Back to Journals » Journal of Pain Research » Volume 18
Short-Term Efficacy of Vitapex Paste in Single-Visit Root Canal Treatment for Acute Irreversible Pulpitis: A Retrospective Cohort Study
Authors Liu J, Li F, Liang X, Niu J
Received 15 September 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:18 Pages 7043—7052
DOI https://doi.org/10.2147/JPR.S563507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Keith
Jia Liu,1 Fangfei Li,2 Xiaolong Liang,1 Jiahui Niu1
1Department of Stomatology, Shijiazhuang Second Hospital, Shijiazhuang, 050000, People’s Republic of China; 2The Second Outpatient Department of the Provincial Organs of Hebei Province, Shijiazhuang, 050000, People’s Republic of China
Correspondence: Jia Liu, Email [email protected]
Background: The selection of root canal obturation material is critical for the successful management of acute irreversible pulpitis. Vitapex, an iodoform-calcium hydroxide-based paste, possesses recognized antimicrobial and biocompatible properties. However, comprehensive evidence comparing its efficacy in single-visit root canal treatment against the conventional gutta-percha/zinc oxide-eugenol (ZOE) sealer combination remains relatively limited.
Objective: To compare the clinical efficacy of Vitapex paste versus gutta-percha/ZOE sealer in single-visit root canal treatment for acute irreversible pulpitis.
Methods: In this single-center retrospective cohort study, clinical data from 112 patients with acute irreversible pulpitis who underwent single-visit root canal therapy between April 2022 and August 2024 were analyzed. Patients were allocated into two groups based on the obturation material: the Vitapex group (n=56), obturated with Vitapex paste, and the gutta-percha/ZOE group (n=56), obturated using the cold lateral compaction technique with gutta-percha points and ZOE sealer. Key outcome measures included time to pain relief, time to swelling resolution, time to return to normal masticatory function, Visual Analogue Scale (VAS) scores, bite force, chewing efficiency, levels of inflammatory factors (hs-CRP, IL-6, TNF-α), periodontal health indices (Bleeding Index-BI, Plaque Index-PLI, Probing Depth-PD), and the incidence of adverse reactions.
Results: The Vitapex group showed significantly shorter recovery times for pain relief, swelling resolution, and return to normal function (all P< 0.001), significantly lower VAS scores at 1 and 4 weeks (P< 0.05), and greater improvements in masticatory function at 4 weeks (P< 0.05). Inflammatory markers and periodontal health indices improved more significantly with Vitapex (all P< 0.001). The adverse reaction rate was lower with Vitapex (5.4% vs 12.5%), though not statistically significant (P=0.325).
Conclusion: Vitapex demonstrates superior outcomes in single-visit treatment for irreversible pulpitis, offering faster recovery, better pain control, improved function, and reduced inflammation compared to gutta-percha/ZOE, making it a valuable clinical alternative.
Keywords: irreversible pulpitis, vitapex, root canal treatment, pain, masticatory function, inflammatory mediators, periodontal health
Introduction
Acute irreversible pulpitis is a common and painful dental condition primarily caused by bacterial invasion of the pulp tissue through caries or trauma. It is characterized by spontaneous, nocturnal, and radiating pain, often leading to pulp necrosis and subsequent apical periodontitis if not treated promptly.1,2 The primary goals of management are to alleviate pain and eliminate infection.
Root canal therapy is the standard of care. While traditional multi-visit approaches with interim medication have been widely used, single-visit root canal treatment (SRCT) has gained prominence due to its advantages in reducing treatment time, minimizing the risk of inter-appointment contamination, and improving patient compliance.3,4 However, the choice of obturation material in SRCT, particularly for teeth with acute pulpal inflammation, is crucial as it directly influences postoperative healing and pain experience.5
The gutta-percha/zinc oxide-eugenol (ZOE) sealer combination, applied using cold lateral compaction, remains a widely accepted standard for root canal obturation, providing excellent mechanical seal.6 In contrast, Vitapex, an injectable paste composed of calcium hydroxide, iodoform, and silicone oil, offers a distinct approach. Its antimicrobial efficacy stems from the sustained release of hydroxyl ions and iodoform, while its high flowability promises superior adaptation to complex root canal anatomy.7,8 Although Vitapex is well-established in pediatric endodontics, its efficacy in SRCT for acute irreversible pulpitis in permanent teeth, particularly in direct comparison to the standard gutta-percha/ZOE technique, has not been thoroughly investigated.
Therefore, this retrospective cohort study aimed to compare the clinical and biochemical outcomes of SRCT for acute irreversible pulpitis using Vitapex paste versus the conventional gutta-percha/ZOE obturation system. We hypothesized that Vitapex would demonstrate superior performance in accelerating postoperative recovery and reducing inflammation.
Materials and Methods
Study Design and Participants
This single-center, retrospective cohort study analyzed the clinical data of 112 patients with acute irreversible pulpitis who underwent single-visit root canal therapy at our hospital between April 2022 and August 2024. A priori sample size calculation was performed using G*Power software (version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Germany). Based on an anticipated effect size of 0.8 for the primary outcome (pain reduction), an alpha level of 0.05, and a power of 0.95, the minimum required sample size was 52 patients per group. Our final sample of 56 per group exceeds this requirement. The patients were allocated into two groups based on the root canal obturation material used: an Vitapex group (n=56) obturated with Vitapex paste, and a gutta-percha/ZOE group (n=56) obturated with gutta-percha and zinc oxide-eugenol sealer.
The inclusion criteria were as follows: (1) Meeting the diagnostic criteria for acute irreversible pulpitis, confirmed by clinical examination and periapical radiography;9 (2) Age between 18 and 65 years; (3) Teeth with complete root apex formation, as verified by clinical and radiographic examination, and suitable for root canal therapy; (4) Single-tooth involvement, primarily single- or double-rooted teeth (including molars and premolars) with restorable crowns and no significant crown structure loss compromising coronal seal; (5) Patients able to comply with the treatment and follow-up schedule.
