Back to Journals » Infection and Drug Resistance » Volume 12
Simultaneous detection of eleven sexually transmitted agents using multiplexed PCR coupled with MALDI-TOF analysis
Authors Xiu L ![]() , Zhang C, Li Y, Wang F
, Zhang C, Li Y, Wang F ![]() , Peng J
, Peng J ![]()
Received 15 June 2019
Accepted for publication 10 August 2019
Published 28 August 2019 Volume 2019:12 Pages 2671—2682
DOI https://doi.org/10.2147/IDR.S219580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Leshan Xiu,1 Chi Zhang,1 Yamei Li,1 Feng Wang,2 Junping Peng1
1NHC Key Laboratory of Systems Biology of Pathogens, Institute of Pathogen Biology, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Shenzhen Center for Chronic Disease Control, Shenzhen, People’s Republic of China
Correspondence: Junping Peng
NHC Key Laboratory of Systems Biology of Pathogens, Institute of Pathogen Biology, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 6 Rongjing Eastern Street, BDA,
Beijing 100176, People’s Republic of China
Tel/fax +86 106 787 8493
Email [email protected]
Purpose: Sexually transmitted infections (STIs), representing a major global health problem, are caused by different microbes, including bacteria, viruses, and protozoa. Unfortunately, infections of different sexually transmitted pathogens often present similar clinical symptoms, so it is almost impossible to distinguish them clinically. Therefore, the aim of the current study was to develop a sensitive, multitarget, and high-throughput method that can detect various agents responsible for STIs.
Methods: We developed and tested a 23-plex PCR coupled with matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry (MS) assay (sexually transmitted infection-mass spectrometry, STI-MS) that simultaneously targets 11 different agents, including 8 most common clinical pathogens related to STIs (HSV-1, HSV-2, Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, Trichomonas vaginalis, Mycoplasma genitalium, and Haemophilus ducreyi) and 3 controversial microorganisms as pathogens (Mycoplasma hominis, Ureaplasma urealyticum, and Ureaplasma parvum).
Results: The results showed that the STI-MS approach can accurately detect the expected agents, without cross-reaction with other organisms. The limit of detection of each STI-MS assay was ranged from 1.739 to 10.009 copies/reaction, using probit analyses. The verification rate for each target organism of the STI-MS ranged from a minimum of 89.3% to a maximum of 100%, using conventional assays and ultrasensitive digital PCR to confirm the STI-MS-positive results. To further evaluate the clinical performance of this assay, 241 clinical specimens (124 urethral/cervical swabs and 117 urine) were tested in parallel using the STI-MS assay and monoplex real-time PCR for each agent. The overall validation parameters of STI-MS were extremely high including sensitivity (from 85.7% to 100%), specificity (from 92.3% to 100%), PPV (from 50% to 100%), and NPV (from 99.1% to 100%) for each target.
Conclusion: STI-MS is a useful high-throughput screening tool for detecting mixed infections of STIs and has great potential for application in large-scale epidemiological programs for specific microorganisms of STI.
Keywords: sexually transmitted infections, timely diagnosis, MALDI-TOF mass spectrometry, digital PCR, high-throughput
Introduction
Sexually transmitted infections (STIs) are a significant contributor to the global burden in public health and medical care. STIs can cause severe fetal and neonatal death, ectopic pregnancy, infertility, and genital neoplasia. Despite leading to such severe complications, clinical and public health practice sometimes underestimates the importance of diagnosing STIs, and moreover, for scientific research, STIs remain a neglected field.1 Many STIs are often asymptomatic during the early infection stages, which increase the risk of unrecognized transmission.2,3 The World Health Organization (WHO) estimated that approximately 357 million new infections of curable STIs occurred each year throughout the world (http://www.who.int/mediacentre/factsheets/fs110/en/). STIs are caused by different microbes, including bacteria, viruses, and protozoa. Unfortunately, infections of different sexually transmitted pathogens often present similar clinical symptoms, so it is almost impossible to distinguish them clinically.3 Therefore, it is important to develop a sensitive, multitarget, and high-throughput method that can detect various agents responsible for STIs. In addition, rapid and accurate identification is critical for preventing onward transmission, offering immediate intervention, adopting early treatment, and reducing patient management costs.4,5
Conventional diagnostic algorithms for STIs include cell culture, microscopic examination, enzyme immunoassay, and other serological investigation techniques.6–8 The diagnosis of STIs by culture or serology remains a challenge.9 Especially for herpes simplex virus and Treponema pallidum detection, cell culture shows low-sensitivity and long turnaround time, making this assay clinically useless.10,11 However, over the past two decades, molecular testing has been widely used to detect pathogens associated with STIs. Compared with traditional methods, molecular tests, such as PCR, real-time PCR, multiplex PCR, and microarray, have rapid turnaround times and superior sensitivities.3,7,12 Several commercial kits or systems based on nucleic acid amplification have been developed to detect pathogens responsible for STIs,13–16 but these systems still have disadvantages, such as high cost, low sample throughput, and the limited number of pathogens that can be detected in a single test reaction.3
In this study, the MassARRAY System (Agena Bioscience, Inc., San Diego, CA, USA), a detection platform combining endpoint multiplex-PCR with matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS), was utilized to develop a sexually transmitted infection assay (STI-MS) that can simultaneously detect and identify common clinical pathogens implicated in STIs, including herpes simplex virus types 1 and 2 (HSV-1 and HSV-2), Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, Trichomonas vaginalis, Mycoplasma genitalium, and Haemophilus ducreyi. Three controversial microorganisms (Mycoplasma hominis, Ureaplasma urealyticum, and Ureaplasma parvum), still not conclusive evidence whether these agents should be considered pathogens, were also included in the panel in our study. The system comes with some considerable benefits of multiplexing and high throughput, and it has been applied successfully in detecting and confirming various kinds of microbes.17–24 For each microorganisms included in the STI-MS assay, two different genes were selected as targets. If either of the genes were detected, the corresponding organisms were positive. Such a strategy can avoid false-negative results, thus making our method more sensitive and comprehensive. The performance of the STI-MS was evaluated using clinical specimens from patients with sexually transmitted infections. All STI-MS results were confirmed by real-time PCR and nested PCR. Discordant results were arbitrated by an ultrasensitive digital PCR method.
Materials and methods
Clinical specimens
The initial evaluation of the STI-MS assay included 176 archived DNA samples from anal swabs that were obtained from men who have sex with men (MSM) attending a local clinic, who tested positive for HIV, or had any susceptible symptoms of STIs. Details about the recruitment method, sample collection, and data collection have been previously described.25 To further evaluate the clinical performance of this assay, 241 clinical specimens (124 urethral/cervical swabs and 117 urine) were collected from Shenzhen Center for Chronic Disease Control. DNA extraction from clinical specimens was performed in the MagNA Pure LC 2.0 Instrument using MagNA Pure LC DNA Isolation Kit 1 (Roche Diagnostics, Mannheim, Germany).
