Back to Journals » Clinical Ophthalmology » Volume 15
Short-Term Outcomes After COVID-19-Related Treatment Interruption Among Patients with Neovascular Age-Related Macular Degeneration Receiving Intravitreal Bevacizumab
Authors Allegrini D ![]() , Raimondi R
, Raimondi R ![]() , Montesano G, Borgia A, Sorrentino T, Tsoutsanis P
, Montesano G, Borgia A, Sorrentino T, Tsoutsanis P ![]() , Romano MR
, Romano MR
Received 11 June 2021
Accepted for publication 7 September 2021
Published 8 October 2021 Volume 2021:15 Pages 4073—4079
DOI https://doi.org/10.2147/OPTH.S323058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Davide Allegrini,1 Raffaele Raimondi,2 Giovanni Montesano,3 Alfredo Borgia,2 Tania Sorrentino,2 Panagiotis Tsoutsanis,2 Mario R Romano1,2
1Eye Center, Humanitas, Bergamo, Italy; 2Department of Biomedical Sciences, Humanitas University, Milano, Italy; 3University of London - Optometry and Visual Sciences, London, UK
Correspondence: Raffaele Raimondi
Department of Biomedical Sciences, Humanitas University, Via Rita Levi Montalcini 4, Pieve Emanuele, Milano, Italy
Tel +39 02 8224 7100
Email [email protected]
Purpose: To assess outcomes and recovery strategy of patients undergoing intravitreal injections for exudative age-related macular degeneration who experienced COVID-19 related interruption in treatment during complete lockdown.
Methods: This was a retrospective, observational case study. We used a mixed effect model with random intercepts to evaluate best corrected visual acuity (BCVA) accounting for measured central macular thickness (CMT) and individual variability of each eye. Furthermore, we analysed measures of the pigmented epithelium detachment as well as presence of subretinal fluid and intraretinal cysts.
Results: We included 39 patients and we found a significant reduction in the BCVA between the pre- and post-lockdown controlling for CMT. There was no significant difference in pigmented epithelium detachment and in presence of subretinal fluid and intraretinal cysts.
Conclusion: We detected a significant loss in visual function. The magnitude of the average loss was, however, limited suggesting good efficacy of the recovery strategy.
Keywords: IVT interruption, covid-19, intravitreal injection, bevacizumab
Introduction
Age-related macular degeneration (AMD) is a leading cause of progressive loss of vision.1 Neovascular AMD is a late form characterized by a choroidal neovascularization (CNV). Inhibition of vascular endothelial growth factor (VEGF) is effective in slowing down the angiogenic process.1 Three main treatment regimens are commonly employed: monthly injections,2,3 treat and extend4 and pro re nata (PRN).5,6 Studies have repeatedly shown the importance of frequent injections for long-term preservation of vision.5,7
COVID-19 pandemic had a disruptive impact during its first wave and as of early November 2020, the WHO has confirmed over 46 million cases and 1.2 million deaths worldwide.8 Our tertiary center located in Bergamo, Italy, was heavily affected by the COVID-19 pandemic and its organization was reshaped to face this new emergency. Indeed, resources and staff were relocated and ophthalmology service only attended to absolute emergencies.9 Consequently, intravitreal injections were suspended for almost three months from 8th of March to 31st of May 2020. Patients were rescheduled following the original order and received the injection under a strict COVID-19 prevention protocol.
While decisions amid a crisis are always difficult and complex, a retrospective evaluation of the adopted strategies could provide insight on the impact and efficacy of our choices. In particular, we decided to carry out a new loading phase of bevacizumab, one injection per month for three months before starting back with the previous regimen.
The purpose of this study is to assess clinical outcomes attributed to the first lockdown and the efficacy of our recovery strategy by retrospectively analyzing data before and after the event, which may provide insight into the effectiveness of our past decisions.
Methods
This retrospective, observational case study was performed at a single center: Humanitas Gavazzeni-Castelli, Bergamo, Italy. The study was approved by the Institutional Review Board of Humanitas Gavazzeni protocol number 69/20 GAV and was conducted in accordance with the principles of the Declaration of Helsinki. All patients signed an informed consent authorizing deidentified retrospective analysis of their outcomes for scientific purposes.
