Back to Journals » Clinical Ophthalmology » Volume 15
Short-Term Use of Dexamethasone/Netilmicin Fixed Combination in Controlling Ocular Inflammation After Uncomplicated Cataract Surgery
Authors Caporossi A, Alessio G ![]() , Fasce F, Marchini G
, Fasce F, Marchini G ![]() , Rapisarda A
, Rapisarda A ![]() , Papa V
, Papa V ![]()
Received 14 April 2021
Accepted for publication 4 June 2021
Published 30 June 2021 Volume 2021:15 Pages 2847—2854
DOI https://doi.org/10.2147/OPTH.S311846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Aldo Caporossi,1 Giovanni Alessio,2 Francesco Fasce,3 Giorgio Marchini,4 Antonio Rapisarda,5 Vincenzo Papa6
1Department of Ophthalmology, Policlinico Universitario A. Gemelli IRCSS Università Cattolica del Sacro Cuore, Roma, Italy; 2Ophthalmology Unit, Dipartimento di Scienze mediche di base, Neuroscienze e Organi di Senso Università di Bari, Azienda Ospedaliera Policlinico Consorziale, Bari, Italy; 3Ophthalmology Unit, IRCSS San Raffaele, Milano, Italy; 4Ophthalmology Unit, Ospedale Policlinico G.B. Rossi, Università di Verona, Verona, Italy; 5Ophthalmology Unit, Azienda Ospedaliera Garibaldi, Catania, Italy; 6Medical Affairs SIFI SpA, Catania, Italy
Correspondence: Vincenzo Papa
Medical Affairs SIFI SpA, Via E. Patti 36, Aci S. Antonio, Catania, Italy
Email [email protected]
Purpose: To evaluate the short-term anti-inflammatory effect of dexamethasone/netilmicin fixed combination in the management of ocular inflammation after cataract surgery.
Patients and Methods: Open-label, randomized, active-controlled, clinical study conducted in 6 sites in Italy; 238 patients were randomized 2:1 to dexamethasone/netilmicin (dexa/net, n=158) or betamethasone/chloramphenicol (beta/chl, n=80). Treatment started the day of surgery and continued 4 times daily for 7 days. The primary efficacy parameter was the anterior chamber (AC) flare. The percentage of patients displaying none or mild (ie, only barely detectable) AC flare was defined as “efficacy rate”, whereas the percentage of patients showing a decrease of AC flare score from baseline was defined as “percentage of responders”. Additional parameters evaluated were AC cells, conjunctival hyperaemia, corneal and lid oedema, symptoms of ocular discomfort, visual acuity, and intraocular pressure. Dexa/net was considered effective if the efficacy rate was not inferior (by means of 97.5% confidence interval) to that of beta/chl.
Results: After 7 days of treatment, no AC flare was observed in 92.8% (dexa/net) and 92.3% (beta/chl) of patients, whereas no AC cells were observed in 91.5% (dexa/net) and 93.6% (beta/chl) of patients, respectively. The “efficacy rate” was 100% in both groups, whereas the “percentage of responders” was 94.1% in the dexa/net and 93.6% in the beta/chl group. The p-value to reject the null hypothesis of inferiority was < 0.001. Other efficacy parameters confirmed both treatments as highly effective, despite their difference in steroid content (2 mg/mL for beta/chl vs 1 mg/mL for dexa/net). IOP and visual acuity at the end of the study were comparable. Two cases of allergic conjunctivitis were considered adverse events and were both related to dexa/net.
Conclusion: Short-term use of dexa/net fixed combination is safe and effective in the control of post-operative inflammation following uncomplicated cataract surgery.
