Back to Journals » Clinical Ophthalmology » Volume 17
Short-Term Total Tamponade with Perfluorocarbon Liquid and Silicone Oil in Complex Rhegmatogenous Retinal Detachment with Severe Proliferative Vitreoretinopathy
Authors Trabelsi O, Bouladi M ![]() , Ouertani A, Trabelsi A
, Ouertani A, Trabelsi A
Received 7 December 2022
Accepted for publication 27 January 2023
Published 8 February 2023 Volume 2023:17 Pages 515—525
DOI https://doi.org/10.2147/OPTH.S400156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Total Tamponade in retinal detachment" [ID 400156].
Views: 463
Omar Trabelsi,1 Mejda Bouladi,2 Amel Ouertani,1 Ahmed Trabelsi1
1Clinique Ophtalmologique de Tunis, Tunis, Tunisia; 2Department of Surgery, Faculty of Medicine of Tunis, University of Tunis El Manar, Tunis, Tunisia
Correspondence: Mejda Bouladi, Faculty of Medicine of Tunis, University of Tunis El Manar, 24, rue Amilcar, cité Wifec, 2070, La Marsa, Tunis, Tunisia, Tel +21698561086, Email [email protected]
Background: To evaluate retinal reattachment, visual functional results, and complications rates after total tamponade (TT) with perfluorocarbon liquid (PFCL) and silicone oil (SO) for 2 days followed by PFCL-SO exchange in complex retinal detachment (RD).
Methods: Retrospective study including 52 consecutive eyes with complex RD and advanced proliferative vitreoretinopathy, who underwent vitrectomy with TT. Patients underwent first surgery by 25-Gauge vitrectomy and partial PFCL-SO exchange (approximately 60% PFCL 40% SO fill) followed by second surgery with extraction of the PFCL and complete SO fill.
Results: After a mean follow-up period of 25.15 ± 6.6 months, the retina remained reattached in 48/52 eyes (92.3%) including 28 eyes (58.3%) without SO and 20 eyes (41.7%) with prolonged SO tamponade. Visual acuity improved in 45 eyes (86.6%) (P< 0.001), remained stable in 4 eyes (7.7%) and decreased in 3 eyes (5.7%). Complications consisted in mild anterior chamber inflammation in 10 eyes, ocular hypertension in 12 eyes, and cataract in 10 eyes.
Conclusion: Two-day TT with PFCL and SO may be considered in complex RD with advanced proliferative vitreoretinopathy especially in monocular patients. Further studies with longer follow-up period and retinal electrophysiologic assessment may be needed.
Keywords: complex retinal detachment, proliferative vitreoretinopathy, monocular patient, perfluorocarbon liquid, silicone oil, positioning
Plain Language Summary
We studied anatomic and functional outcomes after two-day total-tamponade with perfluorocarbon liquid and silicone oil followed by PFCL-SO exchange in complex retinal detachment. Mean follow-up period was 25.15 months; Retina reattached in 92.3% of eyes; Visual acuity improved in 86.6% of eyes (P<0.001). Complications were inflammation (10 eyes), ocular hypertension (12 eyes), and cataract (10 eyes).
Introduction
Vitreo-retinal surgery has benefited from many advances over the past 30 years including the development of intra-operative tamponade agents like perfluorocarbon liquids (PFCL) which improved anatomic and visual outcomes. However, the treatment of complex retinal detachment (RD) remains a challenge, and numerous studies on different modalities of PFCL use have been reported with varying success rates and complications.1–5
Complex RDs are characterized by advanced proliferative vitreoretinopathy (PVR) which is the major risk factor for RD surgery failure. In addition, inferior PVR makes reattachment of the inferior retina difficult to achieve with conventional pars plana vitrectomy.2,6
PFCL have been demonstrated to be well tolerated for intraoperative and short-term post-operative tamponade. Double filling with PFCL and silicone oil (SO) for at least 5 weeks has been reported to be effective in tamponading the inferior and superior retina at the same time.7,8
The aim of our study was to evaluate retinal reattachment, visual functional results, and complications rates after total tamponade (TT) with PFCL and SO for 2 days followed by PFCL–SO exchange.
Patients and Methods
This is a retrospective study including 52 consecutive eyes from 52 patients with complex RD, who underwent vitrectomy with TT between March 2016 and February 2021 at the Clinique Ophtalmologique de Tunis.
Patients included in the study had complex rhegmatogenous RD associated with grade C PVR regardless of the size and the number of breaks and variable capability for post-operative positioning. PVR was classified according the Machemer’s classification defined as the presence of full thickness rigid retinal folds in one area with heavily condensate vitreous organization.9
The minimum follow-up period was 12 months.
