Back to Journals » Patient Preference and Adherence » Volume 17
Sickle Cell Disease Knowledge and Reproductive Decisions: A Saudi Cross-Sectional Study
Authors Alsalman M ![]() , Alhamoud H, Alabdullah Z, Alsleem R, Almarzooq Z, Alsalem F, Alsulaiman A, Albeladi A, Alsalman Z
, Alhamoud H, Alabdullah Z, Alsleem R, Almarzooq Z, Alsalem F, Alsulaiman A, Albeladi A, Alsalman Z ![]()
Received 14 January 2023
Accepted for publication 15 March 2023
Published 21 March 2023 Volume 2023:17 Pages 761—767
DOI https://doi.org/10.2147/PPA.S404811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Mortadah Alsalman,1 Hassan Alhamoud,2 Zainab Alabdullah,1 Raghad Alsleem,1 Zainab Almarzooq,1 Fatemah Alsalem,1 Ahmed Alsulaiman,3 Abdullah Albeladi,2 Zaenb Alsalman4
1Department of Medicine, College of Medicine, King Faisal University, Al Ahsa, Saudi Arabia; 2Department of Medicine, King Fahad Hospital, Al Hofuf, Saudi Arabia; 3College of Medicine, Vision Colleges, Riyadh, Saudi Arabia; 4Departments of Family and Community Medicine, College of Medicine, King Faisal University, Al Ahsa, Saudi Arabia
Correspondence: Zaenb Alsalman, College of Medicine, King Faisal University, Po Box 3311, Al Ahsa, 36346, Saudi Arabia, Tel +966545611633, Email [email protected]
Background and Aim: Sickle cell disease (SCD) is an autosomal recessive disorder. Decisions following premarital screening results might be influenced by several factors. Thus, this study aims to assess the knowledge and beliefs toward SCD and reproductive decisions.
Material and Methods: A cross-sectional study was conducted among adults in the eastern province of Saudi Arabia. Data was collected using a web-based questionnaire. Participants were divided into two groups based on their knowledge scores.
Results: A total of 390 participants were recruited with a mean age of 28.6 years. The majority (90.5%) of participants had general knowledge about the disease mode of inheritance however, 66.9% had poor knowledge about the disease overall. Regarding knowledge level, there was no statistically significant difference between the non-healthy group (diseased and carrier) and healthy participants (P=0.304). Moreover, the participants’ decisions about choosing future partners were more likely to be affected among those with prior knowledge about the disease (p=0.008). However, 152 (91.6%) male participants with prior knowledge would change their decision about selecting a future partner compared to 225 (92.4%) female participants. Regarding reproduction, only 38.5% of participants were aware of in vitro fertilization (IVF) as an assistive reproductive technology. Furthermore, female participants believed that IVF is a way to have healthy babies and would consider it despite the cost more than male participants (p=0.0001, p=0.007 respectively).
Conclusion: SCD is an inherited disease with economic, physical, and psychological burdens. However, curative options are costly, and hence, prevention is key. Therefore, healthcare decision-makers should consider implementing policies to minimize the financial burden that may still affect society despite the availability of free medical care. This study warrants extensive community-based education programs that may contribute toward cost savings. It also highlights the importance of premarital counselling for disease and carrier people including alternative reproduction options.
