Back to Journals » Orthopedic Research and Reviews » Volume 14
Short versus Long-Leg Hip Spica After Closed Reduction in Developmental Dysplasia of the Hip: A Retrospective Comparative Study
Authors Yasin MS, Alisi MS ![]() , Hammad YS
, Hammad YS ![]() , Samarah OQ, Abu Hassan FO
, Samarah OQ, Abu Hassan FO ![]()
Received 11 December 2021
Accepted for publication 15 March 2022
Published 24 March 2022 Volume 2022:14 Pages 71—76
DOI https://doi.org/10.2147/ORR.S353279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Mohamad S Yasin, Mohammed S Alisi, Yazan S Hammad, Omar Q Samarah, Freih O Abu Hassan
Department of Special Surgery, Division of Orthopaedics, School of Medicine, The University of Jordan, Amman, Jordan
Correspondence: Mohamad S Yasin, Department of Special Surgery, Division of Orthopedics, School of Medicine, The University of Jordan, Amman, Jordan, Email [email protected]
Purpose: Closed reduction (CR) is a standard treatment for developmental dysplasia of the hip (DDH) after failed conservative treatment. After CR, the affected hip is held in the reduced position by a spica cast that typically extends below the knee (long). Above knee (short) spica cast is an alternative technique utilized by some pediatric orthopedic surgeons. We aimed to compare short versus long spica cast after CR in terms of success rate and complications.
Methods: Patients who underwent CR with short or long hip spica cast over a 3-year period (2016– 2019) were evaluated for the success (sustainability of the reduction) and complications. The acute and long-term success were recorded retrospectively. Acute success was defined as concentric reduction of the hip confirmed by intraoperative arthrogram and immediate postoperative CT scan. Long-term success was defined as maintained reduction at 12 months’ post reduction.
Results: Forty-seven patients were included in our study. Long spica casts were used in 24 patients and short ones in the remaining 23. The overall acute and long-term success rates were 83% and 66%, respectively. The acute success rate of long spica was 87.5%, while short spica achieved 78.2%. On the long term, the success rate of short spica was higher than long one (73.9% vs 58.3%). Cox regression analysis showed that the type of cast (short vs long spica) was not correlated with acute success (P = 0.405), long-term success (P = 0.263), residual dysplasia (P = 0.405), or avascular necrosis (P = 0.053).
Conclusion: CR in DDH is an important line of management in the younger patient population and can save them an invasive open surgery later in life. A short leg spica could represent an easier and likely as successful alternative to the traditional long spica. More prospective future research is needed to validate our observational findings.
Level of Evidence: III.
Keywords: DDH, spica cast, closed reduction, hip, dysplasia
Corrigendum for this paper has been published
Introduction
A wide spectrum of hip abnormalities and malformations are included under the all-encompassing umbrella named Developmental Dysplasia of the Hip (DDH). These malformations include laxity within the acetabulum, hip subluxation and dislocation, and acetabular dysplasia.1 DDH is an important cause of childhood disability, as well as the underlying disorder for total hip replacement in up to 29% of patients under 60 years of age.1 Advances in imaging techniques, as well as the increase of routine ultrasounds for the screening of DDH in several countries resulted in earlier diagnosis. With early diagnosis, the success rate of DDH treatment is extremely high with simple cost-effective and safe techniques.2 However, in children diagnosed with DDH after the age of 6 months, or in those in whom bracing has failed to achieve satisfactory concentric reduction, closed reduction with application of a spica cast remains the preferred treatment.3 Success rate for closed reduction in the literature is variable ranging from 57% to 91%.4,5 The most feared complications of closed reduction include re-dislocation and avascular necrosis, however others like cast breakage/loosening and nerve palsy exist.
A typical hip spica, as described by Kumar, extends from the lower thoracic cage to below the knee with the hip in 90–100 degrees of flexion and no more than 50 degrees of abduction.6 Few degrees of internal rotation are preferred by most surgeons. There are no previous reports in the literature on using a short form of a hip spica. Our technique utilizes the same typical human position for the hip while sparing the knee. It involves less intra-operative manipulation while applying the cast with a more secure holding position.
The purpose of this study is to compare between two techniques of spica casting (short versus long) and examine the success and complication rates for each.
Methods
A retrospective study was conducted at an academic hospital and included all patients who were diagnosed with DDH between January 1st, 2016 and January 1st, 2019. A Common practice in our country is to obtain a pelvic radiograph for DDH screening after the age of 4 months for all children who were never properly screened previously as the pathology is relatively common.