The exclusion criteria included: (1) Concurrent severe periodontitis, root fracture, or combined endodontic-periodontal lesions; (2) History of using immunomodulators, anti-inflammatory analgesics, or antibiotics within the past month; (3) Severe systemic diseases (eg, diabetes, cardiovascular diseases, tumors) or mental disorders that could affect compliance; (4) Pregnancy or lactation; (5) Incomplete treatment or inadequate follow-up data.
This study was approved by the Institutional Review Board/Ethics Committee of our hospital. The requirement for informed consent was waived due to the retrospective nature of the study, in compliance with the ethical principles of the Declaration of Helsinki.
Treatment Methods
All endodontic treatments were performed by one of four qualified general dentists from the Department of Stomatology at our hospital. Each operator had over three years of clinical experience and had received systematic, standardized training in root canal therapy techniques prior to the study commencement. To minimize inter-operator variability, all operators followed the same detailed clinical protocol, and a calibration session was conducted to ensure consistency in procedures like access cavity preparation, working length determination, and obturation. The potential influence of operator variability on outcomes is addressed in the Discussion.
All patients in both groups received single-visit root canal treatment. Prior to treatment, all patients received a comprehensive oral examination to identify the affected tooth’s position, extent of caries, pulp status, and periapical condition. Standard periapical radiographs were taken using a digital X-ray system (Vatech Co., Ltd., Republic of Korea, Model: EzRay Air) to assess root canal morphology, number, length, and the presence of any periapical lesions. The appropriate method of local anesthesia (infiltration or block anesthesia) was selected based on the individual case. An optimal access point was chosen on the affected tooth, and the pulp chamber was opened using a high-speed dental handpiece (Guilin Woodpecker Medical Instrument Co., Ltd., Registration No.: Gui Xie Zhu Zhun 20172170005, Model: HL11-M4). The pulp chamber roof was completely removed to fully expose the chamber. Subsequently, high-speed dental burs (Shanghai Jinxu Biotechnology Co., Ltd. Luohe Branch, Registration No.: Yu Xie Zhu Zhun 20172550584, Model: 012) were used to refine the pulp chamber walls and establish a straight-line access path.
Root canal debridement was performed using ProTaper Gold nickel-titanium rotary file system (Dentsply Sirona, USA, Ref: RXGLLSIZE) accompanied by irrigation with chlorhexidine acetate solution (Baoding Aihui Pharmaceutical Co., Ltd., National Medicine Approval No. H11021863, Specification: 0.02%) to progressively remove infected pulp tissue, bacteria, and necrotic debris from the root canal system. The working length of the root canal was determined using an electronic apex locator (VDW GmbH, Registration No.: Guo Zhu Jin 20162175192, Model: Raypex 6). Subsequently, the root canals were progressively enlarged and shaped using the aforementioned nickel-titanium instrument systems to create smooth walls with an appropriate taper. During the instrumentation process, alternating irrigation with normal saline and 1% sodium hypochlorite solution (Cattani France S.A.S., France, Lot: 8C295) was performed to prevent canal blockage, with a final irrigation volume of 5–10 mL per canal.10 After preparation was complete, the canals were irrigated again with chlorhexidine acetate solution. Absorbent paper points (Dentsply Sirona, USA) were then used to dry the canals.
For the obturation phase, the two groups differed as follows: Vitapex group: Vitapex paste (DiaDent Group International, Korea, Lot: 230512; primary components: iodoform 40.4%, calcium hydroxide 30.3%, silicone oil 22.4%) was selected. Using a dedicated root canal filling device (Ormco Corporation also trading as SybronEndo, Registration No.: Shi Yao Jian Xie (Jin) Zi 2009 No. 1062553, Model: 974–0058), the paste was slowly injected into the canal. Filling proceeded from the apex coronally until the paste reached the canal orifice, ensuring the paste filled the entire root canal system.11 A post-obturation radiograph was taken to verify the quality of the fill, confirming it was dense, without voids, and with slight extrusion beyond the apical foramen considered acceptable for this calcium hydroxide-based paste. Gutta-percha/ZOE group: The root canals were obturated using the cold lateral compaction technique with standardized gutta-percha points (Dentsply Sirona, USA) and a zinc oxide-eugenol sealer (Dentsply Sirona, USA, Product: Pulpdent Root Canal Sealer). The quality of obturation was verified radiographically, confirming it was dense and without voids.
Following obturation, the procedure was identical for both groups: The cavity was sealed with a glass-ionomer cement base (GC Corporation, Tokyo, Japan, Product: Fuji IX) and restored with light-cured resin composite (3M ESPE, USA, Product: Filtek Z350 XT). The occlusion was adjusted. Full crown restoration was performed 1–2 weeks later.
Evaluation Indicators and Vitapex Group Methods
(1) Primary clinical outcomes: The time to pain relief (defined as the patient reporting a VAS score ≤2), time to swelling resolution (assessed clinically), and time to return to normal masticatory function (patient-confirmed) were recorded.
(2) Pain level assessment: The Visual Analogue Scale (VAS)12 was used to assess pain, scored from 0 to 10, with 0 indicating no pain and 10 indicating unbearable severe pain. The VAS is a validated and widely used tool for subjective pain measurement in dental pain studies.13 Evaluations were conducted Before Treatment, 1 Week After Treatment, and 4 Weeks After Treatment.
(3) Chewing function testing: Occlusal force on the affected side was measured using a T-Scan digital occlusal analysis system (Tekscan Inc., USA, Model: T-Scan III). Patients bit down 10 times, 2 seconds per bite, continuously. The average of the top 3 maximum values was recorded as the occlusal force. Chewing efficiency was assessed using the peanut sieve-weighing method: Chewing efficiency = (Weight difference before and after chewing / Weight before chewing) × 100%. Measurements were taken Before Treatment and 4 Weeks After Treatment.
