Back to Journals » Patient Preference and Adherence » Volume 20
Silent Dissatisfaction Despite High Patient Satisfaction Scores: A Pilot Cross-Sectional Survey of Urban Patients with Prior Rural Care Experience at a Tokyo Dental Clinic
Authors Takahashi M
Received 11 February 2026
Accepted for publication 26 May 2026
Published 8 June 2026 Volume 2026:20 595537
DOI https://doi.org/10.2147/PPA.S595537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mami Takahashi
Faculty of Economics and Business Management, Shunan University, Shunan, Yamaguchi, Japan
Correspondence: Mami Takahashi, Faculty of Economics and Business Management, Shunan University, 843-4-2 Gakuendai, Shunan, Yamaguchi, 745-8566, Japan, Email [email protected]
Purpose: This pilot study examined whether patients who had experienced medical care in both urban and rural areas perceived differences in healthcare service experiences, negative emotions, and unvoiced concerns. The study focused on comparative perception and silent dissatisfaction that may not be captured by conventional patient satisfaction surveys.
Patients and Methods: A cross-sectional, anonymous, self-administered paper questionnaire was conducted at a cooperating dental clinic in Tokyo. The questionnaire addressed hospital visit experiences in urban and rural areas by the same healthcare recipient. The dental clinic was used as a pragmatic field site; the survey asked about medical care experiences rather than dental satisfaction. Descriptive statistics were calculated for 90 respondents.
Results: Among 90 respondents, 38 (42.2%) reported that they strongly or somewhat perceived differences between urban and rural care experiences, whereas 48 (53.3%) reported little or no difference and 4 (4.4%) were missing. Among the 38 respondents who perceived differences, 17 (44.7%) reported negative emotions such as inconvenience, discomfort, dissatisfaction, or endurance. Among the 20 respondents for whom expression of concerns was applicable, 7 (35.0%) communicated their concerns to the facility, whereas 13 (65.0%) did not. Among respondents with perceived differences who answered the comparison item, 8 of 32 (25.0%) reported that they recognized the feelings because they compared facilities across regions.
Conclusion: High satisfaction scores and low complaint rates should not be interpreted as evidence that dissatisfaction is absent. These pilot findings are consistent with, but do not directly test, a reference-point interpretation. Larger multi-site studies using validated instruments are needed to examine the proposed mechanism and its implications for patient feedback systems.
Plain Language Summary: Patients may report high satisfaction even when they have experienced inconvenience, discomfort, dissatisfaction, or the need to endure something during healthcare visits.
This pilot survey focused on people who had experienced care in both urban and rural areas because comparison across settings may make service-process differences more noticeable.
Some respondents reported negative feelings and concrete concerns, but not all communicated those concerns to the healthcare facility.
The findings suggest that high satisfaction scores and low complaint rates do not rule out dissatisfaction. Future studies should test this mechanism in larger multi-site samples and examine whether psychologically safe feedback routes improve detection of unvoiced dissatisfaction.
Keywords: patient satisfaction, silent dissatisfaction, urban-rural comparison, complaint behavior, healthcare quality
Introduction
Patient satisfaction is widely used as an indicator of healthcare quality, yet high satisfaction scores are not equivalent to the absence of dissatisfaction.1,2 In Japan, national, local government, and healthcare-related organizations conduct patient satisfaction or regional healthcare satisfaction surveys. These surveys often show that satisfied respondents constitute the majority and dissatisfied respondents are relatively fewer. The National Cancer Center Japan 2023 Patient Experience Survey reported a mean overall score of 8.2 out of 10 for overall evaluation of cancer diagnosis and treatment, and prefecture-level results are also publicly available.3 At least from publicly available results, patient experience evaluations do not appear to show extreme nationwide differences.