Keywords: sickle cell disease, in vitro fertilization, counselling
Introduction
Medical genetics enhances the understanding of human diseases and reveals that almost all diseases are influenced by genetic variation. However, there are several challenges in the field, and the magnitude of the problem varies across the globe. Genetic disorders are more common in Arab countries with a high prevalence of glucose-6-phosphate dehydrogenase deficiency and hemoglobinopathies.1,2 Hemoglobinopathies are the most commonly inherited diseases in humans, and at least 5% of the world’s population are genetic carriers for them, of which 3.2% carry sickle cell disease (SCD).3,4
SCD is an autosomal recessive disorder characterized by the production of abnormal hemoglobin S and is considered one of the most noteworthy single-gene disorders among human beings. The hallmark of the disease is episodic, recurrent, and unpredictable episodes of acute pain that are reflected on the patient’s health-related quality of life.5,6 Its prevalence has been significantly increasing in most of sub-Saharan Africa, the Mediterranean, and the Middle East.7,8 Saudi Arabia is one of the most prone territories compared to its surrounding countries, particularly in the eastern and southern regions, which may be due to high rates of consanguineous marriages. Therefore, Saudi Arabia launched its premarital screening and genetic counselling program in 2004 to reduce the burden of hemoglobinopathy disorders.3 This program estimated that the sickle cell trait prevalence is 4.2% and the disease prevalence is 0.26%, with the Eastern province having the greatest prevalence (about 17% for trait and 1.2% for disease).7 However, decisions following the premarital screening results might be influenced by several factors. Thus, this study aims to assess the knowledge and beliefs of the community toward SCD and reproductive decisions.
Materials and Methods
A cross-sectional study was conducted from February to March 2021 among adults in the eastern province of Saudi Arabia. Using the Open Epi, the minimum required sample was calculated to be 384 by assuming that the proportion of adults’ knowledge is 50% at a confidence level of 95%, power of 80%, and a degree of precision of 5%.
Data was collected using a web-based, self-administered questionnaire that was sent via social media and included four sections: participants’ sociodemographic data, knowledge about SCD, beliefs on how SCD affects participants’ life, and reproductive decisions. For SCD knowledge each correct answer was scored one point and a total summation of the different items was collected. Participants were divided into two groups based on their knowledge scores; those with scores of less than 60% (4 points) of the maximum score were classified as having poor knowledge, while those with scores of 60% (5 points) or more of the maximum were classified as having good knowledge. To assess the validity and reliability of the questionnaire (Cronbach’s alpha > 0.7), it was reviewed by two experts and piloted among 13 participants who were not part of the sample.
Collected data was analyzed using the International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS), version 23. The descriptive analysis was performed with frequencies and percentages for categorical variables, as well as the mean and standard deviation for continuous variables The significance of the association between categorical variables was evaluated using the chi-square test. A p-value less than 0.05 was considered significant.
The study was approved by King Faisal University’s ethical committee and complied with the Declaration of Helsinki. Also, participants provided their informed consent after being aware of the study’s aim, the benefits of conducting the study, confidentiality, and data anonymity.
Results
Characteristics of Participants
The knowledge and beliefs of the community toward SCD and reproductive decisions were evaluated among 390 participants from the eastern province of Saudi Arabia, with a mean age of 28.6 ± 11.9 years ranging from 18 to 55 years. The remaining participants’ demographic and general characteristics are shown in Table 1.
