Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Silanizing Effectiveness on the Bond Strength of Aged Bulk-Fill Composite Repaired After Sandblasting or Bur Abrasion Treatments: An in vitro Study
Authors Hashim H, Abd-alla MH
Received 17 July 2022
Accepted for publication 30 August 2022
Published 5 September 2022 Volume 2022:14 Pages 265—273
DOI https://doi.org/10.2147/CCIDE.S381235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Huda Hashim, Manal Hussain Abd-alla
Department of Conservative Dentistry, College of Dentistry, Mustansiriyah University, Baghdad, Iraq
Correspondence: Huda Hashim, Department of Conservative Dentistry, College of Dentistry, Mustansiriyah University, Baghdad, Iraq, Tel +9647717485368, Email [email protected]
Objective: To measure the repair shear bond strength (SBS) of an aged bulk-fill composite after different mechanical (diamond bur vs sandblasting) and chemical (universal adhesive with or without a previous silanization) surface treatments.
Materials and Methods: Bulk-fill composite (Filtek One Bulk Fill, 3M ESPE) was used to construct seventy-two specimens aged through 10,000 thermal cycles. The specimens were allocated into two groups (n = 36 each) according to the mechanical roughening: Db, treated with a diamond bur, and Sb, treated by sandblasting. Each group was further subdivided into three subgroups (n = 12 each) according to the chemical conditioning: Db-only and Sb-only, unconditioned specimens; Db-U and Sb-U, specimens were conditioned with silane-containing universal adhesive (Scotchbond Universal adhesive, 3M ESPE); and Db-S-U and Sb-S-U, specimens were conditioned with a silane agent (Prosil, FGM) before employing the universal adhesive. The same composite material was used for repair. An additional reference group was constructed to measure the cohesive strengths of the bulk-fill composite. SBS testing was performed using a universal testing machine at a crosshead speed of 1 mm/min, and the failure modes were evaluated by stereomicroscope. The surface topography of resin composite after roughening was assessed by scanning electron microscopy. SBS data were statistically analyzed by ANOVA, Tukey’s test and independent t-test.
Results: The significantly highest SBS was recorded in the reference group (P ≤ 0.05). Sb-only obtained significantly higher SBS than Db-only (P < 0.001). No significant difference in SBS was noted between Db-U and Sb-U or Db-S-U and Sb-S-U. Likewise, no significant difference was observed between the subgroups treated with or without silane (P > 0.05).
Conclusion: The sandblasted specimens demonstrated a higher repair SBS than the diamond bur-treated specimens. The use of an additional silanizing step before applying silane-containing universal adhesive did not enhance the SBS of the repaired composite.
Keywords: repair, bulk-fill composite, shear bond strength, silane, surface treatment, universal adhesive
Introduction
Composite resins are very popular for restoring anterior and posterior teeth.1 Although composite resins have improved significantly in recent years, failures may still occur due to fractures, secondary caries, discoloration, and marginal defects.2 There are two differing opinions on whether to replace or repair defective restorations. The complete replacement does not comply with the minimally invasive treatment concept and is more time-consuming and costly when compared to repairing the restoration.3 In contrast, the repair is considered a contemporary approach for preserving tooth structure and increasing the survival of direct restorations, avoiding more invasive treatments.4
Successful repairs require good adhesion between the new repair composite and the aged substrate. Achieving adhesion with the aged composite is extremely challenging because they lack an oxygen-inhibited layer of unpolymerized resin,5 have fewer unreacted C–C double bonds, and undergo material degradation through water uptake.6,7 Thus, mechanical and chemical surface conditioning protocols are required to overcome these challenges and improve the repair bond strength.5,8 However, to the best of our knowledge, a gold standard for treating aged composite surfaces has not been established so far.9
Previous studies of mechanical surface treatments have demonstrated that roughening aged composites with diamond burs10–12 or aluminum oxide (Al2O3) sandblasting13–15 enhanced the repair bond strength; however, there are conflicting results regarding the most appropriate surface treatment.16,17
On the other hand, chemical surface treatments using universal multipurpose adhesives are becoming increasingly popular because they can be used in multiple modes for direct and indirect restorations, including bonding to composite resins, dental ceramics, and alloys.18,19 Some universal adhesives have silane agents in their compositions to simplify a multi-step procedure by avoiding the need for an extra silanization step. In a recent systematic review, Mendes et al reported that applying an additional silane agent could increase the repair bond strength of the resin composite. However, they concluded that further studies are needed to evaluate whether a silane-containing universal adhesive could obviate the need for a separate silanizing step for direct resin composite repair.20 Silane coupling agents promote chemical adhesion between the resin matrix and glass filler particles.21 Previous studies have reported conflicting results on the need for an additional silanizing step before using silane-containing universal adhesives.22–24
Bulk-fill resin composites are considered monoincremental resins that can be applied in layers up to a thickness of 4 mm with significantly low rates of polymerization shrinkage.25,26 The utilization of bulk-fill resin composites has expanded due to their ease of application and satisfactory clinical performance.27 However, despite ongoing advancement, they are still susceptible to fractures. Since there is no consensus in the literature regarding the best repair protocol for bulk-fill restorations,28 this study aimed to measure the repair shear bond strength (SBS) of an aged bulk-fill composite after different mechanical (diamond bur vs sandblasting) and chemical (universal adhesive, with or without previous silanization) surface treatments. The tested null hypotheses were: (1) there is no difference in repair SBS between bur and sandblasting surface treatments; and (2) there is no difference in repair SBS when using a silane-containing universal adhesive (Scotchbond Universal Adhesive) with or without a separate silanizing step.