However, many of these existing surveys are cross-sectional. Respondents evaluate their own residential region or care experience, rather than the same individual comparing healthcare services across multiple regions. Therefore, an apparently small regional difference in conventional surveys does not directly demonstrate that differences in healthcare service experience are truly small. It may reflect evaluation based on locally formed standards without sufficient comparative reference points.
This study focuses on silent dissatisfaction, operationally defined as the coexistence of negative emotions or dissatisfaction-related descriptions with non-expression of concerns to the healthcare facility. The concept draws on the exit-voice framework, complaint behavior research, and organizational silence and voice theories adapted to a patient context.4–8
A central mechanism is the reference point. Patients who have experienced only one region may have a limited basis for judging whether a service process is worse, unfair, or uncomfortable, whereas those who have experienced both urban and rural contexts can compare and may be more likely to recognize problems as dissatisfaction. This logic is consistent with social comparison theory and reference-dependent evaluation.9,10
Japan provides a relevant context because universal health coverage coexists with regional differences in healthcare access and quality.11,12 Based on professional experience in healthcare and healthcare-related services across Japan, the author recognized the possibility that regional or facility-level differences may exist not only in medical techniques themselves but also in service experience, including interpersonal care, explanations, waiting experiences, facility flow, psychological consideration, communication, and hospitality.
In this study, healthcare service was defined broadly. It was not limited to medical techniques such as diagnosis and treatment, but included explanations, interpersonal care, waiting experiences, psychological consideration, communication, hospitality, appointment procedures, payment systems, and other patient touchpoints. Particular attention was paid to the possibility that, under information asymmetry between healthcare providers and patients, explanations may be perceived as one-way notifications rather than consultation or shared decision-making. This study does not prove that such communication structures are stronger in rural areas; rather, it treats this as an issue for future research.
Accordingly, this pilot study focused not on satisfaction within a single region, but on patients who had experienced medical care in both urban and rural settings. It used within-person comparative perception to explore whether differences in healthcare service experience and unvoiced dissatisfaction could be observed.
Participants and Methods
Study Design and Purpose
This was a cross-sectional, anonymous, self-administered paper questionnaire survey concerning hospital visit experiences in urban and rural areas by the same healthcare recipient. The purpose of the study was to examine whether differences in treatment satisfaction and healthcare service experience existed between urban and rural areas; it did not aim to estimate prefecture-level patient satisfaction.
Ethical Approval and Consent
This study was reviewed by the Shunan University Research Ethics Review Committee and approved by the Office of Research Promotion (approval number: 2023–19). The study period was from the date of ethics approval to March 31, 2024. The study was conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and return of the completed anonymous questionnaire after checking the consent box was treated as consented participation. Participants were informed that refusal to participate would not affect their care or evaluation. Because the questionnaire was anonymous, participants were also informed that, after collection, identifying and excluding a specific questionnaire would be difficult.
Study Setting
This pilot study used a dental clinic in Tokyo as the survey field. The setting was selected for feasibility and ethical/practical sensitivity, not as representative of all healthcare settings. The reasons were threefold.
First, the study examined comparative perceptions of healthcare service experiences between urban and rural areas rather than patient satisfaction within a single facility. In medical clinics, hospitals, or pharmacies, such a study could be interpreted as comparing facilities or regions and could involve reputational risk or perceived effects on patients and customers. Before this study, cooperation was sought from a nationwide pharmacy chain and a medical group operating several clinics in the Kanto region, but cooperation was not obtained. This experience indicated practical difficulty in building a cooperation framework for comparative evaluation studies in medical and pharmacy settings.
Second, Tokyo was considered an appropriate initial field for this pilot because, compared with rural areas, it has relatively more healthcare facility options, more available information about medical services, and a higher likelihood that patients have alternatives if they experience dissatisfaction or discomfort. Therefore, the research risk associated with regional comparison was considered lower in Tokyo than in rural settings.
