Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Silent Lupus Nephritis: Renal Histopathological Profile and Early Detection with Urinary Monocyte Chemotactic Protein 1
Authors Gouda W ![]() , Abd elaziz Alsaid A, Abbas AS, Abdel-Aziz TM
, Abd elaziz Alsaid A, Abbas AS, Abdel-Aziz TM ![]() , Shoaeir MZ, Abd Elazem AAS, Sayed MH
, Shoaeir MZ, Abd Elazem AAS, Sayed MH
Received 6 May 2022
Accepted for publication 24 August 2022
Published 14 September 2022 Volume 2022:14 Pages 161—170
DOI https://doi.org/10.2147/OARRR.S373589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Chuan-Ju Liu
Wesam Gouda,1 Aldosoky Abd elaziz Alsaid,2 Awad Saad Abbas,1 Tarek M Abdel-Aziz,1 Mohamed Z Shoaeir,1 Abd Allah S Abd Elazem,3 Mohammad Hamdy Sayed4
1Department of Rheumatology, Faculty of Medicine, Al Azhar University, Assiut, Egypt; 2Department of Internal Medicine, Faculty of Medicine, Al Azhar University, Assiut, Egypt; 3Department of Medical Biochemistry, Faculty of Medicine, Suez University, Suez, Egypt; 4Department of Pathology, Faculty of Medicine, Al Azhar University, Assiut, Egypt
Correspondence: Wesam Gouda, Rheumatology Department, Faculty of Medicine, Al Azhar University, Al Azhar University Square, Assiut, 71524, Egypt, Tel +201002753754, Email [email protected]
Objective: Lupus nephritis (LN) affects almost half of all individuals with systemic lupus erythematosus (SLE). Overt LN (OLN) symptoms might vary from asymptomatic microscopic hematuria to renal failure. However, when there are no clinical or laboratory indicators of renal involvement, some people with silent LN (SLN) may have pathological evidence of renal involvement identified by renal biopsy. Monocyte Chemotactic Protein 1 (MCP-1) is a chemotactic factor that promotes leukocyte migration to the kidney. MCP-1 urine levels (uMCP-1) have been demonstrated to be high in individuals with active LN. The purpose of this study was to discover the occurrence of SLN, as well as the possible variations between overt LN (OLN) and SLN across SLE patients based on the histopathological assessment, as well as the role of uMCP-1 in the early detection of SLN.
Methods: An overall of 144 patients with SLE were included in the current research. Patients were subsequently divided into two groups: individuals who did not have clinical evidence of LN (84 patients) and those with OLN (60 patients). All the patients were subjected to the following investigations: uMCP-1, erythrocyte sedimentation rate (ESR), complement C3 (C3), complement C4 (C4), creatinine, albumin/creatinine ratio (uACR), creatinine clearance, quantitative assessment of proteinuria by 24-hour urine proteinuria (24hr UP) and percutaneous renal biopsy.
Results: Sixty patients from group I (71.4%) showed glomerular lesions on renal biopsy (SLN), and class II was the predominant class. uMCP-1 had a sensitivity of 95.2% and a specificity of 98% in the detection of SLN, and uMCP-1 values were markedly higher in patients with OLN in comparison to SLN.
Conclusion: The actual frequency of SLN may be higher than expected. High levels of uMCP-1 may have warranted the early activity of LN. uMCP-1 can be used as a non-invasive, useful tool for the prediction of LN.
