")
Back to Journals » Clinical Ophthalmology » Volume 17
Significance of Acetylcholine Receptor Antibody Titers in Acetylcholine Receptor Antibody-Positive Ocular Myasthenia Gravis: Generalization and Presence of Thyroid Autoimmune Antibodies and Thymoma
Authors Supawongwattana M, Vanikieti K, Jindahra P, Padungkiatsagul T
Received 21 December 2022
Accepted for publication 15 February 2023
Published 27 February 2023 Volume 2023:17 Pages 649—656
DOI https://doi.org/10.2147/OPTH.S402181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Montana Supawongwattana,1 Kavin Vanikieti,1 Panitha Jindahra,2 Tanyatuth Padungkiatsagul1
1Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Tanyatuth Padungkiatsagul, Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Bangkok, 10400, Thailand, Tel +662 201 1526, Email [email protected]
Objective: To evaluate the association in acetylcholine receptor (AChR) antibody-positive ocular myasthenia gravis (OMG) subjects between AChR antibody titers and conversion to generalized myasthenia gravis (GMG), the presence of thyroid autoimmune antibodies, and the presence of thymoma.
Subjects and Methods: A total of 118 subjects with AChR antibody-positive OMG were included. Demographic data, clinical characteristics, serology tests, presence of thymoma, treatment, and conversion to GMG were retrospectively reviewed. The presence of thyroid autoimmune antibodies was defined as the presence of at least one of the following: (1) thyroid peroxidase antibody; (2) thyroglobulin antibody; (3) thyroid-stimulating hormone receptor antibody. Univariate and multivariate logistic regression analyses were used as methods of evaluating association.
Results: AChR antibody titers were determined in all subjects with a median of 3.33 (0.46– 141.09) nmol/L. The median follow-up period was 14.5 (3– 113) months. At the final follow-up time-point, 99 subjects (83.90%) remained with a diagnosis of pure OMG, while 19 subjects (16.10%) had converted to GMG. An AChR antibody titer ≥ 8.11 nmol/L was associated with the conversion to GMG (odds ratio (OR) 3.66, 95% CI: 1.19– 11.26; p = 0.023). Of the 79 subjects with available thyroid autoimmune antibodies data, 26 subjects (32.91%) displayed the presence of thyroid autoimmune antibodies. An AChR antibody titer ≥ 2.81 nmol/L was associated with the presence of thyroid autoimmune antibodies (OR 6.16, 95% CI: 1.79– 21.22; p = 0.004). Finally, of the 106 subjects with available thoracic computed tomography (CT) data, only 9 subjects (8.49%) demonstrated the presence of thymoma. An AChR antibody titer ≥ 15.12 nmol/L was associated with the presence of thymoma (OR 4.97, 95% CI: 1.10– 22.48; p = 0.037).
Conclusion: AChR antibody titers should be considered in AChR antibody-positive OMG patients. Those with AChR antibody titers ≥ 8.11 nmol/L, who are at a greater risk of conversion to GMG, should be closely monitored and encouraged to be aware of early clinical signs of life-threatening GMG. In addition, serum thyroid autoimmune antibodies and thoracic CT screening for thymoma should be performed in AChR antibody-positive OMG patients, particularly in those with AChR antibody titers ≥ 2.81 nmol/L and ≥ 15.12 nmol/L, respectively.
Keywords: ocular myasthenia gravis, acetylcholine receptor antibody levels, generalized myasthenia gravis, conversion, thymoma, thyroid autoimmune antibodies
Corrigendum for this paper has been published.
Introduction
Myasthenia gravis (MG) is an autoimmune disease characterized by fluctuating muscle weakness with the ocular symptoms (ptosis and/or diplopia) being the most common presentation.1 Approximately 50% of patients present with pure ocular symptoms, classified as ocular MG (OMG), corresponding to class I in the Myasthenia Gravis Foundation of America (MGFA) classification, while the other 50% present with the symptoms of generalization (MGFA classification types II, III, IV, and V).2,3 The diagnosis of OMG is not always clinically evident owing to the unspecific pattern of deficits and variety of ocular presentations mimicking other conditions such as cranial nerve palsy, internuclear ophthalmoplegia, or thyroid eye disease. To address this diagnostic challenge, several serology tests have been developed to confirm the diagnosis of OMG. One of the most widely used serology tests is acetylcholine receptor (AChR) antibody testing, which became the gold standard for OMG diagnosis with 99% specificity and 50–70% sensitivity.4 A few methods of AChR antibody detection are currently available: radioimmunoprecipitation assay (RIPA); enzyme-linked immunosorbent assay (ELISA); and cell-based assays (CBAs).