Keywords: cataract surgery, fixed combination, netilmicin, chloramphenicol
Introduction
Cataract surgery the most common surgical medical procedure performed annually across the European Union states in approximately 5 million individuals.1 After cataract extraction, a varying degree of post-surgical inflammation may occur. Although such inflammation is, in most cases, self-limited, the use of anti-inflammatory agents can rapidly resolve it and prevents serious complications resulting from uncontrolled inflammations (as cystoid macular edema).2 Accordingly, the use of topical corticosteroids and/or non-steroidal anti-inflammatory drugs remains the mainstay of post-surgical management of these patients. A recent study funded by the European Society of Cataract and Refractive Surgeons (ESCRS) showed that a combination of a non-steroidal anti-inflammatory drugs and dexamethasone reduces the risk for developing cystoid macular oedema after cataract surgery.3 Apart ocular inflammation, endophthalmitis is the most important complication of cataract surgery. Its severity depends on the virulence and the quantity of inoculated pathogens. Coagulase-negative Staphylococci and S. Aureus are the most common pathogens isolated in this infection.4 Moreover, during the past decade a major concern was related to the high prevalence of infections due to methicillin-resistant S. Aureus (MRSA) and methicillin-resistant Coagulase-negative Staphylococci (MRCoNS). A preoperative antisepsis of the periocular area with topical povidone–iodine and the use of intracameral cefuroxime are actually considered the standard for endophthalmitis prophylaxis.5,6 However, cefuroxime is not effective versus methicillin-resistant strains.4 The use of post-operative topical antibiotics is controversial, but they are frequently used in the real life to sterilize the ocular surface and prevent any access of microorganisms inside the eye.6,7 Topical antibiotics can be administered either alone or in combination with corticosteroids. Steroid/antibiotic fixed combinations have several advantages over the use of single components, as better compliance, lower costs, and reduction of the potential wash-out effect.8 The choice among different products depends on the bacterial susceptibility to the antibiotic and the type and strength of the steroid included in the formulation. A steroid/antibiotic fixed combination containing 1 mg/mL dexamethasone and 3 mg/mL netilmicin is available in several EU and non-EU countries under the trade name of Netildex (SIFI SpA, Italy) and exhibits a fast and effective control of ocular inflammation, either post-operative or not.8–10 Since the use of dexamethasone after cataract surgery is established,11 the product’s added value is the presence of netilmicin, a wide spectrum antibiotic also covering methicillin-resistant strains ensuring a complete sterilization of the ocular surface in the immediate post-surgery period.12–14 In this study, a short treatment with such steroid-antibiotic combination was tested in patients who underwent to uncomplicated cataract surgery.
Patients and Methods
Trial Design
This was a multicenter, open, randomized, active-controlled, parallel group, Phase IV clinical study conducted in 6 sites in Italy at Bari, Milano Verona, Catania, and Rome (2 centres). The main objective of the study was to evaluate the effectiveness of 1 mg/mL dexamethasone plus 3 mg/mL netilmicin (dexa/net) ophthalmic solution treatment for 7 days in the control and treatment of post-surgical ocular inflammation following cataract surgery. A control group of patients was treated with 2 mg/mL betamethasone plus 5 mg/mL chloramphenicol (beta/chl) eye suspension. The study protocol was approved by the institutional review board at each research center. All participants provided written informed consent and the study was conducted according to the Declaration of Helsinki and Good Clinical Practice guidelines. The trial is registered at the European Union Clinical Trials Register (EudraCT) no. 200600330513.
Participants
Any subject older than 40 years, able to give an informed consent and scheduled for having micro-incisional cataract surgery was eligible for the study. Subjects were considered not eligible if they had: 1) history of ocular inflammatory diseases, ocular herpes infection, iritis, uveitis or Sjogren’s syndrome, 2) concomitant ocular pathologies, 3) intraocular pressure >24 mmHg; 4) previous ocular surgery in the affected eye in the previous 12 months; 5) previous laser treatment in the affected eye in the previous 6 months; 5) use of any ocular medication within 14 days prior to study entry; 6) any ocular infection within month prior to study entry; 7) known or suspected allergy to ophthalmic preservatives, aminoglycosides and steroids. Two hundred thirty-eight consecutive patients (116 males and 122 females) were screened and enrolled. Mean age was 72 years (range 42–90 years). Age and gender were well-matched among groups of treatment. Patients disposition, according to the CONSORT diagram, is displayed in Figure 1.
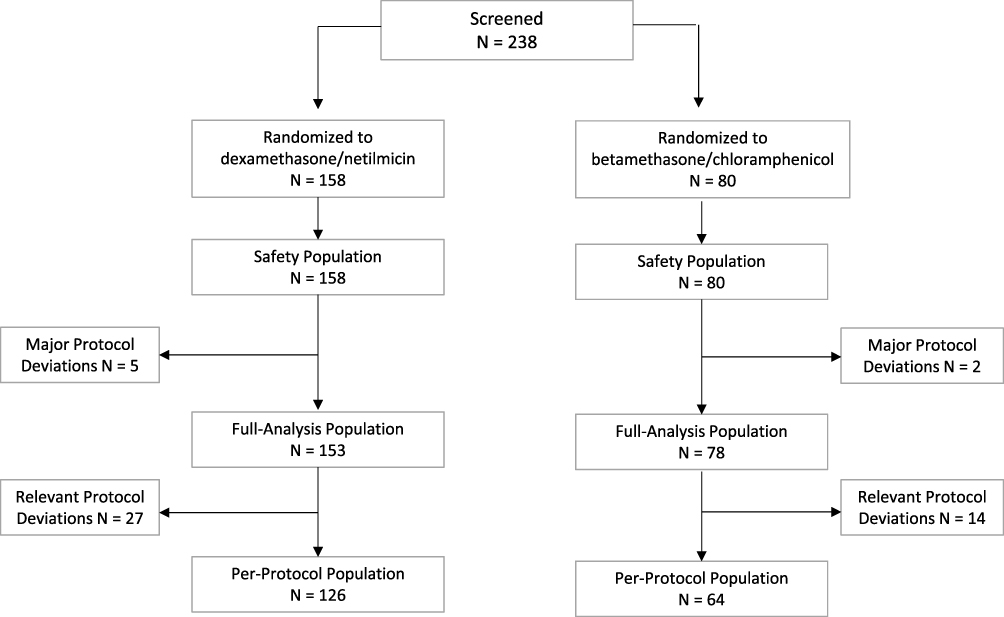 |
Figure 1 Patients disposition. |
Interventions
Two hundred and thirty-eight patients were randomized, using a computer-generated list, in a 2:1 ratio to dexa/net (n=158) or beta/chl (n=80). The different packaging of two products did not allow a double-masked approach. Treatment started the day of surgery (day 0) administering 1 drop in the conjunctival sac of the operated eye and continued 4 times a day for 7±1 day. Afterwards investigators could continue the anti-inflammatory treatment according to patient conditions and their clinical routine. Control visits were scheduled at day 1 and day 7 (±1) after surgery.
