Back to Journals » Patient Preference and Adherence » Volume 11
Simulating clinical trial visits yields patient insights into study design and recruitment
Authors Lim SS, Kivitz AJ, McKinnell D, Pierson ME, O'Brien FS
Received 18 March 2017
Accepted for publication 4 July 2017
Published 31 July 2017 Volume 2017:11 Pages 1295—1307
DOI https://doi.org/10.2147/PPA.S137416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
S Sam Lim,1 Alan J Kivitz,2 Doug McKinnell,3 M Edward Pierson,4 Faye S O’Brien4
1Division of Rheumatology, Department of Medicine, Emory University, Atlanta, GA, USA; 2Altoona Center for Clinical Research, Altoona, PA, USA; 3Deloitte Life Sciences Advisory, Basel, Switzerland; 4Clinical Operations, Global Medicines Development, AstraZeneca, Gaithersburg, MD, USA
Purpose: We elicited patient experiences from clinical trial simulations to aid in future trial development and to improve patient recruitment and retention.
Patients and methods: Two simulations of draft Phase II and Phase III anifrolumab studies for systemic lupus erythematosus (SLE)/lupus nephritis (LN) were performed involving African-American patients from Grady Hospital, an indigent care hospital in Atlanta, GA, USA, and white patients from Altoona Arthritis and Osteoporosis Center in Altoona, PA, USA. The clinical trial simulation included an informed consent procedure, a mock screening visit, a mock dosing visit, and a debriefing period for patients and staff. Patients and staff were interviewed to obtain sentiments and perceptions related to the simulated visits.
Results: The Atlanta study involved 6 African-American patients (5 female) aged 27–60 years with moderate to severe SLE/LN. The Altoona study involved 12 white females aged 32–75 years with mild to moderate SLE/LN. Patient experiences had an impact on four patient-centric care domains: 1) information, communication, and education; 2) responsiveness to needs; 3) access to care; and 4) coordination of care; and continuity and transition. Patients in both studies desired background material, knowledgeable staff, family and friend support, personal results, comfortable settings, shorter wait times, and greater scheduling flexibility. Compared with the Altoona study patients, Atlanta study patients reported greater preferences for information from the Internet, need for strong community and online support, difficulties in discussing SLE, emphasis on transportation and child care help during the visits, and concerns related to financial matters; and they placed greater importance on time commitment, understanding of potential personal benefit, trust, and confidentiality of patient data as factors for participation. Using these results, we present recommendations to improve study procedures to increase retention, recruitment, and compliance for clinical trials.
Conclusion: Insights from these two studies can be applied to the development and implementation of future clinical trials to improve patient recruitment, retention, compliance, and advocacy.
Keywords: systemic lupus erythematosus, lupus nephritis, clinical trial simulation, patient recruitment, patient retention
Introduction
Lack of patient involvement and engagement in clinical trials is a major issue that results in low recruitment and retention.1–3 As a consequence, 45% of clinical trials are unable to recruit their target sample sizes.1 Furthermore, dropout rates of 30% have been reported for some clinical trials.3
Important factors that affect patient recruitment and retention for clinical trials are socioeconomic status and race.4–6 Patients with household incomes <$50,000 have 32% lower odds of participating in a clinical trial compared with higher-income patients.4 Although African-Americans represent 12% of the U.S. population, they make up only 5% of clinical trial participants.5 In addition, patients from racial minority groups have higher dropout rates in clinical trials compared with white patients.5,7
This underrepresentation of African-Americans is particularly relevant for systemic lupus erythematosus (SLE) clinical trials.6,8,9 African-Americans represent a substantial percentage of patients with SLE, with a prevalence of SLE in the United States of 112–119 per 100,000 for African-American women compared with 33–48 per 100,000 for white women.8,9 However, only 64.9% of African-Americans are willing to participate in a clinical trial for SLE compared with 84.3% of whites.6 Furthermore, in the only successful recent trial in SLE, the percentage of African-American patients was no more than 14.8% in any of the individual treatment arms.10 This Phase IIb trial evaluated anifrolumab, a fully human, immunoglobulin G1 κ monoclonal antibody that binds to and neutralizes receptors of all type I interferons and is in clinical development for the treatment of SLE and lupus nephritis (LN).10 In this trial, 12%–30% of the patients in each treatment arm discontinued treatment, including 3%–13% who withdrew consent.10
Understanding elements of clinical trial procedures that contribute to diminished recruitment and retention of patients is important, particularly when the afflicted population is from a minority group. These patients need sufficient representation in clinical trials so that researchers and patients can better understand the efficacy and safety of drugs in this population and results can be generalized to relevant patient groups.