The treatment of OMG includes symptomatic treatment with a cholinesterase inhibitor (pyridostigmine), systemic corticosteroids, and immunosuppressive agents. Despite a generally good response to treatment, conversion to generalized MG (GMG) has been reported to occur within the first 2 years of the disease in 20–80% of OMG patients.5 Previous reports have discovered significant risk factors for GMG conversion, including older age at onset, history of smoking, presence of thymoma, abnormal repetitive nerve stimulation or single fiber electromyography, and positive for the AChR antibody.2,5–8 Although many studies showed that seropositivity to AChR antibody was one of the significant risk factors for GMG conversion, the association between AChR antibody titers and the conversion to GMG has been scarcely studied.
Many studies found that MG is associated with other autoimmune diseases, particularly autoimmune thyroid diseases: Graves’ disease and Hashimoto’s thyroiditis.9 Several studies demonstrated an association between the presence of thymoma with the seropositivity to AChR antibody.10 However, to the best of our knowledge, none of these studies have investigated the association between the quantitative measurement of AChR antibody titers and the presence of thyroid autoimmune antibodies or of thymoma, particularly in OMG patients.
Therefore, we aimed to evaluate the association in AChR antibody-positive OMG subjects between AChR antibody titers and conversion to GMG, the presence of thyroid autoimmune antibodies, and the presence of thymoma.
Materials and Methods
This study followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand (IRB number: COA. MURA2022/379), which waived the need for written informed consent from the subjects due to the retrospective nature of the study. All data were kept confidentially in our database. Electronic medical records were reviewed to identify all subjects diagnosed with MG in the Ramathibodi Hospital, Mahidol University, Bangkok, Thailand from January 2012 to June 2022.
Subject Selection
Subjects who met all of the following criteria were included: (1) age at onset ≥18 years; (2) had ocular symptoms of fluctuating ptosis and/or diplopia at onset and being diagnosed with OMG; (3) had a positive AChR antibody test with quantitatively measured antibody titers obtained at the first visit from January 2012 to June 2022. Exclusion criteria included subjects with one or more of the following at the first visit: (1) presenting with GMG; (2) known underlying autoimmune diseases; (3) taking systemic corticosteroids within the previous 3 months; (4) taking immunosuppressive agents.
Demographic Data, Clinical Characteristics, Serology Tests, and Presence of Thymoma
Demographic data and clinical characteristics, including age at onset, sex, underlying diseases, initial ocular signs (moderate-to-severe ptosis, which was defined as a margin reflex distance 1 (MRD1) ≤3 mm, lid fatigability, Cogan lid twitch, orbicularis oculi weakness, and duction limitation), and ice-pack test result (improvement of MRD1 by 2 mm was considered a positive test result) were reviewed.
Regarding the serology tests, AChR antibody titers performed using an ELISA method (EUROIMMUN Analyzer I, Seekamp, Lübeck, Germany) with a value >0.45 nmol/L were considered a positive result. Abnormal thyroid function tests were defined as an abnormality in at least one of the following: (1) thyroid stimulating hormone; (2) Free T3; (3) Free T4. The presence of thyroid autoimmune antibodies was defined as the presence of at least one of the following: (1) thyroid peroxidase antibody; (2) thyroglobulin antibody; (3) thyroid-stimulating hormone receptor antibody. AChR antibody titers, as well as other serology tests, were performed at the first visit.
The presence of thymoma was defined as the radiological presence of thymoma based on thoracic computed tomography (CT), which was performed within 1 month after the first visit.
Treatment and Conversion to GMG
Treatment was categorized into two groups: “pyridostigmine alone” and “immunosuppressive treatment” (ie, systemic corticosteroids and/or immunosuppressive agents with/without pyridostigmine). Regarding conversion to GMG, pure OMG was defined as subjects with pure ocular symptoms for at least 3 months from the onset of symptoms, and conversion to GMG was defined as the presence of at least one of the following symptoms during follow-up; hoarseness, dysarthria, dysphagia, dyspnea, and weakness of extremities and the neck, predominantly at proximal muscles. The diagnosis of GMG conversion was confirmed by neurologists. Time to conversion was recorded as the interval from onset of ocular symptoms to GMG conversion.