Radiologically we used the Tonnis classification and the International Hip Dysplasia Institute (IHDI) classification in case the ossific nucleus was not apparent yet.7 Patients with Tonnis I–II and IHDI I–II were excluded as they were all successfully treated with bracing.
Closed reduction was typically performed by two of the hospital’s pediatric orthopedic surgeons, one of whom uses long spica casting and the other short spica casting. The surgeons’ preference with the spica technique was based on their training. Adding to that, the surgeon who used short spicas believed that a short spica was technically easier and it simulates bracing where the knee moves freely. On the other hand, the surgeon who used the long spica believed that rotation was better controlled as well as relaxing the tight hamstring with knee flexion helps protect reduction.
Hip spica position was standardized with an average of 90–100 degrees’ flexion and 50–55 degrees of abduction. A limited-cut postoperative CT scan was done for all patients on the same day of their procedure to confirm axial reduction. The spica was exchanged typically at the 6-week mark for all patients with a total of 12 weeks of spica casting. After removal of the second spica, an abduction brace was used for a period of 6 weeks in all patients, after which no formal immobilization was used.
Acute success is defined as a concentric reduction of the hip based on adequate arthrographic findings (everted labrum and medial dye pool <5mm) in addition to confirmed concentric reduction on postoperative limited-cut CT scan. When the reductions were deemed unsuccessful acutely two approaches were generally followed. The surgeon applying the short spica preferred to proceed with medial open reduction without delay, and the long spica surgeon preferred to wait until after 1 year of age for an anterior open reduction, this variation was based on their previous training.
Long-term success is defined as Tonnis/IHDI grade I, with an X-ray taken in 15–20 degrees abduction and internal rotation to unmask any anteversion that could result in pseudo-subluxation, with a follow-up for at least 12 months. The acetabular index was not taken into consideration as residual dysplasia is common after hip reduction in DDH, and it is not the primary measure in our study. Having said that, residual dysplasia was defined as an acetabular index >30 degrees at the age of 1 year upon follow-up.
Kalamchi and MacEwen’s classification of avascular necrosis of the hip was used. Grades II–IV were defined as AVN and follow-up X-ray’s were taken at 6 weeks, 12 weeks, 3 months, 6 months and 1 year after spica removal before ruling out AVN.
Retrospectively, we recorded patients’ demographic information (age at diagnosis, gender, mode of delivery, birth presentation, family history), side of operation, type of spica, acute and long-term success, and complications (avascular necrosis and residual dysplasia).
Univariable and multivariable logistic regression hazard models were performed to evaluate the association of the subject’s data with the success of the different casting methods. Statistical significance was set at P < 0.05, and analysis was performed using STATA v.14.1 (StataCorp LP, College Station, TX).
Informed consent was obtained from all families of patients included in the study.
Results
Of the 1146 patients diagnosed with DDH, 114 patients had grade III–IV on Tonnis and IHDI classifications. Bracing was initiated in those 4–6 months of age and was successful in 67 patients with a total duration of treatment (12–24 weeks), with the goal of having a Tonnis/IHDI I. Forty-seven patients failed bracing or were >6 months of age and needed closed reduction with arthrogram under general anesthesia.
Forty-seven patients were included in this study. Of those, 43 (91.5%) were females and the median age of patients was 7.83 months (range 5–11 months).
Nineteen of the patients (40.4%) had bilateral disease. Twenty-three (49.9%) underwent treatment with a short spica cast, while 24 (51.1%) had long spica casting.
The overall acute success rate was 83%, while the long-term success rate achieved 66%. Every case deemed not acutely successful was included as also not achieving long-term success. Those deemed not successful acutely were as mentioned previously treated with open reduction.
The details of patient’s characteristics, acute and long-term success rate, and complication rate for each group (short vs long spica cast) are demonstrated in [Tables 1 and 2].