To identify factors for improving clinical study protocols and study conduct, we obtained experiences from two simulations of draft Phase II and Phase III anifrolumab studies in which patients went through mock trial visits. One study involved African-American patients from an indigent care hospital in Atlanta, GA, USA, and the other study involved lower-middle-class white patients from a hospital in Altoona, PA, USA. Because this is a novel approach for understanding patient sentiments, we also present lessons learned from the development and implementation of trial simulations in the hope that these lessons will help to inform future efforts.
Materials and methods
Site feasibility
Two clinical trial simulations involving a mock trial environment were performed at separate clinical sites experienced with the SLE clinical trial process. One study site was at Grady Hospital, run by an Emory University School of Medicine investigator and associated staff (Atlanta study). Grady Hospital is a public hospital located in Atlanta, GA, with on site X-ray, electrocardiogram, clinical laboratory, and infusion facilities. The hospital serves a large number of low-income patients, many of whom are uninsured or underinsured, and the majority of whom are African-American. This site, which has been involved in >25 lupus clinical trials and other research studies, houses a large lupus clinic with >600 patients. Clinical research staff are dedicated and experienced in research involving this population, but the significant socioeconomic burdens of its patients are often a challenge.
The second site used was the Altoona Arthritis and Osteoporosis Center (Altoona study), a private health care practice in Altoona, PA, with on site magnetic resonance imaging, X-ray, dual-energy X-ray absorptiometry, and a clinical laboratory. This rheumatology facility has >10,000 registered patients, with a catchment area of up to 150 miles. The population that this facility serves has a median household income that is 68% of the national average, with 16% holding a bachelor’s degree or greater compared with 33% nationwide. This center has completed >1,000 clinical studies (34 SLE trials) for different commercial sponsors and clinical research organizations (CROs) and has dedicated, experienced study teams for clinical trials.
Simulation procedure
The clinical trial simulations were led by Deloitte (London, UK) on behalf of AstraZeneca. The clinical trial simulation study involved four phases: site feasibility assessment, patient recruitment, simulation of two visits of a clinical trial, and a debrief session to gain more insight into what was observed. For both studies, selected patients were directly contacted in person to participate, with no patients declining.
For the Altoona study, recruited patients had mostly mild and stable SLE, whereas for the Atlanta study, recruited patients met at least most of the inclusion and exclusion criteria for the Phase I and II trials for anifrolumab.11,12 Recruitment at both sites was nonbiased. During recruitment, patients were identified by site and provided with the simulation introduction letter, simulation participation agreement forms, and mock informed consent form. A booklet explaining the study was also given to patients to facilitate understanding of the study. For Atlanta study patients, this booklet was received at recruitment and patients had 2–3 days to review it. In the Altoona study, patients received this booklet at the mock screenings and could review it between visits.
Patients underwent a simulation of two key mock study visits for a clinical trial (informed consent procedure, SLE/LN screening visit, and SLE/LN dosing) with a debriefing period for patients and staff. The informed consent procedure, which lasted 30–45 minutes, was conducted by the investigator or study coordinator, according to the standard site practice. During the consent procedure, patients were briefed on visit simulations and procedures, and patient expectations were obtained. The mock SLE/LN screening visit lasted 2.5/2.0-2.5 hours for the Atlanta/Altoona studies. During the mock SLE/LN screening visit, patients were briefed to explain the simulation process and procedures along with patient expectations and received the study booklet (Altoona study). Afterward, they underwent all study procedures per protocol in a noninvasive format, including radiographs and blood draws. The mock SLE/LN first dosing visit lasted 4.5-5.0/3.5-4.0 hours for the Atlanta/Altoona study. Patients were briefed as before and underwent all mock first dosing visit study procedures per protocol, including mock anifrolumab infusion. The patient debrief involved a semi-structured interview conducted by Deloitte. In the Atlanta study, this research was supported by Parexel Clinical Trial Services (Waltham, MA, USA), which provided an African-American lead interviewer. In the patient debrief, patients were interviewed to collect first-hand perceptions on simulated visits, obtain descriptions of patients’ individual concerns, and incorporate discussion of patients’ personal perspectives. Interview questions were based on the patient sentiment assessment concepts listed in Figure 1. Patient-reported outcome questionnaires were provided in paper and electronic formats for patients to complete during each stage of the clinical trial simulation and took ~30 minutes to 1 hour to complete.