Design of the STI-MS method
Candidate assay targets of highly conserved genomic regions for the eleven agents of interest were identified and chosen on the basis of published validation data, reporting used successfully as PCR targets. To avoid the false-negative results, two targets of each agent were used in the STI-MS method. Human β-globin (HBB) gene was selected for internal control. Therefore, we developed a 23-plex method to identify eight etiological agents related to the STIs and other three controversial organisms in this study. The NCBI GenBank database (http://www.ncbi.nlm.nih.gov/genbank/) was used to download all available full and partial nucleic acid sequences for each target. Primer pairs of multiplex PCR and extension probes were designed using Assay Design 4.1 software (Agena Bioscience, Inc., San Diego, CA, USA), and their specificity was confirmed by primer and nucleotide blast tools (NCBI, https://www.ncbi.nlm.nih.gov/tools/primer-blast/). Every PCR primer included a 5ʹ universal 10-mer tag (5ʹ-ACGTTGGATG-3ʹ) to increase the molecular weight. PCR primers and extension probes were obtained from Tsingke Biotechnology (Beijing, China). The final targeting regions and the primers/probes of the STI-MS assay were listed in Table S1 in the supplementary material.
Initial multiplex PCR and SAP reaction
Each 5 μL multiplex PCR reaction was composed of 2 μL DNA template, 0.5 μL PCR buffer, 0.4 μL MgCl2 (Agena Bioscience, Inc.), 0.1 μL mM dNTP (dATP, dUTP, dCTP, dGTP) (Promega, Madison, WI, USA), 1 μL primer mix, 0.2 μL DNA polymerase enzyme (Roche Molecular Systems Inc., Pleasanton, CA, USA), 0.2 μL uracil-DNA glycosylase (ShineGene Molecular Biotechnology, Shanghai, China), and 0.6 μL H2O. Multiplex PCR amplification was performed in a ProFlex PCR system (Applied Biosciences, Foster City, CA, USA) using 384-well PCR plates. The following thermocycler program was used for PCR: 45°C for 2 mins; 94°C for 4 mins; an initial denaturation at 95°C for 2 mins; 45 cycles at 95°C for 30 s, 56.5°C for 30 s, and 72°C for 1 min; and a final step of 72°C for 5 mins. After the PCR amplification, 0.3 U shrimp alkaline phosphatase (SAP) was added and incubated at 37°C for 40 mins, and then 85°C for 5 mins to remove the residual dNTPs.
Single-base extension reaction and mass spectrometry
The single-base extension (SBE) reaction was performed with the iPLEX Pro Reagent kit (Agena Bioscience, Inc.) in a total reaction volume of 9 μL. For the SBE reaction, 0.619 μL H2O, 0.2 μL terminator mix, 0.2 μL iPLEX Pro buffer, 0.94 μL extension probe cocktail, and 0.041 μL ThermoSequenase enzyme were mixed with the products of SAP treatment, using the thermocycling conditions: 94°C for 30 s; 40 cycles at 94°C for 5 s with 5 cycles of 52°C for 5 s and 80°C for 5 s; and a final 72°C for 3 mins. During the SBE reaction, the probe is extended by one mass-modified nucleotide depending on the nucleotide position of interest. The products of the SBE reaction were desalted by rotation with a cationic ion exchange resin (Agena Bioscience, Inc.) for 60 mins. The purified product was spotted onto a 384-spot SpectroChip II (Agena Bioscience, Inc.) using the Nanodispenser RS 1000 equipment (Agena Bioscience, Inc.) and then scanned using the mass spectrometry of MassARRAY system. The results were analyzed by Typer software version 4.1 (Agena Bioscience, Inc.).
Confirmation of positive STI-MS results
To further confirm the positive results obtained by STI-MS assay, the same nucleic acid extracts used for STI-MS analysis were also analyzed either with real-time PCR or nested PCR. All positive specimens were first analyzed using real-time PCR targeting species-specific genes. Real-time PCR was performed using a simplex real-time PCR developed or adapted for the following organisms: HSV-1 and HSV-2, C. trachomatis, T. pallidum, N. gonorrhoeae, M. genitalium, M. hominis, U. urealyticum, and U. parvum. Specimens with a cycle threshold (Ct) value above 38 were considered negative. Any samples that were not confirmed by the initial round of real-time PCR analysis were retested with nested PCR. The primers employed for the nested PCR with sequencing were designed in-house and selected according to the previously published literature.26–28 A negative control was included for each PCR run to ensure the purity of the reagent. A specimen was considered positive for a given result if either of the two assays for that result were positive. Tables S2 and S3 provide details about the primers and probes used in this study for real-time PCR and nested PCR-based confirmation.
Resolution of discordant results
Digital PCR (dPCR) was performed for the arbitration of discrepant results between the STI-MS assay and confirmatory tests. Digital PCR amplifications were carried out on a microchip using a QuantStudio® 3D Digital PCR System (Applied Biosciences, Foster City, CA, USA). A final reaction volume of 14.5 μL was prepared, containing 7.25 μL QuantStudio® 3D Digital PCR Master Mix, 0.29 μL (10 μM) of probe, 0.1305 μL (100 μM) of each primer, 1.699 μL H2O and 5 μL of DNA template. According to the manufacturer’s instructions, a 14.5 μL reaction mixture was immediately loaded on the QuantStudio® 3D dPCR chip using QuantStudio® 3D Digital PCR chip loader. The chip was then placed on the ProFlex PCR system for PCR amplification using the following cycling conditions: initial hold at 96°C for 10 mins; 39 cycles at 58°C for 2 mins, and 98°C for 30 s; and 60°C for 2 mins. Following amplification, the chips were inserted into the chip reader for imaging, and the data were analyzed using the cloud-based QuantStudio® 3D AnalysisSuite software. For each digital PCR run, at least one positive and negative control was included.
Statistical analysis
Differences between the concordance rates among single infection and multiple infection specimens were compared using the χ2 test. Statistical analysis was carried out using SPSS software version 17.0 (SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered significant. Comparison of diagnostic performance between the STI-MS assay and monoplex real-time PCR was assessed by measuring sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) using the VassarStats website (https://vassarstats.net/).
Ethical approval
All experiments were performed according to the ethical standards of the national research committee and with the 1964 Helsinki declaration. Scientific approval to conduct this study was obtained from the Institutional Review Boards of the Institute of Pathogen Biology. Written informed consent was obtained from every participant before the interview and testing.
