Back to Journals » Clinical Ophthalmology » Volume 15
Short-Term Anterior Segment Changes After Nd-YAG Laser Posterior Capsulotomy in Pseudophakic Eyes with Fuchs’ Endothelial Dystrophy
Authors Eleiwa T ![]() , Khedr NED, Fayek H, Bayoumy A
, Khedr NED, Fayek H, Bayoumy A
Received 20 February 2021
Accepted for publication 12 April 2021
Published 30 April 2021 Volume 2021:15 Pages 1819—1825
DOI https://doi.org/10.2147/OPTH.S305306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Taher Eleiwa,1 Negm El-Din Khedr,1,2 Hytham Fayek,1 Ahmed Bayoumy1
1Department of Ophthalmology, Faculty of Medicine, Benha University, Benha, Egypt; 2Department of Ophthalmology, Mataria Teaching Hospital, Mataria, Egypt
Correspondence: Taher Eleiwa
Department of Ophthalmology, Faculty of Medicine, Benha University, 79 Nozha st, Heliopolis, 11341, Cairo, Egypt
Tel/Fax +20 1069901973
Email [email protected]
Purpose: To describe the changes in the central corneal thickness (CCT), endothelial cell count (ECC), intraocular lens (IOL) position, and refractive error 1 and 3 months after Nd-YAG laser posterior capsulotomy (YAG-PC) for posterior capsular opacification (PCO) in pseudophakic eyes with Fuchs’ endothelial cell dystrophy (FECD).
Design: Prospective case-control.
Participants: Fifty pseudophakic eyes of 50 patients with visually significant PCO (25 with healthy corneas, and 25 with FECD grade 1 and 2).
Methods: FECD was clinically graded, and only patients without clinically evident corneal edema were included in the study (grade 1 and 2). All patients received YAG-PC and were followed up after 1 and 3 months. Best-corrected visual acuity, refractive errors, ACD, CCT, and ECC were assessed and compared between the pre-laser values and that of the 2 follow-up visits.
Results: In both groups, BCVA showed significant improvement (P< 0.05). Compared to healthy controls, a significant hyperopic shift was observed in the FECD eyes at the 2 follow-up visits (P=0.027, and 0.019). A significant backward movement of the IOL was observed in the FECD eyes in the 2 follow-up visits (P=0.043, and 0.02). There was a significant correlation between the hyperopic shift in the FECD eyes and the ACD deepening during the 1st month (R= − 0.6, P=0.001) and 3rd month (R= − 0.4, P=0.04). Significant drop in the ECC was noted in both groups but without significant increase in the CCT.
Conclusion: Compared to controls, a hyperopic shift and backward movement of the IOL were observed in the FECD eyes after YAG-PC. No significant corneal thickening was found in both groups despite the significant drop in the ECC. Future studies are required to confirm our results and monitor the long-term changes after YAG-PC in FECD.
Keywords: YAG laser, posterior capsulotomy, Fuchs’ dystrophy, posterior capsular opacification
Introduction
Fuchs’ endothelial corneal dystrophy (FECD) is an autosomal dominant slowly progressive bilateral asymmetric primary disease of the cornea. It is characterized by progressive loss of endothelial cells with thickening of the Descemet’s membrane and development of focal excrescences called guttae that leads to endothelial cell dysfunction, corneal edema and a drop in the visual acuity.1 The reported incidence of FECD is 6.7%,2 while Krachmer et al reported a prevalence of 4–70% according to aging.3 Cataract is the most common cause of global blindness.4 Cataract surgery leads to endothelial cell loss of approximately 10%,5,6 depending on preoperative endothelial cell count, axial length, cataract density, and the surgical technique.7,8 In FECD, even a minimal loss of endothelial cells during phacoemulsification can affect their density to fall below the critical threshold that can lead to corneal decompensation. Central corneal thickness (CCT) greater than 640 μm in FECD has been proposed to be a clinical index of possible postoperative corneal decompensation that warranted a combined cataract and endothelial transplant surgery rather than doing cataract surgery alone.9
Posterior capsule opacification (PCO) is the most frequent complication following cataract surgery that may develop early or many years post-surgery. Its incidence ranges from <5% to as high as 50% depending on the surgical technique and IOL material and design.10 The standard effective treatment for PCO is Nd: YAG laser posterior capsulotomy (YAG-PC) which may be associated with complications such as a spiking intraocular pressure, pitting of IOL, uveitis, cystoid macular edema, vitreoretinal detachments, and refractive changes due to feasible axial IOL movement.11 As one of the rare complications of laser capsulotomy in a patient with FECD, Afriat et al reported a Descemet membrane detachment in a 89-year-old man 1 day after YAG-PC laser capsulotomy.12
The aim of this prospective case-control study was to investigate the influences of YAG-PC on corneal endothelium, central corneal thickness, and IOL position in pseudophakic eyes with FECD and posterior capsular opacification.