(4) Inflammatory factor detection: Gingival crevicular fluid (GCF) samples were collected from the gingival sulcus of the affected tooth using standardized paper strips (Periopaper, OraFlow Inc., USA). After isolating the tooth and gently drying it, the paper strip was inserted 1–2 mm into the sulcus for 30 seconds. Strips contaminated with blood or saliva were discarded. Uncontaminated samples were placed into sterile Eppendorf tubes containing 15% phosphate-buffered saline (PBS). The tubes were then mechanically shaken on a horizontal shaker (Labnet International, Inc., USA, Model: Orbit 1000) at 150 rpm for 1 hour at room temperature, followed by centrifugation at 4°C (3000 rpm, 8 cm radius) for 15 minutes. The supernatant was collected and stored at −80°C until analysis. Levels of high-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) were quantified using commercial enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, USA, Catalog #: DCRP00D, D6050, DTA00D respectively) according to the manufacturers’ instructions.
(5) Periodontal health assessment: Included bleeding index (BI),14 plaque index (PLI),15 and probing depth (PD).16 All periodontal examinations were performed by a single calibrated periodontist who was blinded to the patient’s group assignment. Intra-examiner reliability was assessed by duplicate measurements in 10% of the patients, showing a Cohen’s kappa coefficient of >0.85 for BI and PLI, and an intraclass correlation coefficient of >0.90 for PD.
① BI: The probe was inserted >1 mm subgingivally to observe bleeding and rated on a 5-point scale: 0 = No redness or bleeding; 1 = Redness without bleeding; 2 = Punctate bleeding; 3 = Linear bleeding; 4 = Bleeding overflows from gingival sulcus; 5 = Spontaneous bleeding.
② PLI: Plaque amount was rated on a 4-point scale: 0 = No plaque; 1 = No visible plaque but a small amount removable with a probe; 2 = Moderate visible plaque; 3 = Large amount of visible soft deposits.
③ PD: The distance from gingival margin to the bottom of the pocket at 6 points (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual, disto-lingual) of the affected tooth was measured using a Williams periodontal probe (Hu-Friedy, USA). The average value was recorded. Assessed Before Treatment and 4 Weeks After Treatment.
(6) Radiographic assessment: Periapical radiographs were taken at the 4-week follow-up using the long-cone parallel technique and the same digital X-ray system as baseline. Radiographs were assessed by two independent, experienced endodontists who were blinded to the clinical groups. They evaluated the presence or absence of a periapical radiolucency and the quality of the root canal filling (homogeneity, apical extent). Any disagreements were resolved by consensus.
(7) Adverse reaction recording: Post-treatment adverse events were monitored, including but not limited to persistent postoperative pain, local swelling, allergic reactions, and periapical periodontitis. All adverse events were uniformly recorded by hospital medical staff.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA) was used for generating figures. The normality of the distribution for all continuous variables was confirmed using the Shapiro–Wilk test. Categorical data were expressed as numbers and percentages (%) and analyzed using the Chi-square (χ2) test or Fisher’s exact test as appropriate. Continuous data were expressed as mean ± standard deviation (SD). Independent samples t-test was used for between-group comparisons of normally distributed continuous data. Paired samples t-test was used for within-group comparisons (Before vs After Treatment). For VAS scores measured at multiple time points, repeated-measures analysis of variance (ANOVA) followed by Bonferroni post-hoc test was applied. P < 0.05 was considered statistically significant.
Results
Comparison of General Information
There were no statistically significant differences between the two groups in terms of gender, age, body mass index (BMI), smoking history, or affected tooth location (P > 0.05), indicating comparability. See Table 1.
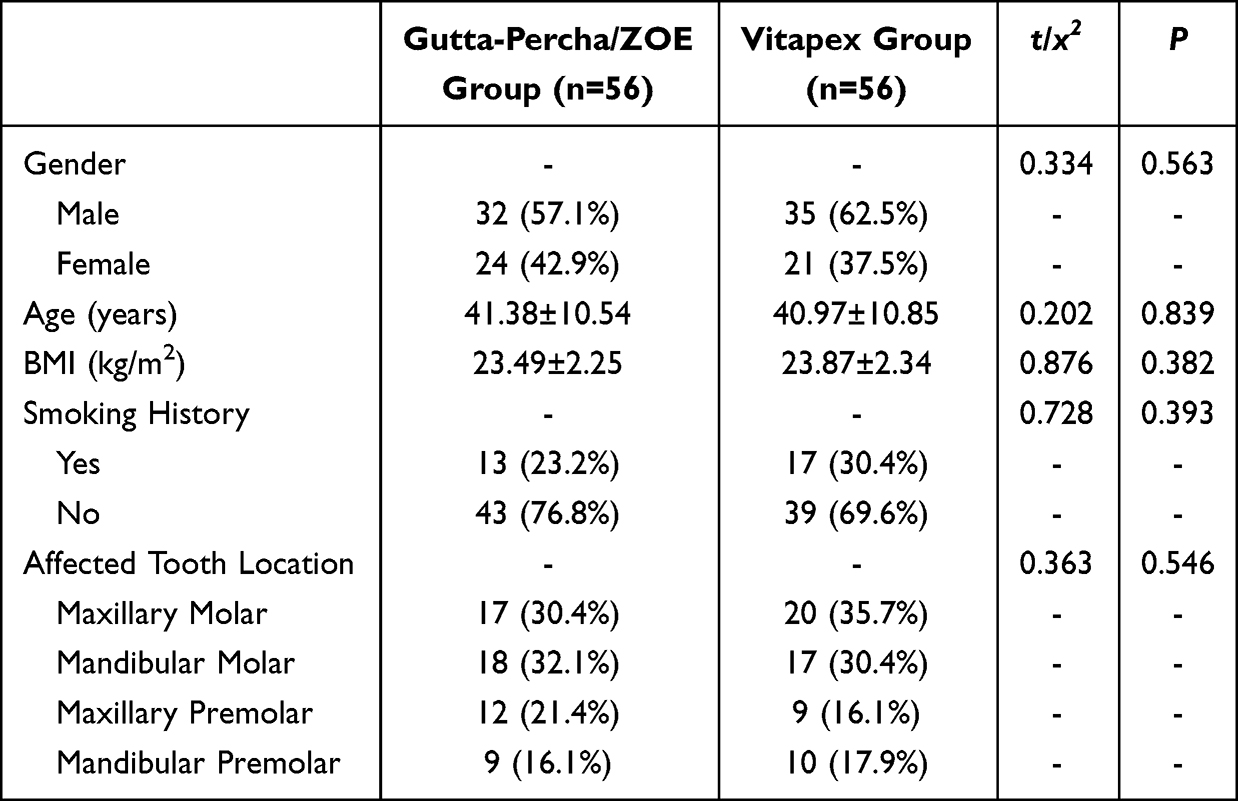 |
Table 1 Comparison of General Information |
Comparison of Recovery Time Indices
The Vitapex group demonstrated significantly shorter times to pain relief, swelling resolution, and return to normal masticatory function compared to the gutta-percha/ZOE group (all P < 0.001). See Table 2.
