often escalate to severe respiratory failure and sepsis (68.2%), significantly increasing morbidity, mortality, and healthcare costs.2–4 ICU patients are especially susceptible to infections due to complex health conditions and frequent immunosuppression,5 impacting both short-term prognosis and long-term quality of life.6,7 The presence of multidrug-resistant (MDR) bacteria, coupled with the need for personalized treatment, makes infection management in ICU challenging, prolonging hospital stays and increasing healthcare resource demands.8,9 Rapid, accurate pathogen detection is thus essential for effective antibiotic stewardship and improving outcomes.
Within the spectrum of pulmonary infections affecting patients in the ICU, ICU-acquired pneumonia, particularly ventilator-associated pneumonia, presents a distinct diagnostic challenge due to its unique pathophysiology.10 The primary difficulty stems from a triad of mechanisms: endotracheal intubation disrupts airway defenses, critical illness induces immune dysfunction, and the combination of broad-spectrum antibiotics with the ICU environment fosters colonization by multidrug-resistant organisms.10 This situation complicates the differentiation between colonization and true infection in respiratory specimens, thereby undermining the reliability of single, static sputum cultures for guiding antimicrobial therapy. Consequently, although sputum cultures remain a fundamental diagnostic tool in the management of pulmonary infections in the ICU—providing pathogen detection comparable to next-generation sequencing (NGS)11 and aligning well with bronchoalveolar lavage fluid for targeted treatment—they are inherently constrained by these pathophysiological factors.12 Nonetheless, timely culturing can aid in preventing misdiagnosis, optimizing antibiotic use, reducing the overuse of broad-spectrum antibiotics, and mitigating the risk of MDR bacteria infections.13
Despite its significance, there is a notable absence of definitive guidelines regarding the optimal frequency of sputum cultures in ICU settings. This ambiguity arises from a clinical conundrum. On one hand, conducting a single daily culture is efficient and conserves resources. On the other hand, various clinical imperatives may compel clinicians to procure multiple cultures within a brief period.14,15 These imperatives include: (1) enhancing diagnostic yield and confirming pathogen persistence when initial empiric therapy proves ineffective, as a solitary negative culture does not definitively exclude infection in a patient;16 (2) distinguishing true infection from airway colonization or contamination by assessing the consistency of pathogen recovery across multiple samples;17 (3) identifying the emergence of new or resistant pathogens during treatment, which is crucial for the timely adjustment of antibiotic regimens in patients whose conditions are deteriorating;18 and (4) obtaining sufficient specimens for complex microbiological analyses when initial samples are inadequate.19 Determining the ideal culture frequency is critical to balancing diagnostic accuracy, resource allocation, and patient outcomes in ICU pulmonary infection management.
Current ATS and IDSA guidelines only recommend repeated cultures for the Mycobacterium avium complex (MAC) in case of recurring symptoms,20,21 leaving a gap in evidence for routine infections. This study aims to bridge the gap by directly comparing the effects of single versus multiple sputum cultures on antibiotic management, ICU and hospital stay, ventilation duration, mortality, and healthcare costs. Our findings offer evidence-based insights to refine antibiotic strategies, optimize resource use, and ultimately improve outcomes for ICU patients with pulmonary infections.
Methods
Study Population and Setting
We included consecutive adult patients admitted to the surgical ICU at the Second Affiliated Hospital of Anhui Medical University between January 1, 2022 and December 31, 2023. This ICU provides comprehensive monitoring and treatment, including vital signs monitoring (such as electrocardiogram, oxygen saturation, blood pressure, respiratory rate, and body temperature), invasive monitoring (such as arterial blood pressure, central venous pressure, and hourly urine output), and mechanical ventilation support. The patient population included individuals from internal medicine, emergency surgery, general surgery, neurosurgery, cardiovascular surgery, and trauma.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Second Affiliated Hospital of Anhui Medical University (Approval No. YX2024-158). The study was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2400091085). Written informed consent was obtained from all participants or their legal representatives.
Study Design and Data Source
This was a retrospective cohort study conducted using data extracted from the hospital’s electronic medical records and laboratory information system. All clinical and microbiological data were generated during the routine care of patients. Consequently, while sputum cultures were processed according to standard laboratory protocols, the decision to send a specimen for culture and the prior assessment of sputum quality (eg, via Gram stain) were at the discretion of the treating clinical team, reflecting real-world practice rather than a prospective research protocol.
Patient Selection
In the laboratory management system at the Second Affiliated Hospital of Anhui Medical University, all eligible sputum cultures with etiological results were recorded by laboratory physicians. Two independent reviewers examined these records to ensure that they met the criteria for positive sputum culture results, resolving any discrepancies through discussion. Information such as the patient’s name, number of admissions, number of sputum cultures, and etiological findings was extracted. Two ICU staff members subsequently screened and verified this information using the hospital’s patient management system, recording the number of sputum cultures collected when pulmonary infection or its exacerbation was suspected. The inclusion criteria encompassed the following: fulfillment of the diagnostic criteria for either community-acquired or hospital-acquired pneumonia (including ventilator-associated pneumonia),22,23 positive sputum culture results, necessity for invasive mechanical ventilation, and an age threshold of 18 years or older. The exclusion criteria comprised cases with incomplete or missing essential information in medical records, unauthorized cases or those not conforming to ethical review standards, and patients with multiple admissions during the study period; only the initial ICU admission was considered for analysis, with any subsequent admissions being excluded.
Exposure
This retrospective cohort study was conducted on ICU patients with microbiologically confirmed pulmonary infections at the Second Affiliated Hospital of Anhui Medical University. Eligible sputum cultures with etiological results were documented in the laboratory management system by laboratory physicians, with two independent reviewers verifying each record for positive culture criteria and resolving any discrepancies through discussion. The extracted information included patient identifiers, admission details, sputum culture frequency, and etiological findings. The ICU staff further validated these data using the hospital’s patient management system, recording the number of sputum cultures performed when a pulmonary infection or its exacerbation was suspected. Patients were divided based on sputum culture frequency before antibiotic initiation or adjustment: the “once-daily” group included patients with one culture collected within a 24-hour period under clinical suspicion of new or worsening infection, either as a single instance or repeated over several days; the “multiple-daily” group included patients with at least two cultures taken within the same 24-hour period at intervals exceeding 8 hours, not both cultures necessarily having to be positive. Sputum samples obtained through endotracheal or tracheostomy tubes were processed for microbiological analysis. Samples were inoculated onto solid culture media: Columbia blood agar for general cultivation, bacterial quantification, and isolation of Staphylococcus aureus; MacConkey agar for the isolation and preliminary identification of Gram-negative bacilli. Following incubation, isolated colonies were purified and identified to the species level using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Antibiotic susceptibility testing was performed using the VITEK 2 Compact automated system (bioMérieux, France). The minimum inhibitory concentration (MIC) method was employed to ascertain the lowest concentration of the drug required to inhibit bacterial growth.
