Back to Journals » Orthopedic Research and Reviews » Volume 14
Short Stem for Total Hip Arthroplasty (THA) – Overview, Patient Selection and Perspectives by Using the Metha® Hip Stem System
Authors Ishaque BA ![]()
Received 6 September 2021
Accepted for publication 3 March 2022
Published 24 March 2022 Volume 2022:14 Pages 77—89
DOI https://doi.org/10.2147/ORR.S233054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Bernd Alexander Ishaque
Department of Orthopaedics and Orthopaedic Surgery, University Hospital Giessen and Marburg (UKGM), Giessen, 35392, Germany
Correspondence: Bernd Alexander Ishaque, Department of Orthopaedics and Orthopaedic Surgery, University Hospital Giessen and Marburg (UKGM), Klinikstraße 33, Giessen, 35392, Germany, Tel +49 641 98542914, Fax +49 641 98542969, Email [email protected]
Abstract: Short stem hip replacement has not only gained attention but also significance over the past decades. However, there still remains uncertainty regarding the correct indications for these stems. Even companies, producing implants, have varying recommendations that are more likely based on a well-meant advice than on statistically evaluated data. Thus, it is important to evaluate the advantages and disadvantages of a short stem prosthesis. The goal of this paper is to reveal some of the existing uncertainty in this field, by analyzing the Metha® short hip stem system. This paper does not only focus on general aspects but also discusses some more specific problems, such as avascular necrosis and post-rheumatic diseases, as well as hip dysplasia and coxarthrosis. The aim is also to convey the opportunity to indicate this type of implant for elderly and obese patients as well as for femoral misalignments following post-Perthes disease, post-traumatic deformities or other malpositions of the hip.
Keywords: hip arthroplasty, metaphyseal anchorage, indication, short hip stem
Introduction
It has been shown that cement-free standard stems have gained outstanding survival rates, with more than 15 years in 95% of the patients. However, long-term studies have impressively shown that the implantation of these systems drastically impacts the load transfer, which directly leads to pathological modifications in the bone structure, possibly resulting in stress-shielding. While there is already a complete bone resection of the femoral neck during the implantation of standard prosthesis, a stress shielding consecutively leads to a further loss of bone matrix in the trochanteric region, directly affecting the function and stability of the joint as the trochanteric region plays a crucial role in its balance as it serves as insertion points for the hip stabilizing muscles. The bone demineralization in this region, following stress shielding, will increase the relative movements of the tensile bone area surrounding the stiff prosthesis, possibly leading to osteolysis around the implant body.
In case of revision surgery, additional bone loss has to be expected and long revision stems become necessary in order to achieve sufficient anchoring in the diaphysis. The functional outcome as well as the survival rates of those stems are not satisfying.1 Alongside an increased bone loss during the primary implantation, one has to acknowledge that the geometry of standard implants is not ideal for minimal invasive techniques as they may lead to further muscle damage.
Even though the median is placed at age 70, 26% of the THA interventions concern patients <65 years. Hence, it is important to consider that these patients are not only numerically young but especially age-biologically. Since the implants do have a limited survival period, one has to recognize that these patients will undergo at least one, but usually two or more revision surgeries. Hence, it is not surprising that the biggest increase in hip joint replacements between 2005 and 2011 have been replacement surgeries (+4300 cases).2 Springer et al have conducted a retrospective study, analyzing survival periods as well as reasons for failure following the first prosthesis replacement in 1100 patients. Both cemented and cement free standard stems have been used. It has been shown that aseptic loosening as well as secondary dislocation have been the main reasons for implant failure, limiting the survival period of the prosthesis to 10 years in 82% of cases.3 However, in situations of minor loosening defects there is an opportunity to improve the functional results as well as the expected survival period by using primary hip stems.4 Therefore, the aim is to realize a soft tissue sparing and bone saving primary implantation of the hip stem in order to create perfect conditions for a successful revision surgery, if possible by, then using a standard stem.