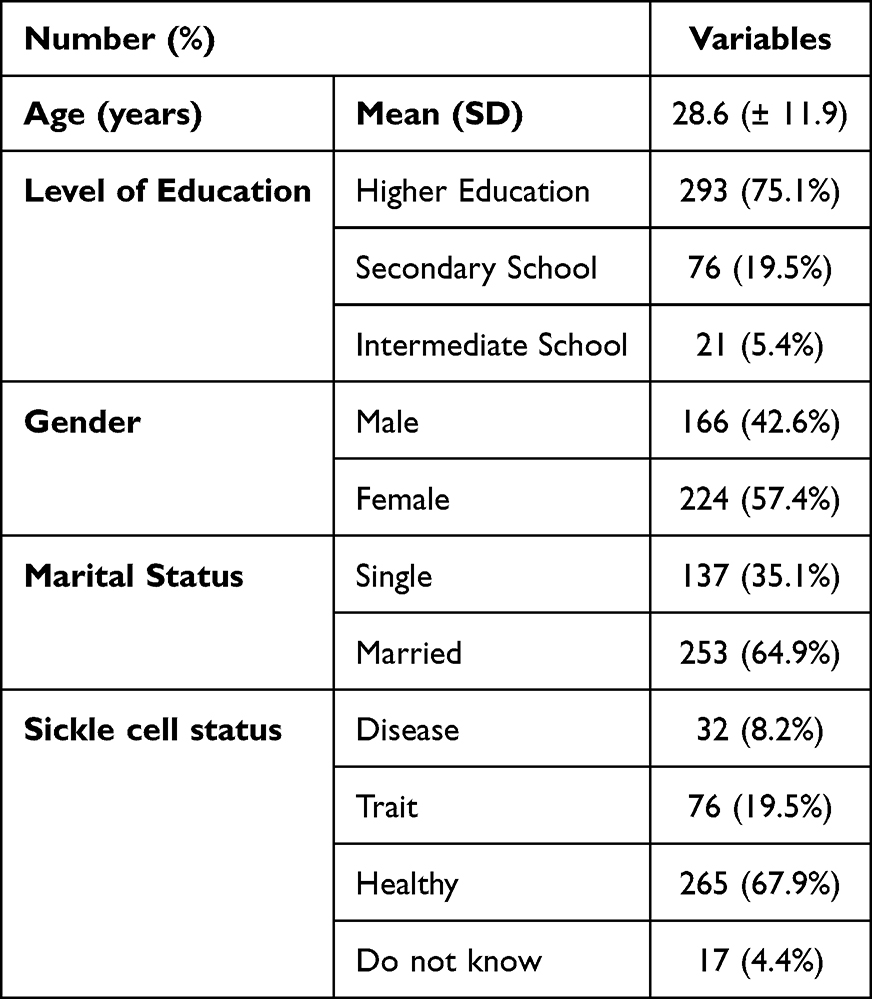 |
Table 1 Demographic and General Characteristics (N=390) |
SCD Knowledge
Out of the 390 participants, 353 (90.5%) had general knowledge about the mode of inheritance of the disease, and 357 (91.5%) were aware that pain is the hallmark of the disease. Over half of the participants (51%) knew about stem cell transplantation as a form of SCD treatment, but only one-third knew about gene therapy. Although the majority of participants (79.5%) reported the blood sample as a diagnostic method, 234 (66.9%) had poor knowledge about the disease overall and its complications (Table 2).
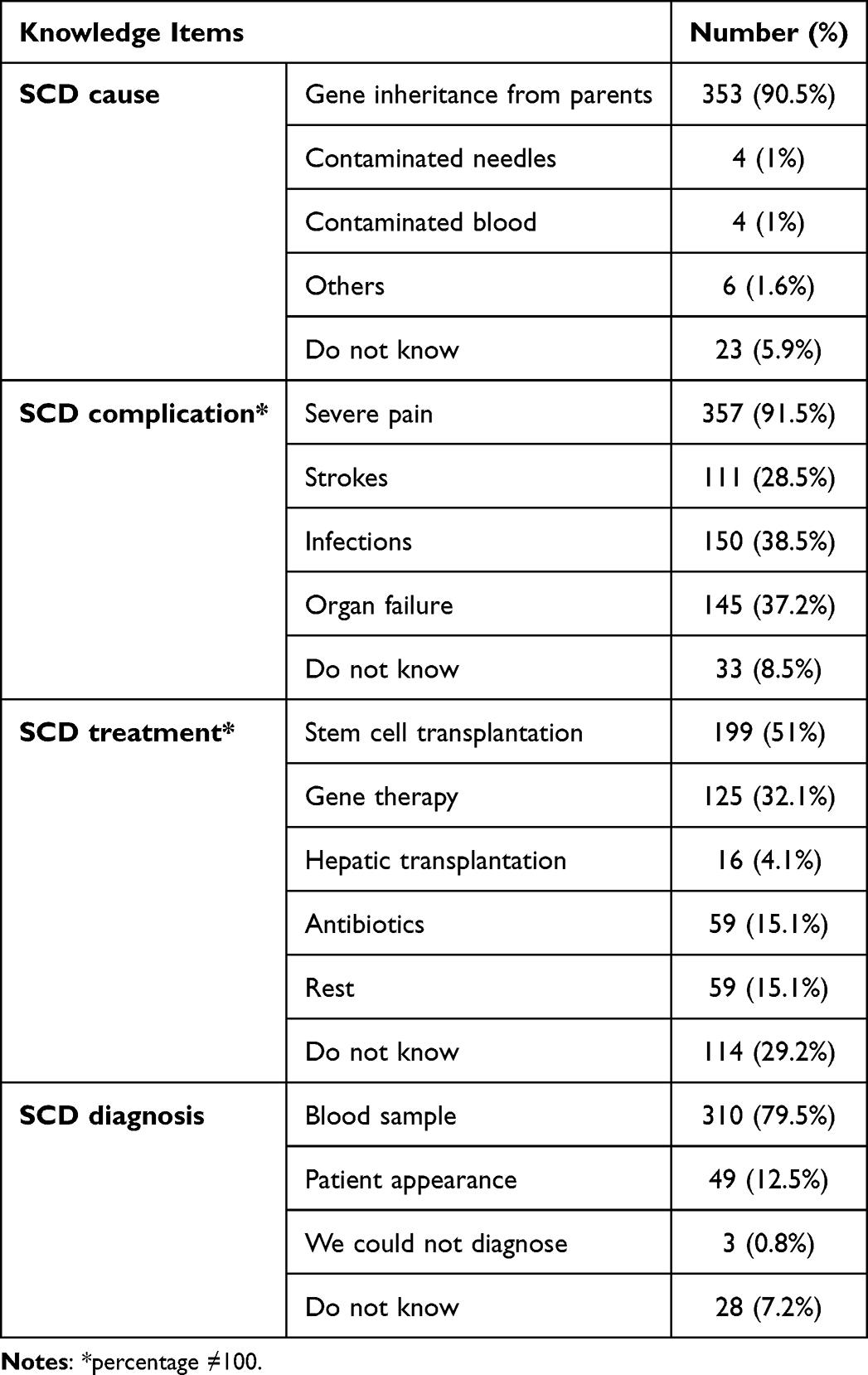 |
Table 2 Participant’s Knowledge About SCD (N=390) |