Patients and Methods
Study Design and Participants
This is a prospective case-control study approved by Institutional Review Board of Benha University (Study ID: MS-922020), and strictly followed the tenets of the Declaration of Helsinki. All patients signed a written informed consent before being enrolled.
Fifty pseudophakic eyes of 50 patients with visually significant posterior capsular opacification (PCO) were included in the study. Patients were recruited during the period between January 2020 and June 2020 from the outpatient clinic at Benha University Hospital. Patients were divided into 2 groups (25 each) according to clinical diagnosis made by a cornea specialist into group 1 (healthy cornea), group 2 (cornea with FECD). FECD was diagnosed clinically by the presence of guttae, with or without clinically evident edema. Furthermore, FECD eyes were clinically graded according to Adamis et al1, grading method. Only grade 1 and 2 were included in our study. Eyes were pseudophakic with an endocapsular posterior chamber intraocular lens implant (AcrySof® hydrophobic single-piece intraocular lens) in the studied groups, without any history of uveitis. All patients had an uneventful cataract surgery at least 6 months before enrollment. Patients received YAG-PC as a management for PCO.
Exclusion criteria were patients with grade 3 or 4 FECD, pseudoexfoliation syndrome, uveitis, glaucoma, diabetes mellitus, systemic diseases with ocular involvement and patients who could not stay at an upright position.
Full ophthalmic examination was conducted including best-corrected visual acuity (BCVA), slit-lamp biomicroscopic and fundus examination, and intraocular pressure (IOP) measurement. Effective IOL position determined by measuring anterior chamber depth (ACD) using IOL-master (ZEISS IOLMaster 500) that gives accurate measurements of AC depth using partial coherence interferometry technique, taking average 5 measurements for detection of IOL position. Corneal endothelium imaging and central corneal thickness were obtained with specular microscopy (Tomey EM-3000) which is a non-contact specular microscope using fixed frame analysis method to image the corneal central area automatically using auto tracking system. The taken images were transferred to the computer that is supplied with a software that analyzes the endothelial cell layer accurately.13 Averages of parameters were used for the analysis. Specular microscope was calibrated so that when the endothelium is in focus, the thickness of the cornea automatically gets displayed digitally. All data were collected from non-dilated eyes prior to YAG-PC, then 1 month and 3 months after the procedure.
Surgical Procedure
Patients were pretreated with dilating drops, such as tropicamide 1.0%. Eye was anesthetized with a drop of Benoxinate hydrochloride 0.4%. The laser power was 1–3 mJ with a Q-switched mode that produces a series of single pulses that last 12–20 nanoseconds. The posterior capsulotomies usually performed with an average diameter of 5.0 mm in a circular pattern, the Nd: YAG laser was defocused posteriorly by 0.50 mm to avoid IOL pitting.14
Postoperative Follow-Up
After laser procedure, all patients were treated with topical brimonidine (0.1%) twice a day for one week and topical steroids (prednisolone acetate 1%) four times daily for a week followed by tapering. Post laser, patients were followed-up and reassessed at 1 week, 1 month and 3 months.
Statistical Analysis
The results were analyzed using SPSS 25. Normally distributed continuous data were expressed as mean ± standard deviation and not-normally distributed continuous data were expressed as median (range). Categorical data were expressed as percentage. t-test used to compare between two groups in case of normally distributed variables. Not-normally distributed variables were analyzed using Mann–Whitney U-test. Chi-square test was used to compare between qualitative variables. Paired samples t-test was used to compare the repeated measures of the tested parameters between the 2 groups at each time point. Results were considered statistically significant at a p-value less than 0.05.