Materials and Methods
The Filtek One Bulk Fill (3M ESPE, St Paul, MN, USA) composite resin was used to construct the substrate and repair material in this study. The adhesive system used was Universal silane-containing Adhesive (Scotchbond Universal Adhesive, 3M ESPE, Neuss, Germany), and a silane coupling agent (Prosil, FGM, Joinville, SC, Brazil) was used for the additional silanizing step. The tested materials and their compositions are presented in Table 1.
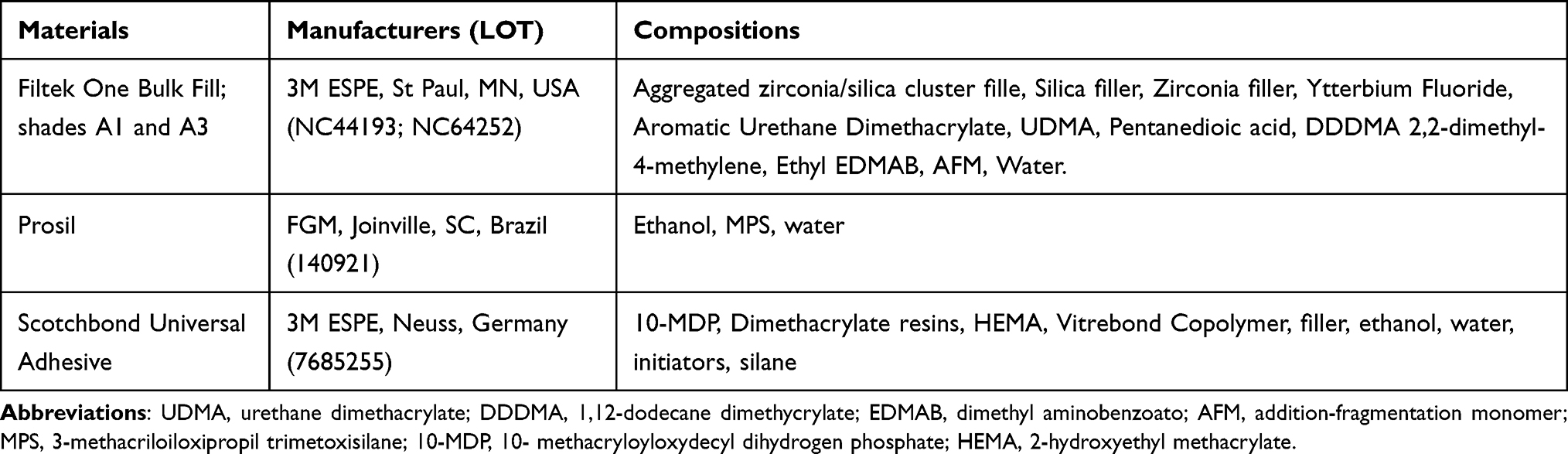 |
Table 1 The Tested Materials, Manufacturers and Their Compositions |
Preparation of Composite Samples
Seventy-two cylindrical specimens measuring 5 mm in diameter × 4 mm in height were constructed from bulk-fill composite (Filtek One Bulk Fill, Shade A1, 3M ESPE, St Paul, MN, USA) using a Teflon mold. This mold was positioned on a glass slide covered with a transparent mylar strip. The resin composite was inserted in a single increment and covered with a second mylar strip followed by a glass slide. Next, a 200 g load was applied on the top surface for one minute to obtain a flat surface and compact the material in a standardized manner.29 Each specimen was photoactivated with an LED unit (Radii Plus, SDI, Bayswater, Australia) for 20s according to the manufacturer’s instructions. The intensity of the light (1250 mW/cm2) was verified with an LED radiometer (SDI, Australia) before each curing. All specimens were incubated for 24 h in distilled water at 37 °C. All samples were aged using a thermocycling machine for 10,000 cycles at 5℃ to 55℃, with a dwell time of 20s.30
The 72 specimens were randomly allocated into two main groups (n = 36 each) based on the type of mechanical surface treatment: group Db was treated with a diamond bur, and group Sb was sandblasted with Al2O3 particles. The specimens in each group were further subdivided into three subgroups (n = 12 each) based on the chemical conditioning method used: subgroups Db-only and Sb-only were left unconditioned; subgroups Db-U and Sb-U were treated with Scotchbond Universal Adhesive (3M ESPE); and subgroups Db-S-U and Sb-S-U were treated with a silane coupling agent (Prosil, FGM) before using the universal adhesive.
Surface Treatment Protocols
In group Db, surface treatment was performed with a fine cylindrical diamond bur (46 μm grit, Komet Dental, Brasseler, Lemgo, Germany), using unidirectional movements for 5 s under water cooling. The electric handpiece (40,000 rpm) holding the diamond bur was attached to an apparatus that maintained a stable load (100 g) and a vertical position during preparation for standardized grinding.31 In group Sb, sandblasting of the composite surfaces was performed with Al2O3(50 μm) using an intraoral sandblaster (KaVo RONDOflex Plus 360, KaVo Dental, Germany) at a pressure of 2.8 bar and a distance of 5 mm for 10s.