Baseline Characteristics
Baseline characteristics included age at ICU admission, sex, chronic health score (which includes the presence of severe organ dysfunction or immunosuppression), surgical status, type of surgery (emergency or elective), Glasgow Coma Scale (GCS) score, body temperature, mean arterial pressure (MAP), heart rate, respiratory rate, partial pressure of oxygen, arterial blood pH, serum sodium concentration, serum potassium concentration, serum creatinine, hematocrit, white blood cell count, and Acute Physiology and Chronic Health Evaluation II (APACHE II) score. The chronic health score encompasses severe conditions such as chronic renal failure, chronic liver disease, congestive heart failure, chronic obstructive pulmonary disease, and any form of immunosuppression, including those caused by chemotherapy, long-term steroid use, or underlying diseases such as HIV/AIDS.
Endpoints
The primary endpoint was the rate of antibiotic adjustments, defined as switching to a new antibiotic or adding a new one to the existing regimen based on culture results. Secondary endpoints included the duration of mechanical ventilation, ICU stay, length of hospital stays, hospitalization costs, and mortality rates. Given the increasing emergence of MDR pathogens, post-hoc analyses for efficacy endpoints were conducted in patients infected by MDR pathogens. The impact of sputum culture frequency on antibiotic adjustments was assessed using multivariable logistic regression analysis. In the pre-matched cohort, the rate of antibiotic adjustments was compared between the single sputum culture group and the multiple sputum culture group. After propensity score matching, differences between the two groups were further evaluated. Chi-square tests were used to compare the prevalence of MDR pathogens, including carbapenem-resistant Acinetobacter baumannii (CRAB), methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamase (ESBL), carbapenem-resistant Enterobacteriaceae (CRE), and carbapenem-resistant Pseudomonas aeruginosa (CRPA). In non-MDR patients, antibiotic adjustment rates were also compared between the two groups. A bubble chart was used to visually display the distribution of MDR pathogens, group allocation, and the frequency of each MDR acquisition per patient, highlighting the differences in MDR pathogen prevalence and antibiotic utilization patterns between the groups.
Statistical Analysis
Continuous variables with a normal distribution are expressed as the means ± standard deviations (SDs) and were compared between groups using the independent-samples t test. Continuous variables with a skewed distribution are presented as the medians (IQRs) and were compared between groups using the Mann–Whitney U-test. Categorical variables are expressed as counts and percentages, with group differences examined using the Fisher’s exact test or chi-square test. To explore the relationship between the frequency of sputum culture and pulmonary infection outcomes, we employed propensity score matching (PSM) using nearest neighbor matching with a caliper size of 0.25. The treatment and control groups were matched at a 1:1 ratio.24 To assess the effectiveness of PSM in balancing the groups, we calculated the standardized mean difference (SMD). We utilized multivariate Cox regression to investigate the association between the frequency of sputum cultures and in-hospital mortality, with potential confounders selected based on p-values < 0.05 in univariate analysis and the clinical expertise of our team. Finally, we conducted linear regression analysis to evaluate the correlation between the frequency of sputum culture and the duration of ICU stay, hospital stay, and mechanical ventilation. Data processing and analysis were performed using R software (version 4.4.0), with a p-value of < 0.05 considered the threshold for statistical significance.
Results
From January 1, 2022 to December 31, 2023, a total of 2411 patients were newly admitted to the ICU. Among them, 563 patients had sputum cultures collected due to pulmonary infections or worsening pulmonary conditions. After 168 patients with negative sputum cultures were excluded, 395 patients had positive sputum culture results. Following the exclusion of 30 patients with a duration of mechanical ventilation of less than 2 days, 2 patients aged under 18 years, and 1 patient with an ICU stay of less than 2 days, a total of 362 patients were included in the final analysis, as shown in Figure 1.
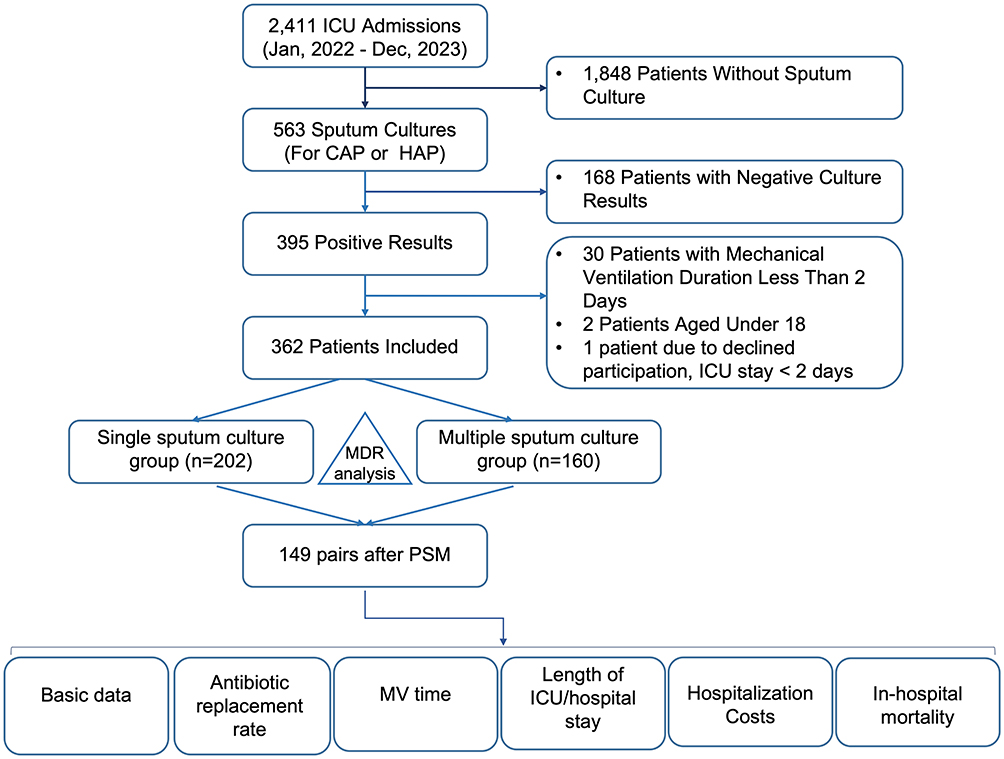 |
Figure 1 Flowchart of the included patients. |
Demographic Characteristics of Cases
As shown in Table 1, this study included 160 patients in the multiple sputum culture group and 202 patients in the single sputum culture group (including 170 patients with daily cultures for more than 2 consecutive days). The median age of patients in the multiple sputum culture group was 59 years (IQR: 50, 69.25), whereas the median age of patients in the single sputum culture group was 58 years (IQR: 45, 69.75). In the multiple sputum culture group, 113 patients (70.62%) were male, whereas in the single sputum culture group, 145 patients (71.78%) were male. Additionally, 13 patients (8.12%) in the multiple sputum culture group had a history of severe organ dysfunction or impaired immune function. In the single sputum culture group, 20 patients (9.90%) had a history of severe organ dysfunction or impaired immune function.
