")
Back to Journals » Patient Preference and Adherence » Volume 17
Significance of Self-Injectable Biologics in Japanese Patients with Severe Allergic Diseases: Focusing on Pen-Type Devices and Copayment
Authors Hanada S , Muraki M, Kawabata Y, Yoshikawa K, Yamagata T, Nagasaki T , Ohara Y, Oiso N, Matsumoto H, Tohda Y
Received 11 July 2023
Accepted for publication 24 October 2023
Published 7 November 2023 Volume 2023:17 Pages 2847—2853
DOI https://doi.org/10.2147/PPA.S430038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Soichiro Hanada,1,* Masato Muraki,1,* Yoshiyuki Kawabata,1 Kazuya Yoshikawa,1 Toshiyuki Yamagata,1 Tadao Nagasaki,1 Yushiro Ohara,2 Naoki Oiso,2 Hisako Matsumoto,3 Yuji Tohda4
1Department of Respiratory Medicine and Allergology, Kindai University Nara Hospital, Ikoma, Nara, Japan; 2Department of Dermatology, Kindai University Nara Hospital, Ikoma, Nara, Japan; 3Department of Respiratory Medicine and Allergology, Kindai University Hospital, Osakasayama, Osaka, Japan; 4Kindai University Hospital, Osakasayama, Osaka, Japan
*These authors contributed equally to this work
Correspondence: Masato Muraki, Department of Respiratory Medicine and Allergology, Kindai University Nara Hospital, 1248-1 Otoda-cho, Ikoma, Nara, 630-0293, Japan, Tel +81 743 77 0880, Fax +81 743 77 0890, Email [email protected]
Patients and Methods: A questionnaire survey was administered to 18, 14, and 3 patients introduced to home self-injection of dupilumab or mepolizumab using a pen-type device for atopic dermatitis, asthma alone, and asthma plus chronic rhinosinusitis with nasal polyps, respectively.
Results: All but one participant wished to continue self-injection. Most participants affirmed the reduction in copayment (88.6%) and saving time and labor for hospital visits (88.6%). Six patients who received dupilumab complained of side effects, but all, except for one, continued the treatment. Of the 13 patients who had previously used a syringe-type device, 10 preferred the pen type because of its ease of use, while 3 (23%) preferred the syringe type because of the self-adjustable injection speed for pain control.
Conclusion: Administration of biologics using pen-type devices is easier, and the introduction of home self-injection leads to a reduction in outpatient visits and copayment.
Keywords: dupilumab, mepolizumab, self-injection, asthma, atopic dermatitis, chronic sinusitis with nasal polyps
Introduction
The major barriers to continued treatment with biologics are usability, efficacy, adverse events, cost of care, and the need for hospital visits. Of these, drug efficacy and adverse events require medical monitoring. However, other important factors that are likely to affect patient compliance include the ease of use and amount of copayment. Five biologics have been approved for the treatment of severe asthma in Japan: omalizumab, an anti-IgE antibody; mepolizumab, an anti-interleukin (IL)-5 antibody; benralizumab, an anti-IL-5 receptor α antibody; dupilumab, an anti-IL-4 receptor α antibody that is also indicated for the treatment of atopic dermatitis and chronic rhinosinusitis with nasal polyps (CRSwNP); and tezepelumab, an anti-thymic stromal lymphopoietin antibody. Of these, three drugs are approved for home self-injection: omalizumab, mepolizumab, and dupilumab; mepolizumab and dupilumab are available for use with syringe- and pen-type devices.
However, the recommendation of additional biological therapy for severe allergic diseases such as severe asthma, is not accepted by all patients. One of the reasons for this is the high copayment.1 In Japan, universal health insurance is available to all citizens; nonetheless, the high cost of biologics is a significant burden for low-income patients.