After the mechanical treatments, subgroups Db-only and Sb-only did not receive any chemical conditioning. Subgroups Db-U and Sb-U were conditioned with Scotchbond Universal Adhesive (3M ESPE) according to the manufacturer’s instructions. It was applied on a composite surface, rubbed for 20s with a disposable brush, air dried for 5s, and light cured for 10s. Subgroups Db-S-U and Sb-S-U were conditioned with a silane coupling agent (Prosil, FGM) applied to the surface according to the manufacturer’s instructions using a disposable brush and allowed to react for 1 min before air drying for 10s. Then, the universal adhesive was applied as described for subgroups Db-U and Sb-U.
An adhesive tape with a central orifice 3 mm in diameter was placed on the exposed surfaces of the composite specimens to demarcate the bonding area on the repaired surfaces. All subgroups were repaired with a single increment of the same composite (Filtek One Bulk Fill, Shade A3, 3M ESPE) using a cylindrical Teflon mold 3 mm in diameter × 3 mm in height. The repair composite was selected in a different shade to allow visual identification of the interface during SBS testing and evaluation of failure modes.
Additional samples (n = 12) were prepared for the reference group (Ref. group) to measure the cohesive strength (composite-composite layers) of the non-aged bulk-fill composite, which represented optimal repair bond strength.32 Samples were prepared as described for the other groups but without aging or surface treatments. Two layers of Filtek One Bulk Fill (Shade A1) were built immediately. The first layer measuring 5 mm in diameter × 4 mm in height was prepared using a Teflon mold and light-cured for 20s. Then, the second layer, 3 mm in diameter × 3 mm in height, was added over the first one using a Teflon mold and light-cured for 20s.
Shear Bond Strength (SBS) Testing and Failure Modes Analysis
After storage in distilled water at 37 °C for 24 h, the specimens were loaded onto a universal testing machine (Tinius Olsen, Augsburg, Germany). The SBS test was performed using a notched-edge blade at a crosshead speed of 1 mm/min until failure, and the SBS value was measured in megapascals (MPa).
The failure mode of each sample was evaluated by two blinded examiners using a stereomicroscope (Meiji EMZ-TR, Meiji Techno, Saitama, Japan) at 40× magnification. It was recorded as adhesive (observed at the interface between the substrate composite and the repair composite), cohesive (occurred within the substrate or the repair composite), or mixed (involving both adhesive and cohesive failures).
Scanning Electron Microscopy (SEM) Evaluation
Six additional specimens (5 mm in diameter × 4 mm in height) were prepared and aged by 10,000 thermal cycles, then were divided into two groups (n = 3 each) based on the mechanical surface treatment (diamond bur abrasion or sandblasting) to evaluate surface topography. The specimens were gold sputtered and examined at 500 × and 1000 × magnifications using field emission SEM (Inspect F50, FEI, Hillsboro, Oregon, USA).
Statistical Analysis
The sample size was calculated using G * Power 3.1.9.7 software (University of Düsseldorf, Düsseldorf, Germany) with a study power of 85% and a two-sided alpha error of probability of 0.05. All statistical analyses were performed at a significance level of 0.05 using SPSS 26 (IBM-SPSS Inc., Chicago, USA). The Shapiro–Wilk test was used to ensure normality, while Levene’s test was used to determine the homogeneity of variance. A one-way ANOVA was performed, followed by Tukey’s multiple comparisons test was conducted to compare SBS among different chemical conditioning within each mechanical treatment. An independent t-test performed the comparison between mechanical surface treatments in each chemical conditioning. Dunnett two-sided tests were used to compare the reference group’s SBS values with each repaired group individually.
Results
Shear Bond Strength (SBS) Test and Failure Modes Analysis
The mean, standard deviation and significance level (P values) of the SBS for the study groups are listed in Table 2. Subgroups that underwent mechanical treatment only (Db-only and Sb-only) recorded the lowest SBS mean values (13.31 MPa and 20.35 MPa, respectively). Sb-only recorded significantly higher SBS than the Db-only subgroup (P < 0.001). In contrast, the SBS was not significantly different between subgroups Db-U and Sb-U (P = 0.248) and between subgroups Db-S-U and Sb-S-U (P = 0.078). Likewise, no significant difference was observed in SBS when the universal adhesive was used with or without an additional silanizing step in both mechanical treatments (P > 0.05). The reference group (cohesive strength) recorded the highest SBS mean value (48.37 MPa), which was significantly higher than all the other subgroups. The failure mode distributions are presented in Figure 1. For subgroups Db-only and Sb-only, all failures were adhesive (100%). Alternatively, the failure modes were predominantly mixed for Db-U: 75%, Db-S-U: 66.6%, Sb-U: 66.6%, and Sb-S-U: 50%. Furthermore, 83.3% of the failures in the reference group were cohesive within the substrate composite.