Results
The STI-MS method
In this study, we developed and tested a 23-plex method that targets eleven different etiological agents simultaneously and can identify the most common pathogens related to STIs, using HBB as an internal control. After nucleic acid extraction of samples, the first step of STI-MS assay was multiplex PCR using specific primers and probes that amplify highly conserved regions of the microbial genome. The second step of STI-MS assay involved the detection of specific products by using a MALDI-TOF mass spectrometer system, in which the mass of each product was measured. The microorganism(s) in the specimen were determined by observing the base composition of the observed. To avoid false-negative results, two targets of each agent were used in the STI-MS assay. The results of the nucleotide BLASTN analysis showed that all tested primers and probes worked well. Our results revealed that the developed STI-MS method had satisfactory analytical specificity and multiplex detection capacity for target organisms.
Analytical specificity and sensitivity
The specificity and detection power of the assay were evaluated using nucleic acid extracted from 303 confirmed clinical isolates and samples (Table 1). Positive clinical samples and isolates of H. ducreyi were not obtained, and positive plasmids with target genes were used to validate the specificity in this study. The results showed that the STI-MS approach can accurately identify the targeted agents, and positive results were not obtained from the negative controls (Figures S1–S11 in the supplementary material). To further evaluate the detection specificity and cross-reactivity, 65 genetically or clinically nonspecific pathogens were tested using the same assay procedure used for the STI detection. All assay results were negative and nonspecific positive reactions were not observed.
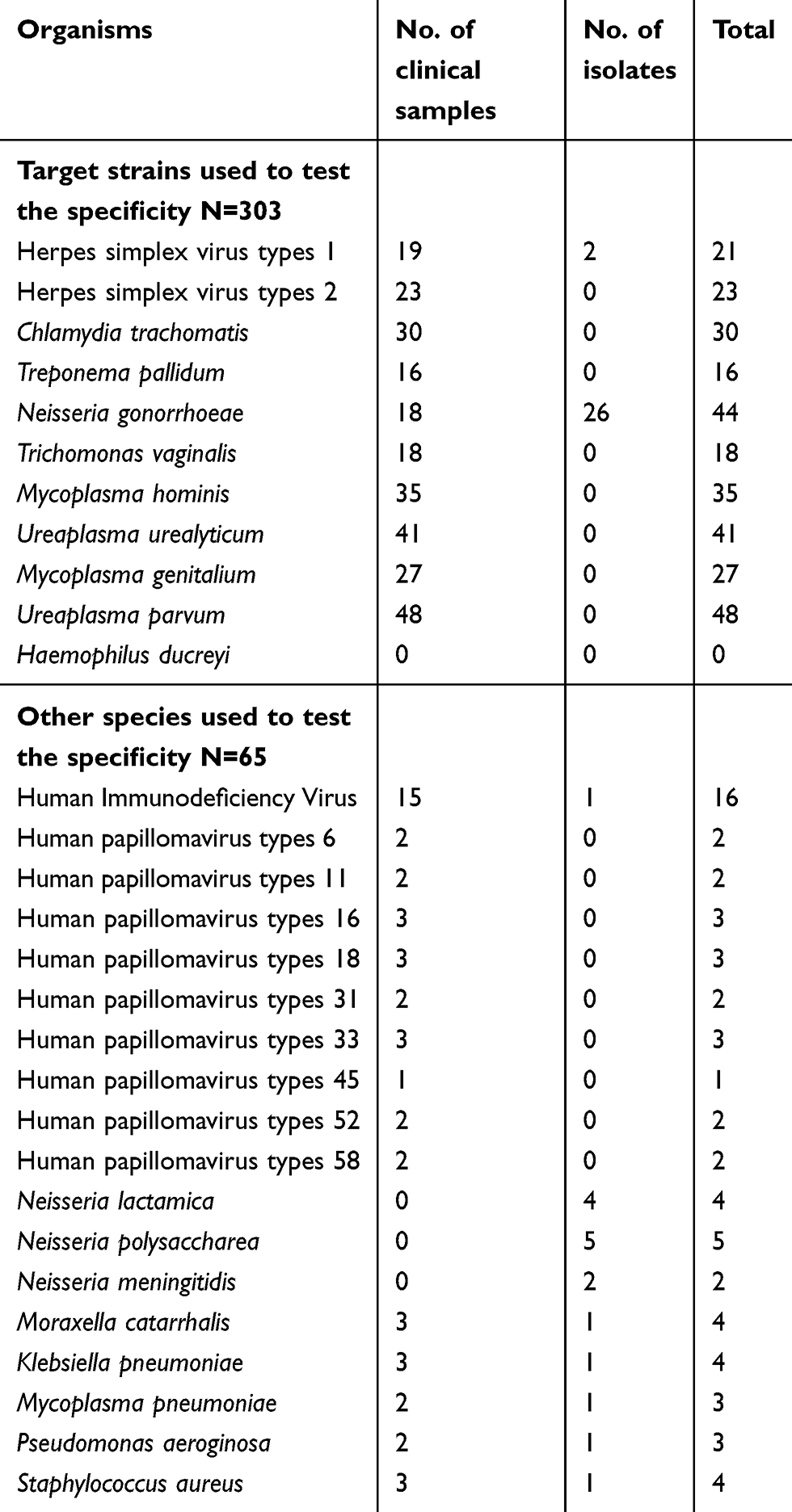 |
Table 1 Sequencing confirmed clinical samples and isolates used for validating specificity |
The analytical sensitivity (limit of detection) of the STI-MS assay developed in this study was determined by testing serial dilutions of positive standards ranging from 100 to 1 copies/μL plasmids carrying the target genes of each agent. A regression probit analysis was carried out using SPSS Statistics 17.0.0 to calculate the limit of detection (LOD) of each assay that could be measured with 95% probability. Probit analysis on four runs with 3 replicate dilutions of 5 different plasmid concentrations gave LODs ranging from 1.739 to 10.009 copies/reaction (Table 2).