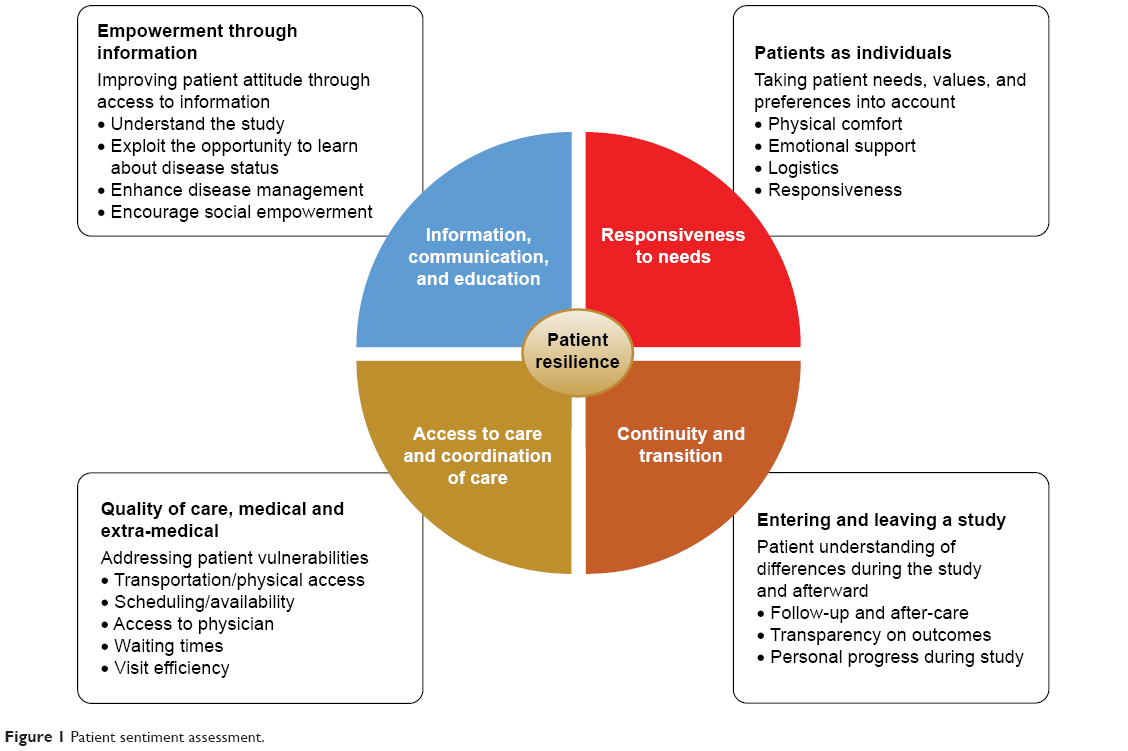 | Figure 1 Patient sentiment assessment. |
A standard staff preparation procedure was used for the trial simulation. Investigators and study coordinators were introduced to the trial simulation concept during the site feasibility and simulation preparation phases. Sites were provided simulation “playbooks,” which described the procedures and activities of all simulation participants, including the patients, site staff, and simulation team. Staff were allowed to use either source documentation templates that were prepared for the simulation or their own forms. Deloitte conducted the pre- and post-simulation briefings with investigators, study coordinators, and other participating staff members.
For the Altoona study, Schulman Associates Institutional Review Board (IRB; Cincinnati, OH, USA) reviewed the simulation summary and study materials. Based on a review of the materials, the IRB determined that a clinical trial simulation did not fall under the definition of clinical research and did not require ethics committee approval. For the Atlanta study, the study simulation proposal was presented to the Emory University IRB, which determined that the simulation did not fall under the definition of clinical research. All patients signed informed consent agreements to participate and to permit audio recordings. No patient-identifying information collected or generated was taken offsite. Transcripts from audio recordings were anonymized.