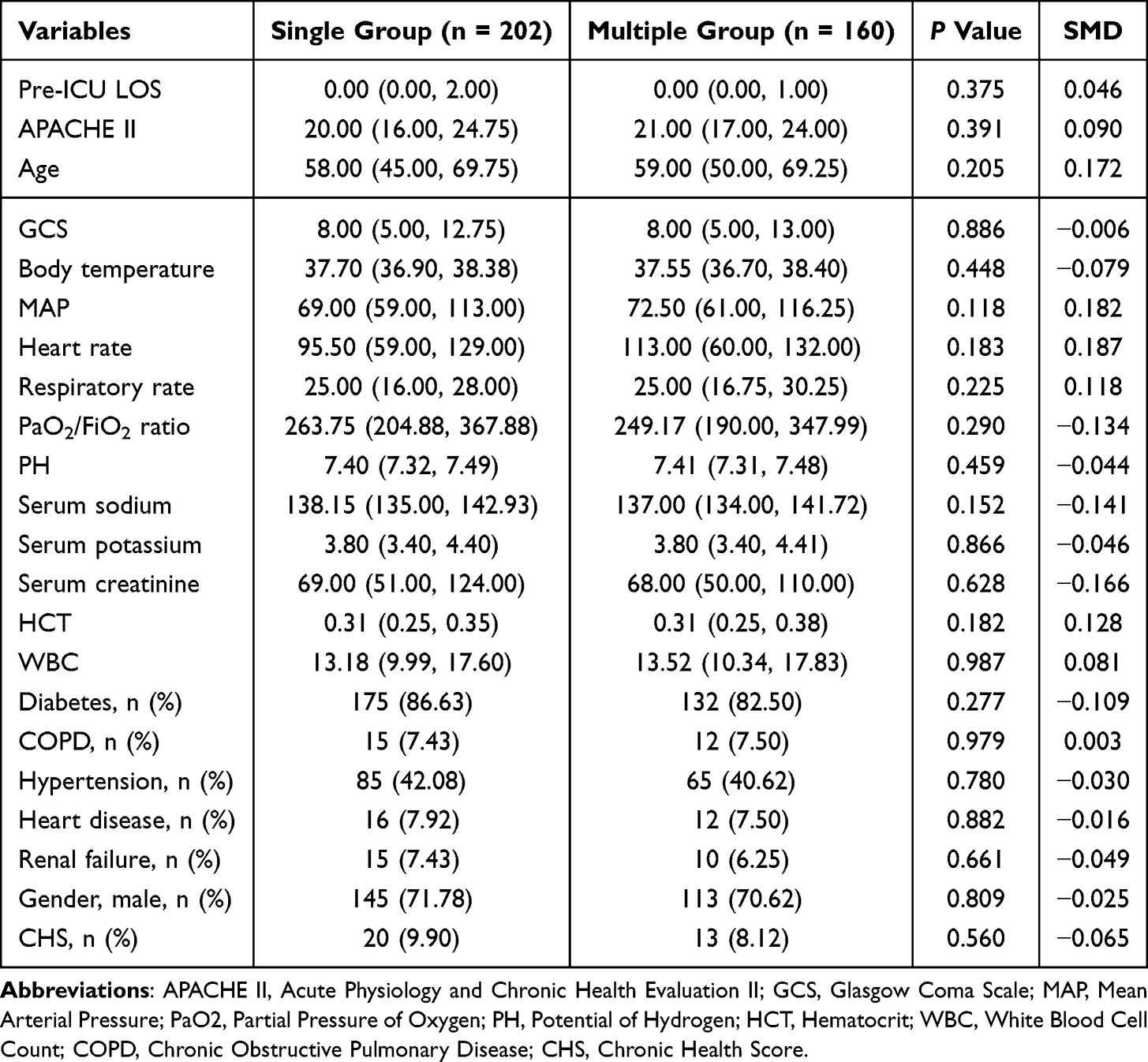 |
Table 1 Basic Characteristics Between Groups Before PSM |
Comparison of Patient Characteristics
To assess differences in disease characteristics and severity affecting prognosis, we compared ICU admission age, sex, chronic health score, surgical status and type, GCS score, body temperature, vital signs, blood gas levels, electrolyte concentrations, hematocrit, white blood cell count, and APACHE II score (details provided in Table 1). This study revealed no significant differences in the indicators. The APACHE II score was 20.00 for the single sputum culture group and 21.00 for the multiple sputum culture group, suggesting severe illness with an expected 40% mortality rate. However, the actual mortality rate at our center was 14.64%, which was lower than expected.
Impact of Sputum Culture Frequency on Antibiotic Adjustments and MDR Pathogens
The influence of sputum culture frequency on antibiotic adjustments was analyzed using multivariable logistic regression. In the pre-matched cohort, the single sputum culture group exhibited a lower rate of antibiotic adjustments (67.33%) compared to the multiple sputum culture group (76.88%, p =0.048), as shown in Table S1, Table 2 and Figure 2, with a small effect size (φ=0.105). Post-propensity score matching, this trend continued, though the difference was no longer statistically significant (p =0.076). The multiple culture group showed 1.61-fold higher odds (OR=1.61) and 14% greater relative risk (RR=1.14) of antibiotic adjustments compared to the single culture group.