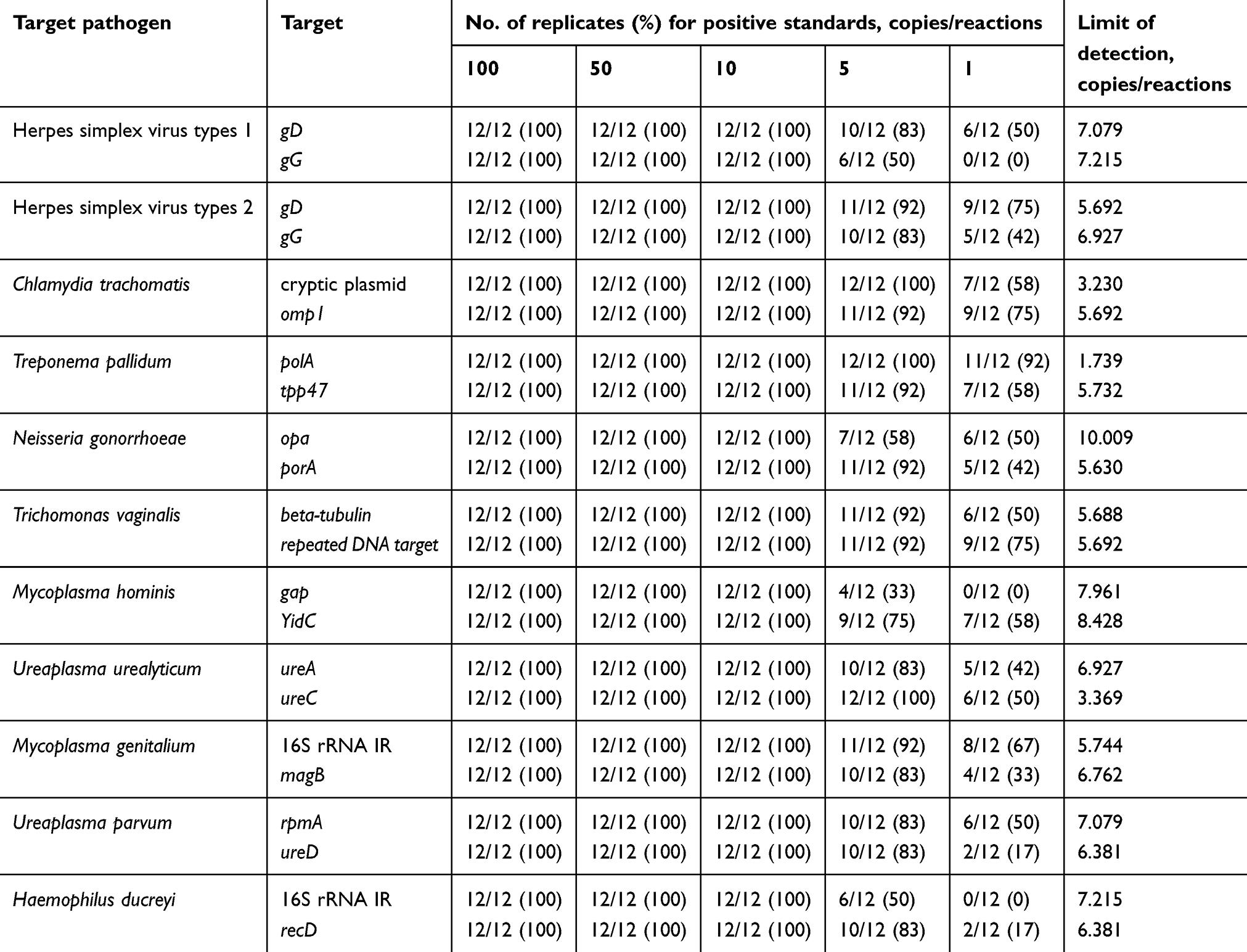 |
Table 2 Limit of detection of each target gene using regression probit analysis |
Evaluation of the performance on archived DNA samples
To evaluate the performance of the simultaneous detection system in clinical samples, we screened a total of 176 anal swabs obtained from MSM using the developed STI-MS assay. Among the 176 archived DNA samples, 121 (68.8%) were positive by the STI-MS method for at least one microorganism. Etiological agents were not detected in 55/176 (31.3%) samples. Our method allowed for the diagnosis of bacterial organisms in 97/176 (55.1%) specimens, viral organisms in 7/176 (4.0%) specimens, and bacterial–viral combinations in 17/176 (9.7%) specimens. Sixty-seven of the 121 (55.4%) specimens were also identified as mixed agent combination for STI-MS assay target organisms. Furthermore, from the multiple combination samples, 33 tested samples (49.3% of the total 67) were identified as dual-combinations with 2 of the 11 microorganisms, and 22 analyzed samples (32.8% of the total 67) were found to be detected with 3 agents, while more than 3 organisms belonging to the STI-MS assay were detected in 12 surveyed samples.
For all positive specimens by the STI-MS method, the results were confirmed using related confirmatory tests. In the 54 samples found positive for single microorganism by STI-MS, 32 (59.3%) samples were also positive for single organism by an initial real-time PCR assay that targeted species-specific genes. However, for multiple agent combination specimens, 30 (44.8% of the total 67) of the positive specimens showed results concordant with the STI-MS assay. The discordant specimens were further verified by nested PCR and bidirectional sequencing. Combining the results of the two confirmatory tests, the concordance rate was 70.4% (38/54) for single organism and 64.2% (43/67) for multiple agent combination. Forty STI-MS-positive specimens were not confirmed by either real-time PCR or nested PCR.
For further analysis of the 40 specimens that yielded discrepant results with the developed STI-MS assay and the confirmatory tests, ultrasensitive digital PCR was performed. Among these 40 STI-MS-positive and confirmatory test-negative samples, 31 (77.5%) were confirmed as positive by a digital PCR assay, whereas 9 (22.5%) remained unverified after the resolution of the discordant results, including 4 single organism samples and 5 multiple agent combination samples (Table 3). The results of the confirmatory tests and arbitration testing revealed that all retested specimens that were verified as positive by either of the tests were indeed accurate positive, irrespective of their classification as negative by either assay. The arbitration testing results are illustrated in Table S4 and Figures S12–S18 in the supplemental material. Table 4 shows the performance of the STI-MS assay as well as the resolution of the discordant results after arbitration testing. The overall verification rate was 92.6% (50/54) for single organism, whereas this rate was 92.5% (62/67) for multiple agent combination. The difference was not significant among these two rates (P>0.05 by χ2 test). The verification rates for each target organism of the STI-MS assay ranged from a minimum of 89.3% (25/28) for N. gonorrhoeae to a maximum of 100% (2/2) for U. parvum, 100% (2/2) for T. pallidum, and 100% (31/31) for M. genitalium. Among the 176 specimens tested, the majority of the screened samples detected were positive for U. urealyticum (n=55; 31.3%), followed by C. trachomatis (n=43; 24.4%) and M. hominis (n=38; 21.6%). T. vaginalis and H. ducreyi were not detected in our study. Most of the samples with multiple combinations included U. urealyticum and M. hominis (35.8%, 24/67). The most frequent types of multiple combinations detected in the surveyed samples were U. urealyticum, C. trachomatis, and M. hominis (n=6). The numbers of tested specimens with multiple combinations are shown in Table S5.