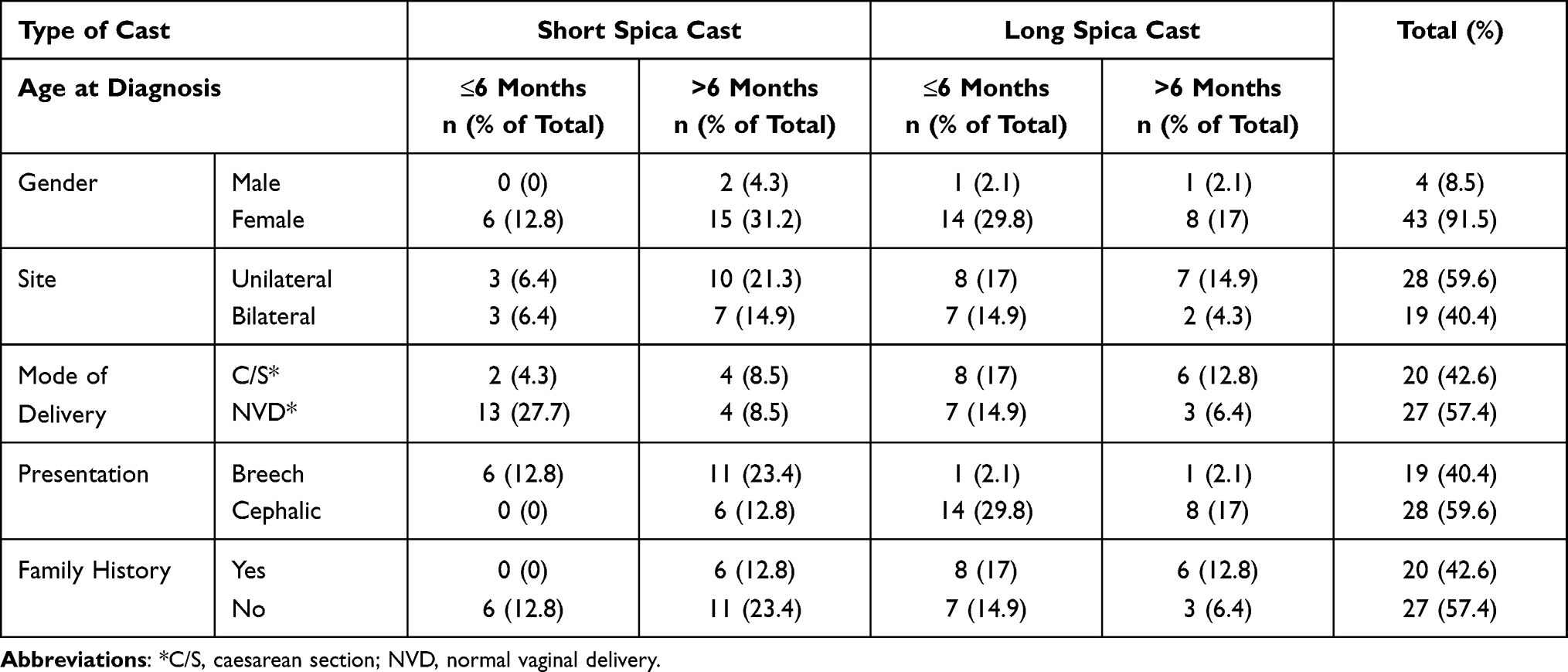 |
Table 1 Site and Characteristics of Patients Who Underwent Closed Reduction for DDH |
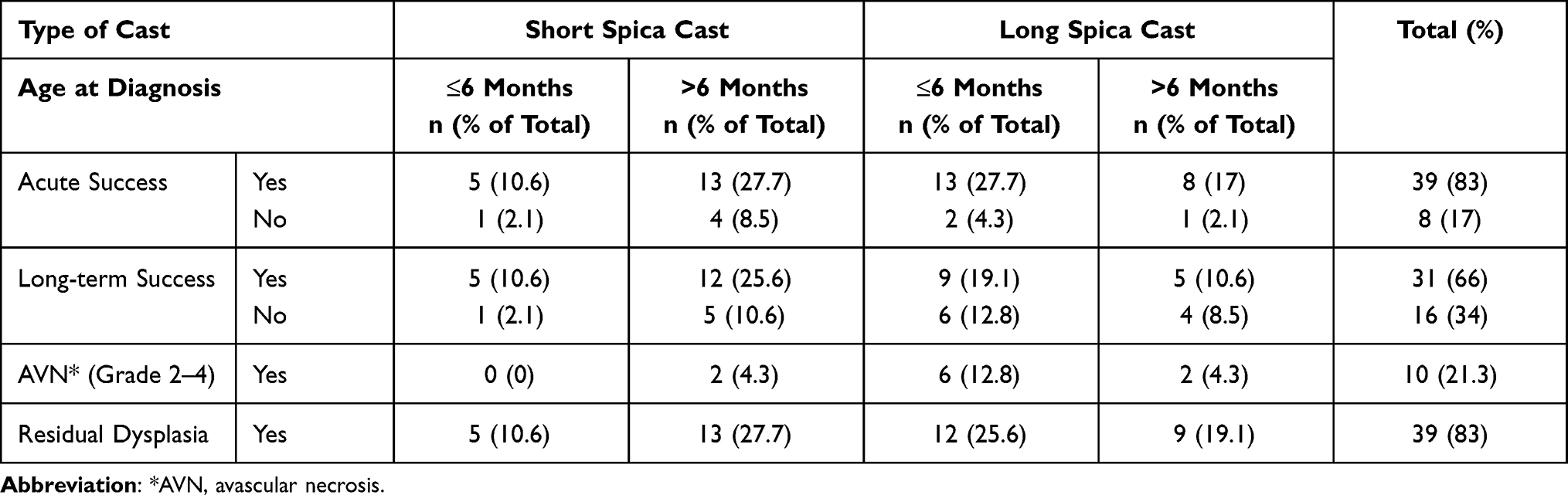 |
Table 2 Success Rates and Complications of Patients Who Underwent Closed Reduction for DDH |
Cox regression analysis for the collected data showed that the type of cast (short vs long spica) was not correlated with acute success, long-term success, residual dysplasia, or avascular necrosis [Table 3].