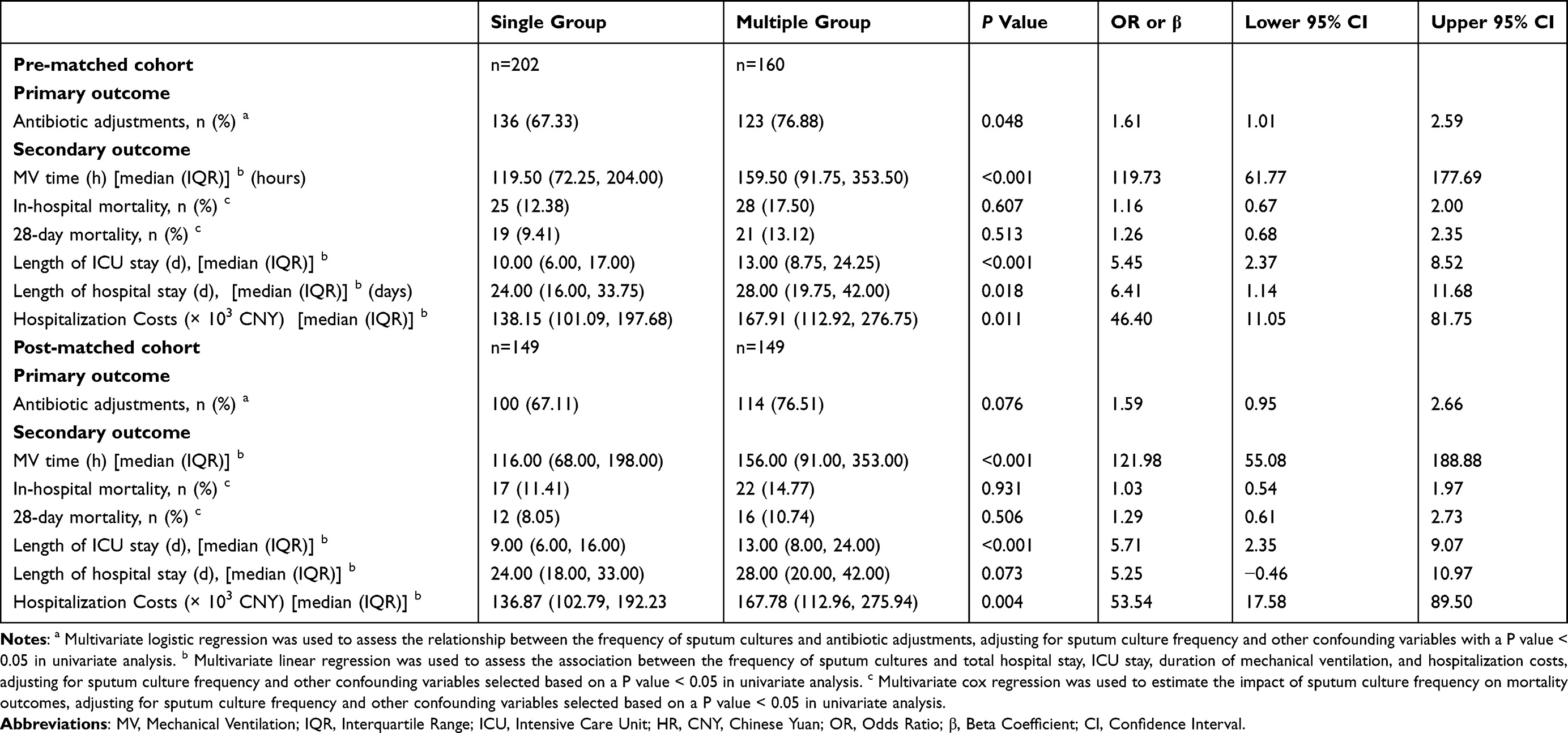 |
Table 2 Association Between Sputum Culture Frequency and Clinical Outcomes in Patients with Pulmonary Infection |
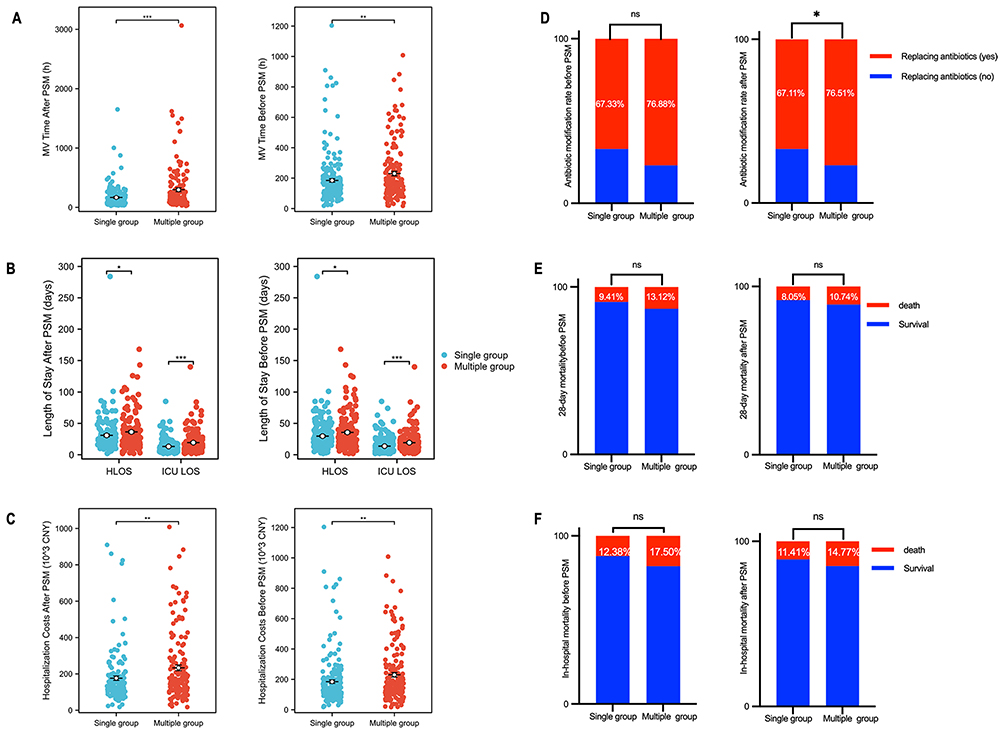 |
Figure 2 Clinical outcomes comparison between single versus multiple sputum culture groups. (A) Mechanical ventilation (MV) duration (hours) between single and multiple sputum culture groups. (B) Comparison of ICU length of stay (days) and total hospitalization duration (days). (C) Total hospitalization costs (103 CNY) between groups. (D) Antibiotic change rates (%) during hospitalization. (E) In-hospital mortality rates (%) comparison. (F) 28-day mortality rates (%) post-admission. *p < 0.05, **p < 0.01, and ***p < 0.001 versus the single culture group; (p ≥ 0.05). Abbreviation: ns, not significant. Note: These are univariate comparisons; see Table 2 for multivariate analysis. |
Chi-square tests further revealed that the multiple sputum culture group had a significantly higher rate of antibiotic adjustments (76.88% vs 67.33%, p =0.046), with a more pronounced difference among MDR cases (87.69% vs 70.69%, p =0.019). MDR pathogens were more prevalent in the multiple group (40.62% vs 28.71%, p =0.017), particularly CRAB (38.46% vs 25.86%, p =0.050) and MRSA (30.77% vs 17.24%, p =0.048), as detailed in Table 3. Additionally, chi-square analyses indicated a significant difference in MRSA detection rates between the two groups when considering the entire study population: the multiple sputum culture group showed a higher detection rate of 12.50% compared to 4.95% in the single sputum culture group (χ2=10.53, p=0.0012). This result, which further confirms the presence of differences in MRSA between the groups. ESBL, CRE, and CRPA also showed higher rates in the multiple group, but these differences were not statistically significant (ESBL: p =0.100; CRE: p =0.190; CRPA: p =0.140). Among non-MDR patients, antibiotic adjustment rates did not differ significantly between the groups (65.97% vs 69.47%, p =0.572). Figure 3, a bubble chart, visually supports these findings by illustrating the distribution of MDR pathogens, group allocation, and the frequency of each MDR acquisition per patient. This visualization highlights the large reaction of the same resistant bacteria, further emphasizing the differences in MDR pathogen prevalence and antibiotic utilization patterns between the groups.