Keywords: systemic lupus erythematosus, silent lupus-nephritis, overt lupus nephritis, urinary chemotactic protein 1, renal biopsy
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that affects many organs and manifests clinically in an exacerbation and remission course. In contrast to other organ affections, renal dysfunction is a serious challenge in SLE patients.1
To date, lupus nephritis (LN) affects more than half of all SLE patients, with approximately 55% of Asians and 51% of Africans. Many different clinical and pathological features of SLE are present in LN.2 Overt LN (OLN) symptoms might vary from asymptomatic microscopic hematuria to renal failure.3 If there are no clinical or laboratory indicators of renal impairment, some people with silent LN (SLN) may have pathological evidence of renal involvement verified by a renal biopsy. Following that, the incidence of LN is likely to be higher than previously stated.4,5
Pathological lesions in SLN patients are often modest. On the contrary, certain individuals may be diagnosed with diffuse proliferative glomerulonephritis, which is associated with a 60% fatality rate.6
Percutaneous renal biopsy is the gold standard approach for diagnosing and categorizing renal impairment, as well as measuring disease activity.7 Renal biopsy is required for individuals with SLN in order to get an accurate diagnosis and discover renal involvement in a timely manner.8 However, it is not routinely performed on SLE patients since some have normal renal findings while others have severe symptoms such as thrombocytopenia, infections, or neuropsychiatric involvement.9 Consequently, predictors of LN in SLE patients who do not have abnormal urine findings or renal impairment can assist clinicians in identifying cases where a renal biopsy should be done, allowing for early diagnosis of nephropathy, establishing a treatment strategy, and increased renal survival.10
Monocyte chemotactic protein-1 (MCP-1) is a chemotactic factor that promotes leukocyte migration to the kidney.11 MCP-1 is secreted by mesangial, podocyte, and monocyte cells in response to proinflammatory factors such as tumor necrosis factor alpha (TNF- α).
In turn, these inflammatory cells and chemicals cause tissue damage and contribute to the development of renal dysfunction. Furthermore, MCP-1 binding has been demonstrated to lower levels of nephrin, a key protector of kidney cell function12 and, MCP-1 suppression has been demonstrated to improve several inflammatory renal disorders, including diabetic nephropathy and SLE.13
Despite no difference in serum MCP-1 levels, diabetic nephropathy patients had considerably greater MCP-1 urine levels (uMCP-1) than control patients.14 uMCP-1 values have been demonstrated to be high in individuals with active LN during a renal exacerbation, and these values appear to decrease with effective LN therapy. Moreover, higher MCP-1 glomerular production appears to be indicative of worse renal outcomes in pediatric LN.11
Based on histopathological assessments, this study explored the potential distinction between OLN and SLN in SLE patients, as well as the role of uMCP-1 in the early diagnosis of SLN.
Materials and Methods
Study Design, Site, Population
This was a cross-sectional study that was performed at the Nephrology and Rheumatology Departments at Al-Azhar University Hospitals in Egypt between October 2020 and September 2021.
Eligibility Criteria
The present research included 144 individuals over the age of 18 who met at least four of the American College of Rheumatology (ACR) diagnostic criteria for SLE.15 After a thorough description of the research methodology and potential side effects, all participants provided informed consent.
Further, patients were categorized into two groups based on their clinical and laboratory findings: Group I, those who had no clinical signs of LN (84 patients), and group II, those with OLN (60 patients). Group I patients had normal creatinine levels (0.6–1.4 mg/dL), creatinine clearance (70–120 mL/minute/1.73 m2 body surface), with no urinary sediment, or proteinuria (<300 mg/day in 24-hour urine collection).
Group II patients with OLN had one or more of the following symptoms: hypertension (> 140/90 mmHg); edema; high creatinine levels (> 1.4 mg/dL); low creatinine clearance (70 mL/minute/1.73 m2 body surface); abnormal urinary sediment (> 5 leucocytes and/or > 5 red cells per 40x power field); and proteinuria (> 300 mg/day in 24-hour urine collection).
Exclusion Criteria
Patients who declined to have a renal biopsy, had an active infection, were pregnant, had substantial hypertension with a DBP > 120 mm Hg, diabetes, advanced renal failure as having a glomerular filtration rate (GFR) < 15 mL/min, or had abnormal coagulation profiles were all excluded from the study. Patients who had used glucocorticoids or immunosuppressive medicines in the previous three months, as well as those with drug-induced nephropathy, congenital renal, or urological disorders, were also excluded from the study.
Methods
Evaluation of Clinical Measurements
All patients had a detailed history and clinical assessment to determine their age, gender, weight, the duration of the disease, clinical signs of SLE, and comorbidities, as well as a general examination.