 |
Table 3 Samples with discordant results by the STI-MS method after arbitration testing |
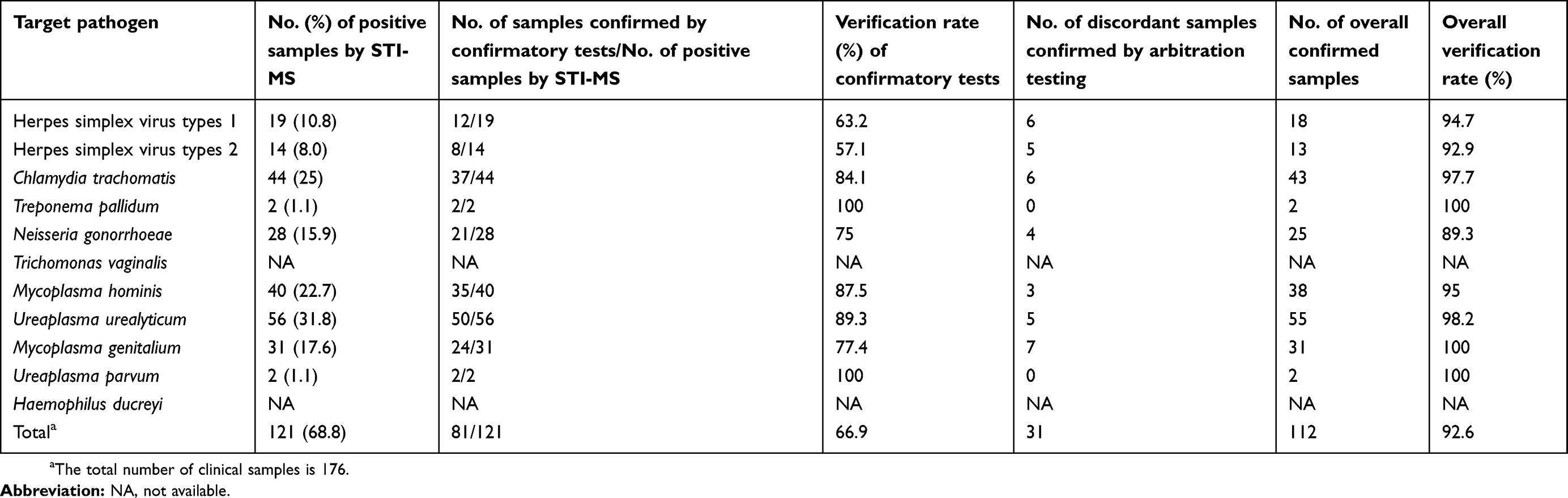 |
Table 4 Results of confirmatory tests of positive samples by the STI-MS assay and resolution of discordant results following arbitration testing |
Performance characteristics of the STI-MS assay compared to the monoplex real-time PCR
To further evaluate the clinical performance of this assay, 241 clinical specimens (124 urethral/cervical swabs and 117 urine) were tested in parallel using the STI-MS assay and monoplex real-time PCR for each agent. The primers and probes used in the monoplex real-time PCR were listed in Table S2 in the supplementary material. The performance characteristics (sensitivity, specificity, PPV, and NPV) of each microorganism for the different specimen types were calculated and listed in Table 5. Overall, there was very good sensitivity (ranging from 85.7% to 100%), specificity (ranging from 92.3% to 100%), and NPV (ranging from 99.1% to 100%) for each of the evaluated targets. Because the STI-MS has a lower LOD than real-time PCR, the results showed a more expanded PPV ranging from 50% to 100% in terms of different agents and specimen types (Table 5).
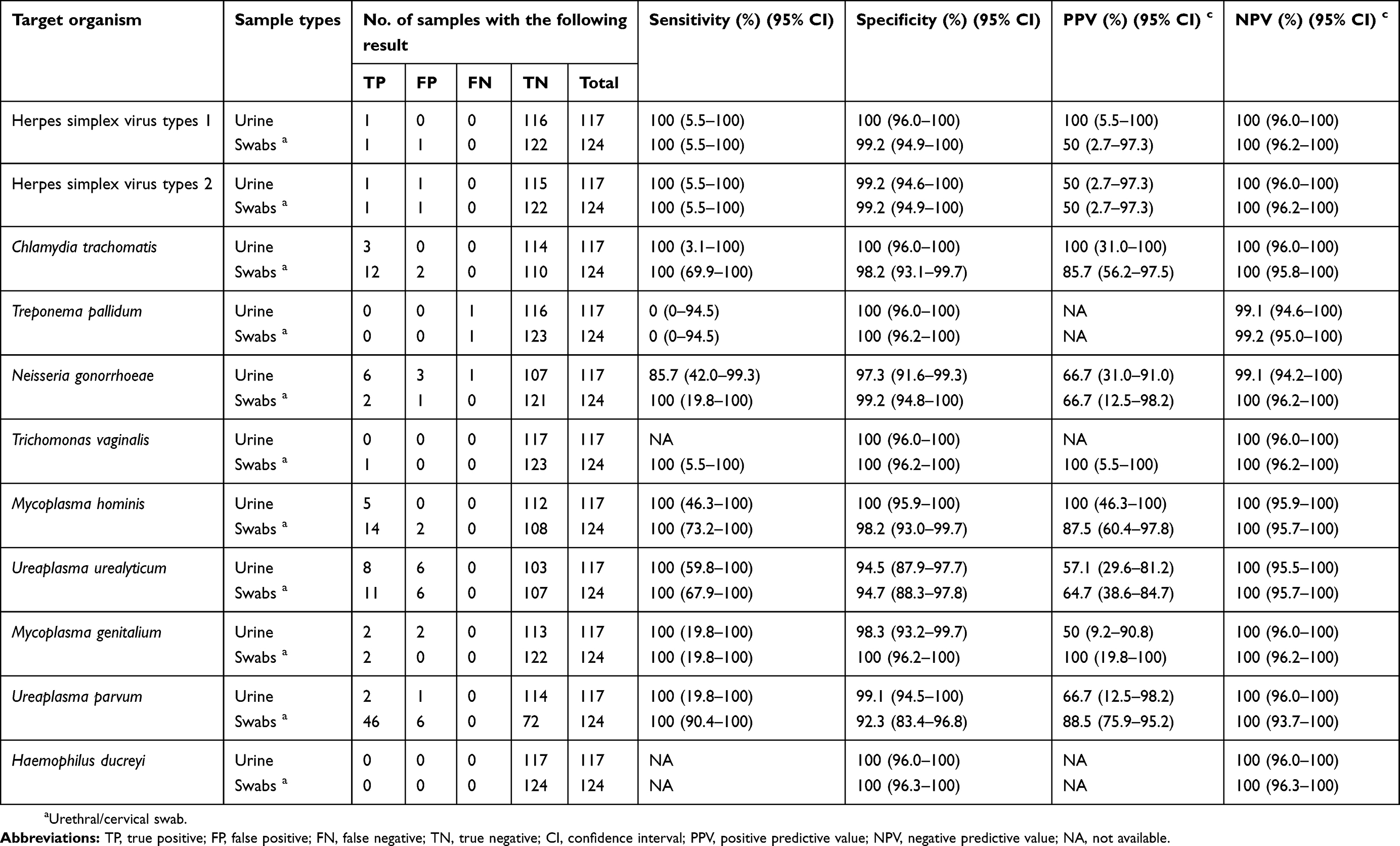 |
Table 5 Clinical performance of the STI-MS assay for organism identification compared to that of monoplex real-time PCR |
Discussion
This work details the design and development of an STI-MS assay that can be used on clinical samples to screen for eleven sexually transmitted microorganisms.