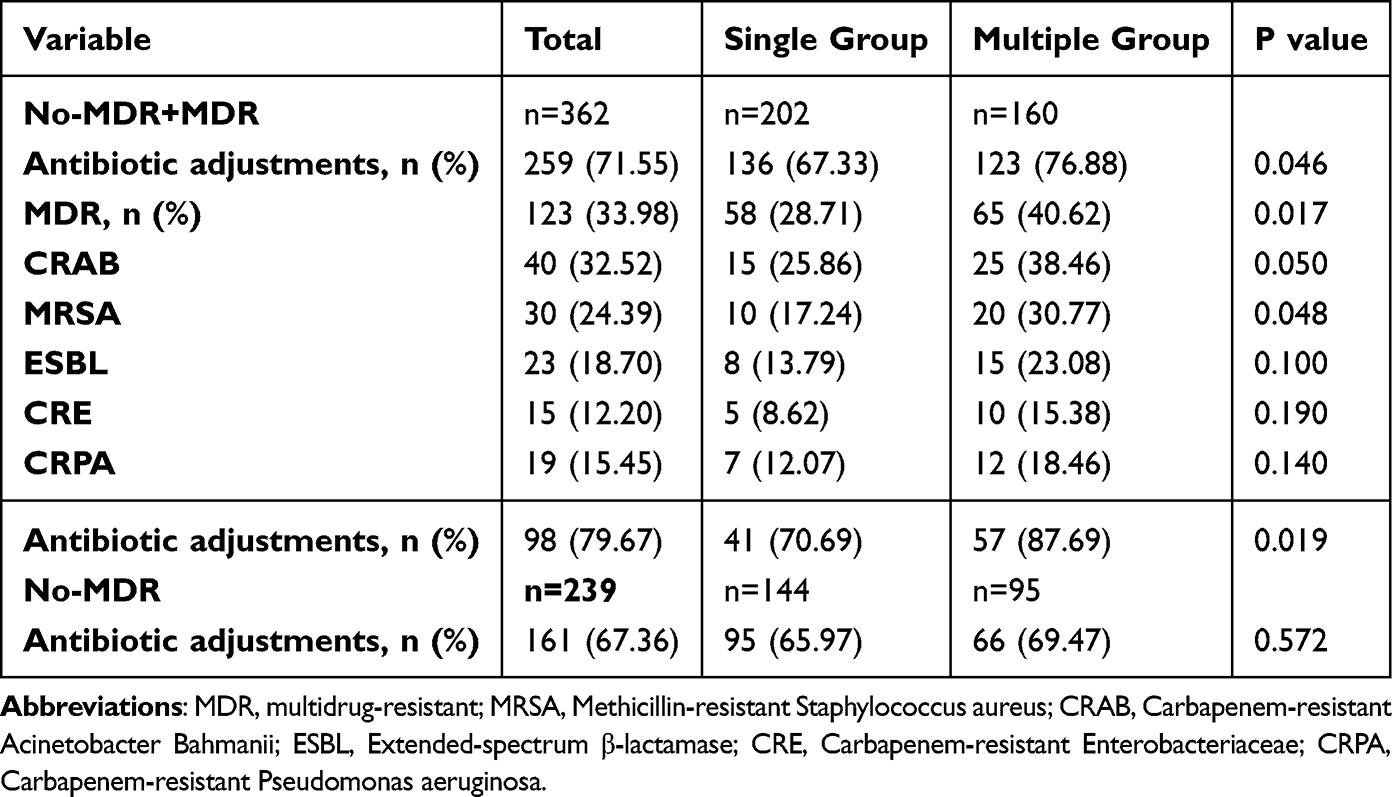 |
Table 3 Comparison of MDR and Antibiotic Adjustments Between Groups |
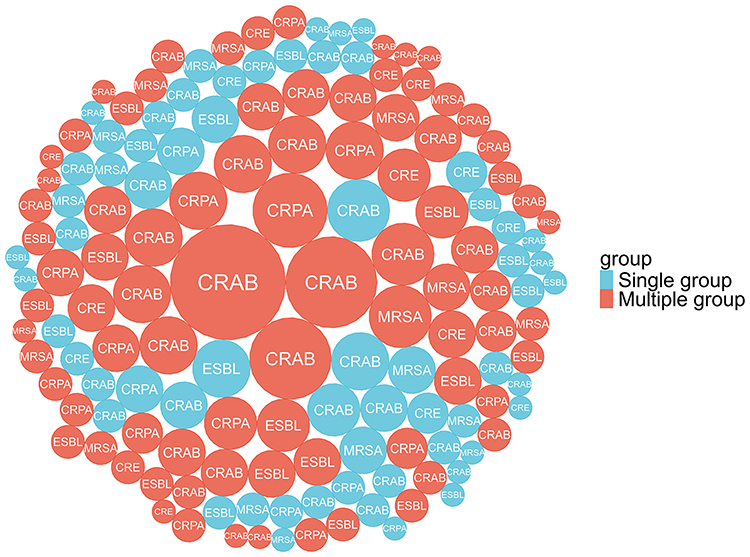 |
Figure 3 Distribution of MDR Pathogens and Frequency of Acquisition per Patient: This bubble chart illustrates the distribution of multidrug-resistant (MDR) pathogens between the single sputum culture group and the multiple sputum culture group. The size of each bubble represents the frequency of acquisition of the same MDR pathogen per patient. Larger bubbles indicate higher frequencies of the same resistant bacteria. |
Sensitivity Analysis: Impact of Considering Only the First Positive Culture
To isolate the effect of the sampling protocol itself from the initial diagnostic yield, a sensitivity analysis was conducted by considering only the first positive culture for each unique pathogen per patient. This conservative method evaluates MDR prevalence based solely on initial microbiological findings. When applying this stringent criterion, the prevalence of MDR pathogens in the multiple sputum culture group decreased substantially from 40.6% (65/160) to 21.3% (34/160). In contrast, the rate in the single sputum culture group remained unchanged at 28.7% (58/202), as this group had only one culture per patient by definition. The difference in MDR prevalence between the groups was no longer statistically significant (21.3% vs 28.7%, χ2=2.62, p=0.105). This analysis indicates that the higher MDR prevalence originally observed in the multiple culture group was largely attributable to the repeated sampling protocol itself, which increased the cumulative probability of detecting MDR pathogens over time. Approximately 47.7% (31/65) of the MDR patients in the multiple group were identified only through subsequent cultures after an initial culture without that specific MDR pathogen.