 |
Table 3 Univariable Logistic Regression to Demonstrate the Correlation Between the Type of Casting Used (Short vs Long) and the Patients Outcome |
Discussion
Recent studies have indicated that the success of closed reduction in patients with failed bracing is low due to the intrinsic and extrinsic obstructing factors responsible for failure of bracing.8 Therefore, the success rate of closed reduction for DDH varies markedly depending on how success is defined, and the most important factor in the success of closed reduction may be age at the initiation of treatment.3 The criteria for accepting arthrography guided closed reduction are stable concentric reduction, L distance (measurement of lateralization) of 4 mm or less, and a non-inverted labrum .9
The typical spica, as described by Kumar et al,6 extends below the knee with the aim of providing rotational stability and possibly preventing the tight hamstrings from exerting destabilizing forces on the reduced hips. It is recommended that abduction in spica casts be limited to less than 50° in children less than or equal to 6 months of age.10 At our institution, the pediatric orthopedic surgeons are divided when it comes to their hip spica. One of them applies the below knee and the other uses an above knee hip spica, both utilizing the same amount of hip abduction (45–55 degrees) and flexion (90–100 degrees) with an added percutaneous adductor tenotomy, as needed. The latter surgeon believes that the success of the short-legged spica is related to the molding of the cast as well as concentricity of the hip as assessed intra-operatively.
Although closed reduction and spica cast application remain an effective and successful treatment option for many patients with DDH, there is a significant rate of early re-dislocation in the older child.10 Also, the development of AVN following a closed reduction procedure can be problematic, with an incidence of 35%.11
The success rate for CR of the hip in the literature varies and changes according to the Tonnis stage, age at time of procedure, previous treatment by other methods, and surgeon experience.12–14 In general, our results showed overall success rate similar to previous reports in the literature.4,5,15,16
In this study, we found that the success rate of the short spica cast is close to that of the long spica with an average overall acute success rate of 83% (78.2% in short spica vs 87.5% in long spica) and average overall long-term success rate of 66% (73.9% in short spica vs 58.3% in long spica). Despite the variation, no statistical significance could be recorded. Bilateral involvement was not well correlated with the success of reduction. The known risk factors for DDH (sex, family history, rank, breech presentation) did not have a significant influence when it came to the choice of spica. There was no specific correlation between these factors and the success of reduction in the literature.
The advantages of short spica include less additional weight to the child and maintaining range of motion of the joints below the hip. These advantages will allow easy handling and manipulation of the child by the family especially in bilateral cases.
The limitations of this study include its retrospective nature and limited number of patients. The low number of patients can be explained by the narrow window of age for choosing closed reduction as treatment for hip dislocation in DDH. Our local guidelines recommend CR for patients who failed Pavlik harness before 6 months of age or those who presented between 6 and 18 months of age.
We are aware that the sample size is small, and conclusions are difficult to be obtained; however, as per our knowledge, no previous studies have looked at this question before and providing that the results of this study show no correlation between the type of cast (short vs long spica) and the success or complication rates, short hip spicas could represent an alternative, technically easier option for use after CR for DDH. Having said that, we know that more prospective randomized work is needed to see if a short spica would become a globally accepted substitute for a traditional long hip spica.