With regard to the relation between knowledge level and SCD status, there was no statistically significant difference between the non-healthy group (diseased and carrier) and healthy participants (37% vs 31.6%; P-value 0.304) (Figure 1).
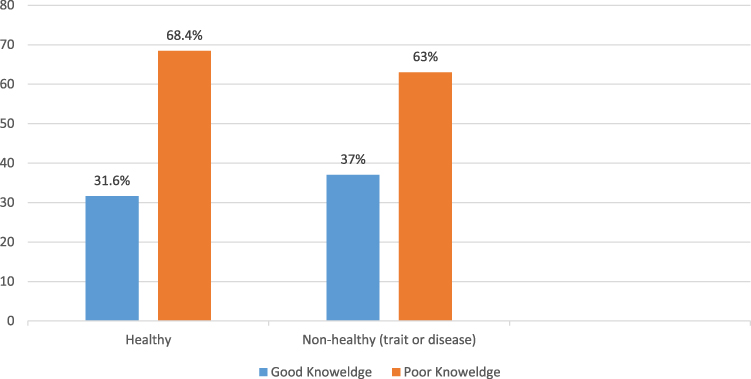 |
Figure 1 Association between level of SCD knowledge and SCD status. |
Beliefs About SCD
Regarding SCD beliefs, 329 (84.4%) of participants agreed that it is a serious disease, and 345 (88.7%) admitted that having a child with SCD is alarming and that such a child requires careful care. Further, 313 (80.3%) reported that having children with SCD will negatively affect their lives (Table 3).