Statistical Analysis
Continuous variables were expressed using the mean or median, with normally distributed results shown as mean ± standard deviation (SD) and non-normally distributed results shown as median and range. Independent t-test or Mann–Whitney U-test, where appropriate, were used to compare continuous variables. Categorical variables were expressed as frequency and percentage. These variables were compared using Chi-squared or exact test where appropriate. The optimal cut-off values were identified using the maximal Youden’s index value.11 For multivariate analysis, logistic regression was applied, to simultaneously regress outcomes with variables whose p-values in univariate analysis were <0.1. The likelihood ratio test was applied to select and retain only significant variables in the final equation. Statistical analyses were performed using STATA software, version 17.0 (StataCorp LLC, College Station, TX, USA). Differences were reported with 95% confidence interval (CI). P-values of <0.05 were considered statistically significant.
Results
A total of 118 subjects with AChR antibody-positive OMG were included in the study. The mean age at onset was 56.1 ± 16.9 years. Of these 118 subjects, 73 (61.86%) were female. The most common initial ocular sign was moderate-to-severe ptosis, which was presented in 90 subjects (76.27%). AChR antibody titers were identified in all subjects with a median of 3.33 (0.46–141.09) nmol/L. Among the 79 subjects with available thyroid autoimmune antibodies data, 26 subjects (32.91%) displayed the presence of thyroid autoimmune antibodies. There were 106 subjects with available thoracic CT data, of whom 9 (8.49%) demonstrated the