Third, the survey questions asked about medical care experiences and were not designed to measure satisfaction with dental care. Nevertheless, dental care often involves repeated contact through regular visits, maintenance, and continuous management. The 2024 Survey of Dental Diseases by the Ministry of Health, Labour and Welfare reported that 63.8% of respondents had undergone a dental check-up within the past year, an increase from 58.0% in the 2022 survey.13 In addition, claims-data-based reports have indicated associations between dental care utilization and medical care utilization, and prior research in a general dental practice showed that medically compromised patients are present among dental patients.14,15 Thus, patients attending a dental clinic may have repeated experience with healthcare processes and may apply evaluative perspectives regarding explanation, interpersonal care, waiting, psychological consideration, and hospitality when receiving medical care.
Because the survey was conducted in a dental clinic, some respondents may have recalled dental care rather than medical care. This possibility is explicitly treated as a limitation. However, the central focus of this study was not the difference between medical and dental care, but whether differences in satisfaction and healthcare service experience existed across urban and rural care contexts.
Participants and Eligibility
Adults attending the cooperating dental clinic were invited to participate. Eligibility was based on self-reported current residence in an urban area and prior experience receiving healthcare in a rural area. The questionnaire asked about current residence, previous residence, distance and travel time to the main hospital, and experience of moving residence. A total of 90 respondents were included in the analysis.
Questionnaire Development
The questionnaire was developed to capture comparative perceptions of healthcare service experiences and silent dissatisfaction. It was informed by existing patient satisfaction and patient experience survey concepts and by the study objective. It was reviewed by a nursing expert researcher with extensive clinical experience. Formal psychometric validation was not conducted; therefore, the questionnaire should be understood as an exploratory instrument for a pilot study rather than as a validated scale. The full questionnaire is provided as Supplementary Appendix 1.
Data Collection and Protection of Individual Responses
Questionnaires were distributed and collected by clinic staff. Individual completed questionnaires were not made available to treating clinicians. This procedure was used to reduce the risk that individual responses would influence the clinical relationship and to protect participant anonymity. The questionnaire was anonymous and no personally identifying information was collected.
Measures
The questionnaire consisted of four sections: background, events during medical care, emotions at that time, and presence of a comparative reference. Background items included age, time flexibility for medical visits, current residence, previous residence, distance and travel time to the main hospital, and moving experience. The events section asked whether respondents had perceived differences between urban and rural areas when receiving medical care. For those who perceived differences, the questionnaire asked about specific situations: attitudes and consideration, explanations, conversations or questions, decisions about treatment policy or procedures, appointment scheduling, technical aspects of treatment or procedures, waiting time, payment or appointment systems, and other items. It also asked whether differences involved physicians, nurses, or other staff.
The emotion section asked whether the experience caused inconvenience, discomfort, dissatisfaction, or endurance. Respondents were then asked whether they had communicated the experience to the hospital or clinic. If not, they could select reasons, including no alternative hospital, reluctance to say it, fear of an angry or unpredictable reaction, anxiety about whether they would continue to receive appropriate treatment, or other reasons. The comparative-reference section asked whether respondents would have had the same feelings if they had known only that region, and whether they recognized the feelings because they were comparing the facility with facilities in other regions.
Analysis
Descriptive statistics were calculated as counts and percentages. Denominators are shown in the relevant tables and text. Free-text responses were examined using single-coder pilot coding with a preliminary codebook focused on service-process issues. Reporting was informed by relevant elements of STROBE and SRQR.16,17 This pilot study was exploratory and was not powered for hypothesis testing. Therefore, the analysis focused on descriptive patterns and did not aim to conduct causal inference or statistical estimation of regional differences.