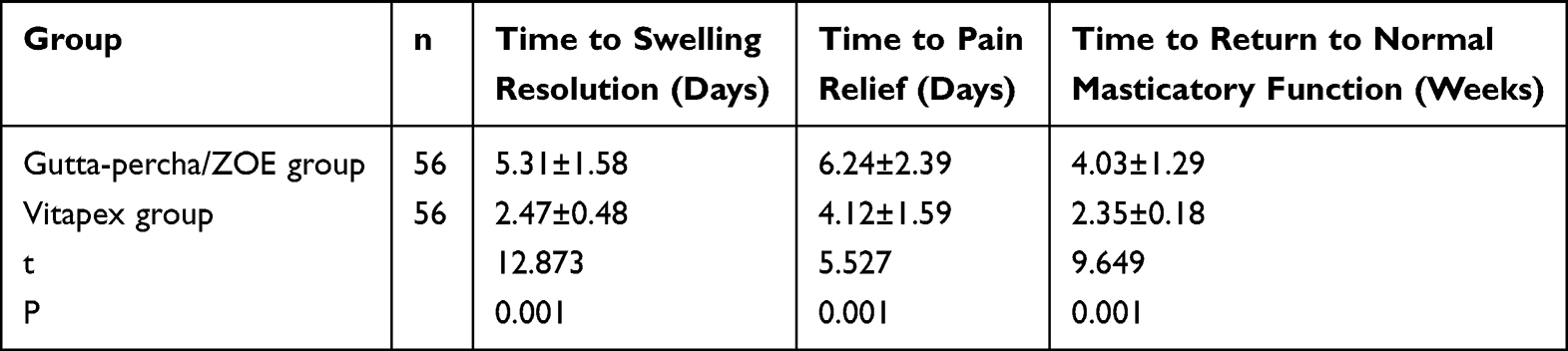 |
Table 2 Comparison of Recovery Time Indices Between the Two Groups |
Comparison of Pain Levels
Repeated-measures ANOVA of VAS scores revealed significant effects for group (F = 14.783, P < 0.001), time (F = 136.891, P < 0.001), and the group-time interaction (F = 67.326, P < 0.001). Post-hoc tests showed that within each group, VAS scores at 1 week and 4 weeks post-treatment were significantly lower than the pre-treatment scores, and scores at 4 weeks were lower than at 1 week (all P < 0.05). Between-group comparisons at each time point showed no significant difference at baseline (P > 0.05). However, the Vitapex group had significantly lower VAS scores than the gutta-percha/ZOE group both at 1 week and 4 weeks after treatment (P < 0.05). See Figure 1.
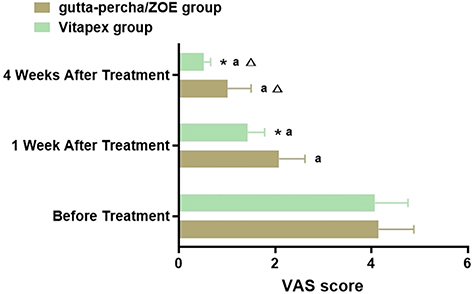 |
Figure 1 Comparison of Pain Levels. Note: Between-group comparison at the same time point, *P < 0.05; Compared with same group Before Treatment, aP < 0.05; Compared with same group 1 Week After Treatment, ΔP < 0.05. |
Comparison of Masticatory Function
At 4 weeks post-treatment, bite force and chewing efficiency significantly increased from baseline in both groups (P < 0.05). The improvement in both bite force and chewing efficiency was significantly greater in the Vitapex group compared to the gutta-percha/ZOE group (P < 0.05). See Figure 2.