Patients
We included patients undergoing intravitreal injections of anti-VEGF (bevacizumab) following Treat and Extend protocol at our institution that received at least three previous injections (loading phase) before the interruption, and that underwent their last injection between January and February 2020. Minimum follow-up was 6 months before the lockdown and 4 months after the lockdown, charts were reviewed starting from March 2019 and up to December 2020. All included patients were scheduled to receive another injection between March and April 2020. Exclusion criteria were concomitant diseases: diabetes mellitus and retinal vessels occlusion. Patients that underwent any kind of eye surgery during the follow-up period were also excluded.
Outcome Measures
The primary outcomes were the mean best corrected visual acuity (BCVA) between the two time intervals before and after lockdown, accounting for measured central macular thickness (CMT).
Secondary outcomes were CNV dimensions, presence of subretinal fluid (SRF), intraretinal cysts (IRC), fibrosis.
Clinical Assessment Protocol
Our standard protocol includes: a comprehensive ophthalmic examination at each follow-up (f/u) visit. The ophthalmic examination protocol included BCVA assessment in Snellen fractions, applanation tonometry, slit-lamp biomicroscopy, dilated fundus examination, and spectral domain (SD)-OCT imaging. All patients underwent the standard protocol assessment on a monthly basis except during the lockdown. At the baseline, the diagnosis was confirmed by fluorescein angiography (FA).
SD-OCT Scan Protocol
We used the Spectralis SD-OCT (Heidelberg Engineering GmbH, Heidelberg, Germany). At each visit, the following scans were acquired in all eyes: a high-definition horizontal fovea-centered cross line B-scan at 30 and the horizontal macula raster consisting of 49 B-scans 120 µm-spaced over an area of 20° · 20°. The “Thickness Map” function was used to automatically measure the mean CMT, based on the mean retinal thickness within a circular area of 0.5-mm radius from the foveal center.
Measurement of the pigmented epithelium detachment (PED) was carried out manually using the caliber function in the foveal scan: height was defined as maximum distance between RPE and the inner most aspect of Bruch’s membrane, width was defined as the maximum distance between lesion edges. PED is a recognized crucial biomarker for progression and prognosis.10
Fibrosis was defined as >50% of CNV occupied by compact, sheet-like hyperreflective material, situated either above or underneath the RPE.11 This variable was assessed on a dichotomic scale: present or absent.
Subretinal fluid was defined as a separation of the neuroretina from the outer high reflectivity band by a well-defined hyporeflective space at the fovea.12 This variable was assessed on a dichotomic scale: present or absent.
Intraretinal cysts were defined as well defined intraretinal hyporeflective spaces at the fovea separated by reflective septae.12 This variable was assessed on a dichotomic scale: present or absent.
Two masked observers (D.A. and R.R.) independently evaluated OCT images quantitatively and qualitatively. A third observer (M.R.R.) resolved any case of disagreement. Segmentation errors were manually corrected with built-in software when needed.
Treatment Protocol
After informed consent, all patients had the IVI performed in our clinic. IVI of anti-VEGF (bevacizumab) were carried out in the operating room by skilled surgeons or trainees under supervision.
Recovery protocol included starting a new loading phase of bevacizumab, one injection per month for three months. Successively, patients were started back on Treat and Extend protocol.
Safety Assessment
At each f/u visit, we investigated frequency and severity of any adverse event.
Statistical Analysis
To carry out the statistical analysis, we used R (R Foundation for Statistical Computing, Vienna, Austria) software and converted all Snellen BCVA values into logarithm of the minimum angle of resolution (logMAR) units. Continuous descriptive data are reported as Median [Interquartile Range].
We used a mixed effect model with random intercepts to evaluate the BCVA (logMAR) accounting for measured CMT and individual variability of each eye. The random effects also accounted for correlations among measurements from the same eye. We used this model to test whether the BCVA in the post-lockdown period was significantly lower compared to the corresponding prediction from the CMT by including a categorical fixed effect that coded whether the observations were measured before or after the lockdown. If significant (p < 0.05), the categorical fixed effect would indicate that, in the post-lockdown period, the observed BCVA was different from that expected from the CMT value. This was our main hypothesis.