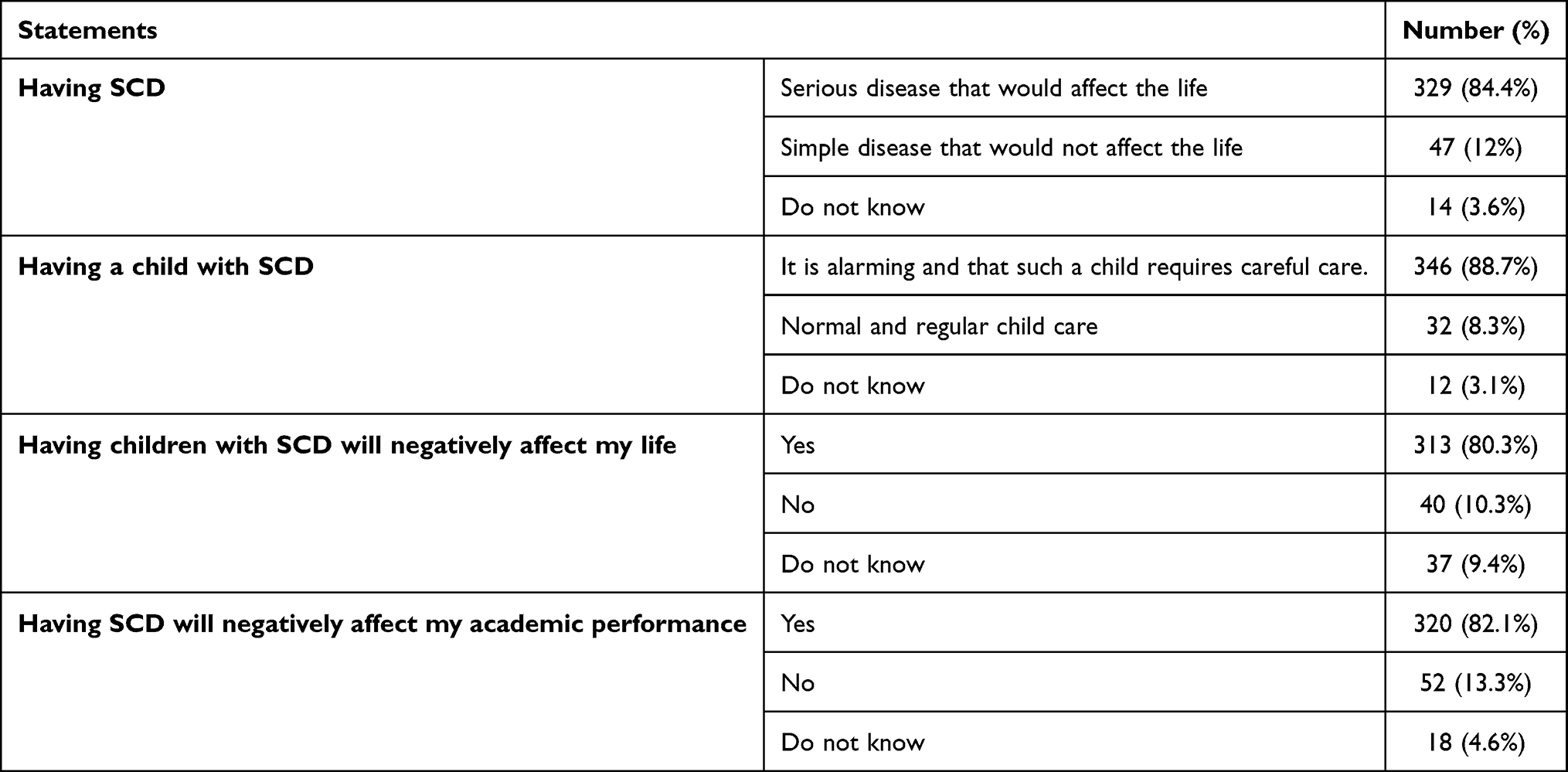 |
Table 3 Participant’s Beliefs on How SCD Affects Their Life (N=390) |
Marital and Reproductive Decision
The participants’ decisions about choosing future partners were more likely to be affected among those with prior knowledge about the disease severity compared to those with poor knowledge about it (97.7% vs 89.3%, p-value 0.008). However, female participants with prior knowledge would change their decision higher than male participants with no statistically significant (92.4% vs 91.6%, p-value 0.81).