Results
Respondent Characteristics
A total of 90 respondents were included in the analysis. Table 1 summarizes respondent characteristics. Respondents were mainly in their 20s and 30s, with 21 respondents (23.3%) in their 20s and 35 (38.9%) in their 30s. Nine respondents (10.0%) were in their 40s, 10 (11.1%) were in their 50s, and 6 (6.7%) were aged 60 years or older. Four respondents (4.4%) selected “other”, and 5 (5.6%) had missing age data. Most respondents currently lived in Tokyo’s 23 wards (67, 74.4%), followed by Kanagawa, Saitama, or Chiba (11, 12.2%) and other metropolitan areas (4, 4.4%); 8 responses (8.9%) were missing for current residence. Time flexibility for medical visits varied: 18 respondents (20.0%) reported very flexible scheduling, 28 (31.1%) reported somewhat flexible scheduling, 22 (24.4%) reported somewhat difficult scheduling, and 11 (12.2%) reported difficult scheduling. Eleven responses (12.2%) were missing, other, or ambiguous.
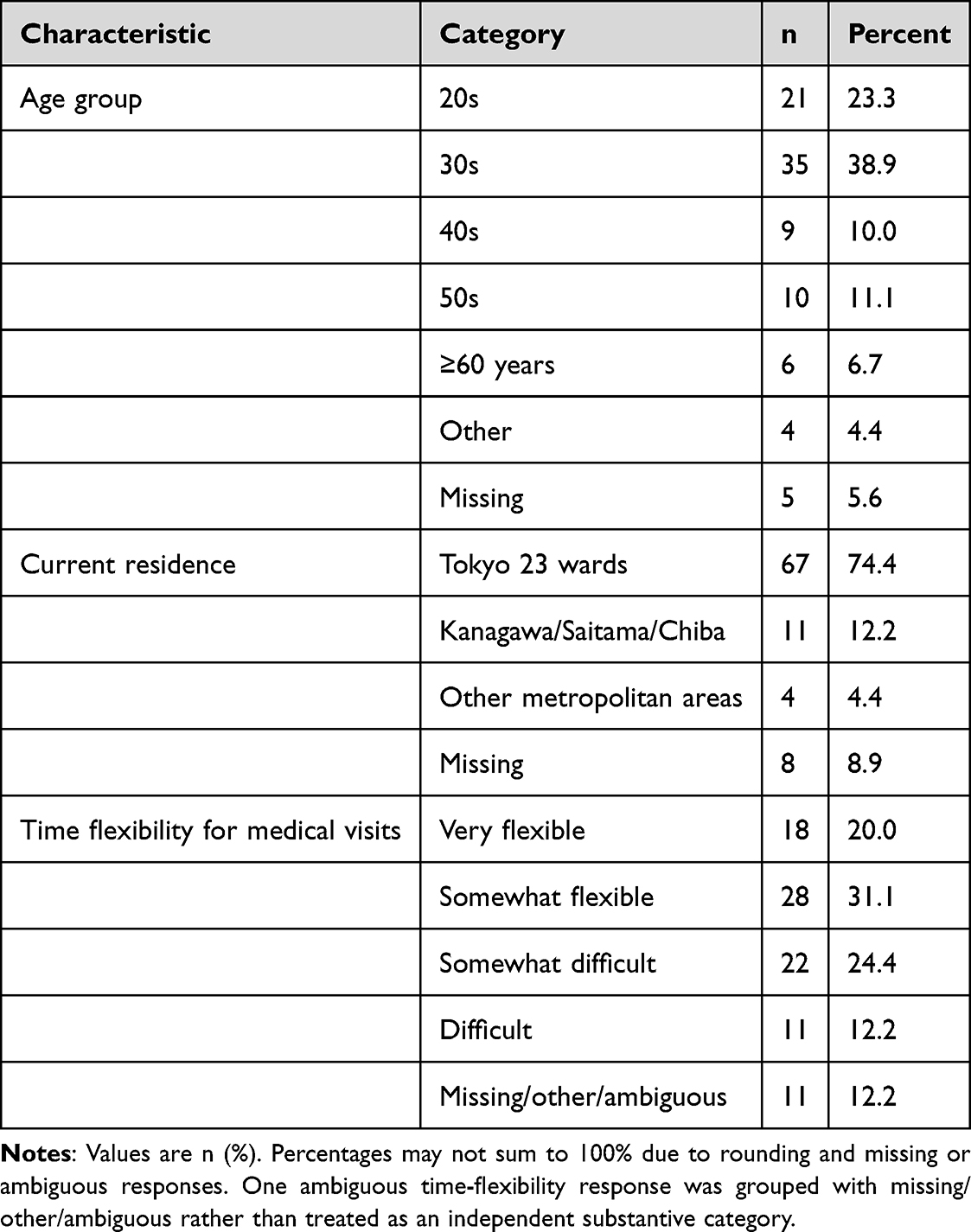 |
Table 1 Participant Characteristics |
Perceived Differences, Negative Emotions, and Expression of Concerns
Table 2 summarizes perceived urban-rural differences, negative emotional responses, expression of concerns, reasons for not expressing concerns, and comparison-related responses. While 38 respondents (42.2%) reported that they strongly or somewhat perceived urban-rural differences, 48 respondents (53.3%) reported little or no difference, and 4 (4.4%) had missing responses. Among the 38 respondents who perceived differences, 17 (44.7%) reported negative emotions such as inconvenience, discomfort, dissatisfaction, or endurance; 20 (52.6%) did not, and 1 (2.6%) had a missing response.