Under the Japanese insurance system, long-term prescriptions of up to 90 days are allowed, and a monthly maximum copayment amount is set depending on the income. The introduction of self-injection at home and 90-day prescriptions will reduce the patient’s copayment. However, patients’ total copayment will remain unchanged if they cannot self-inject the drug. One of the most important factors for patient adherence is the amount of copayment.2,3
At our hospital, the dupilumab and mepolizumab syringes were switched to pen-type devices in April and July 2021, respectively. Therefore, we conducted a questionnaire survey of patients using pen-type devices for dupilumab or mepolizumab self-injection to determine the significance of home self-injection and usefulness of the pen-type device.
Materials and Methods
This study included 35 patients (16 men and 19 women; mean age, 54.9±16.7 years) with asthma, atopic dermatitis, or CRSwNP attending the Department of Respiratory Medicine and Allergology or the Department of Dermatology at Kindai University Nara Hospital (Ikoma, Japan) who were introduced to home self-injection of either dupilumab or mepolizumab using a pen-type device and had been receiving 12-week prescriptions (Table 1). Dupilumab (Dupixent®) 300 mg every two weeks and mepolizumab (Nucala®) 100 mg every four weeks were administered subcutaneously (sc) in 25 and 10 patients, respectively. The indications were atopic dermatitis, asthma, and asthma plus CRSwNP in 18, 14, and 3 patients, respectively.
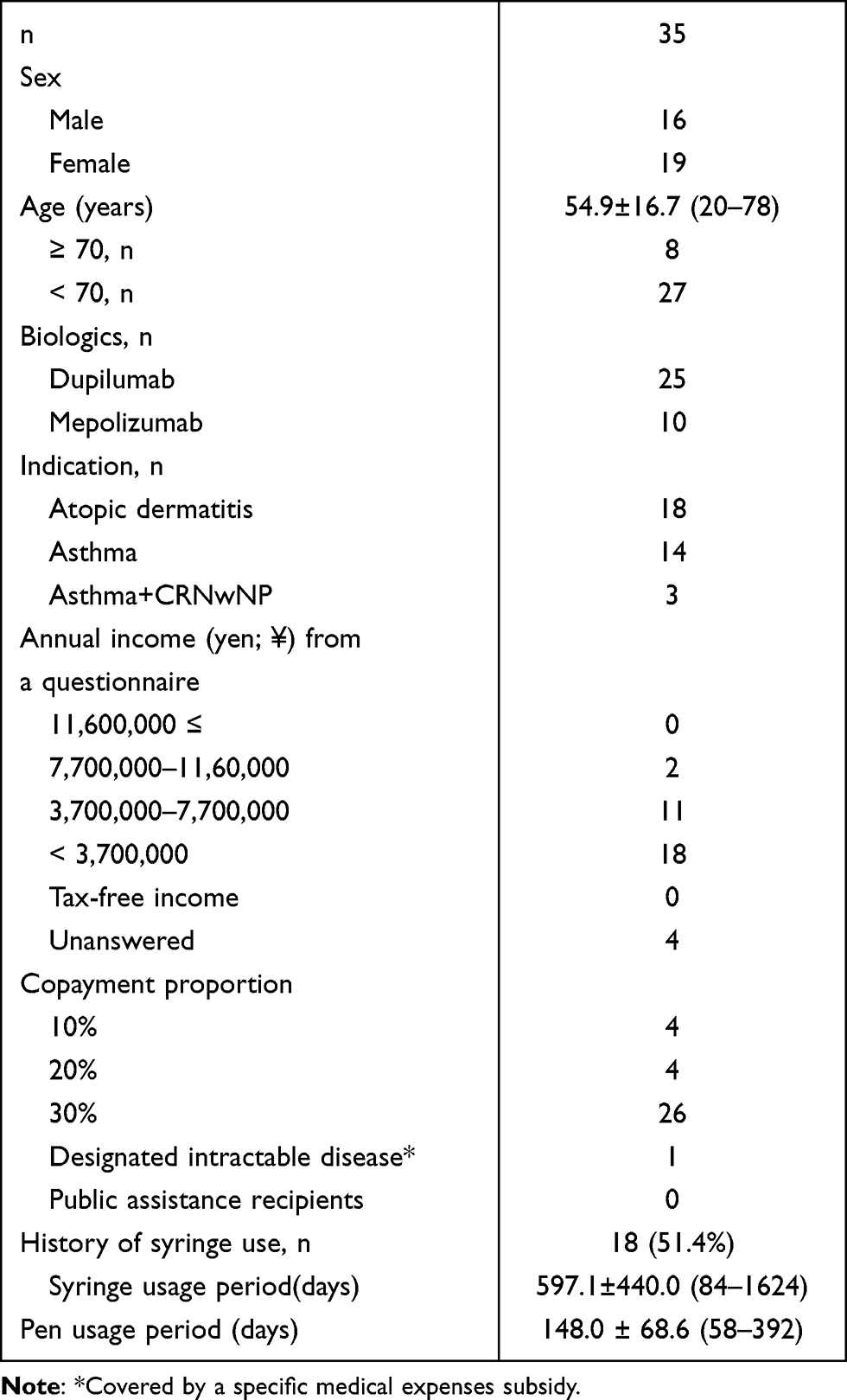 |
Table 1 Patient Characteristics |