To achieve this goal, there has been an increase in prosthesis development over the past three decades that has focused on conserving the femoral neck fully or at least partially and using it as an anchorage zone. One of these implants, the Metha® short hip stem, was launched in August 2004, initially as a modular stem system and since 2008 as the shape of a monobloc short stem. So far, studies provided 5 to 7 years of Kaplan–Meier survival rate between 96.7% and 98.5%.5,6 The load distribution of this short stem hip prosthesis system aims at not only mediating through the metaphyseal, intertrochanteric region, but especially through the calcar femoris, which leads to a more physiological load transfer and can therefore avoid the phenomena of stress shielding process that has been mentioned earlier on. As a great advantage in comparison to standard stems, the Metha® short stem does not compromise the greater trochanter. Further design advantages include soft tissue sparing and bone preserving surgical technique, an anatomical variability, as well as an enhanced stability via Plasmapore u-CaP coating (CaHPO4x2H2O) on the proximal surface. The implant (titanium forged alloy – Isotan®) is available in 8 sizes (0–7) with various CCD angles (120°, 130°, 135°). The range of the stems is graduated with 1.5 mm at the antero-posterior level and 1.2 mm at the lateral view. The femoral osteotomy usually begins just above the fossa piriformis and is ideally performed at a 50°angle. A closed cortical femoral neck ring is needed to secure the anchoring. Preoperative planning is usually done digitally. The aim is to achieve stable support on the calcar femoris and a flat lateral contact with the inner cortex (Figure 1).
 |
Figure 1 Metha® hip stem (130° left, 120° right) (A). Digital templating (mediCAD®) of a Metha® hip prosthesis with a Plasmafit® Cup System (B). |
Classification and Overview of Short Stem Implants
Since there is a significant increase in further short stem models, it is necessary to take a look at the nomenclature as well as the classification in order to discuss the respective indications. Depending on the resection level, short stem prostheses are divided into femoral neck preserving, femoral neck partially preserving and femoral neck resecting systems.7 In addition, the implants are classified by its design: Short stems that represent the anatomy of the femur, “Mayo- principle“, and those that can be seen as shortened straight stems. In addition, the implants differ when taking a look at the anchoring systems: There are metaphysical, meta-short diaphyseal and meta-diaphyseal systems.
The goal of the implants, which preserve the femoral neck, is to introduce the load solely metaphysically. A perfect example of such a prosthesis is the Thrust Plate System designed by Huggler and Jacob. This system was implanted in 1978 for the first time. Some other representatives of these systems, which are also known as femoral neck prostheses, are the Cut® prosthesis, the Spiron® prosthesis and the Silent® prosthesis.
Partially preserving femoral neck prosthesis achieves their anchoring meta- and short diaphysically. There is a large sum of such modern short stem implants that can be seen as design modifications of the Mayo® prosthesis, also known as the “origin of short stems“. One significant feature of the short stem implants that follow the “Mayo principle“ is a closed cortical femoral neck, responsible for a stable and torsion-free anchoring following the resection of the femoral head.8
The load transfer of implants with a multiple point fixation occurs meta- and short meta-diaphysically. This is important to facilitate a physiological stress while at the same time avoiding stiffening and stress shielding. In addition to the Mayo prosthesis itself that meets these criteria, one can find other systems such as Metha®, Aida®, Nanos®, BreXis®, Optimys®, MiniHip®. Alongside the Mayo® prosthesis, the CFP® implant can be seen as a second pioneer of the short stem philosophy. However, the CFP® prosthesis distinguishes by conserving the femoral neck with a combined metaphysical as well as diaphyseal anchoring. By adding a layer for the femoral neck, the CFP® prosthesis acts similar to a Thrust Plate Prosthesis® (TPP) and Spiron® prosthesis.