Analytical methodology
An analytical approach based on the frameworks developed by the Picker Institute and The Institute of Medicine was used to facilitate patient interviews and their subsequent analysis.13,14 Patient sentiment was assessed in the study to determine the impact on four patient-centric care domains: information, communication, and education; responsiveness to needs; access to care and coordination of care; and continuity and transition (Figure 1). Impact on patient resilience was also evaluated in the study, with four key aspects measured: physical, emotional, mental, and social. Patient responses were assessed centrally by Deloitte, with comparisons between the study site responses based on overall responses.
Results
The Atlanta study, which took place on April 2-3, 2015, involved six African-American patients (one male, five females) aged 27–60 years with moderate to severe SLE/LN. Five patients had no previous clinical trial experience (Table 1). In addition, patients differed in their cognitive abilities, general education level, and health literacy. The Altoona study took place on December 1–5, 2014, with 12 white females aged 32–75 years with mild to moderate SLE/LN; two participants had no previous clinical trial experience (Table 1).
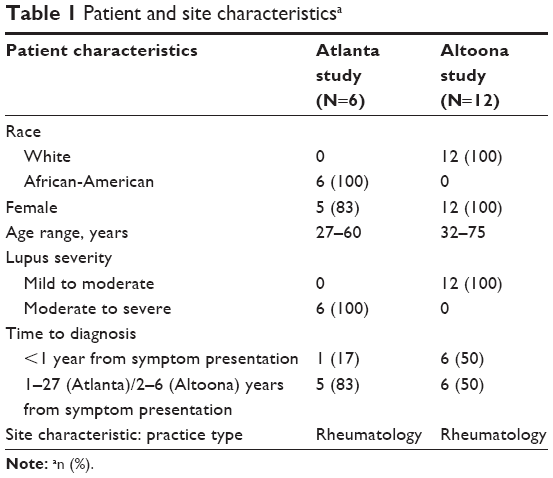 | Table 1 Patient and site characteristicsa |
Common experiences expressed by patients from the Atlanta and Altoona studies
Common positive and negative experiences were expressed by patients from both the Atlanta and the Altoona studies, and spanned across different regional, ethnic, and socioeconomic backgrounds (Figure 2). With respect to the information, communication, and education domain, patients found it valuable to have background material provided prior to or during the study. Patients thought that the informed consent forms were too long and complex and should be revised accordingly. They also thought it was critically important to have knowledgeable site staff for providing information on items including side effects, value of research, and answers to questions. In addition, patients expressed a need for and valued support from family and friends.
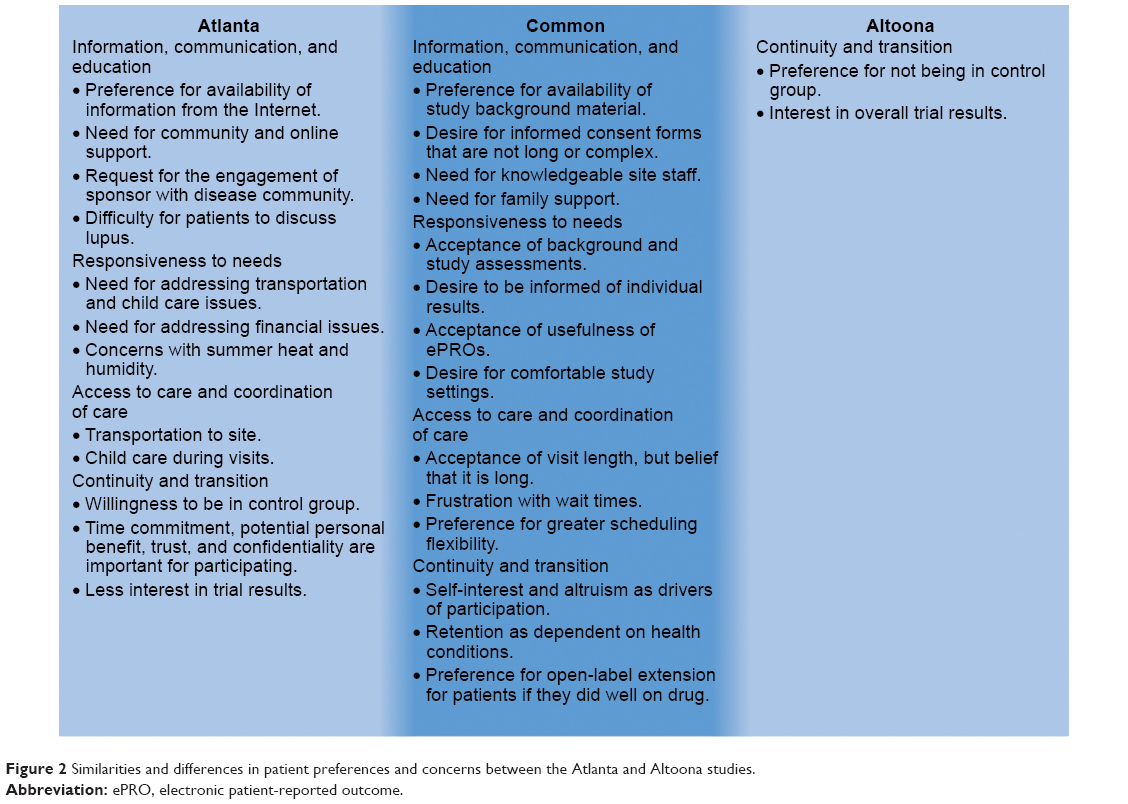 | Figure 2 Similarities and differences in patient preferences and concerns between the Atlanta and Altoona studies. |
Various common statements associated with responsiveness to needs were expressed. In general, patients did not have concerns with performing baseline and study assessments. They appreciated being informed of their personal results on an ongoing basis during the study. Patients found the various electronic patient-reported outcomes instruments relevant to their experience and easy to use. In addition, patients greatly appreciated comfortable settings, including entertainment and refreshments.
For access to care and coordination of care, patients mentioned that visit length, although often long, was acceptable. However, wait times between procedures were a source of frustration for patients. Patients desired flexibility for scheduling matters, such as adjustments for travel planning and family-related issues. Their preferences included flexibility in time windows for visits, availability of evening and weekend hours, and the option of dividing long visits over 2–3 days.