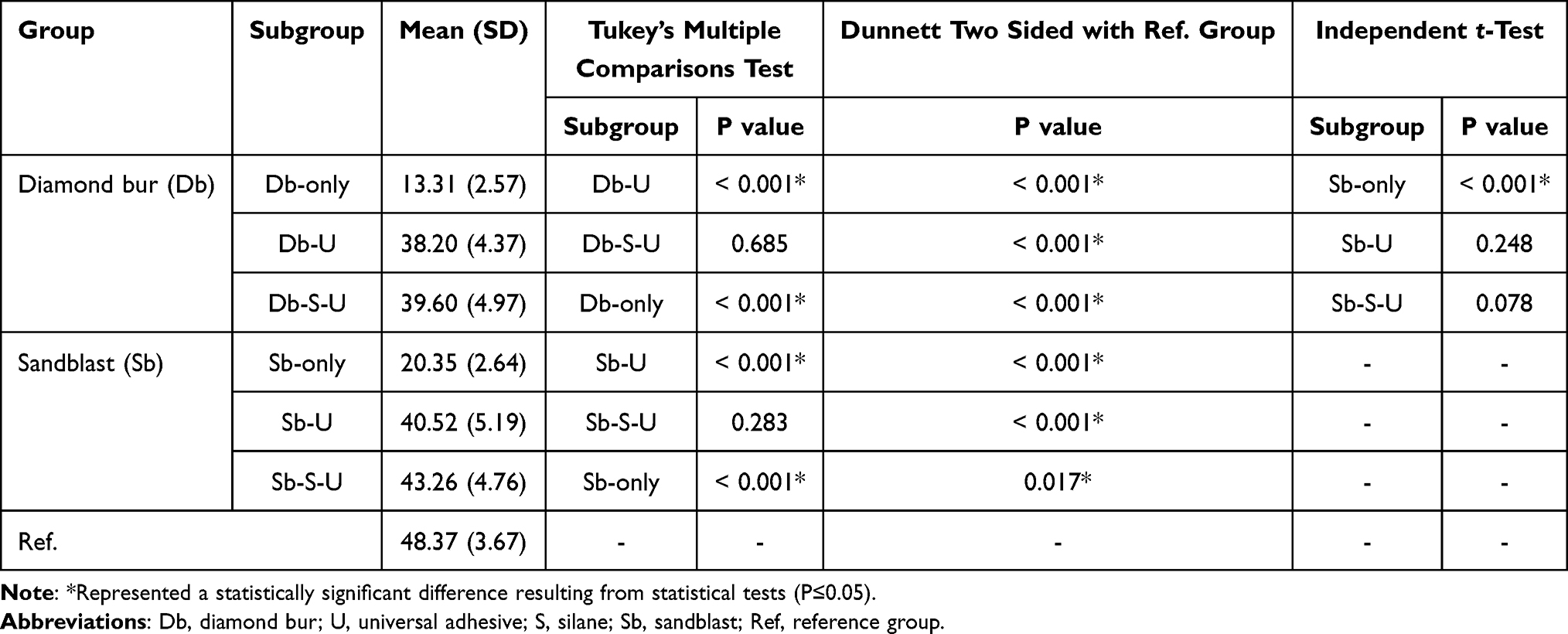 |
Table 2 Mean, Standard Deviation (SD) and Significance Level (p-values) of the Shear Bond Strength (in MPa) for the Study Groups |
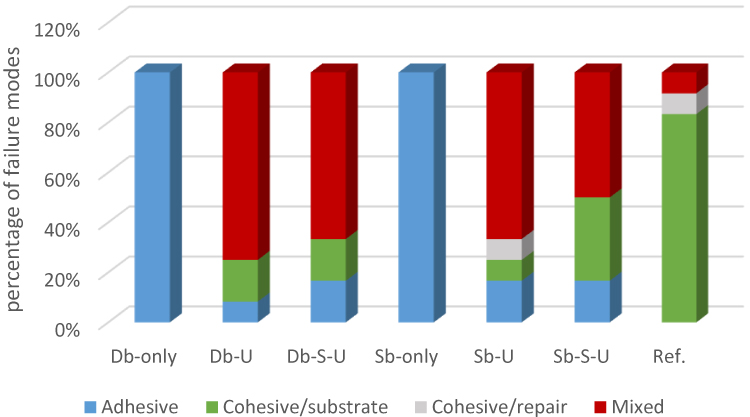 |
Figure 1 Bar chart showing the failure modes distribution (in percentage) of all groups. Abbreviations: Db, diamond bur; U, universal adhesive; S, silane; Sb, sandblast; Ref, reference group. |
Scanning Electron Microscopy (SEM) Analysis
SEM images of the aged composites after the different mechanical surface treatments revealed that the roughness pattern in the diamond burs abraded group was markedly different from that in the sandblasted group. Surfaces roughened with diamond burs showed evident parallel lines, groove patterns and longitudinal scratches caused by the grinding action. On the other hand, the sandblasted surfaces demonstrated porous, micropitted, and a more irregular topography (stone-like pattern), with a high number of microcavities (Figure 2).