Systems resecting the femoral neck – so-called intermediate stems – can actually not be seen as short stem systems, since they are simply shortened straight stem. These systems may aim for a meta- to diaphyseal load transfer, but its resection as well as its bone loss goes along with the standard systems. Such models often display an oblique prosthesis shoulder to avoid the trauma of the trochanteric region and thereby create the possibility of a less invasive approach. Representatives are, for example, SMF®, Fitmore®, GTS®, Profemur Preserve®, Balance®, Tri-Lock®. The Proxima® prosthesis has a special feature because this system uses the cortical region of the major trochanteric region for its anchoring.
Patient Selection
Preliminary Remarks
In general, it is important to consider the individual demands and goals a patient has in order to choose the right prosthesis. It is a surgeon’s task, to evaluate patients’ specific problems and demands, to analyze the radiology in combination with clinical examination and to plan an intervention with a matching prosthesis based on these aspects.9 General aspects have to be taken into consideration: Soft tissue management, bone saving optimization, and the exact and stable placement of the prosthesis in order to reconstruct the hip geometry and establish a stable fixation.
While there are some short- and medium-term results, long-term results are still pending. This should also be taken into consideration when deciding whether using a standard prosthesis or a short stem system, like Metha®. Lastly, it has to be mentioned that a successful outcome of a short stem system does also depend on a surgeon’s experience.
Since the anchoring distance of the Metha® short stem is significantly shorter than that of the standard straight stems, it is very important to achieve an adequate fit and fill in order to have a stable primary anchoring. In this respect, attention to the preoperative femoral configuration is of great importance. Our own investigations of the Metha® prosthesis have shown that patients with a “normal” or “stovepipe configuration” can achieve a good fit and fill in most cases, while a “champagne glass configuration” tends to result in an undesirable distal one.10 Fit and Fill entices and accordingly the requirements for the preparation of the metaphysis are greater in such cases. It is thereby essential to achieve a cortical metaphyseal anchoring by choosing a sufficiently large prosthesis.11,12
In general, it must also be mentioned that short as well as wide femoral neck configurations can be regarded as relative contraindications for the Metha® hip stem, since sufficient primary stability is hardly achievable in these cases, and the risk of leg lengthening is also great.
Regardless of the initial diagnosis, bone quality plays a major role in establishing a Metha® short-stem prosthesis. However, this does not necessarily mean that a bone density analysis is generally needed to establish the indication, but if there is justified doubt about the load-bearing capacity of the bone of the proximal femur, a standard prosthesis should be indicated, which may then also be established in a cemented technique.
In our own routine, the possibility of an intraoperative system change is therefore always pointed out as part of the informed consent of the Metha® prosthesis. The direct intra-operative assessment of the bone quality is of crucial importance. It has been proven that it can be useful to strive for cortical anchoring of the short-stem prosthesis. Securing torsional stability should have already been achieved with the last rasp size, however, if this cannot be achieved, a standard prosthesis is used.
In addition to the quality of the bone, the femoral geometry must also be considered in order to correctly identify a Metha® prosthesis. CCD angles below 120° generally represent borderline or contraindications for this implant.
If the resection of the femoral neck is carried out very close to the base in such cases, an adequate size can be achieved, but the cortical femoral neck ring, which is a basic requirement for anchoring, is usually sacrificed and the prosthesis is immersed in the cancellous bone of the trochanter and loses its stability.
If, on the other hand, a part of the femoral neck is left, this affects the fit and fill and the prosthesis is often undersized and placed in an undesired varying position. As a rule, there is an unfavorable point contact between the tip of the prosthesis and the lateral cortex.
On the other hand, from our experience, the valgus hip is better feasible. With the femoral neck partial-preserving Metha® prosthesis, the tip of the prosthesis runs out in the direction of the medial cortex, sometimes touching it, as it reproduces the osseous valgus and erects accordingly.