Participants introduced to home self-injection using pen-type devices were surveyed about its significance, effectiveness, and safety 148.0 ± 68.6 days after introduction. The preference for the syringe- or pen-type device after switching was examined in 18 participants (51.4%) with a history of syringe use.
Informed consent was obtained from all participants. This study was approved by the Ethics Committee of Kindai University Nara Hospital (approval number 621 on March 11, 2021, for dupilumab and approval number 645 on September 27, 2021, for mepolizumab) and was complied with the tenets of the Declaration of Helsinki. (UMIN ID: 000049878)
Results
The survey results are summarized in Table 2. Most respondents had annual incomes < JPY 7.7 million and were low- to middle-income earners. One participant’s insurance was for a designated intractable disease covered by a specific medical expense subsidy with an upper limit of JPY 20, 000 per month. Of the patients, 77.1% were aged <70 years, and their insurance required a copayment of 30% of the medical expenses. Ninety-seven percent of the participants wished to continue home self-injections. Biologics and other control medications were prescribed for 12 weeks to all participants, contributing to a reduction in the financial burden (88.6%) and hospital visits (88.6%).
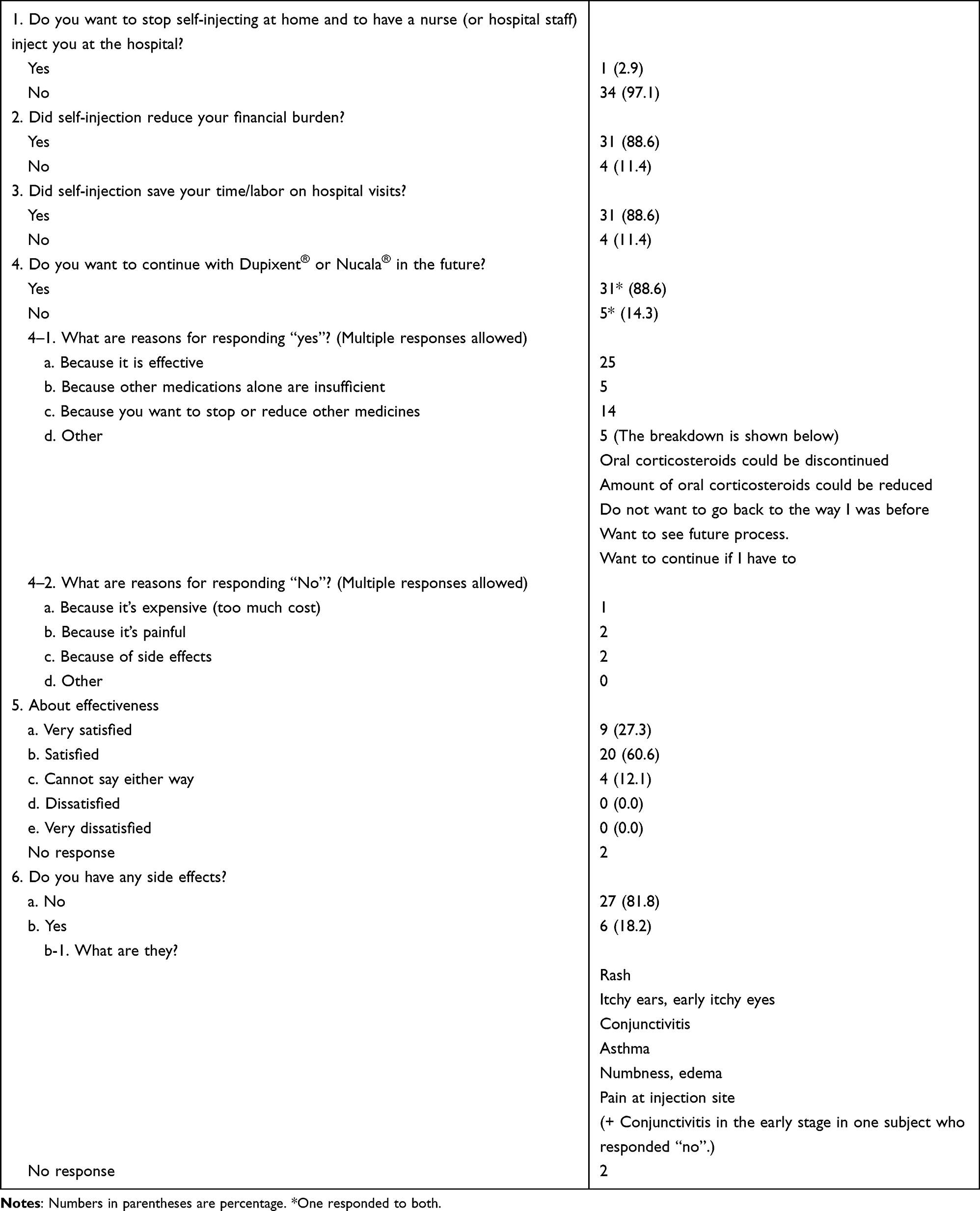 |
Table 2 Questionnaire Survey on Self-Injection and Drug Efficacy and Safety |