The TT approach was decided based on clinical presentation during preoperative ophthalmic examination or intraoperatively, in cases where complete retinal reattachment could not be achieved.
Exclusion criteria were: exudative RD, tractional RD, primary rhegmatogenous RD with grade A or B PVR. Patients with follow-up under 12 months were also excluded from the study.
For each patient, the following data were recorded: age, gender, medical history, pre and postoperative best-corrected visual acuity (BCVA), anterior segment inflammation, lens status, intra-ocular pressure (IOP), retina status with RD classification according to the classification of Retina Society Terminology committee (1991),9 cataract extraction and retinectomy rates, duration of SO tamponade, and complications rate.
The study respected the tenets of the Declaration of Helsinki, was approved by the institutional committee (Comité d’éthique de la Clinique Ophtalmologique de Tunis), and written informed consent was obtained from all patients or legal guardian before the surgical procedure.
Surgical Technique
25-gauge pars plana vitrectomy was performed by an experienced vitreo-retinal surgeon (OT) with Constellation® Vision system – Alcon using non-contact wide-field visualization system (BIOM). Surgery included complete vitreous removal, injection of PFCL (DK-Line perfluorocarbon liquids Bausch and Lomb), PVR dissection (bimanual if necessary, with the use of chandelier), and endo-laser photocoagulation. As decided preoperatively because of advanced PVR or when complete retinal reattachment could not be achieved, we left PFCL in the vitreous cavity and complete with SO injection (oxane 1300 silicone oil (Bausch and Lomb)). The proportions of PFCL and SO obtained were estimated approximately to 60% PFCL and 40% SO.
In some cases, retinectomy and cataract extraction with intraocular lens (IOL) implantation were additionally performed. With the understanding of the complementary physical tamponade properties of SO and PFCL, these patients were not required to follow any specific postoperative positioning protocol (Figure 1).
 |
Figure 1 Schematic drawing representing the location of perfluorocarbon liquid and silicone oil in the vitreous cavity depending on the position of the head. (A) insufficient tamponade of the inferior retina with silicone oil only (B) Upright position head (Ci and Cii) tilted head. Note that superior and inferior retina are always tamponaded regardless of the position of the head. |
After 2 days of TT with 60% PFCL–40% SO, the patients underwent a second surgical procedure with 3 trocars (25G): for endolight, PFCL canula and for SO injection. Gentle aspiration of PFCL was performed by the operator aid simultaneously to SO injection which was made by the surgeon and controlled by the foot pedal (Video S1).
With the understanding of the complementary physical tamponade properties of SO and PFCL, these patients were not required to follow any specific postoperative positioning protocol (Figure 1).
All patients were given mixed topical steroids and antibiotics 5 times daily with tapering over 4 weeks.
Follow-up visits were performed at days 1 and 3, weeks 1, 2 and 4, then every 3 months thereafter. Removal of SO (ROSO) was performed after at least 3 months, if indicated.
Post-operative ophthalmic examination included BCVA, anterior segment examination, IOP, and fundus examination. OCT (Optovue, Angiovue) was performed in some cases. Anterior chamber inflammation was graded according to the SUN (Standardization of Uveitis Nomenclature) working group classification.10
The primary outcome measure was the retinal reattachment rate at the final ophthalmic examination (at least after 12 months of follow-up). The secondary outcome measures were the final BCVA and postoperative complications.
Statistical Analysis
Statistical analysis was performed with SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Data were expressed as mean ± standard deviation (SD). BCVA was converted to the logarithm of the minimum angle of resolution LogMAR for statistical analysis and was reported using Snellen fraction visual acuity.11 Mean final BCVA was compared with baseline using paired t-test and changes were reported in letters of improvements (ETDRS).11 Pearson correlation coefficient was used to correlate variables. P value < 0.05 was considered statistically significant.
Result
Preoperative Characteristics
Fifty-two consecutive eyes of 52 patients with complex RD were included in the study. Patient demographics and baseline clinical characteristics are summarized in Table 1.