Regarding reproduction, only 150 (38.5%) participants were aware of in vitro fertilization (IVF) as an assistive reproductive technology to have a healthy baby. Participants with good knowledge of IVF outnumbered those with poor knowledge of it (55% vs 30.3%, p-value 0.001). However, only 47 (36.4%) of those with good knowledge of IVF would consider it to have healthy children compared to 54 (20.7%) of those with poor knowledge of it (p-value 0.003). Furthermore, 102 (45.5%) female participants believed that IVF is a way to have healthy babies compared to 48 (28.9%) male participants (p-value 0.0001). Moreover, 67 (29.9%) women would consider IVF despite the cost compared to 34 (20.5%) men (p-value 0.007).
Discussion
There are globally increasing concerns and attention for the prevention of non-communicable diseases or chronic diseases.9 However, the establishment of preventive programs for hereditary diseases is central as well. This is particularly relevant for areas where these diseases are endemic and consanguinity has a major influence on their prevalence.10 Autosomal recessive diseases, particularly SCD, are quite prevalent in Saudi Arabia. This is mainly attributed to the increased rate of consanguinity, which can escalate to 50%. Furthermore, several disease-modifying agents such as hydroxyurea have a major role in improving the short- and long-term clinical course of SCD11,12 However, treatment suitability and the complex nature of the disease mandate multimodal therapy, which makes management challenging.13,14 Additionally, the economic burden of the disease itself and the cost of available curative treatment (eg, allogeneic stem cell transplant) is significant.15,16 In the US, the overall cost of SCD-related medical treatment usually increased with age, from $892 to $2562 per patient-month for patients ages 0 to 9 and 50 to 64 years, respectively.16 Although there is a lack of data on the financial impact of SCD in Saudi Arabia, it is expected to cost an average of $13,700 per patient per year in Gulf countries. Despite the fact that healthcare is free of charge in Saudi Arabia, SCD has a significant economic burden on Saudi society as well as an impact on the patient’s quality of life.17 Therefore, launching a premarital screening program is justified in this area.7,10
In our study, we found that the majority of the participants were aware of SCD’s mode of inheritance and pain as the main (and frequent) presentation of the disease. However, their knowledge about the short- and long-term complications of the disease was poor, which is highly consistent with the results of previous reports.18 However, a large percentage of the participants believed that having children with SCD will alter their quality of life. Impressively, our results revealed no statistical difference in knowledge between people with SCD and healthy participants, which emphasizes the urgent need for education programs that focus mainly on sufferers and carriers.