The SLE Disease Activity Index was used to measure SLE activity (SLEDAI). Patients were submitted for laboratory evaluation, including complete blood count (CBC), erythrocyte sedimentation rate (ESR), complement C3 (C3) and complement C4 (C4), anti-double-stranded DNA (anti-dsDNA) antibodies, serum albumin, creatinine, urine albumin/creatinine ratio (uACR), creatinine clearance (CCr), estimated glomerular filtration rate (eGFR), liver function tests, coagulation profile, urine analysis to exclude infection, and quantitative assessment of proteinuria by 24-hour urine proteinuria (24hr UP). All samples and corresponding laboratory examinations were collected before the renal biopsy and were performed in accordance with standard protocols.
Detection of uMCP-1
Urine samples were taken at 9 am and centrifuged for 10 minutes at 1000 rpm in the first 4 hours after they were taken. They were then stored at −80° until they were tested by an enzyme-linked immunosorbent assay (ELISA). Before the renal biopsy, uMCP-1 was measured in urine samples using the Human (CCL2/MCP-1 Quantikine ELISA kit, R & D Systems, USA). All reagents were generated in accordance with the manufacturer’s instructions, which included washing the samples before incubating them for 30 minutes at room temperature with the addition of 200 L of substrate into each well.
Finally, a stop solution was added to each well, and the optical density was measured using a 450 nm microplate reader. All samples were tested in duplicate, and values were recorded as pg/mg creatinine.
Evaluation of Renal Biopsy
All patients underwent percutaneous renal biopsy under local anesthesia and following ultrasonography localization of the left renal pole.
Immunofluorescent and optical microscopy were performed on the acquired tissues.
Hematoxylin-Eosin, PAS, Gomori trichrome, and silver methenamine-hematoxylin stains were used to stain paraffin slices in detail.
Human IgG, IgA, IgM, and complement (C3/C4) levels were measured using immunofluorescent microscopy following fluorescent antiserum treatment of kidney sections. The renal samples that were acquired were categorized using the International Society of Nephrology (ISN)/Renal Pathology Society (RPS) criteria. Aside from that, the activity and chronicity indices were computed.16
Statistical Analysis
For statistical analysis, SPSS software version 23 for Windows was used (SPSS Inc., Chicago, IL, USA). GraphPad Prism (GraphPad Software, Inc., San Diego) software version 7 was used to update the figures. The mean and standard deviation of continuous, normally distributed data were presented (SD). The median and range were used to represent continuous, non-normally distributed data, and the Mann–Whitney U-test was used to compare them. Following that, categorical variables were represented numerically and as percentages, and their respective groups were compared using the chi-square test. A correlation study was done on categorical data using Spearman’s rank correlation coefficient. The overall statistically significant difference was determined to be a P value of 0.001. To examine the contributions of age, sex, creatinine, urea, proteinuria, anti-DNA, C3, C4, AI and CI as predictors in explaining the variance in ISN/RPS renal biopsy Classification, a linear regression analysis was performed.
The features of urine MCP-1 levels that make them good at detecting and predicting LN activity were found by looking at receiver operating characteristic (ROC) curves.
Results
The current study recruited a total of 144 participants with SLE. Among them, 84 patients (group I) had no abnormal urinalysis or renal impairment. Whereas 60 patients had OLN (group II). Sixty patients from group I (71.4%) showed glomerular lesions on renal biopsy (SLN).
There were no statistically significant differences between the SLN and OLN groups considering age, sex, disease duration, and prebiopsy treatment history. In terms of the frequency of hypertensive patients, there was a significant difference (P < 0.001) between the SLN and OLN groups.
In the OLN group, 38 individuals had hypertension, while only six patients in the SLN group had hypertension (Table 1).
 |
Table 1 Demographic Features of the Included Patients |
Following the laboratory test, the mean creatinine and urea levels in the OLN groups were considerably higher (P < 0.001) than in the SLN patients. In particular, the mean creatinine levels in the SLN and OLN groups were 1.010.23 mg/dL and 3.240.97 mg/dL, respectively. Following that, the mean value of urea in the SLN group was 27.659.04 mg/dL, while it was 105.7527.31 mg/dL in the OLN group. When compared to the SLN group, the median values of 24hr UP in the OLN group were statistically (P > 0.001) higher. In this regard, the median value of 24-hour urine collection in the SLN and OLN groups was 72.5 mL and 300 mL, respectively. Similarly, the mean values of proteinuria in the SLN group were 85 mg, while it was 2000 mg in the OLN group. Also, there was a significant (P<0.001) difference between both groups regarding uMCP-1, where its mean +SD was higher in OLN patients 386.27 +124.52 than in SLN patients 270.67 +113.04. Only seven patients in the OLN group had red blood cells (RBCs) and granular casts in their urine. There was a statistically significant difference in the pattern of urine sediments between the two groups. Patients in the SLN group showed significantly lower levels of C3 and C4 (P<0.001), whereas 21 patients had lower levels of both C3 and C4. uMCP-1 correlated significantly with patients’ SLEDAI, 24hr UP, and anti-dsDNA antibodies (Table 2).