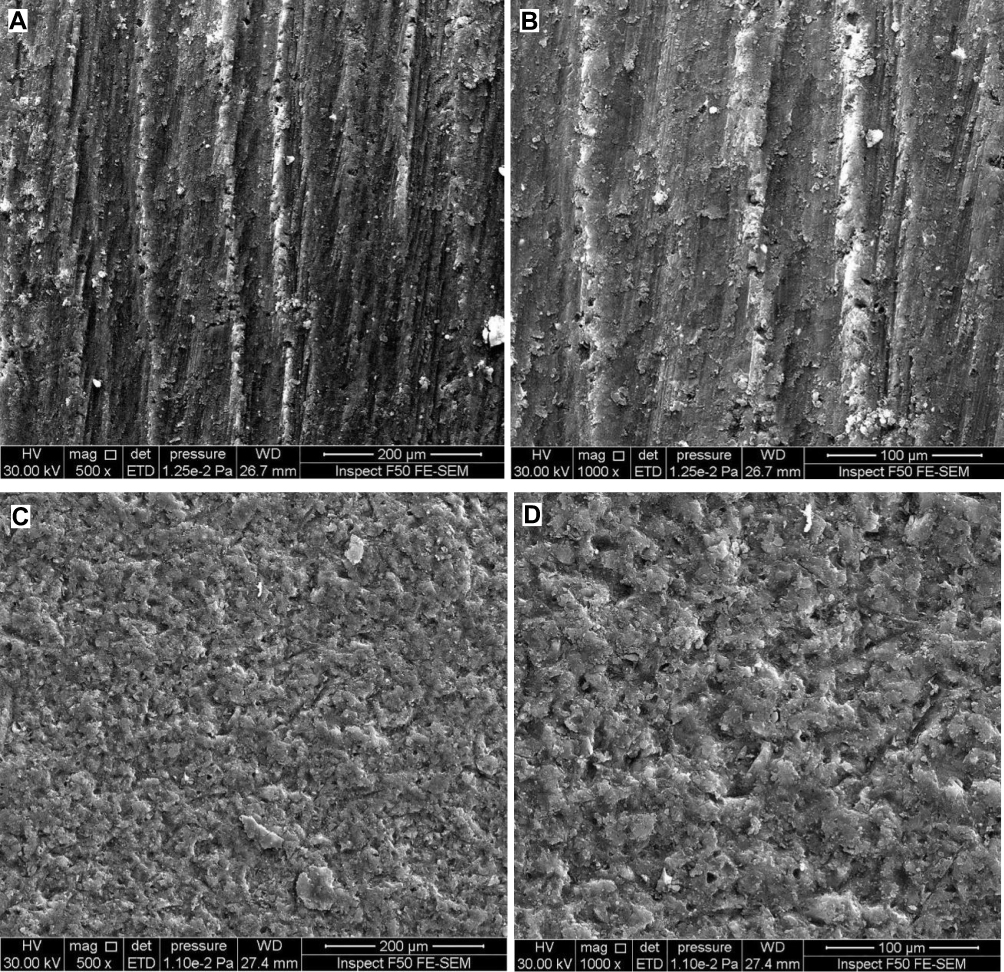 |
Figure 2 Scanning electron microscopy (SEM) images of aged bulk-fill composite after Diamond bur treatment (A and B) and Aluminum oxide sandblasting (C and D). |
Discussion
This study investigated the effects of different surface treatment strategies—two mechanical (air abrasion and bur roughening) and two chemical (universal adhesive with or without separate silanization) on composite–composite bond strength using SBS testing. This test was used because it is considered a quick and easy method that requires no further specimen processing.33,34 Furthermore, this test simulates the forces that typically occur during chewing and mimics the clinical oral setting more realistically than other tests in measuring resin–resin bonding.35
Bonding between old and new composites can occur via distinct mechanisms, including micromechanical interlocking to the substrate surface, chemical bonding with the organic matrix, and through exposed filler particles.8,32
In the present study, when the aged resin composites underwent mechanical treatment only, Al2O3 sandblasting (Sb-only) produced statistically higher SBS values than diamond bur treatment (Db-only). Thus, the first null hypothesis was rejected. A similar finding was reported by Michelotti et al, revealing that sandblasting resulted in higher repair bond strength than bur abrasion.36 This could be attributed to the fact that sandblasting creates a surface with more irregularities and an increased number of micro retentive cavities than diamond bur abrasion.37,38 This result was confirmed by the SEM observations obtained in this study (Figure 2), where sandblasted surfaces have micropits, and more irregular topography than surfaces roughened with a diamond bur, which could increase the surface area and enhance micromechanical interlocking.
Remarkably, the significant difference in SBS between the sandblasted and bur-abraded surfaces diminished when the chemical adhesive agent was applied. No significant difference in SBS was observed between Db-U and Sb-U or between Db-S-U and Sb-S-U subgroups. Thus, chemical conditioning might level out the differences between the mechanical treatments, as described in a previous study.17 However, it should be noted that Al2O3 sandblasting necessitates additional precautions to protect the patient and environment from aerosols during intraoral procedures.39
For the diamond bur-treated group (Db), the SBS of the repaired composite after mechanical treatment only (Db-only) was significantly lower than the combined mechanical and chemical treatment groups (Db-U and Db-S-U). The same results were obtained for the sandblasted group (Sb). These findings are consistent with previous studies,14,40 confirming the importance of combined mechanical and chemical conditioning for composite repairs.