Outcomes
The examination at each visit included best corrected visual acuity, slit-lamp examination, ophthalmoscopy and applanation tonometry. The primary efficacy parameter evaluated was the anterior chamber (AC) flare scored from none to severe using a 0 to 3-point scale (Table 1).15 Other parameters of analysed included: AC cells, conjunctival hyperaemia, corneal and lid oedema, and symptoms of ocular discomfort (pain, burning, and tearing). All these clinical variables were also graded from none to severe using a 0 to 3-point scale (Table 1).15 Safety variables monitored during the study were adverse events, intraocular pressure (IOP), and visual acuity.
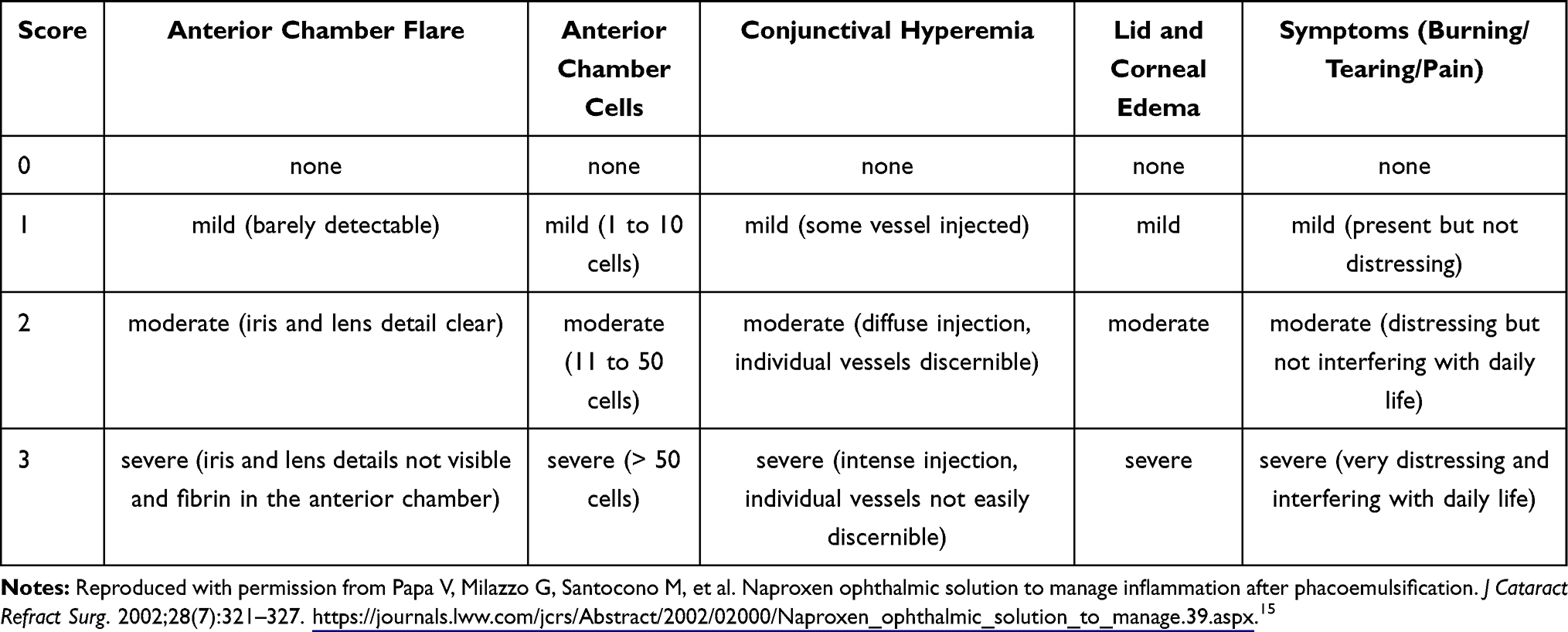 |
Table 1 Scoring Systems Used in the Study |
Statistics
Statistical analysis was performed by an expert statistician using the SAS system version 9.2. The sample size estimate was based on a one-sided test of equality of paired proportions of the primary end point. This was estimated to be 96% in the control group treated with dexamethasone for 10 days. Considering that in this trial treatment duration was 7±1 day, the estimated percentage of patients with AC flares was reduced to 90%. Based on this assumption, 219 evaluable patients were required to detect at 15% difference between treatments to have a 90% chance (delta = 10%) of statistically proving efficacy, in a non-inferiority design study. To allow for about 10% subjects drop-out, a final sample size of 238 patients was planned. Statistical evaluation was performed as previously described for similar studies.8,15, Listing, tables, graphs, and statistical output were generated using the SAS software. Briefly, the main efficacy parameter evaluated was AC flare at day 7 after surgery. The “efficacy rate” (primary efficacy parameter) was defined as the percentage of patients displaying none or mild AC flare (ie, score 0 or 1), whereas the “percentage of responders” (secondary efficacy parameter) was defined as the percentage of patients showing a decrease of AC flare score from baseline and patients scoring 0 at both baseline and at Day 7 after surgery. Dexa/net would be declared effective, if it can be shown that the response rate is not inferior (by means of 97.5% confidence interval) to that of beta/chl. Statistical analyses were performed on predefined subsets. The Full Analysis Population (FA) consisted of subjects