We also included a random slope to account for individual variations between the pre- and post-lockdown periods.
It is important to notice that such a model does not have the goal of predicting BCVA from the CMT. Accurate predictions were only achieved for this specific sample thanks to the use of random effects and do not represent the generic predictive performance of the CMT. Rather, this model allowed us to compare BCVA between the two time intervals accounting for the individual CMT values.
Finally, we performed other exploratory analyses to investigate changes in the features of the CNV. We used another linear mixed effect model with random intercepts to test whether the maximum height and width of the CNV, measured from the OCT scans at each visit, was significantly different between pre- and post-lockdown. In this case, the random intercept term was also necessary to account for correlations among observations from the same eye. The change in the frequency of the SRF and IRC were measured through a mixed effect logistic regression.
Results
Starting from March 2019, we reviewed 75 patients charts. Following our inclusion criteria, 39 patients who were receiving intravitreal anti-VEGF (bevacizumab) for exudative AMD were included in the analysis. Therefore, we excluded a total of 36 patients, 24 patients were excluded because they received different anti-VEGF types in the observed period, and 12 were excluded due to poor compliance in the pre-lockdown period. Median age was 76,2 [Interquartile range: 71.5,82], 15 males [38%], right eye were 21 [53%]. A description of the sample characteristics at baseline before and after lockdown is reported in Table 1.
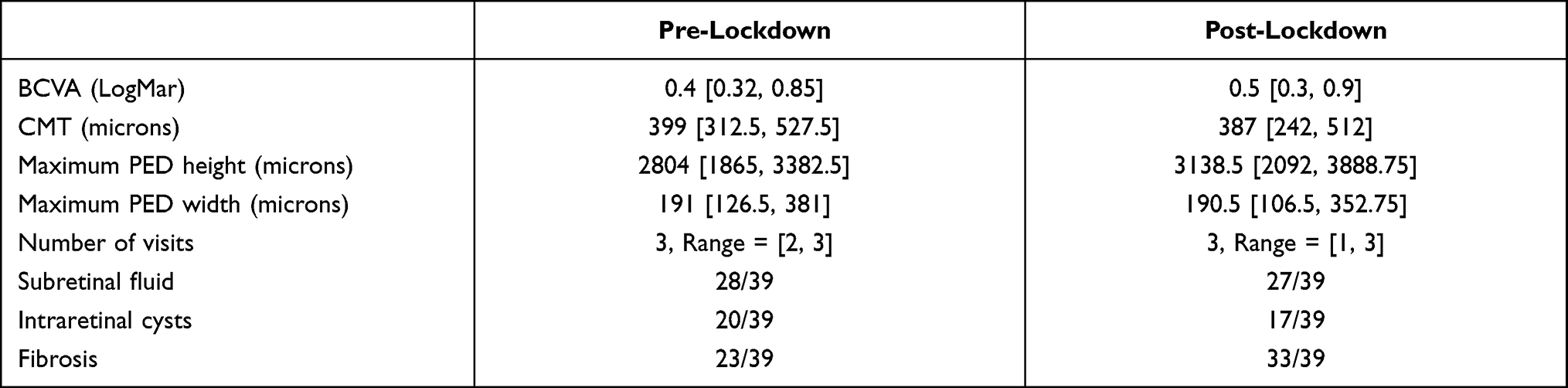 |
Table 1 Descriptive Statistics at First Visit for the Pre- and Post-Lockdown Periods. All Continuous Variables are Reported as Median [Interquartile Range] Except for the Number of Visits Which is Reported as Median [Range] |
The CMT was a significant predictor of the BCVA (p = 0.043). We found a significant, albeit small, reduction in the BCVA predicted controlling for CMT between the pre- and post-lockdown (Estimate [95% Confidence Intervals] = 0.09 [0.02, 0.16] logMAR, p = 0.0201). Of notice, when the time from the first visit was included as a covariate, this was not significant (p = 0.216) but the difference between pre- and post-lockdown retained its significance (p = 0.012). This difference can be visualised by plotting the individual predictions from the mixed effect model (including random effects) as if all the measurements had been performed in the pre-lockdown period (Figure 1). As expected, the predictions lie on the identity line for the pre-lockdown period. However, a large number of predictions were worse than expected for the corresponding CMT in the post-lockdown period. Indeed BCVA significantly dropped after the lockdown compared to before the lockdown but this drop is likely not due only to a change in CMT because BCVA values are lower than predicted based on CMT values.