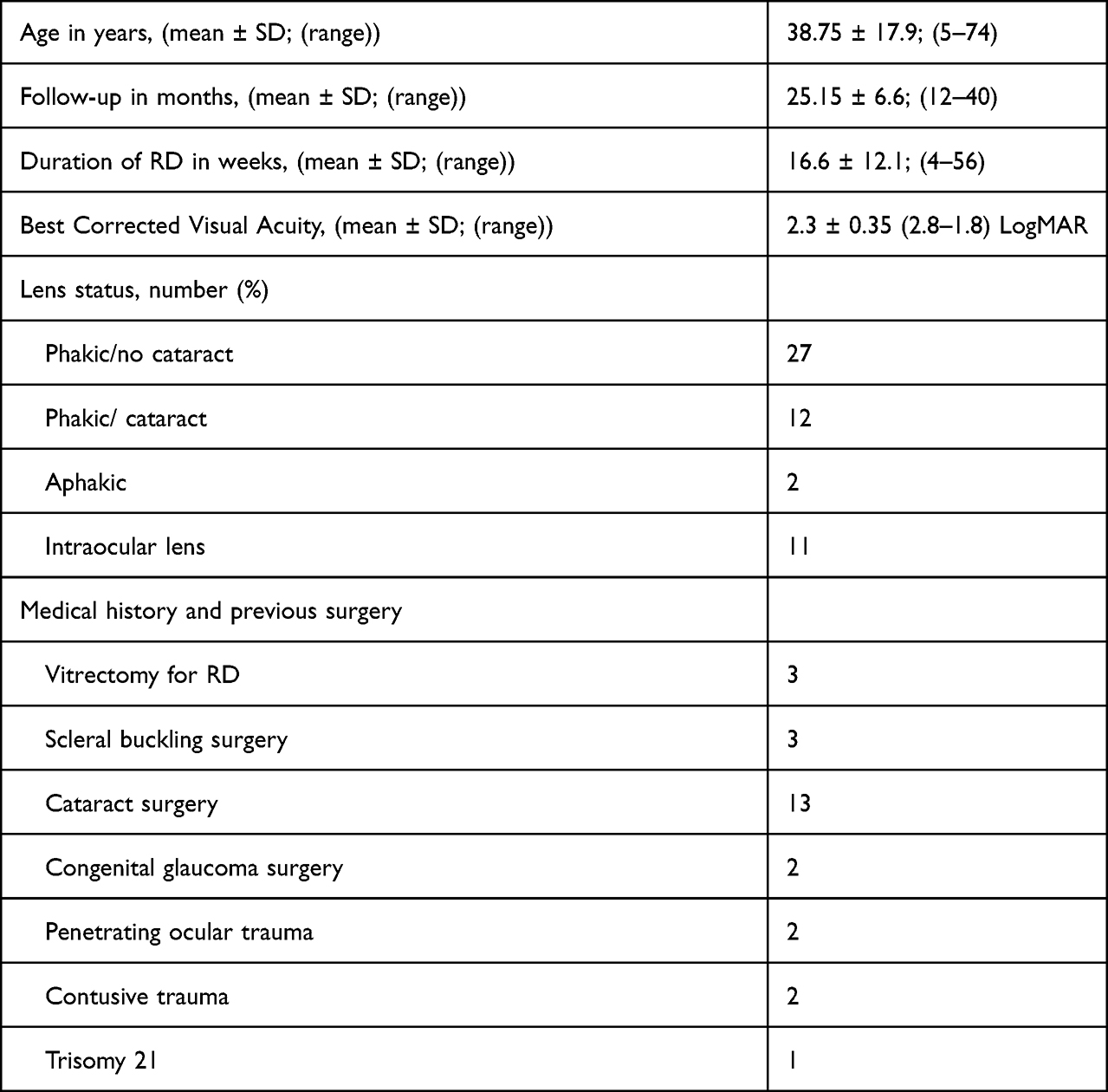 |
Table 1 Baseline Demographic and Clinical Characteristics |
Thirty-seven patients were male and 15 were female. The mean age was 38.75 years. Six patients had undergone previous RD surgery using vitrectomy (3 eyes) and scleral buckling surgery (3 eyes). Mean pre-operative BCVA was 2.3 log MAR (Snellen fraction ranging from 0 to 2/200), and 18 patients (34.6%) were monocular. Characteristics of RD in terms of size and number of breaks and PVR are summarized in Table 2.