STIs comprise a number of fatal and often serious infections, and yet such infections often pose challenges in identifying the causative organisms. Rapid and accurate identification of sexually transmitted infections can reduce onward transmission and improve treatment efficacy. Many pathogens responsible for STIs are identified by cell culture, microscopic examination, or antigen detection methods.7 PCR-based approaches have been shown to be more sensitive at detecting pathogens in clinical samples than traditional diagnostic tests (ie, culture, microscopy and antigen detection) if samples are collected at the appropriate time during infection.3,29 Considering the wide range of etiological agents that can cause STIs and the similarity of the clinical presentations of infection produced by different pathogens, the multiplex molecular diagnostic tools seem to be an optimal method for rapid diagnosis.2,12,30 Therefore, we utilized multiplex PCR and MALDI-TOF MS incorporated into an STI-MS assay, which might be helpful for better understanding the phenomenon of mixed infections in clinical specimens.
Because of the severity and complexity of STIs, feasible and effective screening approaches are essential for timely implementation of effective infection control measures to prevent further transmission. Additionally, increases in antimicrobial drug resistance in N. gonorrhoeae and M. genitalium remain an important concern.1 Large-scale epidemiological studies and surveillance programs are needed to determine optimal prevention strategies and to reduce the global burden of STIs.
Routine screening for pathogens associated with STIs on an annual basis is recommended for all pregnant women, all sexually active females <25 years of age, and at-risk MSM.5,31 To date, nucleic acid amplification tests (NAATs) are accepted worldwide as an important method for screening causative agents of STIs with several approved commercial molecular panels available.32–35 In addition, several emerging nucleic acid amplification platforms combined with fully and partially automated instrumentation are available for targeting multiple microorganisms in a single test reaction.12,14,30,36,37 However, these platforms are low throughput or have a high cost per sample, preventing rapid screening of large numbers of specimens. Compared to other diagnostic strategies, STI-MS using MALDI-TOF MS technologies are generally more reliable and can be more easily automated. The STI-MS assay simultaneously detects the nucleic acid from 1 protozoan, 2 viral, and 8 bacterial organisms and analyzes approximately 760 clinical samples within 1 working day. Because of the high sample throughput of this method, the cost of detecting 11 pathogens using STI-MS is less than $4, not including the cost of the nucleic acid extraction. Therefore, the STI-MS method has great potential to be applied in large-scale epidemiological programs for specific microorganisms of STI and provides important information for public health interventions and disease control and eradication.
One of the main challenges in the design and establishment of these assays was limiting the potential for cross-reactions with other organisms, particularly commensal species. Examples of these tested sites include adequate numbers of commonly Neisseria meningitidis and other commensal Neisseria species, which can cause cross-reaction in the screening assays due to their high degree of nucleic acid homology with N. gonorrhoeae.38 Among the targets used to identify C. trachomatis, a cryptic plasmid has been the most widely used for NAATs.39–41 However, it was subsequently shown that sequence variation of cryptic plasmids has been detected in several countries.42–44 This demonstrates that false-negative results may occur when a cryptic plasmid is used alone as the target for detection of C. trachomatis particularly when screening clinical samples from this region. Previously, several commercial NAATs used a single target on the pathogens associated with sexually transmitted infections, which led to the emergence of a false-negative diagnostic result, and the infection went untreated and was transmitted between individuals without knowledge before being recognized.45 To overcome these potential problems, the STI-MS assay uses two targets of each pathogen to increase the sensitivity and specificity and to reduce false-negative results. The results of this study have shown that the STI-MS method was useful for detecting several microorganisms simultaneously with high specificity and accuracy.
Another aspect that could affect the performance of the assays is the quality of the sample in terms of etiological load and number of copies containing pathogens. In our study, 40 positive specimens using the developed STI-MS assay were not confirmed by confirmatory tests. One possible cause for the higher number of discrepancies in the clinical specimens for causative agents of STIs may be due to target pathogens with a low concentration, as reported by Van et al in an evaluation of BD MAX assay.37 Digital PCR has been successfully applied in the field of pathogen detection46,47 and is particularly suited to the low-level detection of nucleic acid even with a highly complex background.47,48 In the arbitration stage, ultrasensitive digital PCR was performed to resolve discordant results. Thirty-one (77.5%) specimens were confirmed as positive after arbitration testing. To significantly shorten the detection time, ultrasensitive diagnosis methods for STIs are required to detect extremely small amounts of microorganisms directly without culturing the specimen. Based on sensitivity testing, LOD of the STI-MS assay can reach a minimum of 1.739 copies per reaction. Moreover, it was subsequently verified that this method also has a high sensitivity in the evaluation of clinical samples. Thus, when target pathogens with a low concentration in clinical specimens, the STI-MS assay substantially increased our ability to detect potential pathogens and increased the likelihood that an accurate diagnosis will not be missed.
MSM are at risk of acquiring protozoan, viral, and bacterial STIs from both male and female partners. Most of the previous studies have shown the prevalence of STI ranges from 2.6% to 23.7%,49 while our study indicates that the detection rate of agents was 68.8% (121/176) among MSM, which was higher than the data in other studies. We speculate that the difference was caused by the improved coverage of screening using this method. Coinfections are frequently encountered among MSM and present a difficult diagnostic challenge for clinical microbiology laboratories. In our study, 55.4% (67/121) specimens were identified as mixed agent combinations, and most of those with multiple combinations included U. urealyticum and M. hominis (35.8%, 24/67). These findings are consistent with those recently reported in a study using a commercial detection kit.35 As the high detection rates of U. urealyticum and M. hominis might have been caused by infection and commensalism, their roles as pathogens are controversial.50 However, an earlier study suggested that U. urealyticum and M. hominis combination may be associated with an increased drug resistance.51 The detection of STIs using the STI-MS approach might be helpful for the timely discovery of mixed agent combinations, and clinicians could prescribe appropriate antibiotics for patients according to the results of identified pathogens.
However, some limitations exist for the STI-MS assay as we mentioned in the previous studies.18,22 First, when the load of the organism is too low, the STI-MS assay may fail to detect the target pathogen because the volume of specimen used in the initial PCR was 2 μL. Second, the high cost of the equipment and the large footprint of the system limit the application range of the mass spectrometer platform in clinical laboratories. Third, with nearly 8 hours of turnaround time, the STI-MS assay is not suitable for the detection of a small number of samples. Additionally, as anal swabs using in the evaluate stage were archived DNA samples, the limited sample volume prevented us from testing in parallel, using the STI-MS assay and monoplex real-time PCR for each agent. Therefore, additional testing on different sample types (including anal swabs) will be required in the future to evaluate comprehensively the performance of the STI-MS assay. Finally, as positive clinical samples and isolates of H. ducreyi are not available, the specificity of H. ducreyi was determined by analysis of plasmids containing the respective target sequences.