Results
Our study included 50 pseudophakic eyes of 50 patients (25 with FECD versus 25 age-matched controls with healthy corneas) who underwent uneventful YAG laser capsulotomy at (10.2±3.8, range 6–14) months after uneventful cataract extraction. The mean age of the controls was 57.2±4.6 years, and 59.6±5.4 years for the FECD group (P=0.054). Seventeen (68%) of the controls were females, while 9 (36%) of the FECD group were females. In healthy controls, the mean energy used for laser treatment 0.4 MJ/spot, the average total spot count was 7.8 (range: 5–10), and the mean total energy level was 6.4mj (range: 3.9–16.8mj). In FECD group, the mean energy used for laser treatment 0.35 MJ/spot, the average total spot count was 7.5 (range: 4–9) and the mean total energy level was 6.1mj (range: 3.6–15.8mj). There was no statistically significant difference between 2 groups. Table 1 summarizes the changes in BCVA, refractive errors, ACD, ECC, and CCT in each group at each postoperative visit compared to the preoperative ones. Table 2 compares the measured parameters between both groups at each time point.
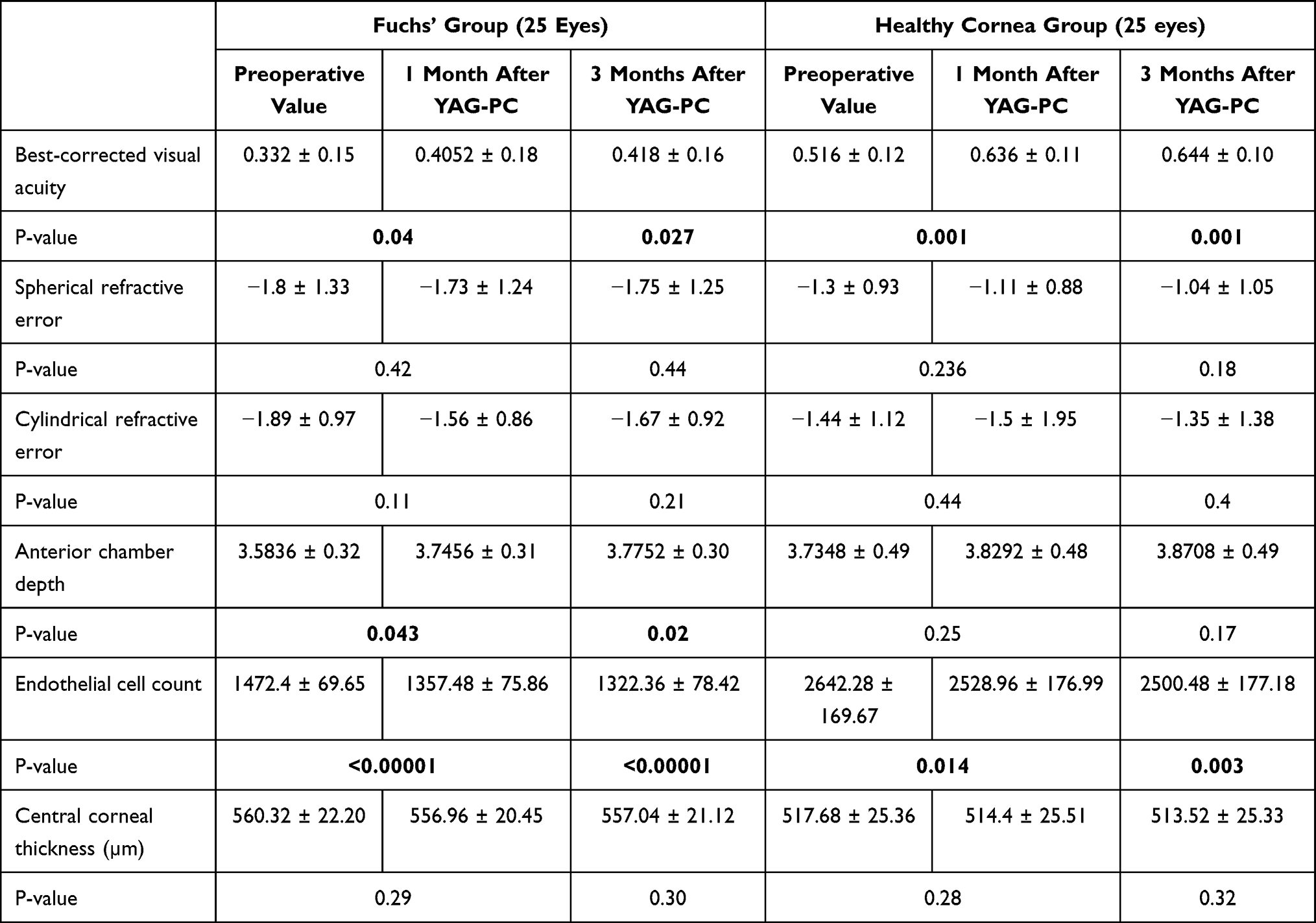 |
Table 1 Postoperative Parameters Compared to the Preoperative Ones at Each Time Point in Both Groups |
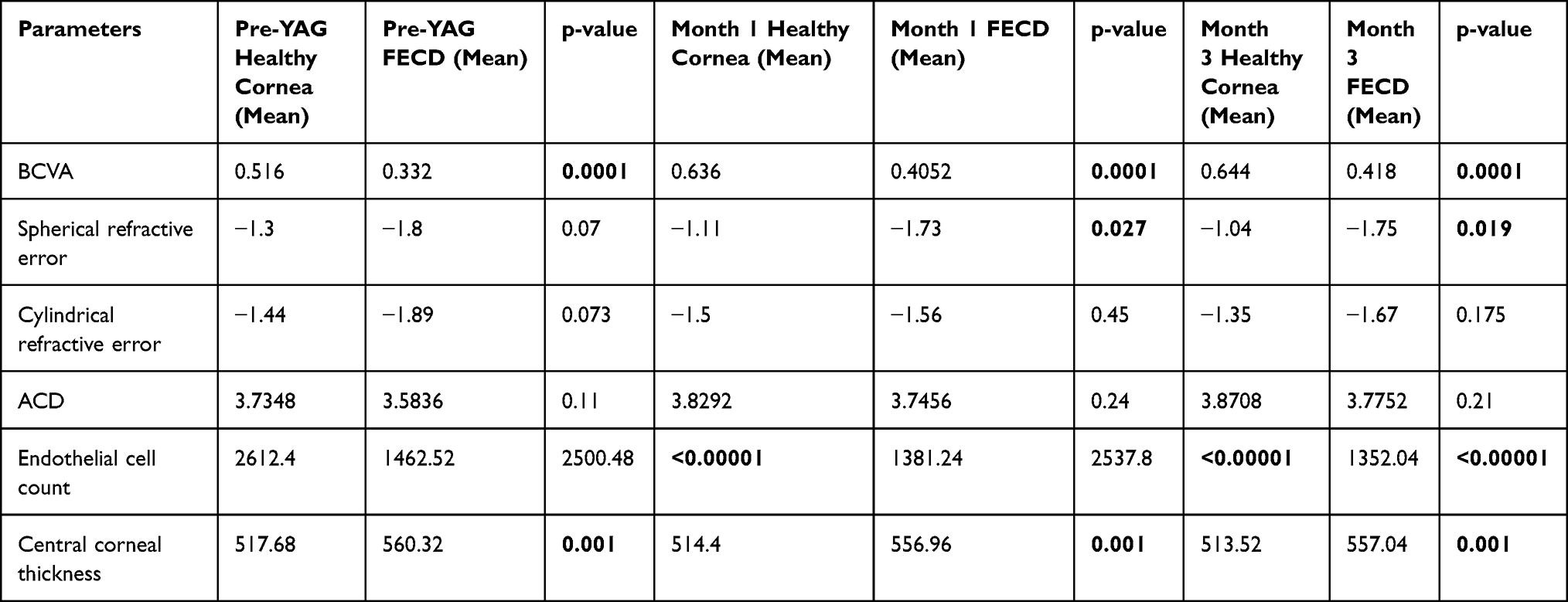 |
Table 2 Comparison of the BCVA, Refractive Errors, ACD, ECC, and CCT Between Both Groups at Each Postoperative Visit |
The BCVA has significantly improved in both groups at the first and the third postoperative month compared to that before the YAG-PC (P<0.05, Table 1). The BCVA was significantly better in the controls compared to the FECD group during the 3 visits (P=0.0001, Table 2). No significant changes were found in the spherical or cylindrical refractive errors in the controls during the 1st and 3rd postoperative months compared to the preoperative ones. Compared to the control group, a significant hyperopic shift was observed in the FECD group at 1st and 3rd postoperative months (P= 0.027, and 0.019, respectively, Table 2).