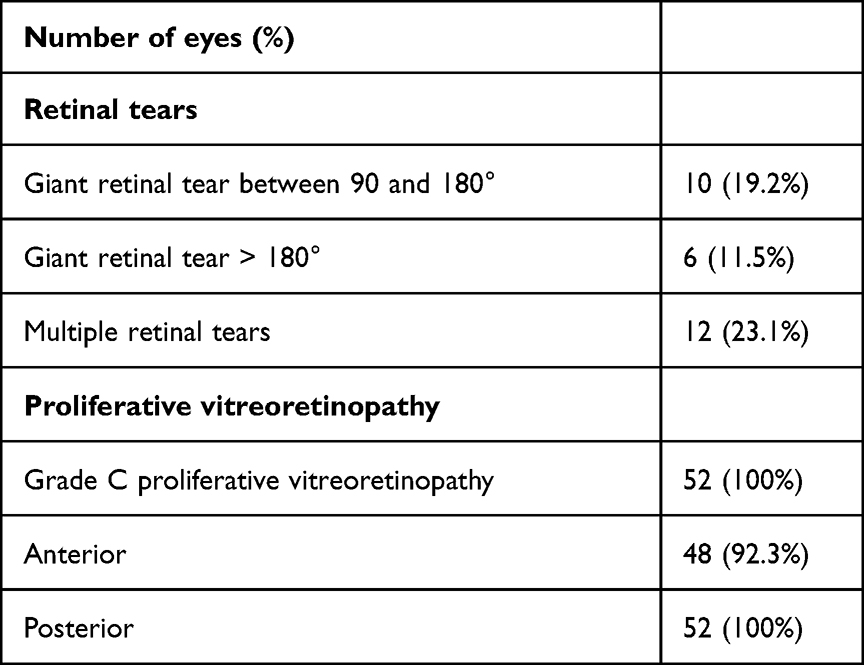 |
Table 2 Characteristics of Retinal Detachment and Retinal Breaks |
Surgical Characteristics
During the first surgery, 6/39 phakic eyes (15.4%) underwent cataract extraction with IOL implantation, and 8/52 eyes (15.4%) had retinectomy. After two-days of PFCL-SO TT, the second surgery was performed including completion of laser photocoagulation in 41 eyes (78.8%), cataract extraction with IOL implantation in one eye and retinectomy in one eye.
Anatomic Results
ROSO was performed in 33 eyes (63.5%) at 7.6 ± 4.9 months (3–24 months) according to the criteria in Table 2. Five eyes needed SO reinjection because of recurrence of partial RD. After a mean follow-up period of 25.15 ± 6.6 months, the retina remained reattached in 48 eyes (92.3%) including 28 eyes (58.3%) without SO and 20 eyes (41.7%) with prolonged SO tamponade (Figures 2–5).
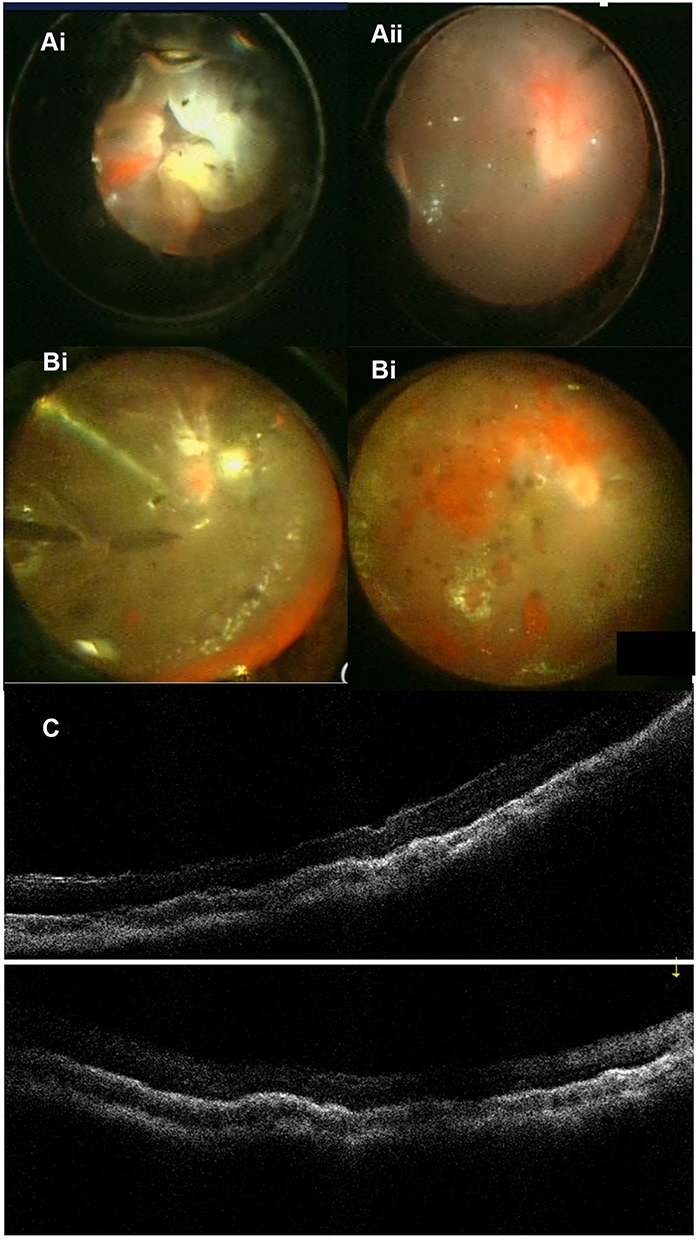 |
Figure 2 A 14 years-old boy with complex retinal detachment. (A) First surgical procedure, intraoperative fundus photography. (Ai) Before vitrectomy: retinal detachment with advanced proliferative vitreoretinopathy. (Aii) End of vitrectomy: total tamponade of the retina with perfluorocarbon liquid and silicone oil. (B) Second surgical procedure, intraoperative fundus photography (Bi) Perfluorocarbon liquid – silicone oil exchange. (Bii) Retinal tamponade with silicone oil. (C) Postoperative optical coherence tomography after 1 month: macular reattachment. |
 |
Figure 3 A 42 years-old monocular man with complex retinal detachment. (A) preoperative ocular ultrasonography: retinal detachment with advanced proliferative vitreoretinopathy. (B) postoperative optical coherence tomography after 4 months: macular reattachment with irregularities in the retinal pigment epithelium. |