 |
Table 2 uMCP-1 Levels, Laboratory Characteristics and Disease Activity in Patients with SLN and OLN |
According to the ISN/RPS Classification, class II was the most common (34 patients) among SLN patients, whereas class V was the most common (22 patients) among OLN patients.
Furthermore, twenty-two and six patients in the SLN and OLN groups, respectively, were in class III. Eventually, no patients in the SLN group reached class VI (Table 3).
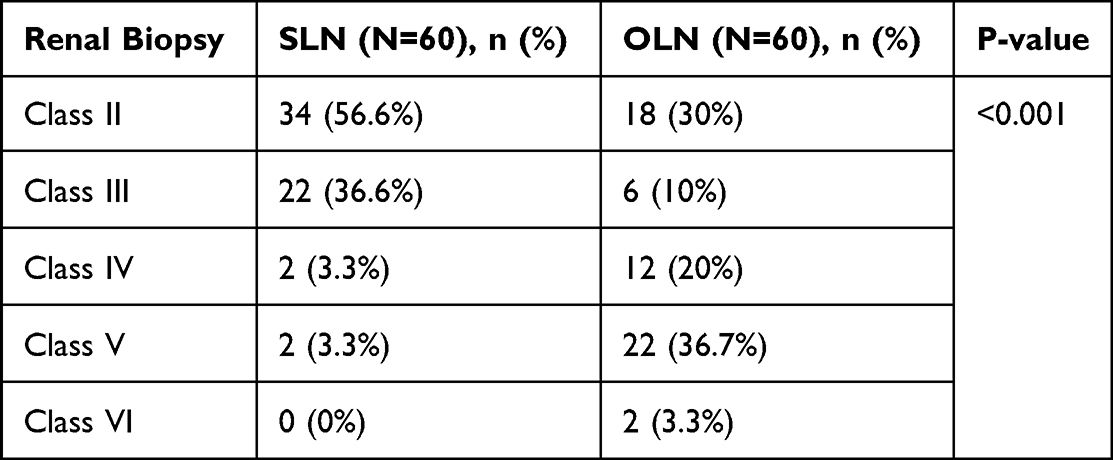 |
Table 3 ISN/RPS Classification of LN Among the Studied Groups |
In terms of activity index (AI), there was no significant difference between SLN and OLN patients (P=0.202), with a mean of 14.54.09 and 12.84.17 in the SLN and OLN groups, respectively.
In contrast, both groups exhibited statistically significant variations in the chronicity index (CI), with OLN patients experiencing considerably (P0.001) greater CI points than SLN patients (Table 4).
 |
Table 4 The Pattern of Chronicity and Activity Indexes Among the Studied Groups |
The presence of RBCs Cast (r=0.479, P=0.032) in urine and lower levels of C3, and C4 (r=0.676, P=0.001), on the other hand, revealed a strong positive correlation with the high LN grades among the SLN group. There is also a significant positive correlation between lupus nephritis classes and uMCP-1 (r=0.769, p0.001) (Table 5), (Figure 1). While lower levels of C4 (beta=−1.921, p=0.009) was negatively associated with renal biopsy classing (Table 6).
 |
Table 5 Correlations Between the Grading of Renal Biopsy and Other Parameters Among the Studied Groups |
 |
Table 6 Linear Regression Analysis Among the Studied Groups |
 |
Figure 1 Scatter plot describing the correlation between ISN/RPS renal biopsy classification and uMCP-1 levels. |
The ROC curve of uMCP-1 for the prediction of SLN showed that AUC was 0.958 and the cutoff value > 148.5 had a sensitivity of 95.2% and a specificity of 98% (Figure 2).