Regarding the effectiveness of silane, it has been reported that silane coupling agents promote chemical adhesion between the resin matrix and glass filler particles. It also increases the substrate surface’s wettability, promoting better infiltration of bonding agents into the repaired restoration.11,21
According to the findings of this study, no significant difference in SBS was observed between specimens treated with the universal adhesive in the presence or absence of an additional silanizing step; thus, the second null hypothesis was not rejected. Similar findings have been reported in other studies.22,23 Scotchbond Universal Adhesive contains 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP), an adhesive functional monomer that can create insoluble calcium salts and chemically bond to zirconia, metals, and tooth tissues.41 The composite substrate material used in this study (Filtek One Bulk Fill) is incorporated with zirconia nanofiller particles, forming a chemical bond with the 10-MDP monomer, which may have increased the repair bond strength.42 Furthermore, as stated by the manufacturer, Scotchbond Universal Adhesive includes pre-hydrolyzed silane in its composition. Therefore, using a separate silane agent before applying the examined universal adhesive was not advantageous in enhancing the SBS in the current study.
In contrast, other researchers disagree with this result and recommend an additional silanization step before using a silane-containing universal adhesive to enhance the bond strength.24 These conflicting findings may be due to methodological differences, as they used tensile SBS testing. Moreover, they used an additional phosphoric acid etching step before the adhesive, which can enhance the surface cleanliness of the substrate composite.43
In this study, the aging of the substrate composite was performed by thermocycling, which simulates clinical conditions better than other in vitro aging methods, such as storage in water or chemical solvents.44 According to Gale et al, 10,000 cycles correspond to one year of clinical service of composite restorations.30 There is disagreement over the clinically acceptable value for repair bond strength; the closer the bond strength to the cohesive strength value of the substrate material, the more effective the repair. A reference group was included in this study, as the cohesive strength of non-aged composite represents the optimal repair bond strength.32,45 The highest mean SBS value was observed in the non-aged specimens of the reference group, and this value was significantly higher than all the other subgroups. This result could be attributed to the bond strength formed by the oxygen-inhibited layer at the bonded interface of the non-aged composite-composite adhered layers,46 whereas aged specimens gradually lose their strength.7 Kiomarsi et al, reported that thermocycling with 10,000 cycles significantly decreased the repair bond strength of the resin composite,12 as it produced a combination of hydrolytic and thermal degradation due to repeated thermal changes between 5 °C and 55 °C in water baths.44,47 Finally, none of the mechanical or chemical treatments used in this study could regain the original cohesive strength of the fresh composite resin.
The stereomicroscopic examination of failure patterns revealed that subgroups Db-only and Sb-only showed 100% adhesive failure, corresponding to the lowest mean bond strength values, as no chemical interaction occurred between the new and aged composites. Conversely, subgroups Db-U, Sb-U, Db-S-U, and Sb-S-U exhibited a predominance of mixed failure as the bond strength increased. In the reference group, cohesive failure was predominant. Similar research in the literature reported high bond strengths correlated with cohesive failure, whereas low bond strengths were associated with increased adhesive failure modes.48,49
One of the limitations of this study is that only one composite substrate and one universal adhesive containing silane were examined. Thus, the results of this study may not apply to other materials with distinct compositions. Moreover, this study was conducted in vitro; Consequently, additional in vivo and in vitro studies are required to investigate the SBS of repaired composite.
Conclusion
The sandblasted specimens presented with higher repair SBS values than those that underwent diamond bur abrasion. However, no difference in the SBS was observed in both these treatment groups after the application of the Scotchbond Universal Adhesive. Furthermore, performing an additional silanizing step before applying the examined universal adhesive did not enhance the SBS of the repaired Filtek One Bulk Fill composite.
Acknowledgments
The research project was conducted in the Mustansiriyah University (www.uomustasiryah.edu.iq), Baghdad-Iraq, who provided insight and expertise that greatly assisted the research.
Disclosure
The authors do not have any financial interest with companies whose materials are included and report no conflicts of interest in this work.