 |
Figure 4 Long term follow-up in a 36 years-old man with complex retinal detachment in his right eye. (Ai and Aii) preoperative ocular ultrasonography: retinal detachment with advanced proliferative vitreoretinopathy. Visual acuity was 2.3 logMar (B and C) Postoperative fundus photography and optical coherence tomography after 28 mois: retinal reattachment under silicone oil prolonged tamponade. Visual acuity improved to 1 logMAR. Silicone oil was not removed because the patient was unwilling to undergo further surgeries. |
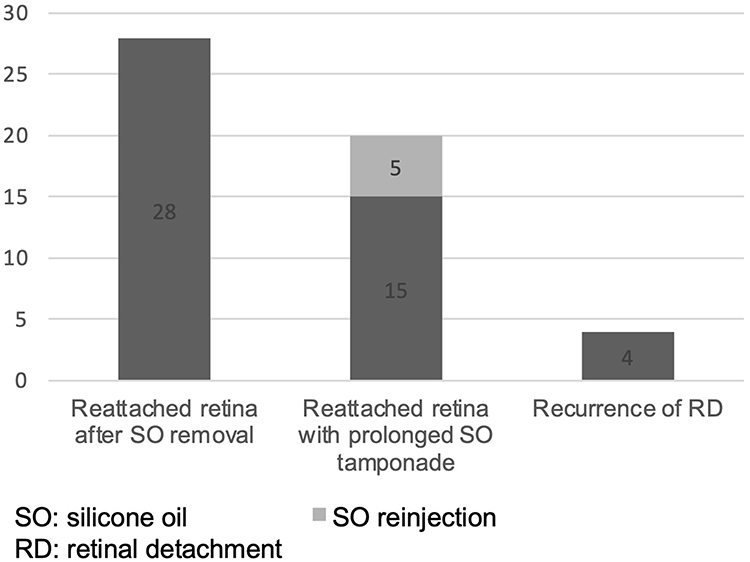 |
Figure 5 Rates of retinal reattachment and recurrence of retinal detachment. |
ROSO was not performed in 20 eyes with reattached retina for several reasons which are summarized in Table 3. Patients who were unwilling to undergo further surgeries were monitored closely for complications of prolonged SO tamponade.
 |
Table 3 Reasons for Prolonged Silicone Oil Tamponade |
Functional Results
VA improved in 45 eyes (86.5%), was remained stable in 4 eyes (7.7%) and decreased in 3 eyes (5.8%). The mean postoperative BCVA at the final visit was 1.1 ± 0.57 (2.8–0.2) logMAR with Snellen fraction ranging from 0 to 6/200 and 32.9 ± 19.5 ETDRS letters of improvement (−2.00 to 73 letters). The difference from the preoperative BCVA was statistically significant (P<0.001) (Figure 6).
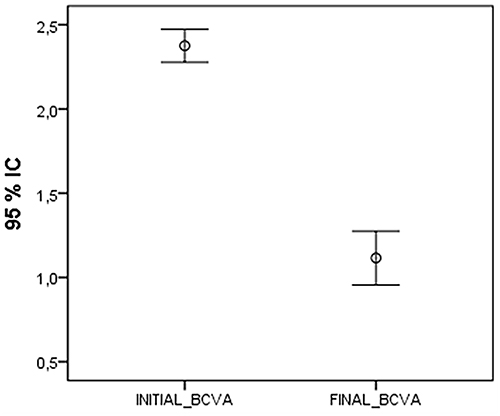 |
Figure 6 Boxplot chart of preoperative and final postoperative logMAR best corrected visual acuity. Abbreviation: BCVA, best corrected visual acuity. |
Thirty-six patients (69.2%) had a final postoperative BCVA of 1.00 log MAR or better. Subjective visual improvement was noticed by 47 patients (90.4%) and a gain of autonomy in everyday life was reported by the 18 monocular patients and/or their family members.