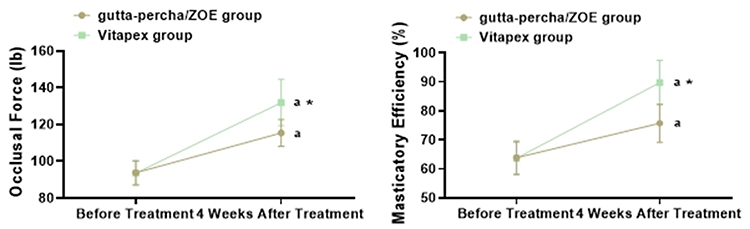 |
Figure 2 Comparison of Masticatory Function. Note: Between-group comparison, *P < 0.05; Compared with same group Before Treatment, aP < 0.05. |
Comparison of Inflammatory Factors
Before treatment, there were no significant differences in serum levels of hs-CRP, IL-6, and TNF-α between the two groups (P > 0.05). At 4 weeks post-treatment, the levels of all three inflammatory factors were significantly reduced in both groups compared to their pre-treatment levels (P < 0.05). The post-treatment levels of hs-CRP, IL-6, and TNF-α were all significantly lower in the Vitapex group than in the gutta-percha/ZOE group (all P < 0.001). See Table 3.
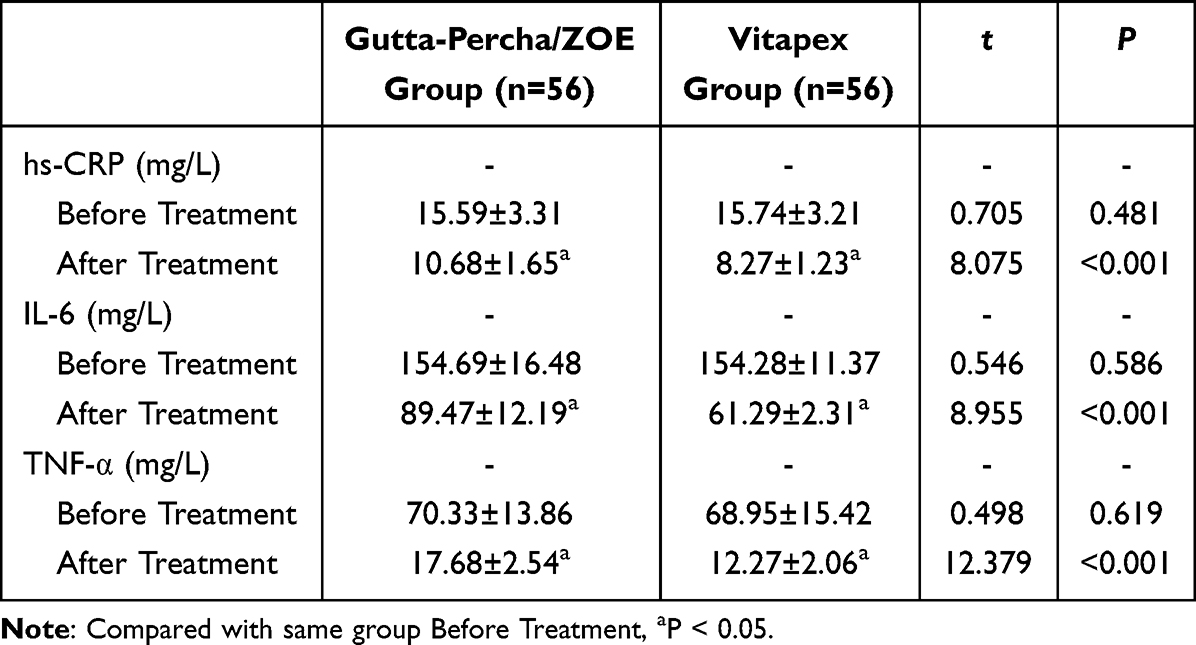 |
Table 3 Comparison of Inflammatory Factors |
Comparison of Periodontal Health
At 4 weeks post-treatment, all periodontal health indices (BI, PLI, PD) were significantly improved in both groups compared to pre-treatment levels (P < 0.05). The Vitapex group exhibited significantly lower post-treatment scores for BI, PLI, and PD compared to the gutta-percha/ZOE group (all P < 0.001). See Table 4.
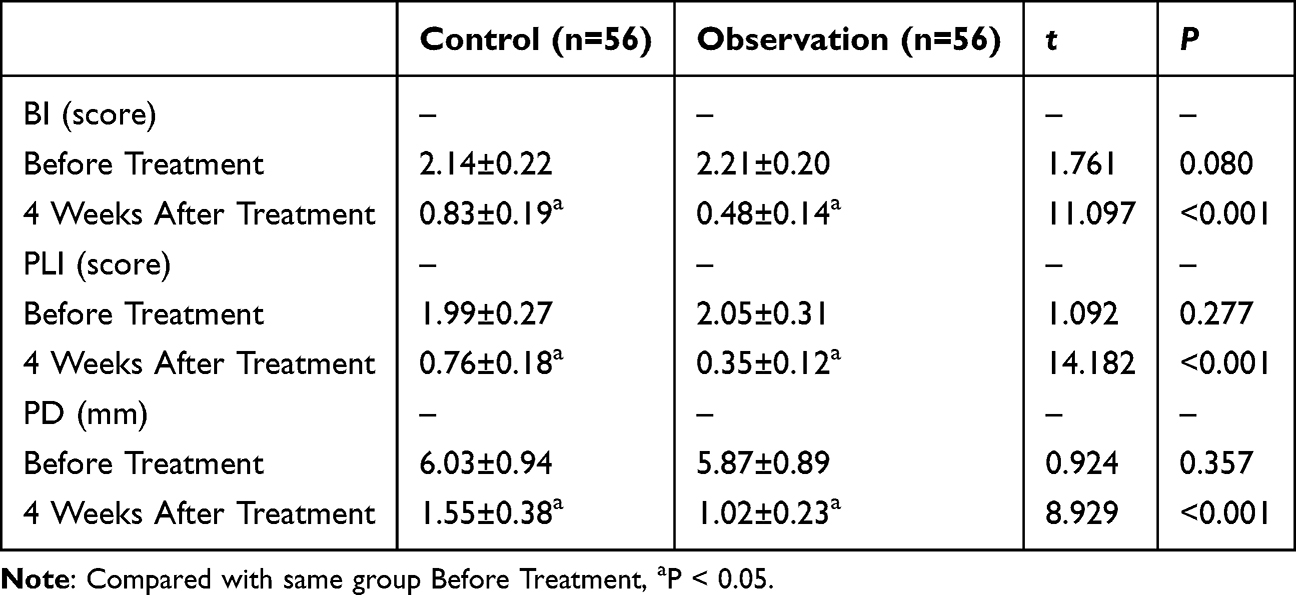 |
Table 4 Comparison of Periodontal Health |
Comparison of Adverse Reactions
The total incidence of adverse reactions was significantly lower in the Vitapex group (5.4%) compared to the gutta-percha/ZOE group (12.5%) (P = 0.325). See Table 5. See Table 5.