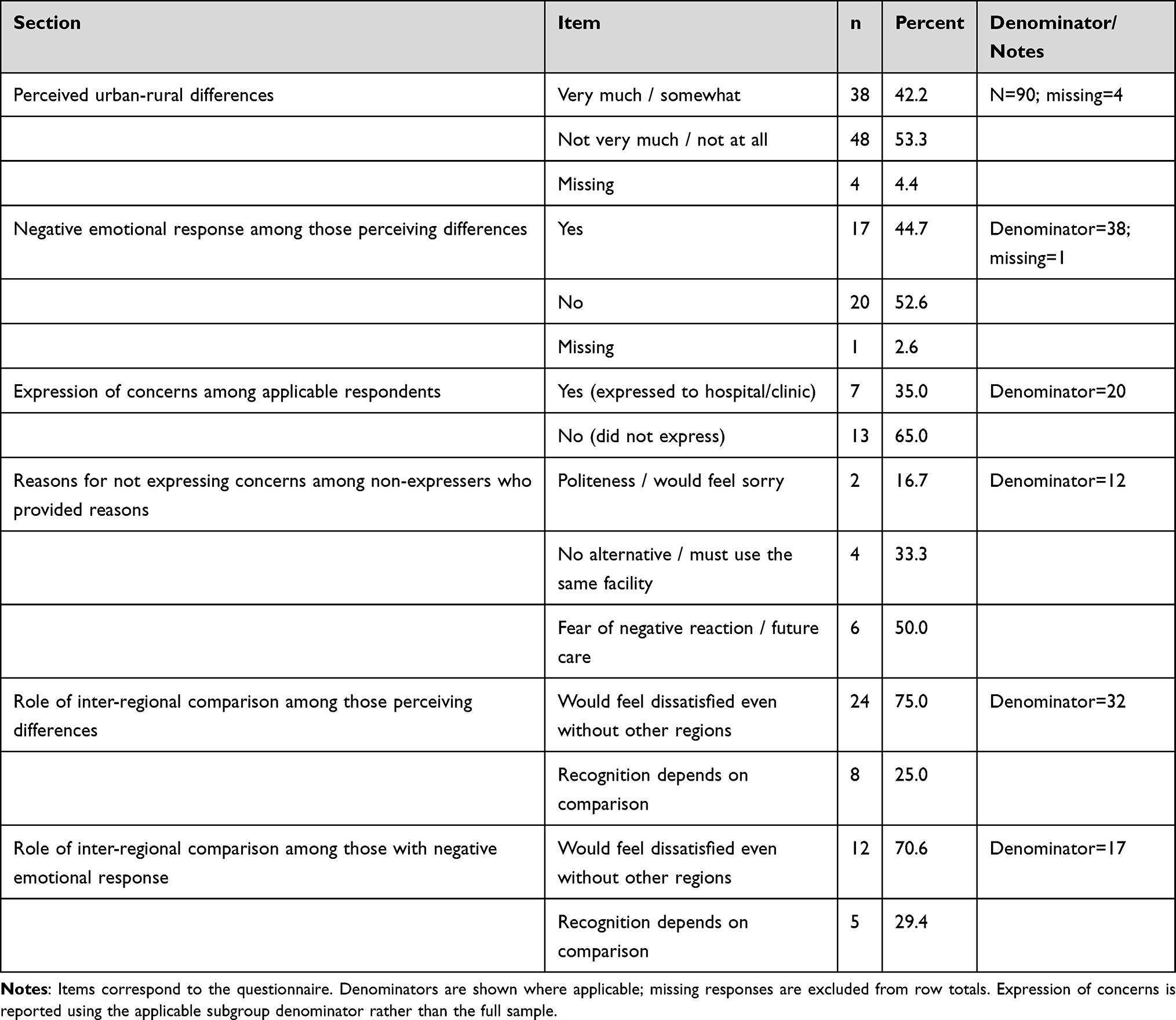 |
Table 2 Perceived Urban-Rural Differences, Emotional Responses, Expression of Concerns, and Comparison Dependence |
Among the 20 respondents for whom expression of concerns was applicable, 7 (35.0%) communicated their experience to the hospital or clinic, whereas 13 (65.0%) did not. Among the 12 non-expressers who provided reasons, 2 (16.7%) indicated politeness or feeling sorry, 4 (33.3%) indicated no alternative or the need to use the same facility, and 6 (50.0%) indicated fear of a negative reaction or anxiety about future care.
Regarding the reference-point item, among 32 respondents who perceived differences and answered the comparison item, 24 (75.0%) indicated that they would have felt dissatisfied even without knowing other regions, whereas 8 (25.0%) reported that they recognized the feelings because they were comparing facilities across regions. Among 17 respondents with negative emotional responses, 12 (70.6%) indicated that they would have felt dissatisfied even without other regions, whereas 5 (29.4%) indicated that recognition depended on comparison. These findings are descriptive and do not test the reference-point mechanism, but they suggest that, for some respondents, within-person inter-regional comparison may have contributed to recognition of dissatisfaction or discomfort.
Discussion
This pilot study examined comparative perceptions of urban and rural healthcare service experiences among respondents with experience in both settings. The main finding is that high satisfaction and low complaint rates do not rule out dissatisfaction. A subset of respondents perceived differences between urban and rural care experiences, and among those with applicable concern-expression items, a majority did not communicate their concerns to the facility.
The findings are consistent with, but do not directly test, a reference-point interpretation. Some respondents reported that they recognized feelings such as inconvenience, discomfort, dissatisfaction, or endurance because they compared facilities across regions. This is aligned with social comparison and reference-dependent evaluation frameworks, in which recognition of dissatisfaction may depend on the availability of a comparator.9,10
The questionnaire structure directly addressed silent dissatisfaction by asking not only whether respondents perceived differences, but also in which situations and with which staff members those differences occurred, whether negative emotions were experienced, whether the experience was communicated to the facility, and why it was not communicated. These items help distinguish an absence of complaints from an absence of negative experience. Figure 1 summarizes the proposed conceptual model used to frame the relationship between within-person inter-regional comparison, recognition of inconvenience, discomfort, dissatisfaction, or endurance, expression or non-expression of concerns, and barriers to speaking up.