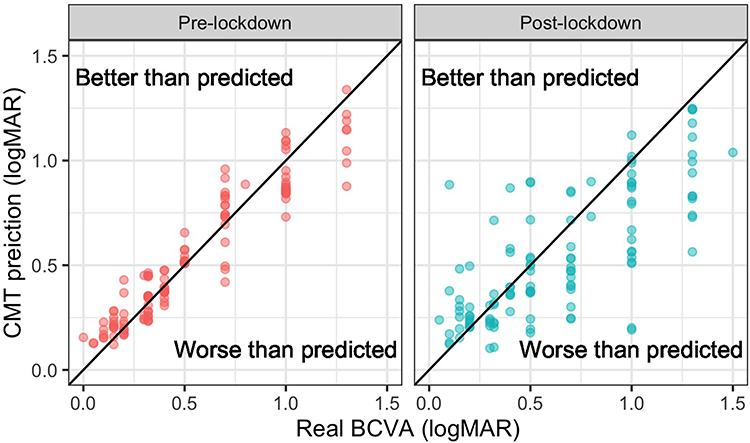 |
Figure 1 Predictions from the mixed effect model as if all measurements had been performed in the pre-lockdown period. The solid diagonal line represents the identity (perfect prediction). Observations below the diagonal line indicate observed best-corrected visual acuity (BCVA) values worse than predicted from the central macular thickness (CMT). |
There was no significant change in either the maximum height (p = 0.195) or width (p = 0.39) of the PED between the pre- and post-lockdown measurements. Twenty-three patients had fibrosis at baseline. Of the remaining 16, 4 converted to fibrosis in the before the lockdown and 9 after the lockdown. However, people who converted to fibrosis in the post-lockdown did not show a significantly different loss in BCVA compared those who did not convert (p = 0.464).
The average time interval between the last visit before the lockdown and the first visit after the lockdown was 130 ± 30 days (Mean ± SD), compared to average 103 ± 97 between the two last visits before lockdown. However, this change in interval did not have a significant effect when used as a predictor in the linear mixed model (p = 0.309).
When measured through mixed effect logistic regression, there was no significant change in the frequency of observed SRF (p = 0.369) and IRC (p = 0.525) between the two time intervals.
No adverse events were reported during the examined period.
Discussion
The aim of this study was to analyze anatomical and functional outcomes after forced interruption-in-care in patients undergoing treatment for nAMD with anti-VEGF intravitreal therapy.
In order to effectively evaluate the effect of our recovery strategy a mixed effect model was built (Figure 1). Importantly, with our model, we were able to show the average functional loss accounting for variations in CMT. This is important, because changes in BCVA due to accumulation of retinal fluid after the interruption-in-care were expected. However, a more pressing issue pertains the visual recovery that can be achieved once treatment has been re-instated and retinal fluid has been reabsorbed. This is what we measured in our analysis. As previously mentioned, BCVA significantly dropped after the lockdown compared to before the lockdown but this drop is likely not due only to a change in CMT because BCVA values are lower than predicted based on CMT values.
On average, the pandemic lengthened the interval between injections by almost a months. For some patients, however, the interval was actually shorted compared to the last interval recorded before the pandemic. This was a consequence of our chosen recovery strategy of starting a new loading phase of bevacizumab, one injection per month for three months. However, this makes it difficult to clearly attribute the observed changes to the increased waiting time. Indeed, we could not observe any significant change between the increase in treatment interval and the functional loss (p = 0.309). Indeed, loading phase of Bevacizumab in patients with AMD has previously demonstrated to moderately reduce long-term visual loss.13
In order to individuate other causes for the observed worsening, we analyzed different parameters on the OCT scan. Firstly, since FA at follow-ups and Optical Coherence Tomography Angiography (OCTA) were not available, we measured PED dimension (height and width) as an indirect parameter of CNV dimension. Indeed, RPE lesions may provide useful insights in CNV assessment but are poorly identified by the conventional OCT systems.14 Our results did not found a statistically significant change in these dimensions before and after interruption. Of course, being a surrogate and indirect measurement of CNV size, PED dimensions do not account for the size of the actual CNV lesion. Moreover, our measurements were based only on one central (foveal) scan and the para-foveal feature of the lesion were not evaluated.