Regarding the ACD, there was a significant deepening at the 1st and 3rd postoperative months in the FECD group only, as compared to the pre-laser ACD (P=0.043, and 0.02, respectively, Table 1). Moreover, there was a significant negative correlation between the changes in the ACD and the changes in the spherical equivalent during the 1st month (R= −0.6, P=0.001, Figure 1A), and 3rd month (R= −0.4, P=0.04, Figure 1B) postoperatively in the FECD group.
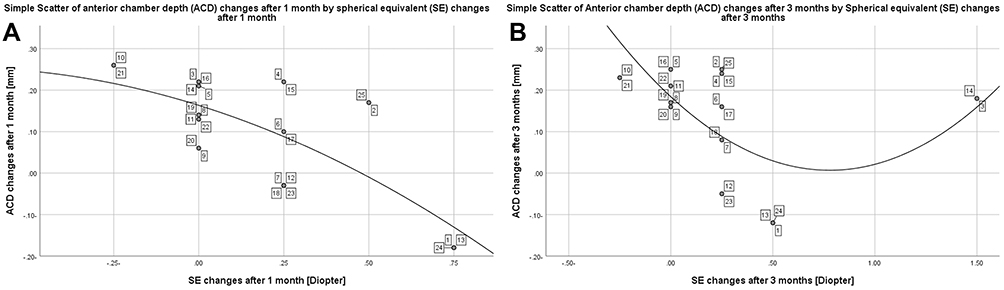 |
Figure 1 Scatter plots showing a significant negative quadratic correlation between the changes in the ACD and the changes in the spherical equivalent during the 1st month (R= −0.6, P=0.001, A), and 3rd month (R= −0.4, P=0.04, B) postoperatively in the FECD group. Case numbers are displayed with connecting lines to each corresponding data value. |
The endothelial cell count (ECC) was significantly less in the FECD group compared to the controls at all visits (P<0.0001). Compared to the pre-laser values, the drop in the ECC at the 1st and 3rd months after the YAG-PC was statistically significant in the FECD (P<0.0001 and P<0.0001, respectively) and the controls (P=0.014, and 0.003, respectively). The mean decrease in endothelial cell count was 75 cells/mm2 after 1 month and 112 cells/mm2 after 3 months in controls, while it was 81 cells/mm2 and 110 cell/mm2 in the FECD group, respectively.
The CCT was significantly thicker in the FECD group during all visits compared to the healthy one (P=0.001). However, no significant changes were found in both groups separately during the 2 postoperative visits compared to that before the YAG-PC (Table 1).
Discussion
To our knowledge, we are the first to report the effects of YAG-PC in pseudophakic eyes with FECD. Nd: YAG-induced photodisruption throughout the anterior chamber leads to impact injury to the endothelium with a maximum damage to the center that could be visualized with the specular microscopy. Before 1970, the corneal endothelium was studied at high magnification only in vitro.15 The development of the specular microscopy has made qualitative and quantitative in vivo evaluation of corneal endothelium possible.16,17 In our study, we compared the changes in IOL position, corneal endothelium, and central corneal thickness after YAG-PC in patients with grade 1 and 2 FECD and patients without FECD.
In a study by Hassan et al18, the time interval between cataract surgery and PCO was reported as 2.49 years. Another study by Rajappa et al17 found that the mean interval was 2.5 years. Khambhiphant et al19 found that the mean time from cataract surgery to the laser treatment of PCO was 28.3 months (range: 5–71 months). In our study, YAG-PC was indicated 6–14 months after cataract surgery.
Rajappa et al17 reported that the Nd: YAG energy required depends upon the type of PCO. The mean energy required for Elschnig’s PCO was 51.33 mJ and that for fibrous type was 63.43 mJ. The mean energy used by Khambhiphant et al19 was 0.8 mJ/spot; the average total spot count was 15.4 (range: 7–39), and the total energy level was 12.6 mJ (range: 5.6–29.5 mJ). In our study, the total energy level was 12.2mj (range: 5.6–28.9mj) and the average total spot count was 14.5 (range: 7–21).