References
1. Eltahlah D, Lynch CD, Chadwick BL, Blum IR, Wilson NH. An update on the reasons for placement and replacement of direct restorations. J Dent. 2018;72:1–7. doi:10.1016/j.jdent.2018.03.001
2. Beck F, Lettner S, Graf A, et al. Survival of direct resin restorations in posterior teeth within a 19-year period (1996–2015): a meta-analysis of prospective studies. Dent Mater. 2015;31(8):958–985. doi:10.1016/j.dental.2015.05.004
3. Kirsch J, Tchorz J, Hellwig E, Tauböck TT, Attin T, Hannig C. Decision criteria for replacement of fillings: a retrospective study. Clin Exp Dent Res. 2016;2(2):121–128. doi:10.1002/cre2.30
4. Casagrande L, Laske M, Bronkhorst EM, Huysmans MCD, Opdam NJ. Repair may increase survival of direct posterior restorations–A practice based study. J Dent. 2017;64:30–36. doi:10.1016/j.jdent.2017.06.002
5. Özcan M, Koc-Dundar B. Composite–composite adhesion in dentistry: a systematic review and meta-analysis. J Adhes Sci Technol. 2014;28(21):2209–2229. doi:10.1080/01694243.2014.954659
6. Curtis A, Shortall A, Marquis P, Palin W. Water uptake and strength characteristics of a nanofilled resin-based composite. J Dent. 2008;36(3):186–193. doi:10.1016/j.jdent.2007.11.015
7. Eliasson ST, Tibballs J, Dahl JE. Effect of different surface treatments and adhesives on repair bond strength of resin composites after one and 12 months of storage using an improved microtensile test method. Oper Dent. 2014;39(5):E206–E216. doi:10.2341/12-429-L
8. Loomans BA, Özcan M. Intraoral repair of direct and indirect restorations: procedures and guidelines. Oper Dent. 2016;41(S7):S68–S78. doi:10.2341/15-269-LIT
9. Kanzow P, Wiegand A, Schwendicke F, Göstemeyer G. Same, same, but different? A systematic review of protocols for restoration repair. J Dent. 2019;86:1–16. doi:10.1016/j.jdent.2019.05.021
10. Valente LL, Silva MF, Fonseca AS, Muenchow EA, Isolan CP, Moraes RR. Effect of diamond bur grit size on composite repair. J Adhes Dent. 2015;17(3):257–263. doi:10.3290/j.jad.a34398
11. Wendler M, Belli R, Panzer R, Skibbe D, Petschelt A, Lohbauer U. Repair bond strength of aged resin composite after different surface and bonding treatments. Materials. 2016;9(7):547. doi:10.3390/ma9070547
12. Kiomarsi N, Saburian P, Chiniforush N, Karazifard M-J, Hashemikamangar -S-S. Effect of thermocycling and surface treatment on repair bond strength of composite. J Clin Exp Dent. 2017;9(8):e945. doi:10.4317/jced.53721
13. da Costa TRF, Serrano AM, Atman APF, Loguercio AD, Reis A. Durability of composite repair using different surface treatments. J Dent. 2012;40(6):513–521. doi:10.1016/j.jdent.2012.03.001
14. Kaneko M, Caldas RA, Feitosa VP, Consani RLX, Schneider LFJ, Bacchi A. Influence of surface treatments to repair recent fillings of silorane-and methacrylate-based composites. J Conserv Dent. 2015;18(3):242. doi:10.4103/0972-0707.157265
15. Martos R, Hegedüs V, Szalóki M, Blum IR, Lynch CD, Hegedüs C. A randomised controlled study on the effects of different surface treatments and adhesive self-etch functional monomers on the immediate repair bond strength and integrity of the repaired resin composite interface. J Dent. 2019;85:57–63. doi:10.1016/j.jdent.2019.04.012
16. Aquino C, Mathias C, Barreto S, Cavalcanti A, Marchi G, Mathias P. Repair bond strength and leakage of non-aged and aged bulk-fill composite. Oral Health Prev Dent. 2020;18:783–791. doi:10.3290/j.ohpd.a45082
17. Dieckmann P, Baur A, Dalvai V, Wiedemeier DB, Attin T, Tauböck TT. Effect of composite age on the repair bond strength after different mechanical surface pretreatments. J Adhes Dent. 2020;22:365–372. doi:10.3290/j.jad.a44867
18. Wagner A, Wendler M, Petschelt A, Belli R, Lohbauer U. Bonding performance of universal adhesives in different etching modes. J Dent. 2014;42(7):800–807. doi:10.1016/j.jdent.2014.04.012
19. Da Rosa WL, Piva E, da Silva AF. Bond strength of universal adhesives: a systematic review and meta-analysis. J Dent. 2015;43(7):765–776. doi:10.1016/j.jdent.2015.04.003
20. Mendes LT, Loomans BA, Opdam NJ, Silva C, Casagrande L, Lenzi TL. Silane coupling agents are beneficial for resin composite repair: a systematic review and meta-analysis of in vitro studies. J Adhes Dent. 2020;22:443–453. doi:10.3290/j.jad.a45175
21. Matinlinna JP, Lung CYK, Tsoi JKH. Silane adhesion mechanism in dental applications and surface treatments: a review. Dent Mater. 2018;34(1):13–28. doi:10.1016/j.dental.2017.09.002
22. Fornazari IA, Wille I, Meda E, Brum R, Souza E. Effect of surface treatment, silane, and universal adhesive on microshear bond strength of nanofilled composite repairs. Oper Dent. 2017;42(4):367–374. doi:10.2341/16-259-L
23. Çakir NN, Demirbuga S, Balkaya H, Karadaş M. Bonding performance of universal adhesives on composite repairs, with or without silane application. J Conserv Dent. 2018;21(3):263–268. doi:10.4103/JCD.JCD_11_18
24. Silva CLD, Scherer MM, Mendes LT, Casagrande L, Leitune VCB, Lenzi TL. Does use of silane-containing universal adhesive eliminate the need for silane application in direct composite repair? Braz Oral Res. 2020;34. doi:10.1590/1807-3107bor-2020.vol34.0045
25. Van Ende A, De Munck J, Lise DP, Van Meerbeek B. Bulk-fill composites: a review of the current literature. J Adhes Dent. 2017;19(2):95–109. doi:10.3290/j.jad.a38141
26. Li X, Pongprueksa P, Van Meerbeek B, De Munck J. Curing profile of bulk-fill resin-based composites. J Dent. 2015;43(6):664–672. doi:10.1016/j.jdent.2015.01.002
27. de Almeida Durão M, de Andrade AKM, da Silva MDCM, Montes MAJR, de Melo Monteiro GQ. Clinical performance of Bulk-Fill resin composite restorations using the United States public health service and federation dentaire internationale criteria: a 12-month randomized clinical trial. Eur J Dent. 2021;15(02):179–192. doi:10.1055/s-0040-1718639
28. Cuevas-Suárez CE, Nakanishi L, Isolan CP, Ribeiro JS, Moreira AG, Piva E. Repair bond strength of bulk-fill resin composite: effect of different adhesive protocols. Dent Mater J. 2020;39(2)2018–2291.