Complications
Complications occurred in 18 eyes (34.6%). Anterior chamber inflammation less than grade 2+ cells and flare was noticed in 8 eyes (15.4%) during the initial 2 days after the first surgery and in 2 eyes (3.8%) after the second surgery, and resolved with increased topic steroids frequency. Ocular hypertension occurred in 12 eyes (23.1%) and was managed with topical antiglaucoma treatment in all eyes and with additional systemic acetazolamide in 5 eyes. Ten eyes developed cataract during the postoperative follow-up. We did not notice PFCL migration to the anterior chamber in any case.
Correlations
No statistically significant correlation was found between postoperative BCVA and preoperative BCVA, number of previous surgeries, or removal of SO.
Discussion
We report the results of surgical repair with vitrectomy and two-day TT by SO and PFCL in eyes with complex RD and advanced PVR. These eyes are generally thought to have a high risk of surgical failure after conventional vitrectomy and were considered inoperable by many vitreoretinal surgeons in our current series.
Retina reattachment was achieved in 92.3% of eyes (48/52) with improvement of BCVA in 86.5% (45/52 eyes) and subjective visual improvement with a gain of autonomy in everyday life noticed in all the 18 monocular patients.
Complex RD is commonly associated with advanced PVR, vitreous hemorrhage, ocular trauma, giant retinal tear and/or multiple or posterior retinal breaks even without PVR. In our study, we included eyes with RD associated with grade C PVR regardless of the size and the number of breaks.
Different surgical techniques have been used for complex RD with anatomic success rates varying from 50% to 100% versus 30% to 75% offered by conventional vitrectomy or association of vitrectomy and scleral buckling surgery.1,8,12–23
Among these techniques, the use of PFCL for 7 days with supine positioning followed by PFCL-SO exchange7,8,24 as well as use of light and heavy SO or F6H8 and SO for 8 to 10 weeks have been popularized.25 Some of the complications and the limitations of these previous techniques include the need for strict postoperative supine positioning, SO emulsification, inflammation, and insufficient tamponade of the superior retina.25,26
Our anatomic and functional results are in line with those of the different techniques for complex RD. But the inclusion criteria were different, especially the severity and the duration of the RD.
In a prospective study using double retinal tamponade with PFCL and C3F8 gas during 4 to 7 weeks for rhegmatogenous RD with inferior breaks, Abdelkader et al27 reported an anatomical success rate of 93.3%. Our results were comparable, but in our series, the mean duration of RD was 16.6 weeks which may be associated with a more severe PVR. In our study, prolonged SO tamponade was needed in 20/48 eyes (41.7%) to achieve permanent retinal reattachment.
PFCL is usually used for temporary intraoperative tamponade facilitating retinal stabilization during vitrectomy and is generally removed and replaced with SO at the end of surgery. Different studies demonstrated the safety of PFCL when used for short-term postoperative tamponade in complicated RD. Most of these studies used PFCL for a period ranging from 5 days to 2 months to obtain adequate chorioretinal laser scars which are reported to develop within 2 weeks after surgery.1,7,8,24,28
We used total tamponade and decided to remove PFCL after 2 days. The aim of this short postoperative tamponade was to unfold the retina and to relax PVR which may allow a better reattachment of the retina. In fact, remaining and adherent PVR were very easier to remove after the two days of total tamponade with PFCL and SO.
In our study, the TT was indicated preoperatively because of the advanced PVR (all eyes had grade C PVR) or intraoperatively when complete retinal reattachment could not be achieved.
The anatomic rate of success of vitrectomy with relaxing retinectomy varies from 47% to 95% in various studies.29 Hocaoglu et al30 reported 94% of retinal attachment rate after retinotomy/retinectomy in 126 eyes with RD complicated by advanced anterior PVR. They reported a negative correlation between postoperative visual acuity and more extensive retinectomy and concluded that retinectomy should be performed at a milder stage of PVR. In our study, retinectomy was not needed in the majority of eyes, and was only necessary in 9 eyes (17.3%).
It is important to note that our technique does not require any limitation on postoperative positioning in our patients. The presence of PFCL and SO simultaneously had the distinct advantage of tamponade of the upper and the lower retina regardless of the position of the head (Figure 1). This property is particularly useful in uncooperative subjects where postoperative positioning may be impossible to obtain.
In our study, mild complications occurred in 18 eyes (34.6%). Mild intraocular inflammation was noticed in 10 eyes (19.2%) at the 2-day visit. Notably, this is a lower rate than that reported by Sigler et al,31 (32%) who used a long period of PFCL tamponade in their series (2–3 weeks).