Conclusion
Closed reduction in DDH is an important line of management in the younger patient population and can save them an invasive open surgery later in life. We believe that if a well-molded above knee cast (short spica) is applied for those hips that feel concentrically reduced intraoperatively, the success rate may not be any lower than the traditional long spica. A short leg spica could represent an easier and likely as successful alternative to the traditional long spica. More prospective future research is needed to validate our observational findings.
Compliance with Ethical Standards
We certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study has been approved by the institutional review board at Jordan University Hospital. All patients/families had signed a written consent to use their data for publication in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vaquero-Picado A, González-Morán G, Garay EG, Moraleda L. Developmental dysplasia of the hip: update of management. EFORT Open Rev. 2019;4(9):548–556. doi:10.1302/2058-5241.4.180019
2. Thomas SR. A review of long-term outcomes for late presenting developmental hip dysplasia. Bone Joint J. 2015;97-B(6):729–733. doi:10.1302/0301-620X.97B6.35395
3. Murray T, Cooperman DR, Thompson GH, Ballock RT. Closed reduction for treatment of developmental dysplasia of the hip in children. Am J Orthop. 2007;36(2):82–84.
4. Tennant SJ, Hashemi-Nejad A, Calder P, Eastwood DM. Bilateral developmental dysplasia of the hip: does closed reduction have a role in management? Outcome of closed and open reduction in 92 hips. J Pediatr Orthop. 2019;39(4):e264–e271. doi:10.1097/BPO.0000000000001297
5. Sankar WN, Gornitzky AL, Clarke NMP, et al. Closed reduction for developmental dysplasia of the hip: early-term results from a prospective, multicenter cohort. J Pediatr Orthop. 2019;39(3):111–118. doi:10.1097/BPO.0000000000000895
6. Kumar SJ. Hip spica application for the treatment of congenital dislocation of the hip. J Pediatr Orthop. 1981;1(1):97–99. doi:10.1097/01241398-198101010-00014
7. Narayanan U, Mulpuri K, Sankar WN, et al. Reliability of a new radiographic classification for developmental dysplasia of the hip. J Pediatr Orthop. 2015;35(5):478–484. doi:10.1097/BPO.0000000000000318
8. Iqbal HJ, Srivastava P, Davies R, Saville S, Bruce C, Garg N. Is closed reduction of DDH successful after failed Pavlik harness treatment? Orthop Proc. 2018;96-B:17.
9. Khoshhal KI, Kremli MK, Zamzam MM, Akod OM, Elofi OA. The role of arthrography-guided closed reduction in minimizing the incidence of avascular necrosis in developmental dysplasia of the hip. J Pediatr Orthop B. 2005;14(4):256–261. doi:10.1097/01202412-200507000-00004
10. Schur MD, Lee C, Arkader A, Catalano A, Choi PD. Risk factors for avascular necrosis after closed reduction for developmental dysplasia of the hip. J Child Orthop. 2016;10(3):185–192. doi:10.1007/s11832-016-0743-7
11. Kothari A, Goulios V, Buckingham R, Wainwright A, Theologis T. Early failure following closed reduction for developmental dysplasia of the hip. Orthop Proc. 2018;94-B:3.
12. Bhaskar A, Desai H, Jain G. Risk factors for early redislocation after primary treatment of developmental dysplasia of the hip: is there a protective influence of the ossific nucleus? Indian J Orthop. 2016;50(5):479–485. doi:10.4103/0019-5413.189610
13. Bian Z, Guo Y, Tian W. [Treatment of developmental dysplasia of the hip in children: results of closed reduction and immobilization in hip spica cast]. Chin J Surg. 2009;47(13):1017–1019. Chinese.
14. Aksoy MC. Gelişimsel kalça displazisi tedavisinde kapali redüksiyon [Closed reduction in the treatment of developmental dysplasia of the hip]. Acta Orthop Traumatol Turc. 2007;41(Suppl 1):25–30.
15. Li Y, Zhou Q, Liu Y, et al. Closed reduction and dynamic cast immobilization in patients with developmental dysplasia of the hip between 6 and 24 months of age. Eur J Orthop Surg Traumatol. 2019;29(1):51–57. doi:10.1007/s00590-018-2289-5
16. Aksoy MC, Ozkoç G, Alanay A, Yazici M, Ozdemir N, Surat A. Treatment of developmental dysplasia of the hip before walking: results of closed reduction and immobilization in hip spica cast. Turk J Pediatr. 2002;44(2):122–127.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.