presence of thymoma. Regarding treatment, 69 subjects (58.47%) were treated with pyridostigmine alone, while the remaining 49 subjects (41.53%) received immunosuppressive treatment. The median follow-up period was 14.5 (3–113) months. Conversion to GMG was observed in 19 subjects (16.10%) with a median time to conversion of 30 (3–96) months. Detailed demographic data, clinical characteristics, serology tests, presence of thymoma, treatment, and conversion to GMG of the study subjects are summarized in Table 1.
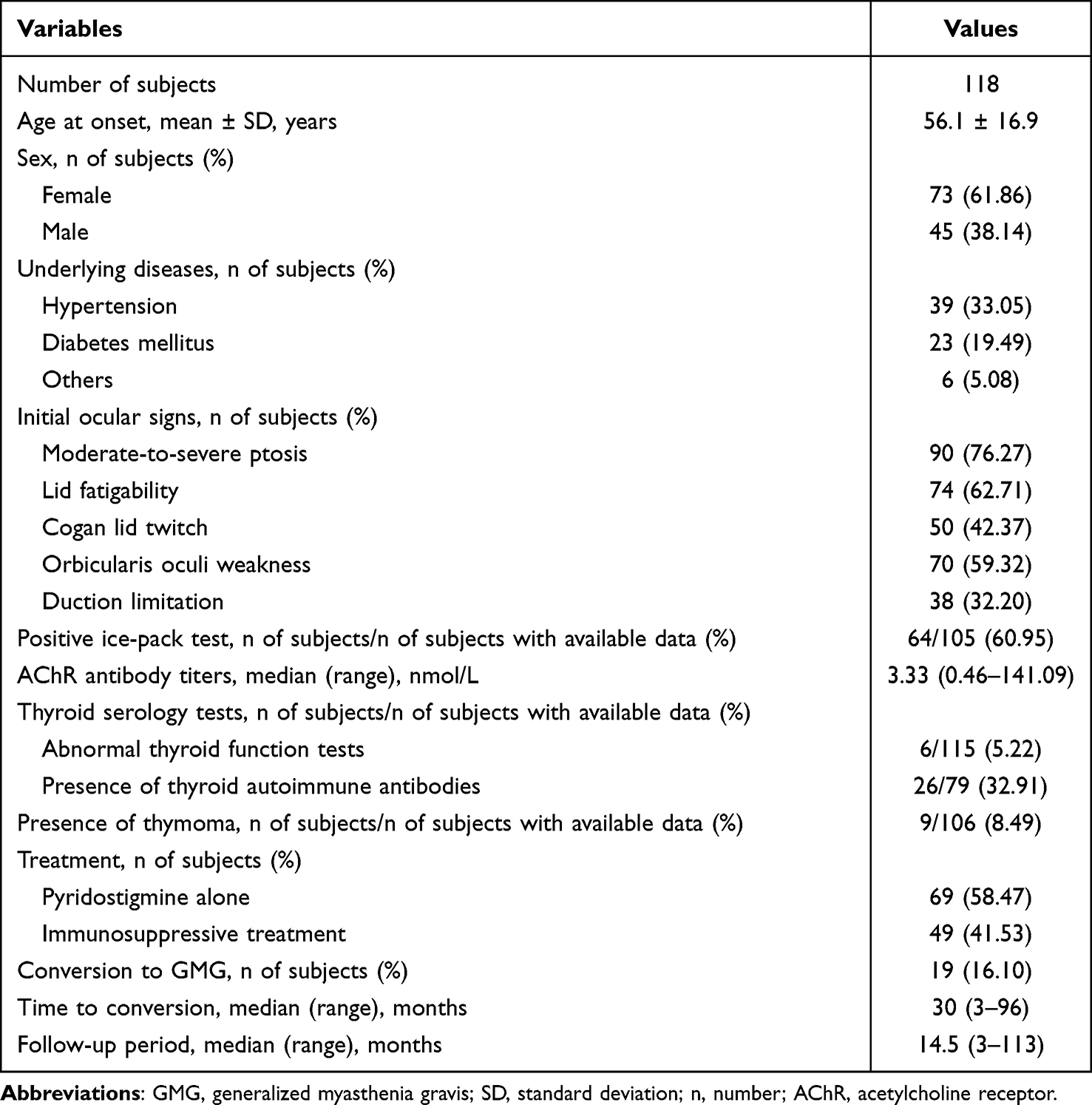 |
Table 1 Detailed Demographic Data, Clinical Characteristics, Serology Tests, Presence of Thymoma, Treatment, and Conversion to GMG of the Study Subjects |
At the final follow-up time-point, 99 subjects (83.90%) remained being diagnosed with pure OMG, while 19 subjects (16.10%) had converted to GMG. The best performance of AChR antibody titers to predict a conversion from OMG to GMG was investigated with a proposed cut-off value of 8.11 nmol/L (area under the curve (AUC) 0.766, 95% CI: 0.642–0.890, sensitivity: 71%, specificity: 70%). Multivariate analysis revealed that an AChR antibody titer ≥8.11 nmol/L (odds ratio (OR) 3.66, 95% CI: 1.19–11.26; p = 0.023) was the only significant factor associated with the conversion to GMG (Table 2).
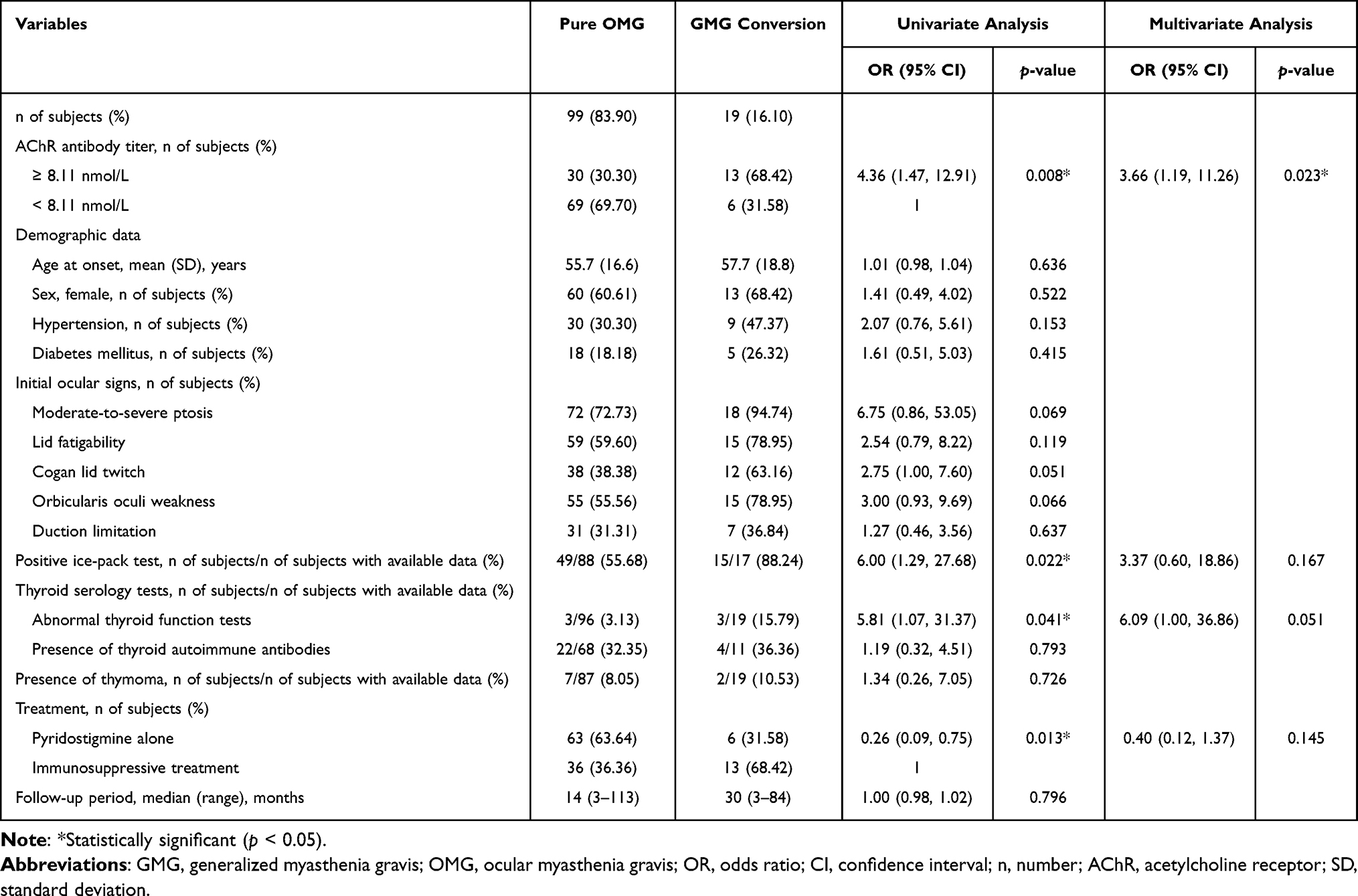 |
Table 2 Factors Associated with Conversion to GMG |
Of the 79 subjects with available thyroid autoimmune antibodies data, 26 subjects (32.91%) displayed the presence of thyroid autoimmune antibodies. The best threshold of AChR antibody titers to be associated with the presence of thyroid autoimmune antibodies was investigated and a cut-off value of 2.81 