Given its rapidity, sensitivity, and specificity, STI-MS is a useful high-throughput screening tool for detecting mixed infections of STIs and has great potential in large-scale STI epidemiological programs.
Acknowledgments
We give special thanks to Junhua Guo for technical assistance, and to Lei Gao and Zhujun Shao for kindly providing us clinical samples and clinical isolates, respectively. This study was supported by grants from the CAMS Innovation Fund for Medical Science (2016-I2M-3-021).
Author contributions
All authors contributed to data analysis, drafting, or revising the article; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
Junping Peng, Junhua Guo, and Leshan Xiu have a patent (201910527364.8, People’s Republic of China) related to this article. The authors have declared that they have no other conflicts of interest in this work.
References
1. Unemo M, Bradshaw CS, Hocking JS, et al. Sexually transmitted infections: challenges ahead. Lancet Infect Dis. 2017;17(8):e235–e279. doi:10.1016/S1473-3099(17)30242-6
2. McKechnie ML, Hillman R, Couldwell D, et al. Simultaneous identification of 14 genital microorganisms in urine by use of a multiplex PCR-based reverse line blot assay. J Clin Microbiol. 2009;47(6):1871–1877. doi:10.1128/JCM.00120-09
3. Cao B, Wang S, Tian Z, Hu P, Feng L, Wang L. DNA microarray characterization of pathogens associated with sexually transmitted diseases. PLoS One. 2015;10(7):e0133927. doi:10.1371/journal.pone.0133927
4. Gaydos C, Hardick J. Point of care diagnostics for sexually transmitted infections: perspectives and advances. Expert Rev Anti Infect Ther. 2014;12(6):657–672.
5. Workowski KA, Bolan GA; Centers for Disease C, Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR–03):1–137.
6. Karaer A, Mert I, Cavkaytar S, Batioglu S. Serological investigation of the role of selected sexually transmitted infections in the aetiology of ectopic pregnancy. Eur J Contracept Reprod Health Care. 2013;18(1):68–74.
7. Trembizki E, Costa AM, Tabrizi SN, Whiley DM, Twin J. Opportunities and pitfalls of molecular testing for detecting sexually transmitted pathogens. Pathology. 2015;47(3):219–226.
8. Van Dyck E, Ieven M, Pattyn S, Van Damme L, Laga M. Detection of Chlamydia trachomatis and Neisseria gonorrhoeae by enzyme immunoassay, culture, and three nucleic acid amplification tests. J Clin Microbiol. 2001;39(5):1751–1756.
9. Battle TJ, Golden MR, Suchland KL, et al. Evaluation of laboratory testing methods for Chlamydia trachomatis infection in the era of nucleic acid amplification. J Clin Microbiol. 2001;39(8):2924–2927.
10. Wald A, Huang ML, Carrell D, Selke S, Corey L. Polymerase chain reaction for detection of herpes simplex virus (HSV) DNA on mucosal surfaces: comparison with HSV isolation in cell culture. J Infect Dis. 2003;188(9):1345–1351. doi:10.1086/379043
11. Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8(1):1–21.
12. Kriesel JD, Bhatia AS, Barrus C, Vaughn M, Gardner J, Crisp RJ. Multiplex PCR testing for nine different sexually transmitted infections. Int J STD AIDS. 2016;27(14):1275–1282. doi:10.1177/0956462415615775
13. Boel CH, van Herk CM, Berretty PJ, Onland GH, van Den Brule AJ. Evaluation of conventional and real-time PCR assays using two targets for confirmation of results of the COBAS AMPLICOR Chlamydia trachomatis/Neisseria gonorrhoeae test for detection of Neisseria gonorrhoeae in clinical samples. J Clin Microbiol. 2005;43(5):2231–2235. doi:10.1128/JCM.43.5.2231-2235.2005
14. Tabrizi SN, Unemo M, Golparian D, et al. Analytical evaluation of GeneXpert CT/NG, the first genetic point-of-care assay for simultaneous detection of Neisseria gonorrhoeae and Chlamydia trachomatis. J Clin Microbiol. 2013;51(6):1945–1947. doi:10.1128/JCM.00806-13
15. Van Der Pol B, Ferrero DV, Buck-Barrington L, et al. Multicenter evaluation of the BDProbeTec ET system for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male urethral swabs. J Clin Microbiol. 2001;39(3):1008–1016. doi:10.1128/JCM.39.3.1008-1016.2001
16. Song T, Ye A, Xie X, et al. Epidemiological investigation and antimicrobial susceptibility analysis of ureaplasma species and Mycoplasma hominis in outpatients with genital manifestations. J Clin Pathol. 2014;67(9):817–820. doi:10.1136/jclinpath-2014-202248
17. Li K, Guo J, Zhao R, et al. Prevalence of 10 human polyomaviruses in fecal samples from children with acute gastroenteritis: a case-control study. J Clin Microbiol. 2013;51(9):3107–3109. doi:10.1128/JCM.01324-13
18. Peng J, Gao L, Guo J, et al. Type-specific detection of 30 oncogenic human papillomaviruses by genotyping both E6 and L1 genes. J Clin Microbiol. 2013;51(2):402–408. doi:10.1128/JCM.01170-12
19. Peng J, Li K, Zhang C, Gao L, Jin Q. Human papillomavirus and polyomavirus coinfections among Chinese men who have sex with men. J Infect. 2016;72(1):118–120. doi:10.1016/j.jinf.2015.09.012
20. Peng J, Li K, Zhang C, Jin Q. MW polyomavirus and STL polyomavirus present in tonsillar tissues from children with chronic tonsillar disease. Clin Microbiol Infect. 2016;22(1):97e91–97e93. doi:10.1016/j.cmi.2015.08.028
21. Peng J, Yang F, Xiong Z, et al. Sensitive and rapid detection of viruses associated with hand foot and mouth disease using multiplexed MALDI-TOF analysis. J Clin Virol. 2013;56(2):170–174. doi:10.1016/j.jcv.2012.10.020
22. Xiu L, Zhang C, Wu Z, Peng J. Establishment and application of a universal coronavirus screening method using MALDI-TOF mass spectrometry. Front Microbiol. 2017;8:1510. doi:10.3389/fmicb.2017.01510
23. Zhang C, Xiao Y, Du J, et al. Application of multiplex PCR coupled with matrix-assisted laser desorption ionization-time of flight analysis for simultaneous detection of 21 common respiratory viruses. J Clin Microbiol. 2015;53(8):2549–2554. doi:10.1128/JCM.00943-15
24. Zhang C, Xiu L, Xiao Y, Xie Z, Ren L, Peng J. Simultaneous detection of key bacterial pathogens related to pneumonia and meningitis using multiplex PCR coupled with mass spectrometry. Front Cell Infect Microbiol. 2018;8:107. doi:10.3389/fcimb.2018.00026
25. Gao L, Zhou F, Li X, Yang Y, Ruan Y, Jin Q. Anal HPV infection in HIV-positive men who have sex with men from China. PLoS One. 2010;5(12):e15256. doi:10.1371/journal.pone.0015256
26. Kessler HH, Muhlbauer G, Rinner B, et al. Detection of Herpes simplex virus DNA by real-time PCR. J Clin Microbiol. 2000;38(7):2638–2642.