Regarding continuation of the biologic, 31 and 5 patients responded “Yes”, and “No”, respectively (one participant selected both “Yes” and “No”). The reason for choosing to continue treatment was the effectiveness of the biologics. In contrast, the reasons for denying continuation were high cost, pain, or side effects; nonetheless, all five deniers continued with biologics. Regarding effectiveness, 87.9% were more than satisfied, and although adverse events were observed in six patients receiving dupilumab, no problems with continuation of biologics were reported at the time of the questionnaire survey (one patient with asthma developed eosinophilic granulomatosis with polyangiitis after 5.5 months of dupilumab treatment and discontinued it). All patients who reported adverse reactions had atopic dermatitis, except for one who developed eosinophilic granulomatosis with polyangiitis.
Failure of dupilumab auto-injection was reported by one participant. The patient was startled by the surrounding noise and pulled the needle out immediately after inserting sc. Because the pen-type is an automatic injection device, once the needle is pulled out, the remaining drug solution is released and cannot be reinjected.
Regarding comparison of device types after switching, out of 18 participants with a history of syringe use, 10 preferred the pen type, and three preferred the syringe (Table 3). Of the five participants who did not respond to this item, three reported failure of self-injection with the syringe. Most participants preferred the pen-type device owing to the ease of use, while all three respondents who preferred the syringe were dupilumab users who indicated that they could self-adjust the injection speed to control the pain caused by the injection.