operated and treated for at least 5 days and that reached the end point visit (Day 7 after surgery). The Per-Protocol (PP) Population consisted of all subjects of the FA population without any relevant protocol deviations. The main efficacy parameters (“efficacy rate” and “percent of responders”) were analysed in both FA and PP populations, whereas all other parameters were analysed in the FA population only. Safety was analysed in all subjects who received at least one dose of drug [Intention-to-Treat (ITT) population]. For other efficacy parameters, intraindividual score differences were calculated, assuming a zero difference if the respective post-dose values were not available. These score differences were compared between treatments by the Mann–Whitney U-test or the Wilcoxon test for independent samples. All secondary efficacy parameters were presented by descriptive analysis. All safety results are presented with their descriptive analyses only. Adverse events (AEs) were coded using the MedDRA dictionary (version 14).
Results
As shown in Figure 1, the ITT population consisted of 238 patients (dexa/net=158 and beta/chl=80). Seven patients were excluded due to a protocol violation and therefore the FA population consisted of 231 patients (dexa/net=153 and beta/chl=78); the PP population included 190 patients fully adherent to the protocol (dexa/net=126 and beta/chl=64). Patients were well-matched among groups regarding baseline characteristics.
Main efficacy results are displayed in Tables 2 and 3. After 7 days of treatment most of patients had no signs of inflammation in the anterior chamber. The main efficacy parameters (“efficacy rate” and “percentage of responders”) were comparable between groups. The p-value to reject the null hypothesis of inferiority was p<0.001 (Table 2). Specifically, at the end point visit no AC flare was observed in 92.8% of patients treated with dexa/net and 92.3% of patients treated with beta/chl. In addition, no AC cell was detected in 92.8% of patients treated with dexa/net and 92.3% of patients treated with beta/chl (Table 3). Furthermore, all additional efficacy parameters evaluated (conjunctival hyperaemia, corneal oedema, and lid oedema) confirmed that both treatments were equally effective in reducing ocular inflammation (Table 3). Same conclusion can be draw also for ocular symptoms (tearing, burning and pain) (Table 4).