27. Nicoll S, Brass A, Cubie HA. Detection of herpes viruses in clinical samples using real-time PCR. J Virol Methods. 2001;96(1):25–31.
28. Jensen JS, Borre MB, Dohn B. Detection of Mycoplasma genitalium by PCR amplification of the 16S rRNA gene. J Clin Microbiol. 2003;41(1):261–266. doi:10.1128/jcm.41.1.261-266.2003
29. Del Prete R, Ronga L, Lestingi M, et al. Simultaneous detection and identification of STI pathogens by multiplex Real-Time PCR in genital tract specimens in a selected area of Apulia, a region of Southern Italy. Infection. 2017;45(4):469–477. doi:10.1007/s15010-017-1002-7
30. Schmitt M, Depuydt C, Stalpaert M, Pawlita M. Bead-based multiplex sexually transmitted infection profiling. J Infect. 2014;69(2):123–133. doi:10.1016/j.jinf.2014.04.006
31. Cosentino LA, Danby CS, Rabe LK, et al. Use of nucleic acid amplification testing for diagnosis of extragenital sexually transmitted infections. J Clin Microbiol. 2017;55(9):2801–2807. doi:10.1128/JCM.00616-17
32. Bercot B, Amarsy R, Goubard A, et al. Assessment of coinfection of sexually transmitted pathogen microbes by use of the anyplex II STI-7 molecular kit. J Clin Microbiol. 2015;53(3):991–993. doi:10.1128/JCM.03370-14
33. Gaydos CA, Quinn TC, Willis D, et al. Performance of the APTIMA Combo 2 assay for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in female urine and endocervical swab specimens. J Clin Microbiol. 2003;41(1):304–309.
34. Gaydos CA, Cartwright CP, Colaninno P, et al. Performance of the Abbott RealTime CT/NG for detection of Chlamydia trachomatis and Neisseria gonorrhoeae. J Clin Microbiol. 2010;48(9):3236–3243.
35. Lee SJ, Park DC, Lee DS, Choe HS, Cho YH. Evaluation of Seeplex(R) STD6 ACE detection kit for the diagnosis of six bacterial sexually transmitted infections. J Infect Chemother. 2012;18(4):494–500.
36. Van Der Pol B. Profile of the triplex assay for detection of chlamydia, gonorrhea and trichomonas using the BD MAX System. Expert Rev Mol Diagn. 2017;17(6):539–547.
37. Van Der Pol B, Williams JA, Fuller D, Taylor SN, Hook EW
38. Tabrizi SN, Unemo M, Limnios AE, et al. Evaluation of six commercial nucleic acid amplification tests for detection of Neisseria gonorrhoeae and other Neisseria species. J Clin Microbiol. 2011;49(10):3610–3615.
39. Jalal H, Stephen H, Curran MD, Burton J, Bradley M, Carne C. Development and validation of a rotor-gene real-time PCR assay for detection, identification, and quantification of Chlamydia trachomatis in a single reaction. J Clin Microbiol. 2006;44(1):206–213.
40. O’Neil D, Doseeva V, Rothmann T, Wolff J, Nazarenko I. Evaluation of Chlamydia trachomatis and Neisseria gonorrhoeae detection in urine, endocervical, and vaginal specimens by a multiplexed isothermal thermophilic helicase-dependent amplification (tHDA) assay. J Clin Microbiol. 2011;49(12):4121–4125.
41. Melendez JH, Huppert JS, Jett-Goheen M, et al. Blind evaluation of the microwave-accelerated metal-enhanced fluorescence ultrarapid and sensitive Chlamydia trachomatis test by use of clinical samples. J Clin Microbiol. 2013;51(9):2913–2920.
42. Ripa T, Nilsson P. A variant of Chlamydia trachomatis with deletion in cryptic plasmid: implications for use of PCR diagnostic tests. Euro Surveill. 2006;11(11):E061109 061102.
43. Ripa T, Nilsson PA. A Chlamydia trachomatis strain with a 377-bp deletion in the cryptic plasmid causing false-negative nucleic acid amplification tests. Sex Transm Dis. 2007;34(5):255–256.
44. Fieser N, Simnacher U, Tausch Y, et al. Chlamydia trachomatis prevalence, genotype distribution and identification of the new Swedish variant in Southern Germany. Infection. 2013;41(1):159–166.
45. Seth-Smith HM, Thomson NR. Whole-genome sequencing of bacterial sexually transmitted infections: implications for clinicians. Curr Opin Infect Dis. 2013;26(1):90–98.
46. Weerakoon KG, Gordon CA, Williams GM, et al. Droplet digital PCR diagnosis of human schistosomiasis: parasite cell-free DNA detection in diverse clinical samples. J Infect Dis. 2017;216(12):1611–1622.
47. Blaya J, Lloret E, Santisima-Trinidad AB, Ros M, Pascual JA. Molecular methods (digital PCR and real-time PCR) for the quantification of low copy DNA of Phytophthora nicotianae in environmental samples. Pest Manag Sci. 2016;72(4):747–753.
48. Belmonte FR, Martin JL, Frescura K, et al. Digital PCR methods improve detection sensitivity and measurement precision of low abundance mtDNA deletions. Sci Rep. 2016;6:25186.
49. Kim EJ, Hladik W, Barker J, et al. Sexually transmitted infections associated with alcohol use and HIV infection among men who have sex with men in Kampala, Uganda. Sex Transm Infect. 2016;92(3):240–245.
50. Choe HS, Lee DS, Lee SJ, et al. Performance of Anyplex II multiplex real-time PCR for the diagnosis of seven sexually transmitted infections: comparison with currently available methods. Int J Infect Dis. 2013;17(12):e1134–e1140.
51. Zhu C, Liu J, Ling Y, et al. Prevalence and antimicrobial susceptibility of Ureaplasma urealyticum and Mycoplasma hominis in Chinese women with genital infectious diseases. Indian J Dermatol Venereol Leprol. 2012;78(3):406–407.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.