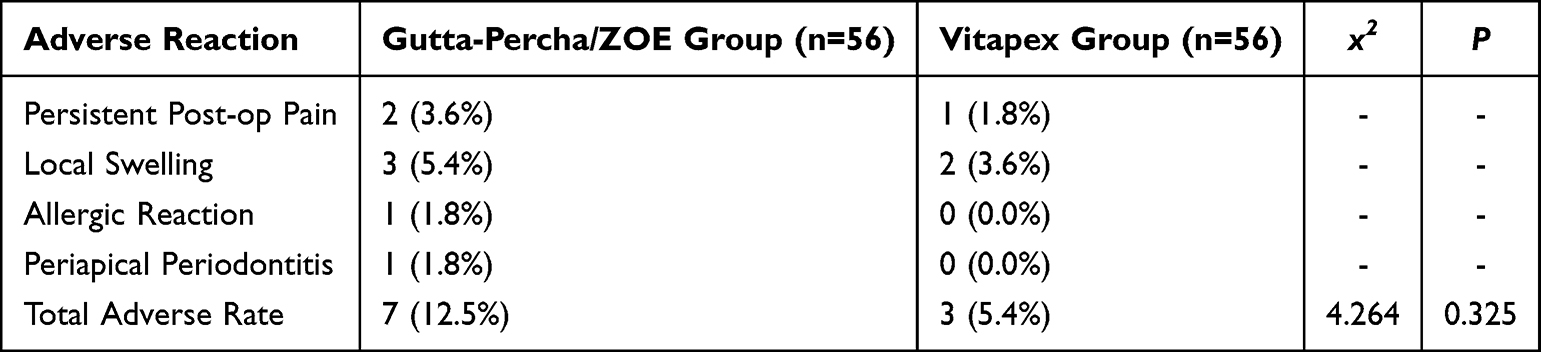 |
Table 5 Comparison of Adverse Reactions |
Discussion
The management of acute irreversible pulpitis necessitates effective root canal treatment, with the choice of obturation material being a critical determinant of postoperative healing, pain control, and long-term success.17 This retrospective cohort study demonstrates that single-visit root canal treatment obturated with Vitapex paste confers significant advantages over obturation with gutta-percha and a zinc oxide-eugenol (ZOE) sealer across multiple clinical parameters, including postoperative recovery, inflammatory resolution, and functional restoration.
Our primary findings indicate that the Vitapex group experienced a markedly accelerated recovery. The significantly shorter times to pain relief, swelling resolution, and return to normal masticatory function (Table 2) underscore the material’s superior efficacy in managing the acute phase of inflammation. This is further corroborated by the longitudinal pain assessment, which revealed significantly lower VAS scores in the Vitapex group at both 1-week and 4-week intervals post-treatment (Figure 1). This enhanced analgesic profile can be attributed to the distinct pharmacological properties of Vitapex. Its key component, iodoform, provides sustained broad-spectrum antimicrobial activity, effectively suppressing residual microorganisms within the root canal system and thereby reducing the inflammatory stimulus on the periapical tissues.18 Furthermore, the calcium hydroxide component creates a local alkaline environment that neutralizes inflammatory acids and may inactivate bacterial toxins, contributing directly to pain reduction.11 In contrast, while the cold lateral compaction with gutta-percha/ZOE provides an excellent mechanical seal, it lacks this sustained chemical antimicrobial and anti-inflammatory action, potentially explaining the slower symptomatic recovery in the gutta-percha/ZOE group.
Beyond symptomatic relief, the Vitapex group exhibited significantly greater improvements in masticatory function, as evidenced by higher post-treatment bite force and chewing efficiency (Figure 2). This suggests that the favorable biological environment created by Vitapex not only controls infection but also actively promotes a more rapid and robust functional rehabilitation of the treated tooth. The excellent flowability and penetrability of the Vitapex paste, facilitated by its silicone oil base, likely enable a more three-dimensional adaptation to the complex root canal anatomy, including accessory canals and isthmuses.19 This comprehensive seal ensures better periradicular tissue stability, creating an optimal biomechanical environment for the early and efficient recovery of occlusal function.