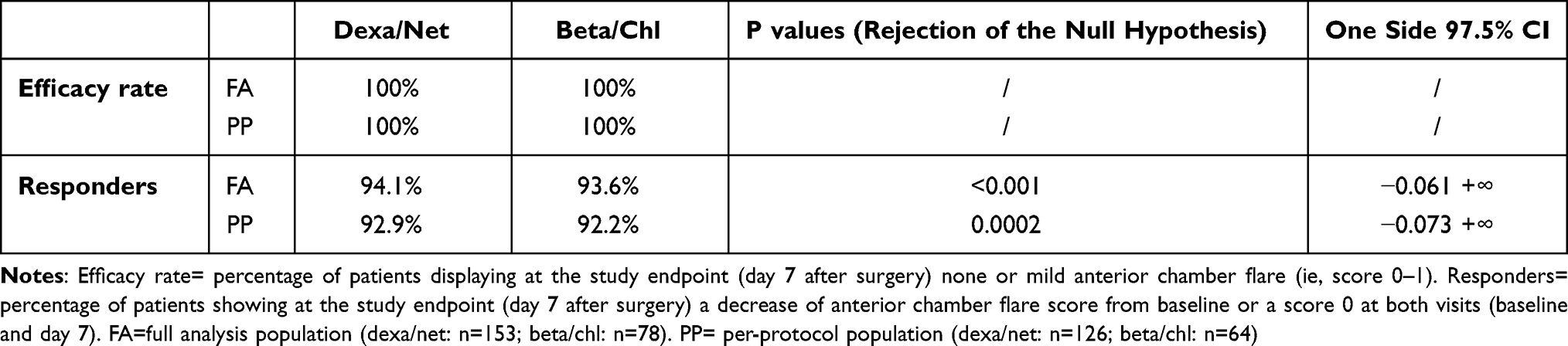 |
Table 2 Primary Efficacy Outcomes |
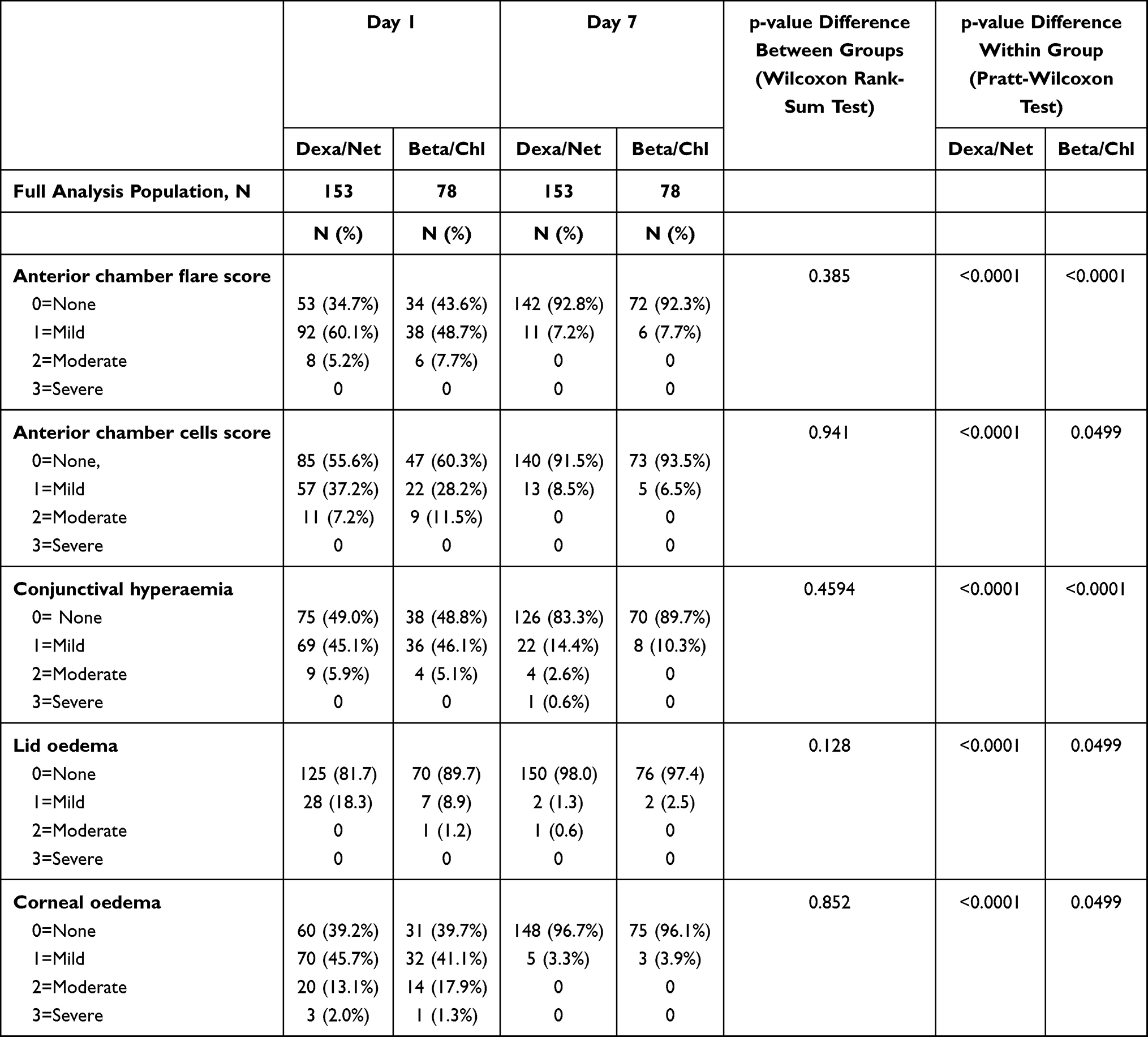 |
Table 3 Additional Efficacy Outcomes |
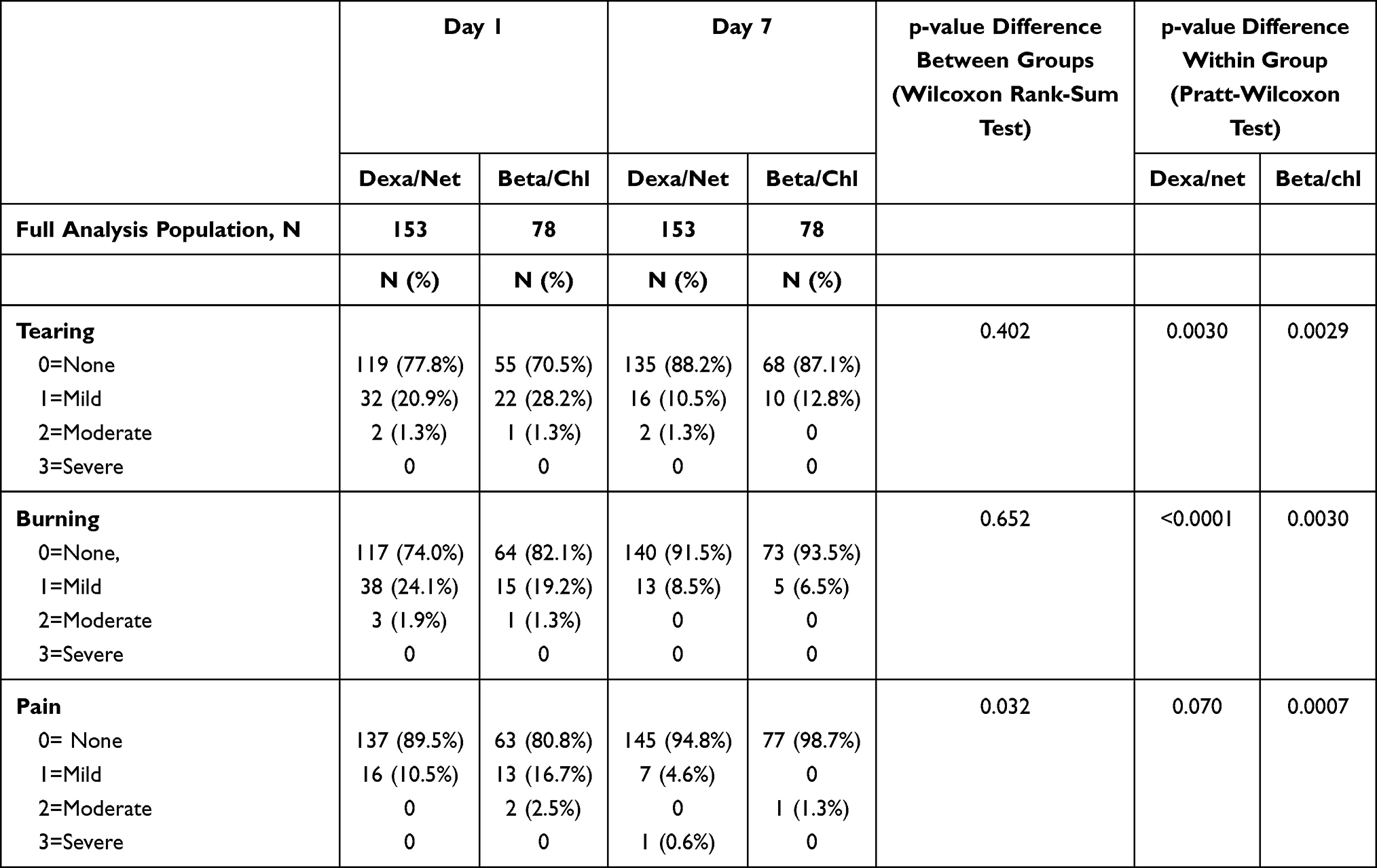 |
Table 4 Ocular Symptoms |
During the study, non-serious AEs occurred in 2.1% of patients (5/238). These AEs occurred in the group treated with dexa/net. Three events (subconjunctival hemorrhage, retinal hemorrhage, and capsular rupture) were considered not related to treatment but to the surgical procedure, whereas two cases of allergic conjunctivitis were considered related to the use of dexa/net. Final IOP was 14.3±2.3 mmHg (mean ±SD) in the group treated with dexa/net and 14.1±2.3 mmHg in the group treated with beta/chl. Final visual acuity was 8.7±2.0 decimals (mean ±SD) in the dexa/net group vs 8.9 ±1.7 in the beta/chl group.