Fibrosis is associated with worse BCVA.15 Therefore, we analyzed the presence and progression to fibrosis in our sample. However, we could not find any statistically significant association between patients who converted to fibrosis in the post-lockdown and patients who did not in terms of worse visual outcome.
Lastly, we assessed subretinal fluid and intraretinal cysts, previous studies have shown that amount of subretinal fluid correlate positively with BCVA.16 Intraretinal cysts are known to correlate with worse BCVA.17 Of course, this would be included in our measurement of CMT, and we did not find any statistical difference between frequencies pre and post lockdown for both subretinal fluid and intraretinal cysts.
Consequences of interruption in treatment of anti-VEGF are well established in literature. Lad et al investigated the suspension rates between two groups treated with anti-VEGF injections for nAMD. Their findings indicated that the rate of anti-VEGF injection was 57% in the first 12 months, as well as 71% after 24 months. These results confirmed that in clinical practice, the approach recommended by clinical trial evidence is sometimes disattended.18
Kim et al noticed a remarkable deterioration in BCVA associated with intraretinal fluid in 35 patients with nAMD after discontinuing intravitreal anti-VEGF for 24-months.19
Recently, Soares et al found after a loss to follow-up for more than 6 months with a worsening in BCVA from a baseline median Snellen of 20/80 to a median Snellen of 20/200, in spite of the OCT macular improvements.20
In addition, Ramakrishnan et al, considering the compliance to the follow-up consultations, stratified patients into 3 groups; the outcome revealed poor results in the groups where the follow-up was done after 36 days as compared with patients seen on time (≤35 days).21
Since extending the injection interval is applied by many centers during the pandemic, Teo KYC et al investigated this protocol and found that there was a significant short-term risk to vision when retreatment interval was extended beyond 12 weeks, hence extensions over 12 weeks should be avoided.22
Tyler E. Greenlee et al, in a study of 2020, evaluated the outcomes of patients which experienced interruption in treatment with anti-VEFG injections for nAMD. Particularly, the latter study demonstrated the importance of frequent follow-up once retinal fluid is ascertain, in order to eschew deferral in treatment. Moreover, this study denoted that the time range to determine long-lasting damages is brief, with the mean interruption length of 5 ± 3.7 months and a prevalent interruption length of 3–4 months.23
Our results are in agreement with Stone et al, who reported that eyes with nAMD experienced the greatest loss of vision with treatment delay, and nAMD eyes were less likely to return to baseline on restarting treatment, indeed in this study 74.6% of nAMD patients returned to a BCVA within 5 letters of their baseline.24
Sekeroglu et al report that visual acuity due to interruption was positively correlated with number of intravitreal anti-VEGF injections at last 6 months before COVID-19 pandemic and central subfoveal thickness at first post-COVID-19 visit; and negatively correlated with follow-up duration.25
All these studies indicate that a interruption in treatment are likely to produce worsening of BCVA despite satisfactory re-absorption of retinal fluid on OCT scans. Of course, our average interruption in treatment was much smaller than those reported and observed in previous studies where a significant effect was described. This was an expected outcome of our recovery strategy, which proved successful in this sense. Despite this, we observed a statistically significant visual loss. Of course, one major limitation of our analysis is that we were not able to disentangle the effect of lockdown from the natural evolution of the disease. Another limitation was the relatively small sample size, with might have prevented the detection of other significant factors in the final outcome. Moreover, the lack of FA and OCTA assessment did not allow to perform a more reliable measurement of the CNV. Unfortunately, these are not part of the standard evaluation performed in our clinics for follow-ups of CNVs.