Relationship Between the Frequency of Sputum Culture and Patient Outcomes
Linear regression is employed to ascertain the quantitative interdependence among two or more variables. In the pre-matched cohort, the duration of mechanical ventilation was significantly shorter in the single sputum culture group than in the multiple sputum culture group, with durations of 119.50 hours (IQR, 72.25, 204.00) versus 159.50 hours (IQR, 91.75, 353.50) (p < 0.001), as detailed in Figure 2 and Table S3. Additionally, the length of hospital stay was shorter in the single sputum culture group, with an average of 24.00 days (IQR, 16.00, 33.75), than in the multiple sputum culture group, with an average of 28.00 days (IQR, 19.75, 42.00) (p =0.018), as illustrated in Table S4. Furthermore, the duration of ICU stay was significantly shorter in the single sputum culture group, with a median of 10.00 days (IQR, 6.00–17.00), than in the multiple sputum culture group, which had a median of 13.00 days (IQR, 8.75–24.25) (p <0.001), as detailed in Table S5. However, it is important to note that the frequency of sputum culture was not correlated with in-hospital mortality or 28-day mortality, as shown in TableS 2, S6 and S7. These results were obtained after adjusting for potential confounding variables.
For PSM, 149 patients with a single sputum culture were matched with 149 patients with multiple cultures. Table S8 compares their characteristics, showing all standardized mean differences (SMDs) for all variables were less than 10%, indicating well-balanced baseline characteristics (see Table S8, Figure 2 and S1, and Figure S2). Consistent with the pre-matching model results, a single sputum culture was associated with a shorter duration of mechanical ventilation (median: 116 hours vs 156 hours) and a reduced length of stay (LOS) in the intensive care unit (median: 9 days vs 13 days), with statistically significant results (p < 0.001), as presented in Tables S9 and S10. Furthermore, there was an observed trend towards shorter overall hospital stays (median: 24 days vs 28 days; p = 0.073), as indicated in Table S12; however, no significant association was identified with in-hospital mortality (11.41% vs 14.77%; p = 0.931) or 28-day mortality (8.05% vs 10.74%; p = 0.506), as shown in Table S13.
Hospitalization Cost Results
The total medical expenses for patients in the pre-matched single sputum culture group were 138,150 CNY (IQR, 101,090.40, 197,680.96) compared with 167,910.20 CNY (IQR, 112,924.62, 276,750.66) in the multiple sputum culture group (p = 0.011), as detailed in Tables S14 and 2. After PSM, the total medical expenses for patients in the single sputum culture group were 136,870 CNY (IQR, 102,790, 192,230), whereas those in the multiple sputum culture group were 167,780 CNY (IQR, 112,960, 275,940) (p = 0.004), as shown in Figure 2, Tables S15 and 2. These results indicate that the total costs remained consistently lower in the single sputum culture group than in the multiple sputum culture group before and after matching.
Discussion
Pulmonary infections in ICU patients are prevalent and pose serious risks, often leading to respiratory failure, septic shock, multi-organ failure, and prolonged hospital stays, all of which can worsen patient outcomes.1,3–5,25 Sputum culture remains a straightforward and cost-effective diagnostic tool, facilitating accurate pathogen identification and guiding targeted antibiotic therapy to help prevent resistance.12 This study compared single and multiple sputum culture frequencies in ICU patients with confirmed pulmonary infections and revealed that multiple daily cultures are associated with more frequent antibiotic adjustments, likely due to enhanced detection of resistant or unexpected pathogens. However, single daily cultures are associated with shorter mechanical ventilation duration, ICU stays, and lower hospitalization costs without compromising in-hospital or 28-day mortality rates. These findings underscore a key dissociation: increased diagnostic yield from repeated sampling did not translate into improved patient outcomes, challenging the routine practice of multiple cultures. These findings provide practical guidance for optimizing sputum culture frequency in ICU settings, balancing the benefits of frequent cultures for antibiotic precision with efficient resource use.
Our study revealed that the single and multiple sputum culture groups generally presented consistent baseline characteristics, with minor differences in the MAP and heart rate. To adjust for these imbalances, we used multivariate regression and propensity score matching (PSM) to create comparable groups. Both groups had a median GCS score of 8 and an APACHE II score of approximately 20, underscoring the high severity in this ICU cohort. This approach enhances the clinical relevance and reliability of our findings for managing critically ill patients.
Sputum culture frequency significantly impacts antibiotic selection. The multiple-culture group had a higher antibiotic adjustment rate (76.88% vs 67.33%, p =0.046), especially in MDR cases (87.69% vs 70.69%, p =0.019), echoing prior studies.26 This likely stems from a higher detection rate of MDR pathogens in the multiple-culture group (40.62% vs 28.71%), particularly Acinetobacter baumannii (38.46% vs 25.86%) and MRSA (30.77% vs 17.24%). Initial empirical antibiotics often failed to cover these resistant pathogens, leading to more frequent antibiotic changes. Moreover, the resistance of MDR pathogens to empirical antibiotics and the presence of multiple MDR infections necessitated broader or combination antibiotic therapy.27 Clinical deterioration in some patients also prompted treatment plan reassessments and antibiotic adjustments.28 In contrast, the single-culture group had lower antibiotic adjustment and MDR detection rates. There was no significant difference in antibiotic adjustment rates between the groups among non-MDR patients (65.97% vs 69.47%, p =0.572). This pattern suggests that the observed increase in antibiotic adjustments in the multiple-culture group is directly attributable to the protocol-driven increase in MDR pathogen detection, rather than to a fundamental difference in disease severity or treatment response. This implies the initial antibiotics in the single-culture group were more effective in pathogen coverage, enabling earlier infection control and better patient outcomes, including shorter ICU stays and mechanical ventilation durations. These findings highlight the importance of selecting effective initial empirical antibiotics to reduce adjustment needs and healthcare costs. Although propensity score matching was used to minimize bias, unmeasured disease severity factors might still affect the results. Notably, multiple sputum cultures in a short time increased clinicians’ confidence in MDR culture results, leading to treatment decision and antibiotic use adjustments, a novel insight from this study. However, procalcitonin (PCT) testing was not routinely performed due to insurance or other factors, which might influence result interpretation. Randomized controlled trials are necessary to confirm whether sputum culture frequency truly impacts clinical decisions and patient outcomes.