nmol/L was proposed (AUC 0.662, 95% CI: 0.532–0.792, sensitivity: 73%, specificity: 57%). Given the higher incidence and prevalence of autoimmune diseases in females and more evidence of thymoma producing various autoantibodies,12,13 these two factors were also included in the multivariate analysis despite their p-values of >0.1 in univariate analysis. However, multivariate analysis demonstrated that an AChR antibody titer ≥2.81 nmol/L (OR 6.16, 95% CI: 1.79–21.22; p = 0.004) was the only significant factor associated with the presence of thyroid autoimmune antibodies (Table 3).
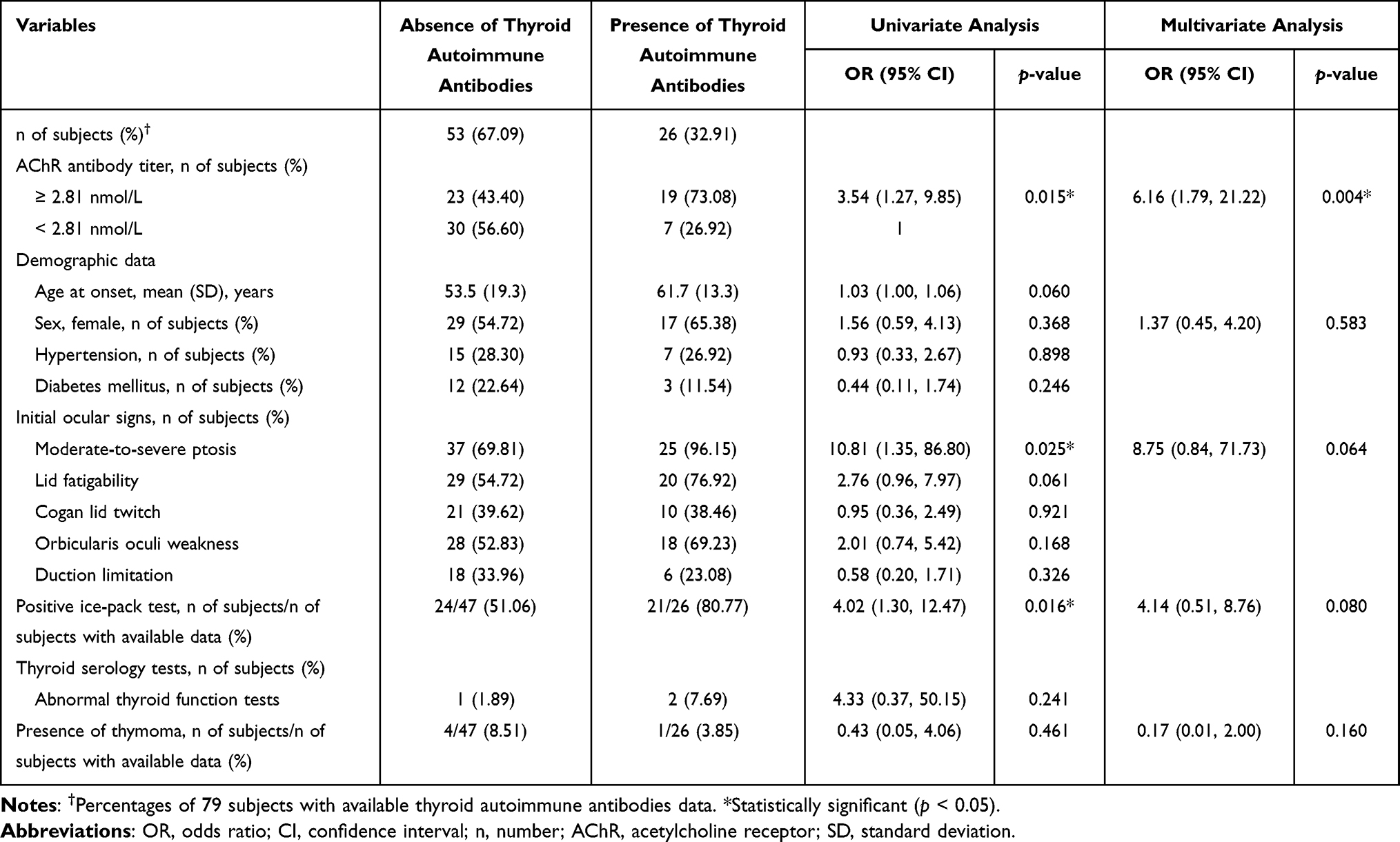 |
Table 3 Factors Associated with the Presence of Thyroid Autoimmune Antibodies |
Of the 106 subjects with available thoracic CT data, only 9 subjects (8.49%) demonstrated the presence of thymoma. The best threshold of AChR antibody titers to be associated with the presence of thymoma was investigated with a proposed cut-off value of 15.12 nmol/L (AUC 0.631, 95% CI: 0.445–0.817, sensitivity: 44%, specificity: 84%). Despite lacking a significant association of age at onset and sex with the presence of thymoma in univariate analysis, both factors were still included in the multivariate analysis owing to the results from previous literature showing a higher prevalence of thymoma in a younger age group and in females.14 Nevertheless, multivariate analysis showed that an AChR antibody titer ≥15.12 nmol/L (OR 4.97, 95% CI: 1.10–22.48; p = 0.037) was the only significant factor associated with the presence of thymoma (Table 4).
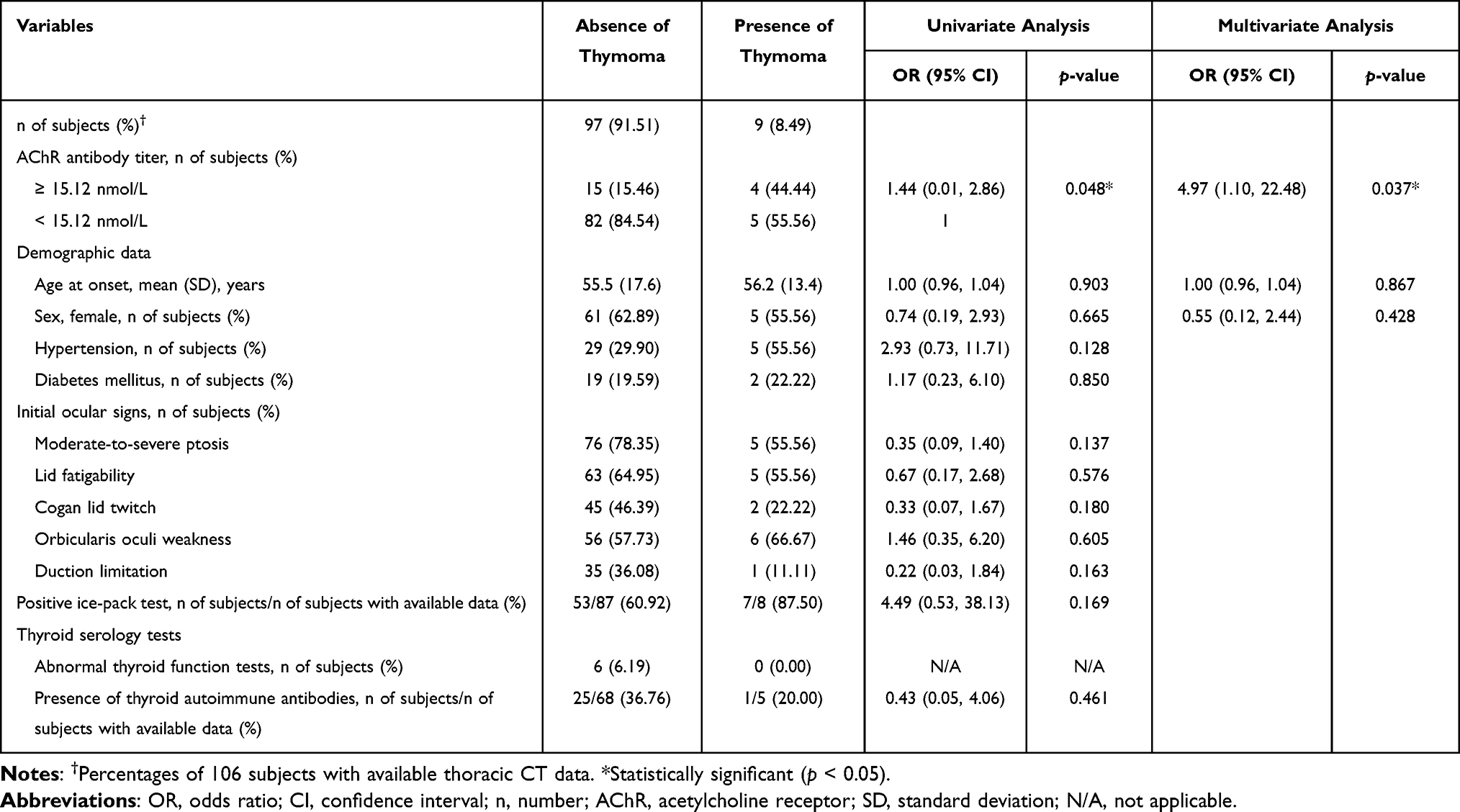 |
Table 4 Factors Associated with the Presence of Thymoma |
Discussion