Other features of the analysis need to be kept in mind when interpreting our results. These are not necessarily limitations but rather intrinsic and unavoidable characteristics of the phenomenon under study. For example, being an unexpected event, studying the effect of a pandemic needs to rely on retrospective analyses, such as ours. Moreover, the evaluation of the effect interruption could not benefit from the presence of a control group with continued anti-VEGF regimen, since the interruption itself was not programmed and applied to our entire cohort of patients indiscriminately.
In conclusion, different guidelines indicated the necessity of continuing intravitreal injections,26 in the forecast of future measures to control COVID-19 pandemic waves we warn about the risks of suspending anti-VEGF therapy and highlight the importance of treatment consistency. Indeed, despite our efforts to minimize the impact of interruption, we could still detect a significant loss in visual function, despite good structural recovery. The magnitude of the average loss was, however, small and this can be viewed as a partially successful outcome.
Acknowledgments
We acknowledge Mrs. Alison Rhodes for revising the English language in the manuscript.
Funding
No additional funding was received for this article.
Disclosure
Professor Mario Romano reports grants, personal fees from Alcon, Bausch and Lomb, Alfaintes, Novartis, Hoya, and Sooft, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Mitchell P, Liew G, Gopinath B, Wong TY. Seminar age-related macular degeneration. Lancet. 2018;392:1147–1159. doi:10.1016/S0140-6736(18)31550-2
2. Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP. Ranibizumab versus Verteporfin Photodynamic Therapy for Neovascular Age-Related Macular Degeneration: two-Year Results of the ANCHOR Study. Ophtha. 2008;116:57–65.e5. doi:10.1016/j.ophtha.2008.10.018
3. Kaiser PK, Chung CY, Kim RY, Study M. Ranibizumab for neovascular age-related macular degeneration. New England Journal. 2006;355:1419–1431.
4. Berg K, Hadzalic E, Gjertsen I, et al. Ranibizumab or Bevacizumab for Neovascular Age-Related Macular Degeneration According to the Lucentis Compared to Avastin Study Treat-and-Extend Protocol Two-Year Results. Ophthalmology. 2015;1–9. doi:10.1016/j.ophtha.2015.09.018
5. Group CR. Ranibizumab and Bevacizumab for Treatment of Neovascular Age-related Macular Degeneration. Ophtha. 2012;119:1388–1398. doi:10.1016/j.ophtha.2012.03.053
6. Chakravarthy PU, Harding PSP, Rogers CA, et al. Alternative treatments to inhibit VEGF in age-related choroidal neovascularisation: 2-year fi ndings of the IVAN randomised controlled trial. Lancet. 2013;382:1258–1267. doi:10.1016/S0140-6736(13)61501-9
7. Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K. Seven-Year Outcomes in Ranibizumab-Treated Patients in ANCHOR, MARINA, and HORIZON A Multicenter Cohort Study (SEVEN-UP). Ophthalmology. 2013;120(11):2292–2299. doi:10.1016/j.ophtha.2013.03.046
8. Cable J, Heymann DL, Uzicanin A, et al. Concise Original Report Pandemic diseases preparedness and response in the age of COVID-19 — a symposium report. Ann New York Acad Sci. 2020:9:1–13. doi:10.1111/nyas.14534
9. Romano MR, Montericcio A, Montalbano C, et al. Facing COVID-19 in Ophthalmology department. Curr Eye Res. 2020;45(6):653–658. doi:10.1080/02713683.2020.1752737
10. Schmidt-Erfurth U, Waldstein SM. A paradigm shift in imaging biomarkers in neovascular age-related macular degeneration. Prog Retin Eye Res. 2016;50:1–24. doi:10.1016/j.preteyeres.2015.07.007
11. Souied EH, Addou-Regnard M, Ohayon A, et al. Spectral-Domain Optical Coherence Tomography Analysis of Fibrotic Lesions in Neovascular Age-Related Macular Degeneration. Am J Ophthalmol. 2020;214:151–171. doi:10.1016/j.ajo.2020.02.016