With respect to continuity and transition, patients in both studies indicated that trial participation was driven by a mixture of self-interest and altruism. Patient willingness to enroll in the study was strong, but retention was dependent on changes in health conditions during the trial. In addition, patients mentioned that if they did well on the study drug, they would be more likely to enroll in an open-label extension.
Different experiences expressed by patients from the Atlanta and Altoona studies
Atlanta study patients also expressed various different preferences and concerns from the Altoona study patients that could potentially be used in clinical trial development for enrolling and retaining African-American patients. These differences may be associated with the two study groups’ socioeconomic and racial dissimilarities. With regard to information, communication, and education, patients from the Atlanta study expressed a greater preference for information from the Internet and conveyed greater importance for strong community and online support than did patients from the Altoona study. Atlanta study patients also recommended that the study and/or sponsor engage with the community (via patient ambassadors or support group leaders) to provide education about the disease and to demonstrate the importance of these studies and their potential impact on patients. Furthermore, unlike Altoona study patients, the Atlanta study patients reported a taboo around discussing SLE that was associated with a lack of education.
For the responsiveness to needs domain, Atlanta study patients indicated a greater importance for transportation and child care help during the visits, particularly during summer months, than did Altoona study patients. Atlanta study patients also had more concerns related to financial matters, such as reimbursement of costs, impact on work, and the potential for stipends. They also mentioned heat and humidity during the summer months as potential issues for retention and compliance, although these concerns could potentially be related to the study location.
For care and coordination of care, Atlanta study patients placed greater emphasis on transportation and child care. With regard to the continuity and transition element, Atlanta study patients, because of their health insurance status (eg, lack of insurance, inadequate insurance), were more satisfied participating than were Altoona study patients, even if they were in the control group. In addition, they placed greater importance on time commitment, understanding of potential personal benefit, trust, and confidentiality of patient data as factors for participation. Furthermore, Atlanta study patients were less interested than Altoona study patients in eventually being told the general results of the trial.
Lessons learned for implementing clinical trial simulations
On the basis of our experience of developing and implementing two clinical trial simulations, we have identified certain factors that we view as important for a successful trial in different locations and for various demographic groups. For planning a clinical trial simulation, sufficient expertise for properly designing and implementing the study is necessary. Objectives of the study (eg, identifying factors to improve enrollment or areas of complexity in a protocol) should be clearly defined. Site selection should be based on factors pertinent to the particular simulation, such as respective disease area experience; racial, ethnic, and demographic interests; and clinical experience.