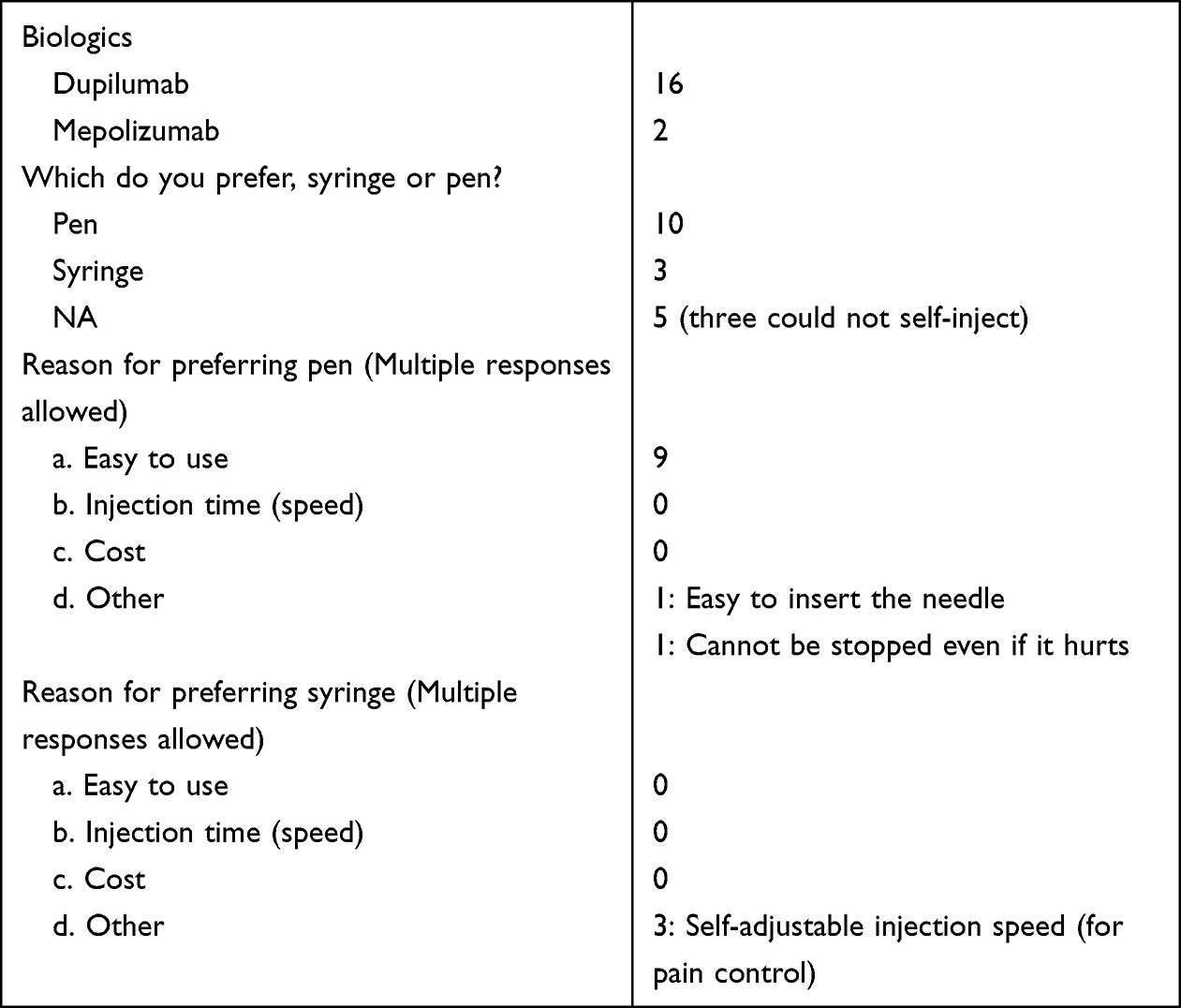 |
Table 3 Questionnaire Survey for Participants with a History of Syringe Use |
Discussion
Patients with severe uncontrolled asthma or atopic dermatitis have greater medical and economic burdens, suggesting that more appropriate treatment according to the treatment guidelines is required.4,5 Moreover, patients with uncontrolled asthma have higher all-cause and asthma-related costs than patients with suboptimally controlled or controlled asthma.6 Furthermore, the continuation of expensive biologics should be rooted in the overall health economics and cost-effectiveness.7–9 Although the definition of remission is controversial,10,11 the introduction of biologics has led to the discontinuation of systemic corticosteroids and prevention of severe exacerbations of asthma12 and atopic dermatitis.13 Regarding the development and approval of medications, unmet medical needs, such as treatment satisfaction and the contribution of biologics to the management of various diseases, including asthma and atopic dermatitis, rank high.14
It has been suggested that biologics should be introduced earlier because of their favorable prognosis (early introduction improves long-term prognosis)15 and the risks associated with oral corticosteroids,16 including infection.17,18 Although biologics are recommended for patients with severe asthma and atopic dermatitis, in whom systemic corticosteroids should be avoided, all patients do not accept them. Although education by the paramedical staff is important for the acceptance of biologics,1 cost burdens can be a problem for the introduction and continuation of biologics.19 In our institution, in the majority of cases, introduction failure was attributed to high copayment.