Marital decisions are influenced by several factors, including knowledge, culture, and personal background. Additionally, couples are not enforced to make decisions based on screening results. This means that prevention through premarital screening is unpredictable, and thus, another method of prevention should be mandated.7,19 In the current study, a lack of knowledge negatively affected the process of making marital decisions, without statistical differences between the male and female participants. These findings are consistent with those of previous studies that reveal that only a minority are aware of SCD and a majority have misconceptions about the potential benefit of family discussions and raising awareness of the disease.20,21
IVF is an example of a successful treatment for infertility. However, the addition of preimplantation genetic screening (PGS) is used to maximize success and is employed to aid in the selection of the embryo with the best chance of live birth.22,23 Though it is an expensive approach, it is worth consideration given the annual economic burden of SCD and other curative options.15,16 However, the literature lacks the benefit of this approach among SCD patients.24 This is reflected in the knowledge at the community level. In our study, we found that only around one-third of the participants were aware of IVF as an assistive reproductive approach to have a healthy baby. The decision to seek IVF treatment might be influenced by religious, cultural, and financial factors. However, the cost is commonly cited as the biggest obstacle, which in Saudi Arabia is on average SR 27,360 per IVF cycle.25 Interestingly, both the female gender and good knowledge about the disease influence the choice of IVF as a preventive method irrespective of the cost. A possible explanation is that men experience more social stigma, and loss of masculine identity when undergoing IVF treatment. Moreover, if couples are aware of the consequences of the disease they will try to minimize the chance of having a child with SCD.
This study shed light on the importance of education and counselling not only about the disease overall but also about its short- and long-term complications, impact on the healthcare system, family burden, academic performance, and reproductive options. The availability of IVF has a significant influence on marital decisions and the future of the disease, but the treatment cost and lack of evidence among SCD patients hamper such influence. On this basis, future studies should consider costs on the overall economic burden of SCD management and the factor influencing decisions to seek IVF treatment among Saudi SCD patients. Some limitations might affect the results of our study. The study was not performed at the time of premarital counselling, and it already included married participants, which may result in bias, and it does not reflect actual responses.
Conclusions
SCD is an inherited multisystemic disease with economic, physical, and psychological burdens. However, curative options are costly and limited, and hence, prevention is key. Therefore, healthcare decision-makers should consider implementing policies to minimize the financial burden that may still affect society despite the availability of free medical care. This study warrants extensive community-based education programs and should not be limited to the physical impact of the disease but rather cover its non-physical aspects as well that may contribute toward cost savings. It also highlights the importance of premarital counselling for disease and carrier people including alternative reproduction options for having healthy babies.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We would like to all participants for their collaboration.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for fit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Gazali L, Hamamy H, Al-Arrayad S. Genetic disorders in the Arab world. BMJ. 2006;333(7573):831–834. doi:10.1136/bmj.38982.704931.AE
2. Claussnitzer M, Cho JH, Collins R, et al. A brief history of human disease genetics. Nat Res. 2020;577:179–189. doi:10.1038/s41586-019-1879-7
3. Alsaeed ES, Farhat GN, Assiri AM, et al. Distribution of hemoglobinopathy disorders in Saudi Arabia based on data from the premarital screening and genetic counseling program, 2011–2015. J Epidemiol Glob Health. 2018;7:S41–7. doi:10.1016/j.jegh.2017.12.001
4. Memish ZA, Owaidah TM, Saeedi MY. Marked regional variations in the prevalence of sickle cell disease and β-thalassemia in Saudi Arabia: findings from the premarital screening and genetic counseling program. J Epidemiol Glob Health. 2011;1(1):61–68. doi:10.1016/j.jegh.2011.06.002
5. Adam SS, Flahiff CM, Kamble S, Telen MJ, Reed SD, de Castro LM. Depression, quality of life, and medical resource utilization in sickle cell disease. Blood Adv. 2017;1(23):1983–1991. doi:10.1182/bloodadvances.2017006940
6. Tran H, Gupta M, Gupta K Targeting novel mechanisms of pain in sickle cell disease; 2017. Available from: http://ashpublications.org/blood/article-pdf/130/22/2377/1403522/blood782003.pdf.
7. Jastaniah W. Epidemiology of sickle cell disease in Saudi Arabia. Ann Saudi Med. 2011;31:289–293. doi:10.4103/0256-4947.81540
8. Piccin A, Fleming P, Eakins E, McGovern E, Smith OP, McMahon C. Sickle cell disease and dental treatment. J Ir Dent Assoc. 2008;54(2):75–79.