For patient recruitment, site directors and staff should make the effort to obtain patient trust, particularly for those patients who are unfamiliar with the site. Furthermore, inclusion of uninsured and underinsured patients should be considered because these patients would find it beneficial to receive treatment, even if in the placebo group. Uninsured and underinsured patients may be a particularly important population to include in trials that initially lack a representative number of minority patients.
For patient retention, responding to patient needs is important. Waiting facilities should be comfortable and should have entertainment provided. Site directors and staff should consider reducing patient wait time for procedures because a decrease in wait time would improve patient recognition that site staff members value their time. Another consideration for improving patient retention and engagement is to provide results that are easy for patients to comprehend so that they can understand their health status. The ever-increasing complexity of study protocols and regulations, coupled with the advanced language and extensive length of informed consent documents, requires the study team to demonstrate great sensitivity and adaptiveness for recognizing and supporting those with more limited health literacy.
The skill and attitude of the study coordinator(s) and site staff are also critically important for patient retention and engagement. Study team members should be nimble, sensitive, and reactive enough to allow for inevitable schedule changes. Site staff should anticipate the necessity of accommodating a patient’s schedule. This degree of schedule change impact may differ according to the region and time of year. Furthermore, site staff should better understand how patients view studies and study procedures. If patients express a desire to withdraw, site staff should discuss with them what could make the study a better experience for them.
Another important factor that we identified for a successful clinical trial simulation is the relationship between the CRO or sponsor and the site staff. A good relationship between the CRO or sponsor and the site staff is crucial, for it opens up lines of effective communication. There should be site feedback related to various aspects of the trial, and there should be responsiveness and accountability on the part of both the CRO or sponsor and the site staff. This factor is essential, for often a mechanism to provide feedback is missing. The relationship between the CRO or sponsor and the site staff is relevant also for dealing with issues that are culturally and community sensitive. For such issues, it is necessary to think creatively and develop different approaches. One such example is preparing patient materials that account appropriately for educational, ethnic, and socioeconomic differences. Furthermore, the CRO may have to tailor its approach directly to sites with significant numbers of patients from ethnic or racial minority groups or with lower socioeconomic status.
Site staff noted that they needed help managing the increased workload associated with protocol amendments. Site staff discouraged risk-based monitoring because of the time/work associated with lengthy monitoring forms.
Discussion
We present the concerns and preferences expressed by patients involved in two clinical trial simulations: one involving African-American patients with moderate to severe SLE/LN from an urban indigent care clinic in Atlanta, and the second involving white female patients with mild to moderate SLE and who were lower-middle-class. On the basis of a literature review, we believe that this is the first report of the use of a mock clinical trial approach that assessed/predicted patient sentiments during the actual clinical trial and proactively adjusted the protocol and the related operational details to optimize patient experience. Clinical trial simulations present various advantages versus other approaches used for obtaining patient feedback, including patient trial surveys and patient advisory boards. Simulations are uniquely designed for the particular trial being developed. For this reason, they can identify patient concerns for related studies in the future that would not necessarily be identified from literature reports involving studies with different trial designs and populations. Simulations can be designed to identify reasons for issues that the investigator expects to encounter in a particular study, such as difficulties in increasing the diversity of the patient population for particular racial or socioeconomic backgrounds. Findings from these simulations can thus improve the recruitment process, which subsequently can increase the retention rate in clinical trials. Simulations are performed in a real-world setting, involving both patient and site feedback. They differ from other types of studies, which lack feedback from some relevant participants and whose feedback is obtained potentially months after the event.
Several sentiments were previously known by the site staff and are consistent with reports from previous studies that evaluated patient surveys from clinical trials for other diseases.15,16 In a review of 4,961 surveys from patients at 15 U.S. clinical research centers, patients were more likely to rate their experience as highly favorable if they trusted their investigators and had good communication with them.15 Furthermore, most patients (85%) wished to receive results from the study.15 In a survey of patients infected with human immunodeficiency virus who participated in the ESPRIT study of different therapeutic regimens, 90% of patients indicated an altruistic reason for their involvement.16
Some of the findings reported in this study are analogous also to those in a report that investigated reasons for inadequate recruitment for a feasibility study in an SLE clinical trial.17 Patients in the study identified health status, involvement with their personal physician, the chance to learn more about their disease, and altruism as key factors in their decision to participate.17 Patients who did not participate in the study noted health status, medication concerns, randomization apprehensions, and personal issues (eg, time allocation) as reasons for not participating.17 In our Atlanta study, African-American patients with low income emphasized that studies should place greater consideration on their financial requirements and logistical needs, such as those related to transportation and child care.