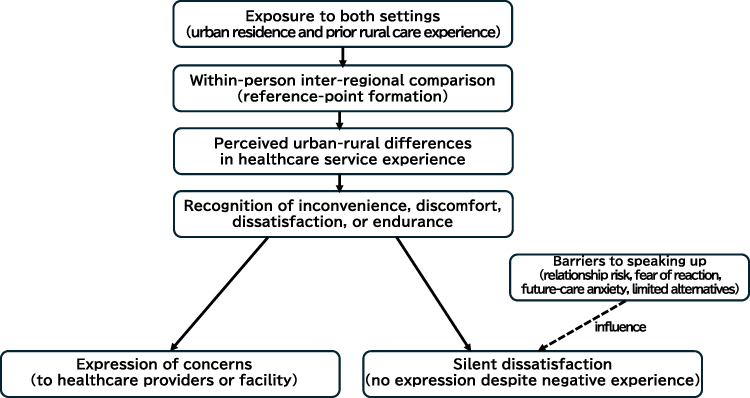 |
Figure 1 Conceptual model of reference-point and silent dissatisfaction mechanisms. Inter-regional comparison refers to within-person comparison between urban and rural healthcare experiences. Barriers to speaking up are shown as factors influencing whether negative experiences remain unexpressed as silent dissatisfaction. |
This study does not demonstrate that one-way communication or suppressed voice is stronger in rural areas. That issue remains a question for future research. The present study instead provides exploratory evidence that conventional single-region satisfaction surveys may fail to capture within-person comparative perceptions and unvoiced dissatisfaction.
For practice, this pilot suggests that healthcare providers should be cautious about interpreting high satisfaction scores or few complaints as evidence that dissatisfaction is absent. It warrants further study whether low-burden and psychologically safe feedback routes can improve detection of unvoiced dissatisfaction. However, the present study did not evaluate any feedback intervention.
Limitations
This study has several limitations. First, it was a single-site pilot study conducted at a dental clinic in Tokyo, and national representativeness cannot be claimed. Second, although the questionnaire was designed to ask about medical care experiences, some respondents may have recalled dental care because the survey was conducted in a dental setting. Third, the questionnaire was exploratory and was not formally psychometrically validated. Fourth, the study relied on retrospective self-report, which may have been affected by response processes in sensitive surveys.18 It did not measure objective medical quality, clinical outcomes, healthcare resource levels, or facility performance.19
Fifth, although clinic staff distributed and collected the questionnaires and treating clinicians could not view individual responses, hand distribution in a healthcare setting may still have reduced willingness to report negative experiences.18 Finally, this study cannot prove causal pathways linking regional structure, information asymmetry, patient participation, limited alternatives, and voice suppression. These mechanisms require future multi-site studies using validated instruments.
Conclusion
This exploratory pilot survey suggests that high patient satisfaction and low complaint rates do not necessarily indicate the absence of dissatisfaction. Among respondents with experience in both urban and rural care contexts, some perceived regional differences, experienced negative emotions, and did not communicate concerns to the facility. These findings are consistent with, but do not directly test, a reference-point interpretation. Larger multi-site studies with validated instruments are needed to examine the mechanism and its implications for patient feedback systems.
Data Sharing Statement
The de-identified dataset and the English translation of the questionnaire can be made available from the corresponding author upon reasonable request, subject to institutional policy and participant confidentiality.
Ethics Approval and Informed Consent
Ethics approval was obtained from the Shunan University Research Ethics Review Committee and approved by the Office of Research Promotion (approval number: 2023-19). Participants received written information about the study, voluntariness, anonymity, and data handling. Checking the consent box and returning the anonymous questionnaire were treated as consented participation. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The author thanks the staff and patients of the cooperating dental clinic for their participation in the pilot survey and the colleagues who commented on the questionnaire design. The author also thanks the nursing expert researcher with extensive clinical experience who reviewed the questionnaire.