9. Budreviciute A, Damiati S, Sabir DK, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.574111
10. Meyer BF. Strategies for the prevention of hereditary diseases in a highly consanguineous population. Ann Hum Biol. 2005;32:174–179. doi:10.1080/03014460500075217
11. Alsalman M, Alkhalifa H, Alkhalifa A, et al. Hydroxyurea usage awareness among patients with sickle-cell disease in Saudi Arabia. Health Sci Rep. 2021;4:4. doi:10.1002/hsr2.437
12. Piccin A, Murphy C, Eakins E, et al. Insight into the complex pathophysiology of sickle cell anaemia and possible treatment. Eur J Haematol. 2019;102(4):319–330. doi:10.1111/ejh.13212
13. Yawn BP, Buchanan GR, Afenyi-A Nnan AN, et al. Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312(10):1033–1048. doi:10.1001/jama.2014.10517
14. Jagadeeswaran R, Rivers A. Evolving treatment paradigms in sickle cell disease. Hematology. 2017;2017(1):440–446. doi:10.1182/asheducation-2017.1.440
15. Booth A, Bonham V, Porteus M, Ormond KE. Treatment decision-making in sickle cell disease patients. J Community Genet. 2022;13(1):143–151. doi:10.1007/s12687-021-00562-z
16. Kauf TL, Coates TD, Huazhi L, Mody-Patel N, Hartzema AG. The cost of health care for children and adults with sickle cell disease. Am J Hematol. 2009;84(6):323–327. doi:10.1002/ajh.21408
17. Bin Zuair A, Aldossari S, Alhumaidi R, Alrabiah M, Alshabanat A. The burden of sickle cell disease in Saudi Arabia: a single-institution large retrospective study. Int J Gen Med. 2023;13(16):161–171. doi:10.2147/IJGM.S393233
18. Schultz CL, Tchume-Johnson T, Jackson T, Enninful-Eghan H, Schapira MM, Smith-Whitley K. Reproductive intentions in mothers of young children with sickle cell disease. Pediatr Blood Cancer. 2020;67:5. doi:10.1002/pbc.28227
19. AlHamdan NAR, AlMazrou YY, AlSwaidi FM, Choudhry AJ. Premarital screening for thalassemia and sickle cell disease in Saudi Arabia. Genet Med. 2007;9(6):372–377. doi:10.1097/GIM.0b013e318065a9e8
20. Treadwell MJ, Mcclough L, Vichinsky E. Using qualitative and quantitative strategies to evaluate knowledge and perceptions about sickle cell disease and sickle cell trait. J Natl Med Assoc. 2006;98:704–710.
21. Long KA, Thomas SB, Grubs RE, Gettig EA, Krishnamurti L. Attitudes and beliefs of African-Americans toward genetics, genetic testing, and sickle cell disease education and awareness. J Genet Couns. 2011;20(6):572–592. doi:10.1007/s10897-011-9388-3
22. Sullivan-Pyke CS, Senapati S, Mainigi MA, Barnhart KT. In vitro fertilization and adverse obstetric and perinatal outcomes. Semin Perinatol. 2017;41(6):345–353.
23. Collins SC, Xu X, Mak W. Cost-effectiveness of preimplantation genetic screening for women older than 37 undergoing in vitro fertilization. J Assist Reprod Genet. 2017;34(11):1515–1522. doi:10.1007/s10815-017-1001-8
24. Oyewo A, Salubi-Udu J, Khalaf Y, et al. Preimplantation genetic diagnosis for the prevention of sickle cell disease: current trends and barriers to uptake in a London teaching hospital. Hum Fertil. 2009;12(3):153–159. doi:10.1080/14647270903037751
25. Almaslami F, Aljunid SM. Cost-effectiveness of assisted reproductive technologies in Saudi Arabia: comparing in vitro fertilization with intrauterine insemination. SAGE Open Med. 2020;13(8):2050312120931988.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.