This study compared clinical outcomes of ICU patients on mechanical ventilation who received either a single culture or multiple sputum cultures within 24 hours. The results revealed a significantly shorter duration of mechanical ventilation, ICU stay, and hospital stay in the single culture group. These findings contrast with the literature, which suggests that multiple sputum cultures enhance pathogen detection, potentially enabling targeted therapy and improved recovery rates.29,30 This discrepancy may be best explained by the inherent properties of repeated sampling: it increases the cumulative probability of detecting MDR organisms (as supported by our sensitivity analysis), which in turn prompts more antibiotic changes but does not necessarily accelerate clinical recovery. The appropriateness of the initial empirical antibiotic therapy may be a more critical determinant of outcome than culture frequency alone.
The hospitalization costs for patients with a single sputum culture are lower than those for patients with multiple sputum cultures. Although sputum cultures can be beneficial, they often do not result in changes to antibiotic treatment. Studies have indicated that even when cultures are obtained, the treatment is frequently not adjusted, which ultimately increases the overall diagnostic costs.31,32 In our study, patients in the single sputum culture group had a lower rate of antibiotic changes, indicating that the empirically used antibiotics in this group were likely more effective against the identified pathogens. These findings suggest that initial empirical antibiotics were more appropriate, leading to better patient outcomes. Consequently, earlier administration of suitable antibiotics resulted in improved prognostic indicators, such as reduced length of stay and a decreased likelihood of adverse outcomes for healthcare-associated pneumonia (HCAP) patients.33 The median APACHE II scores (20 vs 21) and PaO2/FiO2 ratios indicate slight baseline differences, with the multiple-culture group having marginally worse hypoxemia. Despite propensity score matching, it is challenging to match all indicators related to disease severity. These persistent differences suggest that patients selected for multiple sputum cultures may have had a more severe or complex clinical presentation, inherently requiring more intensive monitoring and treatment, which itself contributes to higher costs. Studies have shown that each one-unit increase in the APACHE II score can add approximately $1000 to hospital costs.34 Overall, a single sputum culture may lower costs and support effective antibiotic use, whereas multiple cultures increase expenses without improving outcomes.
This study has several important limitations. First, the observational design precludes establishing direct causal relationships between sputum culture frequency and secondary outcomes (eg, hospitalization costs, ICU stay duration), as these are influenced by multifactorial determinants. Second, the lack of molecular confirmation (eg, Whole Genome Sequencing) limits our ability to definitively interpret the dynamics of pathogen detection in the multiple-culture group. Third, the small effect size (φ = 0.105) suggests limited clinical relevance of the observed statistical differences in antibiotic adjustment rates (p = 0.048). Finally, despite propensity score matching, residual confounding by disease severity may persist. These limitations highlight the need for randomized controlled trials with standardized sampling protocols to validate our findings and optimize clinical strategies.
Conclusions
This study undertook a comparative analysis of the frequency of single versus multiple sputum cultures in ICU patients with pulmonary infections. These findings demonstrated that multiple cultures were associated with more frequent adjustments in antibiotic therapy. In contrast, single daily cultures were linked to a reduced length of stay in the ICU, shorter duration of mechanical ventilation, and decreased hospitalization costs without impacting in-hospital or 28-day mortality rates. These results suggest that while multiple cultures may improve antibiotic management, single cultures may result in greater resource efficiency. Further validation through randomized controlled trials is necessary.
Abbreviations
ICU, Intensive Care Unit; PS, Propensity Score; APACHE II, Acute Physiology and Chronic Health Evaluation II; GCS, Glasgow Coma Scale; CNY, Chinese Yuan; ATS, American Thoracic Society; IDSA, Infectious Diseases Society of America; MAC, Mycobacterium avium complex; NGS, Next-Generation Sequencing; HCAP, Healthcare-Associated Pneumonia; PSM, Propensity Score Matching; LOS, Length of Stay; MDR, Multidrug-resistant; CAP, Community-acquired pneumonia; HAP, Hospital-acquired pneumonia.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy concerns and institutional regulations but are available from the corresponding author, Zhonghua Lu, upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was granted by the Ethics Committee of the Second Affiliated Hospital of Anhui Medical University (YX2024-158).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by several funding sources: the Clinical Research Cultivation Program of the Second Affiliated Hospital of Anhui Medical University (2021LCYB12), the National Natural Science Foundation Incubation Program of the Second Affiliated Hospital of Anhui Medical University (2022GMFY10), and the Natural Science Research Project of Anhui Higher Education Institutions (2023AH053168).
Disclosure
All authors declare no competing interests.