Funding
This study was supported by the 2023 Shunan University Internal Research Grant Program for Supporting Female Researchers. The funder had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Cleary PD, McNeil BJ. Patient satisfaction as an indicator of quality care. Inquiry. 1988;25(1):25–9.
2. Sitzia J, Wood N. Patient satisfaction: a review of issues and concepts. Soc Sci Med. 1997;45(12):1829–1843. doi:10.1016/S0277-9536(97)00128-7
3. National Cancer Center Japan. Report on the 2023 patient experience survey. Tokyo: National Cancer Center Japan; 2024. Available from: https://www.ncc.go.jp/jp/icc/policy-evaluation/project/010/2023/index.html.
4. Hirschman AO. Exit, Voice, and Loyalty: Responses to Decline in Firms, Organizations, and States. Cambridge, MA: Harvard University Press; 1970.
5. Reader TW, Gillespie A, Roberts J. Patient complaints in healthcare systems: a systematic review and coding taxonomy. BMJ Qual Saf. 2014;23(8):678–689. doi:10.1136/bmjqs-2013-002437
6. Singh J. Consumer complaint intentions and behavior: definitional and taxonomical issues. J Mark. 1988;52(1):93–107. doi:10.1177/002224298805200108
7. Morrison EW, Milliken FJ. Organizational silence: a barrier to change and development in a pluralistic world. Acad Manage Rev. 2000;25(4):706–725. doi:10.2307/259200
8. Van Dyne L, Ang S, Botero IC. Conceptualizing employee silence and employee voice as multidimensional constructs. J Manage Stud. 2003;40(6):1359–1392. doi:10.1111/1467-6486.00384
9. Festinger L. A theory of social comparison processes. Hum Relat. 1954;7(2):117–140. doi:10.1177/001872675400700202
10. Tversky A, Kahneman D. Loss aversion in riskless choice: a reference-dependent model. Q J Econ. 1991;106(4):1039–1061. doi:10.2307/2937956
11. Ikegami N, Yoo B-K, Hashimoto H, et al. Japanese universal health coverage: evolution, achievements, and challenges. Lancet. 2011;378(9796):1106–1115. doi:10.1016/S0140-6736(11)60828-3
12. Kaneko M, Ohta R, Mathews M. Rural and urban disparities in access and quality of healthcare in the Japanese healthcare system: a scoping review. BMC Health Serv Res. 2025;25(1):667. doi:10.1186/s12913-025-12848-w
13. Ministry of Health, Labour and Welfare. Summary of the 2024 survey of dental diseases. Tokyo: Ministry of Health, Labour and Welfare; 2025. Available from: https://www.mhlw.go.jp/stf/newpage_59190.html.
14. Ministry of Health, Labour and Welfare. Summary of research studies on dental and oral health. Tokyo: Ministry of Health, Labour and Welfare; 2024. Available from: https://www.mhlw.go.jp/content/11201250/001306353.pdf.
15. Iijima M, Shinozuka Y, Takahashi K. Ippan shika shinryojo no shoshin kanja ni okeru yubyosharitsu ni tsuite [Prevalence of medically compromised patients among first-visit patients in a general dental practice]. Nihon Yubyosha Shika Iryo Gakkai Zasshi. 2003;12(1):7–12. Japanese.
16. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
17. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
18. Tourangeau R, Yan T. Sensitive questions in surveys. Psychol Bull. 2007;133(5):859–883. doi:10.1037/0033-2909.133.5.859
19. Donabedian A. The quality of care. How can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.1988.03410120089033
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Patient Satisfaction With MRI Department Services and Staff in Saudi Hospitals
Alghamdi SA
Risk Management and Healthcare Policy 2025, 18:419-428
Published Date: 12 February 2025
Patient Satisfaction with Primary Health Care Services in Riyadh, Saudi Arabia
Albaqami NM, Alshagrawi S
International Journal of General Medicine 2025, 18:835-845
Published Date: 17 February 2025