 |
Figure 2 Receiver operating characteristic (ROC) curves and corresponding areas under the curve (AUC) of uMCP-1 in prediction of SLN. Note: The AUC of uMCP-1 was 0.70 (95% CI 0.69–0.72). |
Discussion
LN is one of the most common and severe consequences of SLE. However, early identification of nephritis combined with the use of current therapeutic guidelines may greatly improve long-term outcomes. As a result, for effective therapy and follow-up of the glomerular lesion in SLN, a definite histologic diagnosis is essential.17
In the present work, Surprisingly, SLN was observed in 71.4% of SLE patients who did not have abnormal urinalysis or renal impairment prior to the renal biopsy. All paraclinical parameters, including S. creatinine, S. urea, and 24hr UP, were within their normal range in the SLN group. In contrast to the OLN group, renal lesions were detected in the SLN group despite the absence of renal symptoms, regardless of how long it had been since the diagnosis, patient age, or gender. These data matched the criteria of SLN, which specifies that “silent nephritis” is a substantial renal impairment that manifests in certain SLE patients in the absence of abnormal urinalysis findings or other clinical indications such as high blood creatinine and hypertension.18
Likewise, in an early report by Wakasugi et al,9 SLN was found to be present in 73% of SLE patients without clinical renal involvement. In addition, Ishizaki et al3 found that 75% of SLE patients who did not have an abnormal urinalysis had a SLN that was histopathologically proven.
Because the emergence of OLN is considered to be accelerated in SLN, our findings imply that SLN is a moderate type of LN. In our study, there was no significant difference between the SLN and OLN groups regarding the AI, despite the fact that the AI was relatively high among the OLN group. These findings show that it is hard to distinguish between SLE individuals who will develop OLN and those whose renal disease will remain quiet.
In terms of histological results, the current study found that the majority of patients in the SLN group showed intermediate histological staging (classes II and III) compared to the OLN group (classes IV and V).
Because of the large difference in the CI between the SLN and OLN groups, our findings imply that people with LN may have had a period of SLN before developing clinical and paraclinical symptoms. According to our findings, the majority of patients (63.3%) in the SLN group were in class II, whereas 37.5% and 25% of patients in the OLN group were in the IV and V classes, respectively.19 The locations of immune deposits in the mesangial, subendothelial, and/or sub-epithelial compartments of the glomerulus are generally associated with the types of glomerular damage found in SLE.20 Individuals with proliferative changes had shorter renal survival than those with mesangial lesions, according to a study examining kidney histopathological characteristics as significant markers of renal and patient survival in LN.21
Individuals with widespread proliferative LN may have a 60% mortality risk, with renal failure being a major cause of death despite treatment with glucocorticoids and immunosuppressive medications. Following that, it has been advocated that all lupus patients get a renal biopsy at the time of diagnosis in order to evaluate the prognosis and maybe the treatment strategy. This could be because reports suggest that clinical symptoms of renal involvement in the LN are nonspecific and can be found in different types of renal diseases.22
Clinical symptoms of SLE patients underestimate the degree of renal dysfunction. In our study, individuals with class III accounting for 25% of SLN had lower levels of creatinine, urea, and proteinuria compared to those with class II. According to pathophysiology, the occurrence of hematuria and proteinuria may be a sign of renal failure associated with SLE.23
In the current work, uMCP-1 showed a sensitivity of 95.2% and a specificity of 98% in detecting SLN, and uMCP-1 values were substantially higher in patients with OLN in comparison to SLN. Similarly, in an early report, El-Shahawy et al24 revealed that the uMCP-1 values of active patients were substantially greater than in controls. Furthermore, Alharazy et al25 found that uMCP-1 levels in patients with renal exacerbation were considerably greater than in non-renal exacerbation patients and controls. Singh et al26 discovered that uMCP-1 could tell the difference between people who had active LN and those who had inactive renal disease or stable SLE, while Torabinejad et al27 and Alharazy et al28 discovered that active LN patients had a higher value, which reduced in response to treatment.