A particularly compelling finding is the significant reduction in systemic inflammatory markers (hs-CRP, IL-6, TNF-α) in the Vitapex group compared to the gutta-percha/ZOE group (Table 3). This indicates that the benefits of Vitapex extend beyond the local site, contributing to a more effective downregulation of the host’s systemic inflammatory response. The mechanisms are multifactorial. The antimicrobial action of iodoform reduces the bacterial load and associated endotoxins (eg, LPS), which are potent stimulators of pro-inflammatory cytokines like TNF-α and IL-6.20,21 Concurrently, the alkaline pH induced by calcium hydroxide can inhibit the activity of inflammatory cells and enzymes, such as those in the 5-lipoxygenase pathway responsible for LTB4 synthesis.22,23 Our results align with previous research; for instance, a meta-analysis by Tong et al indicated that calcium hydroxide-based sealers were associated with more favorable periapical healing outcomes and reduced postoperative inflammation compared to ZOE-based sealers.24
The assessment of periodontal health indices (BI, PLI, PD) revealed significantly better outcomes in the Vitapex group (Table 4). Given the intimate anatomic connection between the pulp and periodontium, effective control of endodontic infection is paramount for periodontal health.25 The superior antibacterial and anti-inflammatory properties of Vitapex likely mitigate the indirect negative impact of pulpal inflammation on the periodontal ligament, thereby facilitating better periodontal repair. Moreover, calcium hydroxide is known to promote hard tissue formation and healing, which may indirectly support the health of the adjacent periodontium.26,27
In terms of safety, the Vitapex group demonstrated a lower incidence of adverse reactions, although the difference did not reach statistical significance in our revised analysis (Table 5). This trend towards better tolerability is clinically relevant. While ZOE sealer is a time-tested material, eugenol can exhibit cytotoxic effects and has been associated with postoperative sensitivity and occasional allergic reactions in periodontal tissues.28 In contrast, Vitapex, with its resorbable nature and biocompatible silicone oil vehicle, is well-tolerated by periapical tissues, which may account for the observed trend towards fewer postoperative complications such as persistent pain and swelling.29,30
Despite these promising results, several limitations of this study must be acknowledged. Firstly, its retrospective and single-center design inherently carries risks of selection and information bias. Secondly, the sample size, though adequate for primary outcomes, may be underpowered to detect statistically significant differences in less frequent events like specific adverse reactions. Most importantly, the 4-week follow-up period is sufficient to assess short-term recovery and inflammatory control but is inadequate to evaluate long-term outcomes such as the permanence of the root canal seal, the long-term fate of the Vitapex material in the canal, and the true incidence of periapical tissue regeneration or disease recurrence. Future prospective, randomized, multi-center trials with extended follow-up periods, incorporating advanced imaging like cone-beam computed tomography (CBCT) and molecular biomarkers, are essential to validate these findings and elucidate the long-term performance and mechanisms of action of Vitapex in single-visit endodontic therapy.
Conclusion
In conclusion, this study provides evidence that for single-visit root canal treatment of acute irreversible pulpitis, obturation with Vitapex paste offers clinical advantages over the conventional gutta-percha/ZOE combination. Vitapex was associated with a faster symptomatic recovery, superior restoration of masticatory function, a more pronounced reduction in systemic inflammation, and a trend towards better periodontal health and fewer adverse events. These benefits are likely attributable to its sustained antimicrobial efficacy, biocompatibility, and ability to create a favorable biological environment for periapical healing. Based on these findings, Vitapex represents a valuable obturation material for clinicians seeking to optimize outcomes in single-visit endodontics. However, further high-quality, long-term studies are warranted to firmly establish its position in clinical practice.
Ethical Approval Statement
This study was approved by the ethics committee of Shijiazhuang Second Hospital. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research on the Correlation between Multiple Interleukin Gene Polymorphisms and Genetic Susceptibility to Diabetic Periodontitis (20231629).
Disclosure
The authors declare that they have no competing interests.
References
1. Han YX, Chen BZ, Yan QQ, et al. [Research progress in autophagy in the development of pulp inflammation and dental pulp injury reparation and regeneration]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2024;59(3):274–278. doi:10.3760/cma.j.cn112144-20230718-00009
2. Xiao W, Shi WT, Wang J. [Study of vital inflamed pulp therapy in immature permanent teeth with irreversible pulpitis and apical periodontitis]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2022;57(3):287–291. doi:10.3760/cma.j.cn112144-20211223-00563
3. He WX, Yu Q. [New advances in vital pulp therapy and pulp regeneration for the treatment of pulpitis: from basic to clinical application]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2022;57(1):16–22. doi:10.3760/cma.j.cn112144-20210917-00417
4. Hu YP, Qian Y. [The influence of different preparation methods on interappointment emergency and filling effect of root canal therapy]. Shanghai Kou Qiang Yi Xue. 2022;31(2):198–200.
5. Koçer A, Dönmez Özkan H, Turk T. Postoperative pain intensity and incidence following single visit root canal treatment with different obturation techniques: a randomized clinical trial. PeerJ. 2022;10:e13756. doi:10.7717/peerj.13756
6. Kaukab A, Nekkanti S. Antimicrobial efficacy of intracanal medicaments incorporated with nanoparticles in primary teeth: an in vitro study. Sci World J. 2025;2025:5182716. doi:10.1155/tswj/5182716
7. Shafaee H, Bardideh E, Nazari MS, et al. The effects of photobiomodulation therapy for treatment of alveolar osteitis (Dry Socket): systematic review and meta-analysis. Photodiagnosis Photodyn Ther. 2020;32:102000. doi:10.1016/j.pdpdt.2020.102000
8. Coll JA, Dhar V, Chen C-Y, et al. Primary tooth vital pulp treatment interventions: systematic review and meta-analyses. Pediatr Dent. 2023;45(6):474–546.
9. Agarwal SR, Bendgude VD, Kakodkar P. Evaluation of success rate of lesion sterilization and tissue repair compared to vitapex in pulpally involved primary teeth: a systematic review. J Conserv Dent. 2019;22(6):510–515. doi:10.4103/JCD.JCD_76_20
10. Tonini R, Salvadori M, Audino E, Sauro S, Garo ML, Salgarello S. Irrigating solutions and activation methods used in clinical endodontics: a systematic review. Front Oral Health. 2022;3:838043. doi:10.3389/froh.2022.838043
11. Hu R, Zhang F, Guo X, Jing Y, Lin X, Tian L. [Retracted] Effect of vitapex combined with AH‐plus paste on inflammation in middle‐aged and elderly patients with periodontal‐endodontic disease. Comput Math Methods Med. 2022;2022(1):7540961. doi:10.1155/2022/7540961
12. Tran HT, Kong Y, Talati A, Posada‐Quintero H, Chon KH, Chen IP. The use of electrodermal activity in pulpal diagnosis and dental pain assessment. Int Endodontic J. 2023;56(3):356–368. doi:10.1111/iej.13868
13. Yu J, Jiang R, Nie EM, Zhang CY, Li X. The prevalence of dental anxiety associated with pain among Chinese adult patients in Guangzhou. Pain Res Manag. 2021;2021(1):7992580. doi:10.1155/2021/7992580
14. Bosma ML, McGuire JA, Sunkara A, et al. Efficacy of flossing and mouthrinsing regimens on plaque and gingivitis: a randomized clinical trial. Am Dent Hyg Assoc. 2022;96(3):8–20.