Currently, the following biological products are covered by insurance for home self-injection in Japan: syringe- and pen-type devices for dupilumab from May 1, 2019, and September 18, 2020, respectively; syringe- and pen-type devices for mepolizumab from April 21, 2021; and syringe-type devices for omalizumab from August 12, 2021. Most participants in this study belonged to the middle to low annual income group (≤JPY 7.7 million); however, they self-reported owing to the protection of personal information. Although socioeconomic status is associated with asthma severity,20,21 no high taxpayers, tax-free income recipients, or public assistance recipients were included in this survey. In other words, the survey participants had an average income. High medical costs place a heavy copayment burden on patients. Under the Japanese insurance system, individuals aged <70 years are required to pay 30% of their medical costs, while those aged ≥ 70 years are required to pay either 10% or 20%. Although the monthly copayment limit is set according to the annual income and age (< 70 years and ≥70 years), the total medical costs for biologics, other medication for asthma or atopic dermatitis and comorbidities, doctor’s fees, management fees, and laboratory fees, will often reach or approach the copayment limit.
The individual burden of monthly injection at a medical office, instead of home self-injection, may affect the possibility of making a living. The maximum prescription period in Japan is 90 days. With the introduction of home self-injection, long-term prescription of medications, including biologics, for up to 90 days, which is the maximum allowed time, will eliminate the need for hospital visits in the remaining two months in stable patients. In addition, it leads to a reduction in copayment. Although the total cost of medications remains the same, the amount of copayment can reduce to almost one-third. However, the actual amount of each copayment varies according to the insurance system. This will lead to a reduction in the copayment amount by approximately half to one-third. The results of this study suggest that the long-term prescription may lead to better acceptance of biological therapy in a larger number of eligible patients.
Regarding the continuation of biological treatment, the onset and persistence of its effects as well as its safety are important. The effectiveness of biologics was confirmed in several participants in this study. In addition, adverse events did not result in discontinuation, except in one case. Among the participants in this study, three patients using syringe-type devices were unable to inject themselves and switched to a pen-type device, which allowed them to inject themselves. This was thought to be due to the ease of using pen-type devices.22 No participant reported inability to self-inject after switching to a pen-type device.
As a limitation, we were unable to determine the number of patients for whom treatment with the two medications was recommended, and only those patients who initiated treatment were included. Therefore, the treatment induction rate could not be calculated, and the reasons for failure of induction remain unknown.
Based on this study, the advantages of home self-injection are as follows: 1) reduced copayment, 2) reduced time and labor for hospital visits, and 3) administration is easier with a pen-type device to than with a syringe-type device, although both formulations achieve the same therapeutic effect. The disadvantages of home self-injection are: 1) it cannot be used in patients incapable of self-injection; 2) adherence issues (forgetting to inject); and 3) the possibility of failure due to pen-type autoinjection.