Discussion
Cataract surgery is the most common surgical intervention. Despite actual techniques have reduced considerably signs of post-surgical inflammation and the risk of endophthalmitis, patients are often treated in the post-operative period with topical steroids and antibiotics (frequently in a fixed combination) as well as with non-steroidal anti-inflammatory drugs.2–7
The aim of this study was to evaluate the effectiveness of a short treatment with a steroid/antibiotic fixed combination containing 1 mg/mL dexamethasone and 3 mg/mL netilmicin in the control of post-operative inflammation. Results have shown that after 7 days more that 90% of patients have no sign of inflammation in the anterior chamber (AC flare and AC cells = score 0) and that the others have only a negligible level of inflammation (score 1). Accordingly, also signs of ocular surface inflammation were absent (score 0) at the study endpoint (7 days) in most patients (82% for conjunctival hyperaemia, 97% for corneal oedema and 98% lid oedema). The control treatment used in the study was another steroid-antibiotic fixed combination containing 2 mg/mL betamethasone and 5 mg/mL chloramphenicol. It is interesting to note that both treatments had a comparable anti-inflammatory efficacy rate despite the double dose of steroid present in beta/chl. This finding suggests, therefore, that a short-term treatment with 1 mg/mL dexamethasone is appropriate to manage post-surgical inflammation and that a stronger and extended exposure to steroids is not necessary. This ensures an effective control of post-operative inflammation and, at the same time, reduces the risk of developing corticosteroid-related side effects and avoids an overuse of antibiotics.
In our opinion, the main benefit of dexa/net over other available steroid-antibiotic fixed combinations is related to the antibiotic component. Indeed, netilmicin has a wide-spectrum activity (which also includes methicillin-resistant strains)12–14 and a negligible toxicity for the ocular surface.16 Since post-surgical infections are due to microorganisms resident in the ocular surface, mainly Coagulase-negative Staphylococci (in particular S. epidermidis) and S. Aureus,17 it is critical to use antibiotics highly effective on these germs. If not eradicated, these bacteria may enter inside the eye starting the day of surgical procedure until corneal incision is fully closed. For this reason, antibiotic treatment, when used, should starts the same day of surgery. Netilmicin is able to sterilize lid margins and conjunctiva when given before cataract surgery.14,18 Moreover, the bacterial flora on the ocular surface isolated from patients undergoing cataract surgery is highly susceptible to netilmicin and much less to other antibiotics.14 It is important to highlight that, regardless their source, S.Aureus and Coagulase-negative Staphylococci isolates are often characterized by methicillin resistance (MR) and multiresistance (MDR) to several classes of antibiotics; this finding is even more common in older patients, as those operated for cataract.19 Netilmicin is effective on methicillin-resistant S. Aureus (MRSA), methicillin-resistant Coagulase-negative Staphylococci (MRCoNS) and MDR Coagulase-negative Staphylococci,12–14 whereas these microorganisms display a high resistance to fluoroquinolones.12,13,19
As a potential limitation of the study, AC inflammation was measured, for practical reasons, by slit-lamp examination rather than by a laser flare and cell meter. Even if the scoring system used to measure flare and cells by slit-lamp examination is subjective and semi-quantitative, yet it corresponds to the actual daily routine of practice. Moreover, a consistency of results obtained with bio-microscopy and laser flare and cells meter measurements has been described.20 In summary, a short-term use of dexa/net fixed combination is effective as beta/chl in the control of post-operative inflammation following uncomplicated cataract surgery.
Data Sharing Statement
The raw data of the study used may be released upon request to the corresponding author.
Acknowledgments
Following Good Publication Practice (GPP3) guidelines and the International Committee of Medical Editors (ICMJE) recommendations, authors thank Laura C Collada Ali for providing medical writing support, which was funded by SIFI SpA (Italy). Authors also thank Debora Santoro, B.S in statistics, for analysing the data and providing statistical report of the study. This study was sponsored by SIFI SpA (Italy).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
VP is an employee of SIFI SpA (Italy). AC and AR are retirees. All remaining authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Eurostat. surgical operations and procedures statistics. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Surgical_operations_and_procedures_statistics$stable=0$redirect=no#Number_of_surgical_operations_and_procedures.