15. Liang F, Zhou Y, Zhang Z, Zhang Z, Shen J. Association of vitamin D in individuals with periodontitis: an updated systematic review and meta-analysis. BMC Oral Health. 2023;23(1):387. doi:10.1186/s12903-023-03120-w
16. Llera-Romero AS, Adobes-Martín M, Iranzo-Cortés JE, Garcovich D, Garcovich D. Periodontal health status, oral microbiome, white-spot lesions and oral health related to quality of life-clear aligners versus fixed appliances: a systematic review, meta-analysis and meta-regression. Korean J Orthod. 2023;53(6):374–392. doi:10.4041/kjod22.272
17. Elnaghy AM, Elshazli AH, Elsaka SE. Effectiveness of oral premedication of meloxicam, ketorolac, dexamethasone, and ibuprofen on the success rate of inferior alveolar nerve block in patients with symptomatic irreversible pulpitis: a prospective, double-blind, randomized controlled trial. Quintessence Int. 2023;54(2):92–99. doi:10.3290/j.qi.b3605097
18. Srikumar GP, Kumar RS, Bardia S, et al. Antifungal effectiveness of various intracanal medicaments against candida albicans: an in vitro study. J Contemp Dent Pract. 2020;21(9):1042–1047. doi:10.5005/jp-journals-10024-2923
19. Doneria D, Thakur S, Singhal P, et al. Comparative evaluation of clinical and radiological success of zinc oxide-ozonated oil, modified 3mix-mp antibiotic paste, and vitapex as treatment options in primary molars requiring pulpectomy: an in vivo study. J Indian Soc Pedod Prev Dent. 2017;35(4):346–352. doi:10.4103/JISPPD.JISPPD_359_16
20. Najjar RS, Alamoudi NM, El‐Housseiny AA, et al. A comparison of calcium hydroxide/iodoform paste and zinc oxide eugenol as root filling materials for pulpectomy in primary teeth: a systematic review and meta-analysis. Clin Exp Dent Res. 2019;5(3):294–310. doi:10.1002/cre2.173
21. Ma HX, Shen -L-L, Liu K, et al. [Scanning electron microscope analysis of the root dentin bonding interface filled with different pastes or bonded by different program in fiber post and resin bonded repair]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2012;47(9):538–541. doi:10.3760/cma.j.issn.1002-0098.2012.09.007
22. Clarkson JE, Ramsay CR, Mannocci F, et al. Pulpotomy for the management of irreversible pulpitis in mature teeth (PIP): a feasibility study. Pilot Feasibility Stud. 2022;8(1):77. doi:10.1186/s40814-022-01029-9
23. Özkabadayı Y, Türk M, Kumandaş A, et al. Amino acid surface modified bioglass: a candidate biomaterial for bone tissue engineering 1. Microsc Res Tech. 2025;88(1):26–41. doi:10.1002/jemt.24659
24. Yoneda T, Tomofuji T, Kunitomo M, et al. Preventive effects of drinking hydrogen-rich water on gingival oxidative stress and alveolar bone resorption in rats fed a high-fat diet. Nutrients. 2017;9(1):64. doi:10.3390/nu9010064
25. Dong M, TANG J, LI L-J, et al. Curcumin inhibits the neuroimmune response mediated by mast cells after pulpitis. J Appl Oral Sci. 2024;32:e20230456. doi:10.1590/1678-7757-2023-0456
26. Xia C, Sadeghi L, Strååt K, et al. Intrinsic 5-lipoxygenase activity regulates migration and adherence of mantle cell lymphoma cells. Prostaglandins Other Lipid Mediat. 2021;156:106575. doi:10.1016/j.prostaglandins.2021.106575
27. Hu Z, Chen Y, He J, et al. EZH2 might affect macrophage chemotaxis and anti-inflammatory factors by regulating CCL2 in dental pulp inflammation. Stem Cells Int. 2021;2021:3060480. doi:10.1155/2021/3060480
28. Gupta S, Gupta A, Arora S, et al. Efficacy of different obturating materials - A comparative study. Indian J Dent Res. 2025;36(1):42–48. doi:10.4103/ijdr.ijdr_132_24
29. Guedes Pinto T, Claudia Muniz Renno A, Nunes Dos Santos J, et al. Genotoxicity induced by endodontic sealers: a systematic review. Saudi Dent J. 2024;36(2):249–257. doi:10.1016/j.sdentj.2023.11.019
30. Sijini OT, Sabbagh HJ, Baghlaf KK, et al. Clinical and radiographic evaluation of triple antibiotic paste pulp therapy compared to Vitapex pulpectomy in non-vital primary molars. Clin Exp Dent Res. 2021;7(5):819–828. doi:10.1002/cre2.434
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Articaine Needle - Free Anesthesia Vs Conventional Anesthesia in Root Canal Treatment of Irreversible Pulpitis in Permanent Teeth: A Prospective Study on Anesthetic Efficacy and Effects on Pain
Qian S, Meng Z, Zhang H, Li K, Zhang F, Zhang S, Liu J, Zhou Z
Journal of Pain Research 2025, 18:2115-2125
Published Date: 21 April 2025