As reported in the literature, we report a significant improvement in visual acuity in both groups after YAG-PC. Hossain et al20 reported an 80% improvement in visual acuity. Likewise, Terry et al21 and Aron-Rosa et al22 reported visual improvement in 92%, and 94% of their cohorts, respectively. Regarding the changes in the spherical refractive error, several studies had reported that the change in the spherical error after YAG-PC was statistically insignificant,20,23–25 in agreement with our results in the non-FECD group. In the FECD eyes, there was a significant hyperopic shift compared to the controls in the 1st month and 3rd months after laser. This might be attributed to the significant deepening in the ACD observed in the FECD group at the same time (Figure 1A and B). Further studies are required to observe the long-term changes in the ACD and the refractive errors in FECD after YAG-PC.
Regarding the changes in the effective IOL position, the published reports in the literature are perplexing. Khambhiphan et al,19 Hu et al25 and Ozkurt et al26 had reported nonsignificant changes in ACD after YAG-PC. In contrast, Findl et al27 reported an immediate increase in the ACD in their cohort after the YAG-PC with a more pronounced backward movement in plate-haptic IOLs than both 1-piece or 3-piece IOLs. In addition, Monteiro et al11 reported a significant posterior movement after YAG-PC in pseudophakic eyes with C-loop acrylic hydrophobic single-piece AcrySof® SA60AT. In our study, despite having the same IOL implanted and the insignificant difference in the energy consumed to disrupt the PCO in both groups, we report a significant backward shift of the AcrySof® hydrophobic single-piece IOL in the FECD group versus no significant changes of the ACD in the controls 1 and 3 months after YAG-PC. A limitation in our study is not measuring the changes in the size of capsulotomy, as it can affect the IOL movement after YAG-PC. Many studies have shown that the posterior IOL movement and the hyperopic shift were associated with the larger the size of capsulotomy.11,27,28 Further studies with larger sample size are required to confirm our results and verify whether the changes in the IOL position after YAG-PC depend in part on the corneal health status.
For the ECC, it is well reported in the literature that ECC drops significantly after YAG laser capsulotomy.19,29 Likewise, we reported the same finding in our cohort. Besides, there was a statistically significant difference between two groups in preoperative value, 1 month after and 3 months after YAG laser. However, it is noteworthy to mention that the ECC drop was not associated with a significant corneal thickening in both groups, as reported by Rajappa et al17 Clinically, the corneas of both groups remained clear throughout the follow-up visits. Further studies are mandated to observe the long-term effects of Nd: YAG capsulotomy on the ECC in pseudophakic eyes with early stages of FECD (without clinically evident corneal edema) to find out the threshold ECC and CCT to proceed without having the risk of corneal decompensation after laser or a corneal transplant might be required soon.
Our study has a few limitations. First, our results stem from limited sample size, and larger cohorts are mandated to replicate our findings. Second, we did not include all grades of FECD; however, we included grades 1 and 2 FECD to shed light on the short-term effects of YAG laser in FECD eyes. Third, AS-OCT and Scheimpflug imaging were not done for our cases.30,31 Using these imaging techniques would help quantify the changes in the corneal microlayers and describe the refractive changes more precisely.32,33 Despite the recently reported findings of these imaging devices in detecting subclinical edema in FECD, they are not routinely requested before YAG capsulotomy. Fourth, owing to the short-term nature of our study, we were not able to predict the risk of corneal decompensation and monitor FECD progression. Future longitudinal studies are required to address the aforementioned limitations.
In conclusion, we report a significant deepening of the AC associated with a hyperopic shift in pseudophakic eyes with FECD (grades 1 and 2) 1 and 3 months after YAG posterior capsulotomy. On the other hand, a significant drop in ECC without functional corneal decompensation was observed in both groups. Further studies are required to identify the pseudophakic eyes with early-stage FECD and PCO on the brink of corneal decompensation and requiring a corneal transplant before doing the laser capsulotomy.