12. Sahni J, Stanga P, Wong D, Harding S. Optical coherence tomography in photodynamic therapy for subfoveal choroidal neovascularisation secondary to age related macular degeneration: a cross sectional study. Br J Ophthalmol. 2005;89:316–320. doi:10.1136/bjo.2004.043364
13. Menon G, Chandran M, Sivaprasad S, Chavan R, Narendran N, Yang Y. Is it necessary to use three mandatory loading doses when commencing therapy for neovascular age-related macular degeneration using bevacizumab? (BeMOc Trial). Eye. 2013;27:959–963. doi:10.1038/eye.2013.93
14. Ahlers C, Simader C, Geitzenauer W, et al. Automatic segmentation in three-dimensional analysis of fibrovascular pigmentepithelial detachment using high-definition optical coherence tomography. Br J Ophthalmol. 2008;92:197–203. doi:10.1136/bjo.2007.120956
15. Willoughby AS, Ying G-S, Toth CA, et al. Subretinal hyperreflective material in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2015;122:1846–53.e5. doi:10.1016/j.ophtha.2015.05.042
16. Waldstein SM, Simader C, Staurenghi G, et al. Morphology and Visual Acuity in Aflibercept and Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration in the VIEW Trials. Ophthalmology. 2016;123:1521–1529. doi:10.1016/j.ophtha.2016.03.037
17. Waldstein SM, Philip A-M, Leitner R, et al. Correlation of 3-dimensionally quantified intraretinal and subretinal fluid with visual acuity in neovascular age-related macular degeneration. JAMA Ophthalmol. 2016;134:182–190. doi:10.1001/jamaophthalmol.2015.4948
18. Lad EM, Hammill BG, Qualls LG, Wang F, Cousins SW, Curtis LH. Anti-VEGF treatment patterns for neovascular age-related macular degeneration among medicare beneficiaries. Am J Ophthalmol. 2014;158:537–43.e2. doi:10.1016/j.ajo.2014.05.014
19. Kim JH, Chang YS, Kim JW. Natural course of patients discontinuing treatment for age-related macular degeneration and factors associated with visual prognosis. Retina. 2017;37:2254–2261. doi:10.1097/iae.0000000000001494
20. Soares RR, Mellen P, Garrigan H, et al. Outcomes of eyes lost to follow-up with neovascular age-related macular degeneration receiving intravitreal anti-vascular endothelial growth factor. Ophthalmol Retin. 2020;4:134–140. doi:10.1016/j.oret.2019.07.010
21. Ramakrishnan MS, Yu Y, VanderBeek BL. Association of visit adherence and visual acuity in patients with neovascular age-related macular degeneration: secondary analysis of the comparison of age-related macular degeneration treatment trial. JAMA Ophthalmol. 2020;138:237–242. doi:10.1001/jamaophthalmol.2019.4577
22. Teo KYC, Nguyen V, Barthelmes D, Arnold JJ, Gillies MC, Cheung CMG. Extended intervals for wet AMD patients with high retreatment needs: informing the risk during COVID-19, data from real-world evidence. Eye. 2020;1–9. doi:10.1038/s41433-020-01315-x
23. Greenlee TE, Wang VY, Kang H, et al. Consequences of interruptions in treatment with vascular endothelial growth factor inhibitors in neovascular age-related macular degeneration in routine clinical practice. Retina. 2020. doi:10.1097/IAE.0000000000002888
24. Stone LG, Grinton ME, Talks JS. Delayed follow-up of medical retina patients due to COVID-19: impact on disease activity and visual acuity. Graefe’s Arch Clin Exp Ophthalmol. 2021;259:1773–1780. doi:10.1007/s00417-021-05174-4
25. Sekeroglu MA, Kilinc Hekimsoy H, Horozoglu Ceran T, Doguizi S. Treatment of neovascular age related macular degeneration during COVID-19 pandemic: the short term consequences of unintended interruptions. Eur J Ophthalmol. 2021;11206721211010612. doi:10.1177/11206721211010613
26. Korobelnik J-F, Loewenstein A, Eldem B, et al. Guidance for anti-VEGF intravitreal injections during the COVID-19 pandemic. Graefe’s Arch Clin Exp Ophthalmol. 2020:1–8. doi:10.1007/s00417-020-04703-x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.