Despite the data provided in the ongoing study, some limitations exist. The relatively small sample size, which addresses only a tiny proportion of patients with comparable environmental and demographic features, may limit our ability to generalize our findings. Furthermore, there is a lack of subsequent follow-up time, which restricts the capacity to recognize the development of SLN in both the short and long term to identify patients who would develop OLN within the SLN group. Larger and longer prospective research is recommended.
Conclusion
The actual frequency of SLN may be higher than expected. Although most cases among the SLN cases had moderate histopathological staging (ISN/RPS classes II and III), ISN/RPS classes III or IV were found in 6.6% of our study.
High levels of uMCP-1 may warrant early LN activity. We can use uMCP-1 with a cutoff value of > 148.5 pg/mg creatinine as a non-invasive useful tool for the prediction of LN. Early, accurate diagnosis and treatment are required to limit disease progression, morbidity, and death rates.
Abbreviations
AI, activity index; ACR, American College of Rheumatology; CI, chronicity index; C3, complement C3; C4, complement C4; CBC, complete blood count; ESR, erythrocyte sedimentation rate; ISN, International Society of Nephrology; LN, lupus nephritis; OLN, overt lupus nephritis; RBCs, red blood cells; RPS, Renal Pathology Society; SLN, Silent lupus nephritis; SLE, Systemic lupus erythematosus; uMCP-1, urinary Monocyte Chemotactic Protein 1.
Data Sharing Statement
The original data generated and analyzed for this study are included in the published article. Further inquiries can be directed to the corresponding author.
Ethical Approval
The study was conducted under the Helsinki Declaration. Ethics committee approval was received for this study from the ethics committee and IRB of Al Azhar University School of Medicine (No. 2020103–1), Assiut City, Egypt. All participants were given informed consent after a clear explanation of the study process and possible side effects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Mohamed El-Sayed K, Allam Mohamed E, Mohamed Rashed AS, Said Abd El-Aziz Shehata M, Mohamed Ragab Mandour E. Renal histopathological profile in patients with silent lupus nephritis. Al-Azhar Medl J. 2021;50(2):1281–1292. doi:10.21608/amj.2021.158472
2. Davidson A, Aranow C, Mackay M. Lupus Nephritis–challenges and progress. Curr Opin Rheumatol. 2019;31(6):682. doi:10.1097/BOR.0000000000000642
3. Ishizaki J, Saito K, Nawata M, et al. Low complements and high titre of anti-Sm antibody as predictors of histopathologically proven silent lupus nephritis without abnormal urinalysis in patients with systemic lupus erythematosus. Rheumatology. 2015;54(3):405–412. doi:10.1093/rheumatology/keu343
4. Hoover PJ, Costenbader KH. Insights into the epidemiology and management of lupus nephritis from the US rheumatologist’s perspective. Kidney Int. 2016;90(3):487–492. doi:10.1016/j.kint.2016.03.042
5. Moroni G, Depetri F, Ponticelli C. Lupus nephritis: when and how often to biopsy and what does it mean? J Autoimmun. 2016;74:27–40. doi:10.1016/j.jaut.2016.06.006
6. Xu S, Liu Z, Chen H, Zeng C, Zhang H, Hu W. Diffuse segmental and pure diffuse global proliferative glomerulonephritis: different patterns of class IV lupus nephritis. Clin Nephrol. 2014;81(6):411–418. doi:10.5414/CN108191
7. Hsieh SC, Tsai CY, Yu CL. Potential serum and urine biomarkers in patients with lupus nephritis and the unsolved problems. Open Access Rheumatol. 2016;8:81–91. PMID: 27843374; PMCID: PMC5098719. doi:10.2147/OARRR.S112829
8. Haładyj E, Cervera R. Do we still need renal biopsy in lupus nephritis? Reumatologia. 2016;54(2):61. doi:10.5114/reum.2016.60214