Based on these results, we propose certain recommendations to improve study procedures to increase retention, recruitment, and compliance for clinical trials (Table 2). Although we were able to implement some of these recommendations in different ways in our studies, we were not able to apply all of them. In all cases, compliance and Good Clinical Trial Practice guidelines and appropriate country and local regulations would need to be met before applying these recommendations. Some of these recommendations may be relevant for simulations and clinical trials for diseases other than SLE. In addition, some of these recommendations may be particularly relevant for African-American patients.
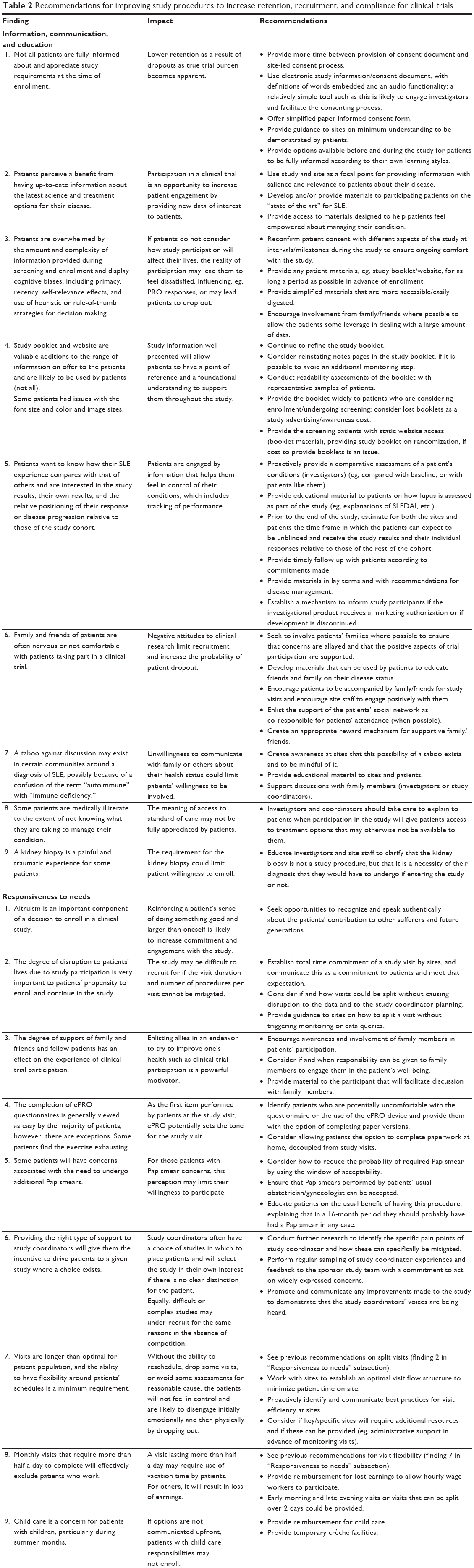  | Table 2 Recommendations for improving study procedures to increase retention, recruitment, and compliance for clinical trials |
Although these were SLE trial simulations, we believe that many of our findings would be useful in studies of other diseases. However, we understand that investigators may be interested in conducting simulations specific to their particular disease. Because implementation of clinical trial simulations is complicated, we recommend reviewing certain considerations from our experience before deciding if a trial simulation would be of value (Table 3). For instance, investigators should determine whether they fully understand the patient population, any difficulties in patient recruitment, and the complexity of the protocol. Furthermore, we recommend conducting such simulations in an established framework, as we have done, to analyze and report the findings more thoroughly.