In this study, we retrospectively reviewed electronic medical records of 118 AChR antibody-positive OMG subjects aiming to evaluate the association between AChR antibody titers and conversion to GMG, the presence of thyroid autoimmune antibodies, and the presence of thymoma.
Our study revealed that an AChR antibody titer ≥8.11 nmol/L was significantly associated with conversion to GMG. Only a few studies showed an association between a higher titer of AChR antibodies and GMG conversion. Peeler et al were the first to report that OMG subjects who developed GMG had significantly higher AChR antibody titers (RIPA method) than those who did not develop GMG (mean: 12.7 vs 4.2 nmol/L; p <0.05).2 Feng et al also revealed a parallel trend to ours, demonstrating a strong association between higher AChR antibody titers (ELISA method) and conversion to GMG.15 They proposed AChR antibody titers ≥6.13 nmol/L as a predictive factor of GMG conversion. However, there were only 19 subjects with available AChR antibody titers in their study. Therefore, from our results, close monitoring and encouraging awareness of the higher risk of life-threatening GMG are recommended in AChR antibody-positive OMG patients with AChR antibody titers ≥8.11 nmol/L.
Autoimmune thyroid diseases are associated with MG, with Graves’ disease and Hashimoto’s thyroiditis as the two most common such autoimmune diseases.9 Amin et al reported a 2.36-fold increased risk of autoimmune thyroid diseases in MG patients.9 However, to the best of our knowledge, no reports have shown an association between AChR antibody titer and the presence of thyroid autoimmune antibodies, particularly in OMG patients. We discovered that an AChR antibody titer ≥2.81 nmol/L