Conclusion
Long-term prescriptions associated with the introduction of self-injection may be useful for patients’ acceptance of biologics, as they eliminate the need for hospital visits and lead to lower copayments. This prevents exacerbations and improves the quality of life of patients with asthma23,24 and atopic dermatitis,25 which may improve prognosis and ultimately lead to a reduction in overall healthcare costs.26–28 Pen-type devices are easier than syringe-type devices for self-injection and may be more useful for introducing self-injection.
Acknowledgments
We would like to thank Editage (www.editage.com) for the English language editing.
Funding
No funding was obtained for this study.
Disclosure
Prof. Dr. Masato Muraki reports personal fees from GlaxoSmithKline K.K., AstraZeneca K.K., Sanofi K.K., Novartis Pharma K.K., Nippon Boehringer Ingelheim Co., Ltd., and Kyorin Pharmaceutical Co., Ltd., outside the submitted work. Prof. Dr. Hisako Matsumoto reports personal fees from AstraZeneca, Sanofi, GSK, and Novartis, outside the submitted work. Prof. Dr. Yuji Tohda reports consultant work for AstraZeneca, Kyorin, Sanofi, TeijinPhama, and Novartis, outside the submitted work. The authors report no other conflicts of interest related to this work.
References
1. Tamada T, Fukui K, Makita N, et al. An Internet Survey on recommendation process of biologics in severe asthma patients. Therap Res. 2021;42(12):857–866.
2. Gelhorn HL, Balantac Z, Ambrose CS, Chung YN, Stone B. Patient and physician preferences for attributes of biologic medications for severe asthma. Patient Prefer Adherence. 2019;13:1253–1268. doi:10.2147/PPA.S198953
3. Kashitani Y, Yamanaka Y, Hanada K, Tashiro N, Tsuji T. Patient preferences for selection of biologics in Japanese patients with severe asthma. J New Rem Clin. 2022;71(10):1042–1059.
4. Nagase H, Adachi M, Matsunaga K, et al. Prevalence, disease burden, and treatment reality of patients with severe uncontrolled asthma in Japan. Allergol Int. 2020;69(1):53–60. doi:10.1016/j.alit.2019.06.003
5. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018;32(6):850–878. doi:10.1111/jdv.14888
6. Reibman J, Tan L, Ambrose C, et al. Clinical and economic burden of severe asthma among US patients treated with biologic therapies. Ann Allergy Asthma Immunol. 2021;127(6):318–325. doi:10.1016/j.anai.2021.03.015
7. Wu AC, Fuhlbrigge AL, Robayo MA, Shaker M. Cost-effectiveness of biologics for allergic diseases. J Allergy Clin Immunol Pract. 2021;9(3):1107–1117. doi:10.1016/j.jaip.2020.10.009
8. McCoy T, Natarelli N, Pan A, Shakhbazova A, Sivamani RK, Chambers CJ. Systematic review and estimated cost-efficacy of biologics compared with narrowband ultraviolet B light for the treatment of moderate to severe psoriasis and atopic dermatitis. Int J Dermatol. 2023;62(8):986–999. doi:10.1111/ijd.16677
9. Tohda Y, Matsumoto H, Miyata M, et al. Cost-effectiveness analysis of dupilumab among patients with oral corticosteroid-dependent uncontrolled severe asthma in Japan. J Asthma. 2022;59(11):2162–2173. doi:10.1080/02770903.2021.1996596
10. Menzies-Gow A, Bafadhel M, Busse WW, et al. An expert consensus framework for asthma remission as a treatment goal. J Allergy Clin Immunol. 2020;145(3):757–765. doi:10.1016/j.jaci.2019.12.006
11. Thomas D, McDonald VM, Pavord ID, Gibson PG. Asthma remission: what is it and how can it be achieved? Eur Respir J. 2022;60(5):2102583. doi:10.1183/13993003.02583-2021
12. Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020;75(5):1023–1042. doi:10.1111/all.14221
13. Thaçi D, Simpson EL, Beck LA, et al. Efficacy and safety of dupilumab in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical treatments: a randomised, placebo-controlled, dose-ranging phase 2b trial. Lancet. 2016;387(10013):40–52. doi:10.1016/S0140-6736(15)00388-8
14. Human Science Foundation. Domestic basic technology research report FY2020 “Medical Needs Survey on 60 Diseases (6th)”. (in Japanese). Available from: https://u-lab.my-pharm.ac.jp/%7Esoc-pharm/achievements/img/index/r02.pdf.