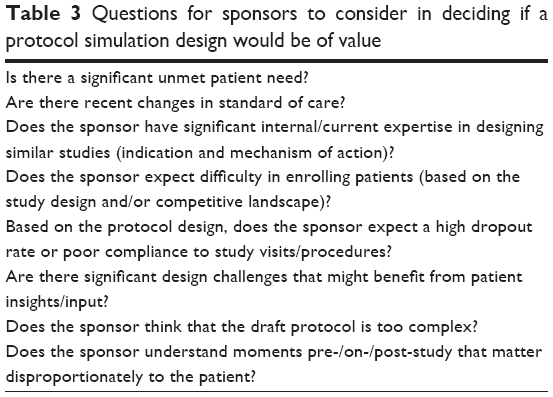 | Table 3 Questions for sponsors to consider in deciding if a protocol simulation design would be of value |
In conclusion, insights from these simulations can be directed toward designing future clinical trials to improve recruitment, retention, compliance, and advocacy, especially for minority patients.
Acknowledgments
Editorial assistance was provided by Alan Saltzman, of Endpoint Medical Communications, Conshohocken, PA, USA, and Michael A Nissen, ELS, of AstraZeneca. Study support was funded by AstraZeneca.
Disclosure
SSL and AJK are study investigators contracted by AstraZeneca and their respective institutions, DM is an employee of Deloitte and an AstraZeneca vendor. MEP and FSO are AstraZeneca employees. The authors report no other conflicts of interest in this work.
References
Sully BG, Julious SA, Nicholl J. A reinvestigation of recruitment to randomised, controlled, multicenter trials: a review of trials funded by two UK funding agencies. Trials. 2013;14:166. | ||
McDonald AM, Knight RC, Campbell MK, et al. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials. 2006;7:9. | ||
National Research Council Panel on Handling Missing Data in Clinical Trials. The Prevention and Treatment of Missing Data in Clinical Trials. Washington, DC: The National Academy Press; 2010. | ||
Unger JM, Gralow JR, Albain KS, Ramsey SD, Hershman DL. Patient income level and cancer clinical trial participation: a prospective survey study. JAMA Oncol. 2016;2(1):137–139. | ||
The Society for Women’s Health Research, United States Food and Drug Administration Office of Women’s Health. Dialogues on diversifying clinical trials. Successful strategies for engaging women and minorities in clinical trials. 2011. Available from: http://www.fda.gov/downloads/ScienceResearch/SpecialTopics/WomensHealthResearch/UCM334959.pdf. Accessed November 2, 2016. | ||
Vina ER, Utset TO, Hannon MJ, Masi CM, Roberts N, Kwoh CK. Racial differences in treatment preferences among lupus patients: a two-site study. Clin Exp Rheumatol. 2014;32(5):680–688. | ||
Cooper AA, Conklin LR. Dropout from individual psychotherapy for major depression: a meta-analysis of randomized clinical trials. Clin Psychol Rev. 2015;40:57–65. | ||
Lim SS, Bayakly AR, Helmick CG, Gordon C, Easley KA, Drenkard C. The incidence and prevalence of systemic lupus erythematosus, 2002–2004: the Georgia Lupus Registry. Arthritis Rheumatol. 2014;66(2):357–368. | ||
Somers EC, Marder W, Cagnoli P, et al. Population-based incidence and prevalence of systemic lupus erythematosus: the Michigan Lupus Epidemiology and Surveillance program. Arthritis Rheumatol. 2014;66(2):369–378. | ||
Furie R, Petri M, Zamani O, et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63(12):3918–3930. | ||
Furie R, Khamashta M, Merrill JT, et al. Anifrolumab, an anti-interferon-α receptor monoclonal antibody, in moderate-to-severe systemic lupus erythematosus. Arthritis Rheumatol. 2017;69(2):376–386. | ||
Goldberg A, Geppert T, Schiopu E, et al. Dose-escalation of human anti-interferon-alpha receptor monoclonal antibody MEDI-546 in subjects with systemic sclerosis: a phase 1, multicenter, open label study. Arthritis Res Ther. 2014;16(1):R57. | ||
Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. | ||
Institute of Medicine (US), Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. | ||
Kost RG, Lee LM, Yessis J, Wesley RA, Henderson DK, Coller BS. Assessing participant-centered outcomes to improve clinical research. N Engl J Med. 2013;369(23):2179–2181. | ||
Wendler D, Krohmal B, Emanuel EJ, Grady C; ESPRIT Group. Why patients continue to participate in clinical research. Arch Intern Med. 2008;168(12):1294–1299. | ||
Costenbader KH, Brome D, Blanch D, et al. Factors determining participation in prevention trials among systemic lupus erythematosus patients: a qualitative study. Arthritis Rheum. 2007;57(1):49–55. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.