was significantly associated with the presence of thyroid autoimmune antibodies. This finding is comparable with a previous study from China, which reported that thyroid autoimmune antibodies-positive MG subjects had higher AChR antibody titers than thyroid autoimmune antibodies-negative MG subjects.16 However, unlike our study, they included subjects who for the majority of the study presented with GMG. Thereby, we suggest investigation for serum thyroid autoimmune antibodies in AChR antibody-positive OMG patients, particularly in those with AChR antibody titers ≥2.81 nmol/L.
We demonstrated that an AChR antibody titer ≥15.12 nmol/L in OMG subjects was significantly associated with the presence of thymoma. The increase in T-follicular helper cell activity in thymomatous MG patients, which leads to increased autoimmune antibody production (eg, AChR antibody), might explain this finding.13 Accordingly, we emphasize the importance of thoracic CT screening for thymoma in AChR antibody-positive OMG patients, particularly in those with AChR antibody titers ≥15.12 nmol/L.
This study had several strengths. First, to the best of our knowledge, this is the first study to establish an association between AChR antibody titers in OMG subjects and the presence of thyroid autoimmune antibodies and of thymoma. It is also the first study among the Thai population to demonstrate an association between AChR antibody titers and conversion to GMG. Second, the diagnosis of OMG in all included subjects was confirmed by an AChR antibody test together with its quantitative titers. Finally, this study enrolled the largest number of AChR antibody-positive OMG subjects for any such study in Thailand.