Ocular hypertension occurred in 12 eyes (23.1%), comparable to the rates reported in the literature ranging from 4.8% to 36%.7,24,31 All patients responded to medical anti-glaucoma treatment and no one required filtrating surgery.
At the final visit, SO tamponade was still needed in 20/48 eyes (41.7%) because of the risk of RD recurrence. This finding was in line with reported results by Vidne-Hay et al,32 who demonstrated the safety of long-term silicone oil tamponade (>12 months) in 43 eyes with complicated retinal detachment.
Our study had some limitations including its retrospective design, the lack of a control group, the need for 2 surgical procedures with the consequent cost effectiveness.
However, we noticed many advantages of short-term TT with PFCL and SO for complex RD with advanced PVR. Our technique allowed reattachment of the retina in 92.3% of eyes. In addition, a functional visual improvement was seen as early the first day after the exchange. Another important practical advantage was the lack of requirement for postoperative positioning.
In conclusion, we suggest that surgeons consider two-day TT with PFCL and SO in complex RD with advanced PVR. Further studies with longer follow-up period and retinal electrophysiologic assessment may be needed to better investigate the results of this technique.
Acknowledgment
This work was presented at the 128e Congrès International de la Société Française d’Ophtalmologie and the 6th International Red Sea Ophthalmology Symposium.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sirimaharaj M, Balachandran C, Chan WC, et al. Vitrectomy with short term postoperative tamponade using perfluorocarbon liquid for giant retinal tears. Br J Ophthalmol. 2005;89(9):1176–1179.
2. Bottoni F, Sborgia M, Arpa P, et al. Perfluorocarbon liquids as postoperative short-term vitreous substitutes in complicated retinal detachment. Graefes Arch Clin Exp Ophthalmol. 1993;231(11):619–628. doi:10.1007/BF00921955
3. Ghosh YK, Banerjee S, Savant V, et al. Surgical treatment and outcome of patients with giant retinal tears. Eye. 2004;18(10):996–1000. doi:10.1038/sj.eye.6701390
4. Glaser BM, Carter JB, Kuppermann BD, Michels RG. Perfluoro-octane in the treatment of giant retinal tears with proliferative vitreoretinopathy. Ophthalmology. 1991;98(11):1613–1621. doi:10.1016/S0161-6420(91)32076-1
5. Kramer SG, Hwang D, Peyman GA, Schulman,JA, Sullivan B. Perfluorocarbon liquids in ophthalmology. Surv Ophthalmol. 1995;39(5):375–395. doi:10.1016/S0039-6257(05)80093-1
6. Khan MA, Brady CJ, Kaiser RS. Clinical management of proliferative vitreoretinopathy: an update. Retina. 2015;35(2):165–175. doi:10.1097/IAE.0000000000000447
7. Zenoni S, Romano MR, Palmieri S, et al. Ocular tolerance and efficacy of short-term tamponade with double filling of polydimethyloxane and perfluoro-n-octane. Clin Ophthalmol. 2011;5:443–449. doi:10.2147/OPTH.S17315
8. Bottoni F, Arpa P, Vinciguerra P, et al. Combined silicone and fluorosilicone oil tamponade (double filling) in the management of complicated retinal detachment. Ophthalmologica. 1992;204(2):77–81. doi:10.1159/000310273
9. Machemer R, Aaberg TM, Freeman HM, et al. An updated classification of retinal detachment with proliferative vitreoretinopathy. Am J Ophthalmol. 1991;112(2):159–165. doi:10.1016/S0002-9394(14)76695-4
10. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. J Ophthalmol. 2005;140:509–516.
11. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. doi:10.1097/IAE.0b013e3181d87e04
12. Blinder KJ, Peyman GA, Desai UR, et al. Vitreon, a short-term vitreoretinal tamponade. Br J Ophthalmol. 1992;76(9):525–528. doi:10.1136/bjo.76.9.525
13. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142–2154. doi:10.1016/j.ophtha.2007.09.013
14. Adelman RA, Parnes AJ, Sipperley JO, et al. Strategy for the management of complex retinal detachments: the European vitreo-retinal society retinal detachment study report 2. Ophthalmology. 2013;120(9):1809–1813. doi:10.1016/j.ophtha.2013.01.056
15. Rizzo S, Genovesi-Ebert F, Vento A, et al. A new heavy silicone oil (HWS 46-3000) used as a prolonged internal tamponade agent in complicated vitreoretinal surgery: a pilot study. Retina. 2007;27(5):613–620. doi:10.1097/01.iae.0000251228.33870.64
16. Auriol S, Pagot-Mathis V, Mahieu L, et al. Efficacy and safety of heavy silicone oil densiron 68® in the treatment of complicated retinal detachment with large inferior retinectomy. Graefes Arch Clin Exp Ophthalmol. 2008;246(10):1383–1389. doi:10.1007/s00417-008-0876-6
17. Li W, Zheng J, Zheng Q, et al. Clinical complications of densiron 68 intraocular tamponade for complicated retinal detachment. Eye. 2010;24(1):21–28. doi:10.1038/eye.2009.57
18. Joussen AM, Rizzo S, Kirchhof B, et al. Heavy silicone oil versus standard silicone oil in as vitreous tamponade in inferior PVR (HSO study): interim analysis. Acta Ophthalmol. 2011;89(6):e483–e489. doi:10.1111/j.1755-3768.2011.02139.x
19. Boscia F, Furino C, Recchimurzo N, et al. Oxane HD vs silicone oil and scleral buckle in retinal detachment with proliferative vitreoretinopathy and inferior retinal breaks. Graefes Arch Clin Exp Ophthalmol. 2008;246(7):943–948. doi:10.1007/s00417-008-0806-7
20. Herbrig E, Sandner D, Engelmann K. Anatomical and functional results of endotamponade with heavy silicone oil – densiron 68 – in complicated retinal detachment. Ophthalmic Res. 2007;39(4):198–206. doi:10.1159/000104681
21. Herbert E, Stappler T, Wetterqvist C, et al. Tamponade properties of double-filling with perfluorohexyloctane and silicone oil in a model eye chamber. Graefes Arch Clin Exp Ophthalmol. 2004;242(3):250–254. doi:10.1007/s00417-003-0830-6
22. Abrams GW, Azen SP, McCuen BW, et al. Vitrectomy with silicone oil or long-acting gas in eyes with severe proliferative vitreoretinopathy: results of additional and long-term follow-up. Silicone study report 11. Arch Ophthalmol. 1997;115(3):335–344. doi:10.1001/archopht.1997.01100150337005
23. Duan A, She H, Qi Y. Complications after heavy silicone oil tamponade in complicated retinal detachment. Retina. 2011;31(3):547–552. doi:10.1097/IAE.0b013e3181eef2fd
24. Zhang Z, Wei Y, Jiang X, Zhang S. Surgical outcomes of 27-gauge pars plana vitrectomy with short-term postoperative tamponade of perfluorocarbon liquid for repair of giant retinal tears. Int Ophthalmol. 2018;38(4):1505–1513. doi:10.1007/s10792-017-0613-4
25. Caporossi T, Franco F, Finocchio L, et al. Clinical research densiron 68 heavy silicone oil in the management of inferior retinal detachment recurrence: analysis on functional and anatomical outcomes and complications. Int J Ophthalmol. 2019;12(4):615–620. doi:10.18240/ijo.2019.04.15
26. Wong D, Van Meurs JC, Stappler T, et al. A pilot study on the use of a perfluorohexyloctane/silicone oil solution as a heavier than water internal tamponade agent. Br J Ophthalmol. 2005;89(6):662–665. doi:10.1136/bjo.2004.055178
27. Abdelkader MF, Abd-Elhamid S, Elwan M, Abdelhalim AS. Double retinal tamponade for treatment of rhegmatogenous retinal detachment with proliferative vitreoretinopathy and inferior breaks. J Ophthalmol. 2020;2020:6938627. doi:10.1155/2020/6938627
28. Imaizumi A, Kusaka S, Noguchi H, et al. Efficacy of short-term postoperative perfluoro-n-octane tamponade for pediatric complex retinal detachment. Am J Ophthalmol. 2014;157(2):384–389. doi:10.1016/j.ajo.2013.10.002
29. Churashov SV, Kulikov AN, Maltsev DS. Surgical outcomes in inferior recurrences of rhegmatogenous retinal detachment. Int J Ophthalmol. 2021;14(12):1909–1914. doi:10.18240/ijo.2021.12.15
30. Hocaoglu M, Karacorlu M, Giray Ersoz M, Musulbas IS, Arf S. Retinotomy and retinectomy for anterior inferior proliferative vitreoretinopathy: can visual outcome be improved? Eur J Ophthalmol. 2021;22:11206721211012848.
31. Sigler EJ, Randolph JC, Charles S. Foreign body response within postoperative perfluoro-N-octane for retinal detachment repair: clinical features, grading system, and histopathology. Retina. 2014;34(2):237–246. doi:10.1097/IAE.0b013e31829d002e
32. Vidne-Hay O, Platner E, Alhalel A, Moisseiev J. Long-term silicone oil tamponade in eyes with complicated retinal detachment. Eur J Ophthalmol. 2022;32(3):1728–1734. doi:10.1177/11206721211019551
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.