9. Wakasugi D, Gono T, Kawaguchi Y, et al. Frequency of class III and IV nephritis in systemic lupus erythematosus without clinical renal involvement: an analysis of predictive measures. J Rheumatol. 2012;39(1):79–85. PMID: 22089455. doi:10.3899/jrheum.110532
10. Park DJ, Choi SE, Xu H, et al. Chronicity index, especially glomerular sclerosis, is the most powerful predictor of renal response following immunosuppressive treatment in patients with lupus nephritis. Int J Rheum Dis. 2018;21(2):458–467. doi:10.1111/1756-185X.13254
11. Singh S, Wu T, Xie C, et al. Urine VCAM-1 as a marker of renal pathology activity index in lupus nephritis. Arthritis Res Ther. 2012;14(4):1. doi:10.1186/ar3912
12. Tarabra E, Giunti S, Barutta F, et al. “Effect of the monocyte chemoattractant protein-1/CC chemokine receptor 2 system on nephrin expression in streptozotocin-treated mice and human cultured podocytes,”. Diabetes. 2009;58(9):2109–2118. doi:10.2337/db08-0895
13. Haller H, Bertram A, Nadrowitz F, Menne J. Monocyte chemoattractant protein-1 and the kidney. Curr Opin Nephrol Hypertens. 2016;25(1):42–49. PMID: 26625862. doi:10.1097/MNH.0000000000000186
14. Kim MJ, Tam FW. Urinary monocyte chemoattractant protein-1 in renal disease. Clin Chim Acta. 2011;412(23–24):2022–2030. doi:10.1016/j.cca.2011.07.023
15. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. doi:10.1002/art.1780400928
16. Mubarak M, Nasri H. ISN/RPS 2003 classification of lupus nephritis: time to take a look on the achievements and limitations of the schema. J Nephropathol. 2014;3(3):87. doi:10.12860/jnp.2014.17
17. Fu SM, Sung SS, Wang H, Gaskin F. Pathogenesis of lupus nephritis Dubois’ Lupus Erythematosus and related syndromes; 2019:269–293.
18. Hong WA, Ren YL, Chang J, Luo GU, Ling-Yun SU. A systematic review and meta-analysis of prevalence of biopsy-proven lupus nephritis. Archiv Rheumatol. 2018;33(1):17. doi:10.5606/ArchRheumatol.2017.6127
19. Houssiau FA, Lauwerys BR. Current management of lupus nephritis. Best Pract Res Clin Rheumatol. 2013;27(3):319–328. doi:10.1016/j.berh.2013.07.004
20. Fibbe WE, Rabelink TJ. Mesenchymal stromal cells in lupus nephritis. Nat Rev Nephrol. 2017;13(8):452–453. doi:10.1038/nrneph.2017.100
21. Tang Y, Zhang W, Zhu M, et al. Lupus nephritis pathology prediction with clinical indices. Sci Rep. 2018;8(1):1–8. doi:10.1038/s41598-018-28611-7
22. Almaani S, Meara A, Rovin BH. Update on lupus nephritis. Clin J Am Soc Nephrol. 2017;12(5):825–835. doi:10.2215/CJN.05780616
23. Yu F, Haas M, Glassock R, Zhao MH. Redefining lupus nephritis: clinical implications of pathophysiologic subtypes. Nat Rev Nephrol. 2017;13(8):483–495. doi:10.1038/nrneph.2017.85
24. El-Shahawy EE, Gawish HH, Abd El-Bary EH. Serum, urinary and tissue monocyte chemoattractant protein 1 in patients with lupus nephritis (A comparative study). Life Sci J. 2012;9(2):865–873.
25. Alharazy S, Kong CT, Mohd M, Shah SA, Báin A, Abdul Gafor AH. Urinary monocyte chemoattractant protein and lupus nephritis activity. J Clin Cell Immunol. 2014;5(1):187.
26. Singh RG, Usha Rathore SS, Behura SK, Singh NK. Urinary MCP-1 as diagnostic and prognostic marker in patients with lupus nephritis flare. Lupus. 2012;21(11):1214–1218. doi:10.1177/0961203312452622
27. Torabinejad S, Mardani R, Habibagahi Z, et al. Urinary monocyte chemotactic protein-1 and transforming growth factor-b in systemic lupus erythematosus. Indian J Nephrol. 2012;22(1):5–12. doi:10.4103/0971-4065.91179
28. Alharazy S, Kong NC, Mohd M, Shah SA, Ba’in A, Abdul Gafor A. Urine monocyte chemoattractant protein-1 and lupus nephritis disease activity: preliminary report of a prospective longitudinal study. Autoimmune Dis. 2015;2015:962046. doi:10.1155/2015/962046
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.