There were some limitations to this study. First, it had a retrospective design, which resulted in some data loss. Second, given that our inclusion criteria included subjects exclusively with a positive AChR antibody test, the application of our results to AChR antibody-negative OMG patients is limited. Finally, this study did not determine the association between AChR antibody titers and the time to conversion in those subjects who converted to GMG.
Conclusions
AChR antibody titers should be considered in AChR antibody-positive OMG patients. We recommend that those with AChR antibody titers ≥8.11 nmol/L, and who thereby are at a greater risk of conversion to GMG, should be closely monitored and encouraged to be aware of early clinical signs of life-threatening GMG. In addition, we recommend that serum thyroid autoimmune antibodies and thoracic CT screening for thymoma should be performed in AChR antibody-positive OMG patients, particularly in those with AChR antibody titers ≥2.81 nmol/L and ≥15.12 nmol/L, respectively.
Acknowledgments
The authors would like to thank Ms Sasiporn Sitthisorn, Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, for her advice on the statistical analysis. We thank Robert Blakytny, DPhil, from Edanz (www.edanz.com/ac) for editing a draft of this manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kirzinger L, Schotz S, Schalke B. Pure ocular myasthenia gravis. Neurol Int Open. 2018;2:E51–E55. doi:10.1055/s-0043-122245
2. Peeler CE, Lott LBD, Eggenberger ER, et al. Clinical utility of acetylcholine receptor antibody testing in ocular myasthenia gravis. JAMA Neurol. 2015;72(10):1170–1174. doi:10.1001/jamaneurol.2015.1444
3. Jaretzki AIII, Barohn RJ, Sanders DB, et al. Myasthenia gravis: recommendations for clinical research standards. Neurology. 2000;55(1):16–23. doi:10.1212/WNL.55.1.16
4. Lazaridis K, Tzartos SJ. Autoantibody specificities in myasthenia gravis; implications for improved diagnostics and therapeutics. Front Immunol. 2020;11:212. doi:10.3389/fimmu.2020.00212
5. Apinyawasisuk S, Chongpison Y, Thitisaksakul C, et al. Factors affecting generalization of ocular myasthenia gravis in patients with positive acetylcholine receptor antibody. Am J Ophthalmol. 2020;209:10–17. doi:10.1016/j.ajo.2019.09.019
6. Kisabay A, Ozdemir HN, Gokcay F, et al. Risk for generalization in ocular onset myasthenia gravis: experience from a neuro-ophthalmology clinic. Acta Neurol Belg. 2022;122(2):337–344. doi:10.1007/s13760-020-01582-1
7. Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2 years in patients with ocular myasthenia gravis. Arch Neurol. 2003;60(2):243–248. doi:10.1001/archneur.60.2.243
8. Hendricks TM, Bhatti MT, Chen JJ, et al. Incidence, epidemiology, and transformation of ocular myasthenia gravis: a population based study. Am J Ophthalmol. 2019;205:99–105. doi:10.1016/j.ajo.2019.04.017
9. Amin S, Aung M, Malik H, et al. Myasthenia gravis and its association with thyroid diseases. Cureus. 2020;12(9):e10248. doi:10.7759/cureus.10248
10. Okumura M, Fujii Y, Shiono H, et al. Immunological function of thymoma and pathogenesis of paraneoplastic myasthenia gravis. Gen Thorac Cardiovasc Surg. 2008;56(4):143–150. doi:10.1007/s11748-007-0185-8
11. Hakian-Tialaki K. The choice of methods in determining the optimal cutoff value for quantitative diagnostic test evaluation. Stat Methods Med Res. 2018;27(8):2374–2383. doi:10.1177/0962280216680383
12. Angum F, Khan T, Hussain A, et al. The prevalence of autoimmune disorders in women: a narrative review. Cureus. 2020;12(5):e8094. doi:10.7759/cureus.8094
13. Song Y, Zhou L, Chen Z, et al. Increased frequency of thymic T follicular helper cells in myasthenia gravis patients with thymoma. J Thorac Dis. 2016;8(3):314–322. doi:10.21037/jtd.2016.03.03
14. Zhang J, Zhang H, Zhang P, et al. Thymectomy in ocular myasthenia gravis - prognosis and risk factors analysis. Orphanet J Rare Dis. 2022;17(1):309. doi:10.1186/s13023-022-02454-y
15. Feng X, Huan X, Zhao C, et al. Adult ocular myasthenia gravis conversion: a single-center retrospective analysis in China. Eur Neurol. 2020;83(2):182–188. doi:10.1159/000507853
16. Chen YP, Wei DN, Chen B. The clinical features of myasthenia gravis associated with thyroid abnormalities. Zhonghua Nei Ke Za Zhi. 2010;49(7):602–605.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.