29. ElEmbaby AES. The effects of mouth rinses on the color stability of resin‐based restorative materials. J Esthet Restor Dent. 2014;26(4):264–271. doi:10.1111/jerd.12061
30. Gale M, Darvell B. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. 1999;27(2):89–99. doi:10.1016/S0300-5712(98)00037-2
31. Deari S, Wegehaupt FJ, Tauböck TT, Attin T. Influence of different pretreatments on the microtensile bond strength to eroded dentin. J Adhes Dent. 2017;19:147–155. doi:10.3290/j.jad.a38142
32. Valente LL, Sarkis-Onofre R, Goncalves AP, Fernandez E, Loomans B, Moraes RR. Repair bond strength of dental composites: systematic review and meta-analysis. Int J Adhes Adhes. 2016;69:15–26. doi:10.1016/j.ijadhadh.2016.03.020
33. McDonough WG, Antonucci JM, He J, et al. A microshear test to measure bond strengths of dentin–polymer interfaces. Biomaterials. 2002;23(17):3603–3608. doi:10.1016/S0142-9612(02)00089-3
34. Flury S, Peutzfeldt A, Lussi A. Influence of increment thickness on microhardness and dentin bond strength of bulk fill resin composites. Dent Mater. 2014;30(10):1104–1112. doi:10.1016/j.dental.2014.07.001
35. Cho S, Rajitrangson P, Matis B, Platt J. Effect of Er, Cr: YSGG laser, air abrasion, and silane application on repaired shear bond strength of composites. Oper Dent. 2013;38(3):E58–E66. doi:10.2341/11-054-L
36. Michelotti G, Niedzwiecki M, Bidjan D, et al. Silane effect of universal adhesive on the composite–composite repair bond strength after different surface pretreatments. Polymers. 2020;12(4):950. doi:10.3390/polym12040950
37. Costa TR, Ferreira SQ, Klein-Júnior CA, Loguercio AD, Reis A. Durability of surface treatments and intermediate agents used for repair of a polished composite. Oper Dent. 2010;35(2):231–237. doi:10.2341/09-216-L
38. Puleio F, Rizzo G, Nicita F, et al. Chemical and mechanical roughening treatments of a supra-nano composite resin surface: SEM and topographic analysis. Appl Sci. 2020;10(13):4457. doi:10.3390/app10134457
39. Roeters JJ. A simple method to protect patient and environment when using sandblasting for intraoral repair. J Adhes Dent. 2000;2(3):235–238.
40. Altinci P, Mutluay M, Tezvergil-Mutluay A. Repair bond strength of nanohybrid composite resins with a universal adhesive. Acta Biomater Odontol Scand. 2018;4(1):10–19. doi:10.1080/23337931.2017.1412262
41. Chen C, Niu L-N, Xie H, et al. Bonding of universal adhesives to dentine–Old wine in new bottles? J Dent. 2015;43(5):525–536. doi:10.1016/j.jdent.2015.03.004
42. Nagaoka N, Yoshihara K, Feitosa VP, et al. Chemical interaction mechanism of 10-MDP with zirconia. Sci Rep. 2017;7(1):1–7. doi:10.1038/srep45563
43. Loomans BA, Cardoso MV, Roeters F, et al. Is there one optimal repair technique for all composites? Dent Mater. 2011;27(7):701–709. doi:10.1016/j.dental.2011.03.013
44. Szczesio-Wlodarczyk A, Sokolowski J, Kleczewska J, Bociong K. Ageing of dental composites based on methacrylate resins—A critical review of the causes and method of assessment. Polymers. 2020;12(4):882. doi:10.3390/polym12040882
45. Bin-Shuwaish MS. Shear bond strength of Bulk-Fill composites to resin-modified glass ionomer evaluated by different adhesion protocols. Clin Cosmet Invest Dent. 2020;12:367. doi:10.2147/CCIDE.S273842
46. Suh BI. Oxygen‐inhibited layer in adhesion dentistry. J Esthet Restor Dent. 2004;16(5):316–323. doi:10.1111/j.1708-8240.2004.tb00060.x
47. Rinastiti M, Özcan M, Siswomihardjo W, Busscher HJ. Effects of surface conditioning on repair bond strengths of non-aged and aged microhybrid, nanohybrid, and nanofilled composite resins. Clin Oral Investig. 2011;15(5):625–633. doi:10.1007/s00784-010-0426-6
48. Baur V, Ilie N. Repair of dental resin-based composites. Clin Oral Investig. 2013;17(2):601–608. doi:10.1007/s00784-012-0722-4
49. Ayar MK, Guven ME, Burduroglu HD, Erdemir F. Repair of aged bulk‐fill composite with posterior composite: effect of different surface treatments. J Esthet Restor Dent. 2019;31(3):246–252. doi:10.1111/jerd.12391
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.