2. Kessel L, Tendal B, Jørgensen KJ, et al. Post-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: a systematic review. Ophthalmology. 2014;121(10):1915–1924. doi:10.1016/j.ophtha.2014.04.035
3. Wielders LHP, Schouten JSAG, Winkens B, et al.; ESCRS PREMED study group. Randomized controlled European multicenter trial on the prevention of cystoid macular edema after cataract surgery in diabetics: ESCRS PREMED Study Report 2. J Cataract Refract Surg. 2018;44(7):836–847. doi:10.1016/j.jcrs.2018.05.015
4. Behndig A, Cochener B, Güell JL, et al. Endophthalmitis prophylaxis in cataract surgery: overview of current practice patterns in 9 European countries. J Cataract Refract Surg. 2013;39(9):1421–1431. doi:10.1016/j.jcrs.2013.06.014
5. Behndig A, Cochener-Lamard B, Güell J, et al. Surgical, antiseptic, and antibiotic practice in cataract surgery: results from the European Observatory in 2013. J Cataract Refract Surg. 2015;41(12):2635–2643. doi:10.1016/j.jcrs.2015.06.031
6. Grzybowski A, Schwartz SG, Matsuura K, et al. Endophthalmitis prophylaxis in cataract surgery: overview of current practice patterns around the World. Curr Pharm Des. 2017;23(4):565–573. doi:10.2174/1381612822666161216122230
7. Kessel L, Flesner P, Andresen J, Erngaard D, Tendal B, Hjortdal J. Antibiotic prevention of postcataract endophthalmitis: a systematic review and meta-analysis. Acta Ophthalmol. 2015;93(4):303–317. doi:10.1111/aos.12684
8. Russo S, Papa V, Di Bella A, et al. Dexamethasone-netilmicin: a new ophthalmic steroid-antibiotic combination. Efficacy and safety after cataract surgery. Eye (Lond). 2007;21(1):58–64. doi:10.1038/sj.eye.6702123
9. Faraldi F, Papa V, Rasà D, Santoro D, Russo S. Netilmicin/dexamethasone fixed combination in the treatment of conjunctival inflammation. Clin Ophthalmol. 2013;7:1239–1244. doi:10.2147/OPTH.S44455
10. Rapisarda A, Arpa P, Fantaguzzi PM, et al. Dexamethasone/Netilmicin eye drops and eye gel for the treatment of ocular inflammation after micro-incisional vitreoretinal surgery. Clin Ophthalmol. 2020;14:3297–3303. doi:10.2147/OPTH.S257541
11. Nielsen RH. The use of dexamethasone in ophthalmologic steroid therapy: a preliminary report. Arch Ophthalmol. 1959;62(3):438–444. doi:10.1001/archopht.1959.04220030094014
12. Blanco AR, Roccaro AS, Spoto CG, et al. Susceptibility of methicillin-resistant staphylococci clinical isolates to netilmicin and other antibiotics commonly used in ophthalmic therapy. Curr Eye Res. 2013;38(8):811–816. doi:10.3109/02713683.2013.780624
13. Sanfilippo CM, Morrissey I, Janes R, et al. Surveillance of the activity of aminoglycosides and fluoroquinolones against ophthalmic pathogens from Europe in 2010–2011. Curr Eye Res. 2015;41(5):581–589. doi:10.3109/02713683.2015.1045084
14. Papa V, Blanco AR, Santocono M. Ocular flora and their antibiotic susceptibility in patients having cataract surgery in Italy. J Cataract Refract Surg. 2016;42(9):1312–1317. doi:10.1016/j.jcrs.2016.07.022
15. Papa V, Milazzo G, Santocono M, et al. Naproxen ophthalmic solution to manage inflammation after phacoemulsification. J Cataract Refract Surg. 2002;28(7):321–327. doi:10.1016/S0886-3350(01)01077-X
16. Papa V, Leonardi A, Getuli C, Pacelli V, Russo P, Milazzo G. Effect of ofloxacin and netilmicin on human corneal and conjunctival cells in vitro. J Ocul Pharmacol Ther. 2003;19(6):535–545. doi:10.1089/108076803322660459
17. ESCRS Guidelines for Prevention and Treatment of Endophthalmitis Following Cataract Surgery: Data, Dilemmas and Conclusions. European Society of Cataract and Refractive Surgeons, Temple House, Temple Road, Blackrock, Co Dublin, Ireland; 2013.
18. Aslan O, Teberik K, Yucel M, Gur N, Karakoc AE. Effect of topical netilmicin on the reduction of bacterial flora on the human conjunctiva. Eur J Ophthalmol. 2008;18(4):512–516. doi:10.1177/112067210801800402
19. Asbell PA, DeCory HH. Antibiotic resistance among bacterial conjunctival pathogens collected in the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) surveillance study. PLoS One. 2018;13(10):e0205814. doi:10.1371/journal.pone.0205814
20. Roberts CW, Brennan KM. A comparison of topical diclofenac with prednisolone for postcataract inflammation. Arch Ophthalmol. 1995;113(6):725–727. doi:10.1001/archopht.1995.01100060051031
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.