Abbreviations
CCT, central corneal thickness; ECC, endothelial cell count; IOL, intraocular lens; YAG-PC, Nd-YAG laser posterior capsulotomy; PCO, posterior capsular opacification; FECD, Fuchs’ endothelial cell dystrophy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Adamis AP, Filatov V, Tripathi B. Fuchs’ endothelial dystrophy of the cornea. Surv Ophthalmol. 1993;38(2):149–168. doi:10.1016/0039-6257(93)90099-S
2. Kitagawa K, Kojima M, Sasaki H, et al. Prevalence of primary cornea guttata and morphology of corneal endothelium in aging Japanese and Singaporean subjects. Ophthalmic Res. 2002;34(3):135–138. doi:10.1159/000063656
3. Krachmer JH, Purcell JJ, Young CW, Bucher KD. Corneal endothelial dystrophy: a study of 64 families. Arch Ophthalmol. 1978;96(11):2036–2039. doi:10.1001/archopht.1978.03910060424004
4. Congdon N, West SK, Buhrmann RR, Kouzis A, Munoz B, Mkocha H. Prevalence of the different types of age-related cataract in an African population. Invest Ophthalmol Vis Sci. 2001;42(11):2478–2482.
5. Bourne WM, Nelson LR, Hodge DO. Continued endothelial cell loss ten years after lens implantation. Ophthalmology. 1994;101(6):1014–1023. doi:10.1016/S0161-6420(94)31224-3
6. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors for corneal endothelial injury during phacoemulsification. J Cataract Refract Surg. 1996;22(8):1079–1084. doi:10.1016/S0886-3350(96)80121-0
7. Walkow T, Anders N, Klebe S. Endothelial cell loss after phacoemulsification: relation to preoperative and intraoperative parameters. J Cataract Refract Surg. 2000;26(5):727–732. doi:10.1016/S0886-3350(99)00462-9
8. Beesley R, Olson R, Brady S. The effects of prolonged phacoemulsification time on the corneal endothelium. Ann Ophthalmol. 1986;18(6):216–219, 222.
9. Covert DJ, Koenig SB. New triple procedure: descemet’s stripping and automated endothelial keratoplasty combined with phacoemulsification and intraocular lens implantation. Ophthalmology. 2007;114(7):1272–1277. e1272. doi:10.1016/j.ophtha.2006.12.030
10. Ursell PG, Dhariwal M, O’Boyle D, Khan J, Venerus A. 5 year incidence of YAG capsulotomy and PCO after cataract surgery with single-piece monofocal intraocular lenses: a real-world evidence study of 20,763 eyes. Eye. 2020;34(5):960–968. doi:10.1038/s41433-019-0630-9
11. Monteiro T, Soares A, Leite RD, Franqueira N, Faria-Correia F, Vaz F. Comparative study of induced changes in effective lens position and refraction after Nd: YAG laser capsulotomy according to intraocular lens design. Clin Ophthalmol. 2018;12:533. doi:10.2147/OPTH.S156703
12. Afriat M, Gueudry J, Chérif HY, Maringe E, Muraine M. Descemet membrane detachment after Nd: YAG laser capsulotomy in a patient with fuchs dystrophy. Cornea. 2014;33(10):1103–1105. doi:10.1097/ICO.0000000000000222
13. Hirst LW, Ferris F, Stark WJ, Fleishman J. Clinical specular microscopy. Invest Ophthalmol Vis Sci. 1980;19(1):2–4.
14. Krueger RR, Talamo JH, Lindstrom RL. Textbook of Refractive Laser Assisted Cataract Surgery (Relacs). Springer Science & Business Media; 2012.
15. Laing RA, Sandstrom MM, Leibowitz HM. In vivo photomicrography of the corneal endothelium. Arch Ophthalmol. 1975;93(2):143–145. doi:10.1001/archopht.1975.01010020149013
16. Bourne WM, Kaufman HE. Specular microscopy of human corneal endothelium in vivo. Am J Ophthalmol. 1976;81(3):319–323. doi:10.1016/0002-9394(76)90247-6
17. Rajappa N, Lune A, Radhakrishnan O, Magdum R, Patil P, Mehta R. Evaluation of corneal endothelium before and after neodymium: yttrium-aluminium-garnet laser capsulotomy in posterior capsular opacification. Sudanese J Ophthalmol. 2013;5(2):73. doi:10.4103/1858-540X.124831