References
1. Snell N, Gibson J, Jarrold I, et al. Epidemiology of bronchiectasis in the UK: findings from the British lung foundation’s ‘Respiratory health of the nation’ project. Respir Med. 2019;158:21–14. doi:10.1016/j.rmed.2019.09.012
2. Xie J, Wang H, Kang Y, et al. The epidemiology of sepsis in Chinese ICUs: A national cross-sectional survey. Crit Care Med. 2020;48(3):e209–e18. doi:10.1097/CCM.0000000000004155
3. Beumer MC, Koch RM, van Beuningen D, et al. Influenza virus and factors that are associated with ICU admission, pulmonary co-infections and ICU mortality. J Crit Care. 2019;50:59–65. doi:10.1016/j.jcrc.2018.11.013
4. Spatenkova V, Bradac O, Fackova D, et al. Low incidence of multidrug-resistant bacteria and nosocomial infection due to a preventive multimodal nosocomial infection control: a 10-year single centre prospective cohort study in neurocritical care. BMC Neurol. 2018;18(1):23. doi:10.1186/s12883-018-1031-6
5. Boomer JS, To K, Chang KC, et al. Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA. 2011;306(23):2594–2605. doi:10.1001/jama.2011.1829
6. Lambermont B, Kisoka G, Grégoire C. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med. 2021;47(1):60–73. doi:10.1007/s00134-020-06294-x
7. Park PK, Napolitano LM, Bartlett RH. Extracorporeal membrane oxygenation in adult acute respiratory distress syndrome. Crit Care Clin. 2011;27(3):627–646. doi:10.1016/j.ccc.2011.05.009
8. Davey P, Marwick CA, Scott CL, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2017;2(2):Cd003543. doi:10.1002/14651858.CD003543.pub4
9. Morales E, Cots F, Sala M, et al. Hospital costs of nosocomial multi-drug resistant Pseudomonas aeruginosa acquisition. BMC Health Serv Res. 2012;12:122. doi:10.1186/1472-6963-12-122
10. Wicky PH, Niedermann MS, Timsit JF. Ventilator-associated pneumonia in the era of COVID-19 pandemic: how common and what is the impact? Crit Care. 2021;25(1):153. doi:10.1186/s13054-021-03571-z
11. Zhou JJ, Ding WC, Liu YC, et al. Diagnostic value of metagenomic next-generation sequencing for pulmonary infection in intensive care unit and non-intensive care unit patients. Front Cell Infect Microbiol. 2022;12:929856. doi:10.3389/fcimb.2022.929856
12. Post AE, Bathoorn E, Postma DF, et al. The agreement between bronchoalveolar lavage, bronchial wash and sputum culture: a retrospective study. Infection. 2024;52(4):1481–1488. doi:10.1007/s15010-024-02238-5
13. Zhou W, Li J. Correlation between sputum bacterial culture positive rate and drug sensitivity test results and disease severity ininpatients and its clinical significance: a systematicreview and meta-analysis. Comput Intell Neurosci. 2022;2022:5102100. doi:10.1155/2022/5102100
14. Iwasaki T, Yamaguchi F, Hayashi M, et al. Combination of anti-glycopeptidolipid-core IgA antibody and clinical features for diagnosing potential nontuberculous mycobacterium pulmonary disease in routine practice. Ther Adv Respir Dis. 2022;16:17534666221138002. doi:10.1177/17534666221138002
15. Ramanan P, Barreto JN, Osmon DR, et al. Rothia bacteremia: a 10-year experience at Mayo Clinic, Rochester, Minnesota. J Clin Microbiol. 2014;52(9):3184–3189. doi:10.1128/JCM.01270-14
16. Zhang J, Gao L, Zhu C, et al. Clinical value of metagenomic next-generation sequencing by Illumina and Nanopore for the detection of pathogens in bronchoalveolar lavage fluid in suspected community-acquired pneumonia patients. Front Cell Infect Microbiol. 2022;12:1021320. doi:10.3389/fcimb.2022.1021320
17. Lyu J, Zhang J, Ren X. Detection and identification of bacterial pathogens directly from sputum samples by pyrosequencing. J Med Microbiol. 2019;68(3):368–373. doi:10.1099/jmm.0.000917
18. Bhattacharyya A, Sinha M, Singh H, et al. Mechanistic insight into the antifungal effects of a fatty acid derivative against drug-resistant fungal infections. Front Microbiol. 2020;11:2116. doi:10.3389/fmicb.2020.02116
19. Pool KL, Heuvelings CC, Bélard S, et al. Technical aspects of mediastinal ultrasound for pediatric pulmonary tuberculosis. Pediatr Radiol. 2017;47(13):1839–1848. doi:10.1007/s00247-017-3954-2
20. Bashford J, Flowers W, Haworth C, et al. Evaluation of a novel ELISA test using synthetic mycolic acid antigens for serodiagnosis of non-tuberculous mycobacterial (NTM) infections. Thorax. 2023;78(3):309–312. doi:10.1136/thorax-2022-218800
21. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416. doi:10.1164/rccm.200604-571ST
22. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the American thoracic society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
23. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2(Suppl 2):S27–72. doi:10.1086/511159
24. Harder VS, Stuart EA, Anthony JC. Propensity score techniques and the assessment of measured covariate balance to test causal associations in psychological research. Psychol Methods. 2010;15(3):234–249. doi:10.1037/a0019623
25. Craven DE, Chroneou A, Zias N, et al. Ventilator-associated tracheobronchitis: the impact of targeted antibiotic therapy on patient outcomes. Chest. 2009;135(2):521–528. doi:10.1378/chest.08-1617
26. Harris AD, Pineles L, Belton B, et al. Universal glove and gown use and acquisition of antibiotic-resistant bacteria in the ICU: a randomized trial. JAMA. 2013;310(15):1571–1580. doi:10.1001/jama.2013.277815
27. Fatsis-Kavalopoulos N, Roemhild R, Tang PC, et al. CombiANT: antibiotic interaction testing made easy. PLoS Biol. 2020;18(9):e3000856. doi:10.1371/journal.pbio.3000856
28. Zgliczyński WS, Bartosiński J, Rostkowska OM. Knowledge and practice of antibiotic management and prudent prescribing among polish medical doctors. Int J Environ Res Public Health. 2022;19(6):3739. doi:10.3390/ijerph19063739
29. Barr DA, Kerkhoff AD, Schutz C, et al. HIV-associated mycobacterium tuberculosis bloodstream infection is underdiagnosed by single blood culture. J Clin Microbiol. 2018;56(5):e01914–17. doi:10.1128/JCM.01914-17
30. Liu Y, Zhang R, Yao B, et al. Metagenomics next-generation sequencing provides insights into the causative pathogens from critically ill patients with pneumonia and improves treatment strategies. Front Cell Infect Microbiol. 2022;12:1094518. doi:10.3389/fcimb.2022.1094518
31. Sloan CE, Bernard S, Nachamkin I. Appropriateness of expectorated sputum cultures in the hospital setting. Diagn Microbiol Infect Dis. 2015;83(1):74–76. doi:10.1016/j.diagmicrobio.2015.05.009
32. da Fonseca Lima EJ, Lima DE, Serra GH, et al. Prescription of antibiotics in community-acquired pneumonia in children: are we following the recommendations? Ther Clin Risk Manag. 2016;12:983–988. doi:10.2147/TCRM.S101709
33. Asti L, Bartsch SM, Umscheid CA, et al. The potential economic value of sputum culture use in patients with community-acquired pneumonia and healthcare-associated pneumonia. Clin Microbiol Infect. 2019;25(8):
34. Morrison JL, Cai Q, Davis N, et al. Clinical and economic outcomes of the electronic intensive care unit: results from two community hospitals. Crit Care Med. 2010;38(1):2–8. doi:10.1097/CCM.0b013e3181b78fa8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the Efficacy of a Nomogram to Predict Multidrug-Resistant Pulmonary Infections Based on Data from Neurosurgery Ward Patients
Zhou R, Chen X, Jia H, Duan W
Infection and Drug Resistance 2025, 18:3723-3734
Published Date: 26 July 2025