15. Kroes JA, Zielhuis SWJ, De Jong K, et al. Cumulative corticosteroid-sparing effect of anti-interleukin-5/5Ra in eosinophilic asthma. Eur Respir J. 2022;60(5):2102983. doi:10.1183/13993003.02983-2021
16. Skov IR, Madsen H, Henriksen DP, Andersen JH, Pottegård A, Davidsen JR. Low-dose oral corticosteroids in asthma associates with increased morbidity and mortality. Eur Respir J. 2022;60(3):2103054. doi:10.1183/13993003.03054-2021
17. Adir Y, Saliba W, Beurnier A, Humbert M. Asthma and COVID-19: an update. Eur Respir Rev. 2021;30(162):210152. doi:10.1183/16000617.0152-2021
18. Kamata M, Tada Y. A literature review of real-world effectiveness and safety of dupilumab for atopic dermatitis. JID Innov. 2021;1(3):100042. doi:10.1016/j.xjidi.2021.100042
19. Tamada T, Fukui K, Makita N, et al. An internet survey on patient perception about current treatment and asthma symptoms in severe asthma patients. Therap Res. 2021;42(12):847–855.
20. Cardet JC, Chang KL, Rooks BJ, et al. Socioeconomic status associates with worse asthma morbidity among Black and Latinx adults. J Allergy Clin Immunol. 2022;150(4):841–849. doi:10.1016/j.jaci.2022.04.030
21. Kachmar AG, Wypij D, Perry MA, Curley MAQ; RESTORE Study Investigators. Income-driven socioeconomic status and presenting illness severity in children with acute respiratory failure. Res Nurs Health. 2021;44(6):920–930. doi:10.1002/nur.22182
22. Hosoya K, Komachi T, Masaki K, et al. Barrier factors of adherence to dupilumab self-injection for severe allergic disease: a non-interventional open-label study. Patient Prefer Adherence. 2023;17:861–872. doi:10.2147/PPA.S389865
23. Israel E, Canonica GW, Brusselle G, et al. Real-life effectiveness of mepolizumab in severe asthma: a systematic literature review. J Asthma. 2022;59(11):2201–2217. doi:10.1080/02770903.2021.2008431
24. Berger P, Menzies-Gow A, Peters AT, et al. Long-term efficacy of dupilumab in asthma with or without chronic rhinosinusitis and nasal polyps. Ann Allergy Asthma Immunol. 2023;130(2):215–224. doi:10.1016/j.anai.2022.11.006
25. Koskeridis F, Evangelou E, Ntzani EE, Kostikas K, Tsabouri S. Treatment with dupilumab in patients with atopic dermatitis: systematic review and meta-analysis. J Cutan Med Surg. 2022;26(6):613–621. doi:10.1177/12034754221130969
26. Lugogo NL, Bogart M, Corbridge T, Packnett ER, Wu J, Hahn B. Impact of mepolizumab in patients with high-burden severe asthma within a managed care population. J Asthma. 2023;60(4):811–823. doi:10.1080/02770903.2022.2102036
27. Ferrari M, Donadu MG, Biondi G, et al. Dupilumab: direct cost and clinical evaluation in patients with atopic dermatitis. Dermatol Res Pract. 2023;2023:4592087. doi:10.1155/2023/4592087
28. Faverio P, Ronco R, Monzio Compagnoni M, et al. Effectiveness and economic impact of Dupilumab in asthma: a population-based cohort study. Respir Res. 2023;24(1):70. doi:10.1186/s12931-023-02372-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.