18. Hasan KSAM, Aziz M, Shah N, Farooqui M. Nd:YAG laser posterior capsulotomy. Pak J Ophthalmol. 1996;12:3–7.
19. Khambhiphant B, Liumsirijarern C, Saehout P. The effect of Nd: YAG laser treatment of posterior capsule opacification on anterior chamber depth and refraction in pseudophakic eyes. Clin Ophthalmol. 2015;9:557. doi:10.2147/OPTH.S80220
20. Hossain M, Hossain M, Hossain M. Visual outcome after Nd: YAG laser Capsulotomy. J Armed Forces Med Coll. 2009;5(2):29–31. doi:10.3329/jafmc.v5i2.4580
21. Terry AC, Stark WJ, Maumenee AE, Fagadau W. Neodymium-YAG laser for posterior capsulotomy. Am J Ophthalmol. 1983;96(6):716–720. doi:10.1016/S0002-9394(14)71912-9
22. Aron-Rosa DS, Aron -J-J, Cohn HC. Use of a pulsed picosecond Nd: YAG laser in 6664 cases. Am Intra-Ocular Implant Soc J. 1984;10(1):35–39. doi:10.1016/S0146-2776(84)80074-9
23. Thornval P, Naeser K. Refraction and anterior chamber depth before and after neodymium: YAG laser treatment for posterior capsule opacification in pseudophakic eyes: a prospective study. J Cataract Refract Surg. 1995;21(4):457–460. doi:10.1016/S0886-3350(13)80540-8
24. Vrijman V, van der Linden JW, Nieuwendaal CP, van der Meulen IJ, Mourits MP, Lapid-Gortzak R. Effect of Nd: YAG laser capsulotomy on refraction in multifocal apodized diffractive pseudophakia. J Refractive Surg. 2012;28(8):545–551. doi:10.3928/1081597X-20120723-03
25. Hu C-Y, Woung L-C, Wang M-C, Jian J-H. Influence of laser posterior capsulotomy on anterior chamber depth, refraction, and intraocular pressure. J Cataract Refract Surg. 2000;26(8):1183–1189. doi:10.1016/S0886-3350(00)00453-3
26. Ozkurt YB, Sengör T, Evciman T, Haboğlu M. Refraction, intraocular pressure and anterior chamber depth changes after Nd: YAG laser treatment for posterior capsular opacification in pseudophakic eyes. Clin Exp Optometry. 2009;92(5):412–415. doi:10.1111/j.1444-0938.2009.00401.x
27. Findl O, Drexler W, Menapace R, et al. Changes in intraocular lens position after neodymium: YAG capsulotomy. J Cataract Refract Surg. 1999;25(5):659–662. doi:10.1016/S0886-3350(99)00010-3
28. Holladay JT, Bishop JE, Lewis JW. The optimal size of a posterior capsulotomy. Am Intra-Ocular Implant Soci J. 1985;11(1):18–20. doi:10.1016/S0146-2776(85)80107-5
29. Bazard M, Guldenfels Y, Raspiller A. Early endothelial complications after treatment using a neodymium-Yag laser. J francais d’ophtalmologie. 1989;12(1):17–23.
30. Eleiwa T, Elsawy A, Tolba M, Feuer W, Yoo S, Shousha MA. Diagnostic performance of 3-dimensional thickness of the endothelium–descemet complex in fuchs’ endothelial cell corneal dystrophy. Ophthalmology. 2020;127(7):874–887. doi:10.1016/j.ophtha.2020.01.021
31. Sun SY, Wacker K, Baratz KH, Patel SV. Determining subclinical edema in Fuchs endothelial corneal dystrophy: revised classification using Scheimpflug tomography for preoperative assessment. Ophthalmology. 2019;126(2):195–204. doi:10.1016/j.ophtha.2018.07.005
32. Oztas Z, Palamar M, Afrashi F, Yagci A. The effects of Nd: YAG laser capsulotomy on anterior segment parameters in patients with posterior capsular opacification. Clin Exp Optometry. 2015;98(2):168–171. doi:10.1111/cxo.12205
33. Kulikov AN, Maltsev DS, Kudryashova EV, Burnasheva MA. Decreased epithelial to corneal thickness ratio in healthy fellow eyes of patients with unilateral bullous keratopathy. Br J Ophthalmol. 2020;104(2):230–234. doi:10.1136/bjophthalmol-2018-313648
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.