Since, as already mentioned, it is essential to ensure that the size of the implant is adequate, a femoral neck resection closer to the base is often necessary in these cases and the anchoring of the prosthesis shifts more towards the diaphysis (Figure 2).
 |
Figure 2 Coxa valga et antetorta (A). A femoral neck resection close to the base leads to valgus alignment and more diap hyseal anchoring of the Metha® stem. The tips of the prostheses point medially (B and C). Data from Ishaque B.13 |
In the case of an additionally increased anteversion angle, a limited correction can be achieved with this stem by sloping the osteotomy posteriorly.
Metha® in Patients with Avascular Necrosis (AVN) of the Femoral Head
Idiopathic femoral head necrosis usually affects patients in the 3rd to 5th decade of life, and men are affected five times more often than women. The chances of success of a joint-preserving surgical measure such as retrograde drilling for decompression are very uncertain from necrosis stage ARCO III upwards and lead to a (partial) success in only about every fourth patient.14,15
Once the femoral head has lost its sphericity, secondary osteoarthritis occurs and the only option left in order to maintain active hip function is an endoprosthetic replacement. When choosing the implant, the extent of the necrosis area, on the one hand, and the generally young age of the patient, on the other hand, must be considered. Furthermore, the etiology of the femoral head necrosis should also be included in the considerations, as it has been shown that this has a decisive influence on the survival rate and the rate of complications of the endoprosthesis.16
The analysis of the bone matrix and trabecular cancellous architecture of the metaphysis show that a fundamental change in metabolism and microarchitecture can be expected and this reduces the load-bearing capacity of the cancellous bone.17 The reduction in biomechanical and biological bone quality can lead to early failure of a prosthesis, which is why the survival rates caused by post-traumatic and idiopathic femoral head necrosis are significantly better than, for example, in the cases of alcohol- or steroid-induced AVN.
Fink et al demonstrated a high failure rate in the purely metaphyseal anchoring TPP, especially in patients with AVN after kidney transplantation and in alcohol-induced femoral head necrosis.18 In contrast, Yasunaga et al evaluated a survival rate of 96.6% for 6 years, even though 20 of the 50 femoral head necroses treated with TTP’s were steroid or alcohol-induced. They performed MRI on all patients preoperatively and implanted the prosthesis if the necrosis zone did not protrude into the femoral neck region.19
Our own studies depicted a survival period of ten years in 95.1% when analyzing 62 patients with a femoral head necrosis that were supplied with a TPP (70 prostheses). However, success does partially correlate with the critical selection of patients.20,21 Since the cancellous bone is at least partially needed in order to achieve a femoral neck conserving anchoring, it is advised to detect necrotic expansions in the metaphysis by running an MRI prior to the insertion of such a system.
Short stem systems that partially preserve the femoral neck (Mayo principle) like the Metha® stem have the advantage that by using the cortical region for anchoring, a sufficient fit and fill in the metaphysis is achieved while simultaneously accomplishing a multiple point anchoring in the proximal epiphysis. Hence, the pathologically altered cancellous bone is removed while, on the other hand, the anchoring distance is greater and the involvement of the femoral neck metaphysis should be clarified by MRI. However, this should not consequently be interpreted as a contraindication. The usage of such a short stem system should then be placed in the context of the respective etiology, the femoral geometry, and the expected remaining lifetime alongside the advantages and disadvantages for the patients’ demands (Figure 3).
 |
Figure 3 Idiopathic femoral head necrosis with metaphyseal involvement ARCO III–IV (A and B). 4-year follow-up shows good osteointegration of the Metha® stem and slight calcar rounding (Engh I) (C and D). |
The indication for a short stem is set more generously in one’s own practice when treating very young patients who are highly likely to have two or more interventions in future (Figure 4). From the author’s point of view, the advantage of saving one generation of prosthesis with the help of the Metha® short-stem prosthesis prevails and justifies the slightly higher risk of an earlier loosening in cases of secondary femoral head necrosis, eg on the basis of steroid therapy.
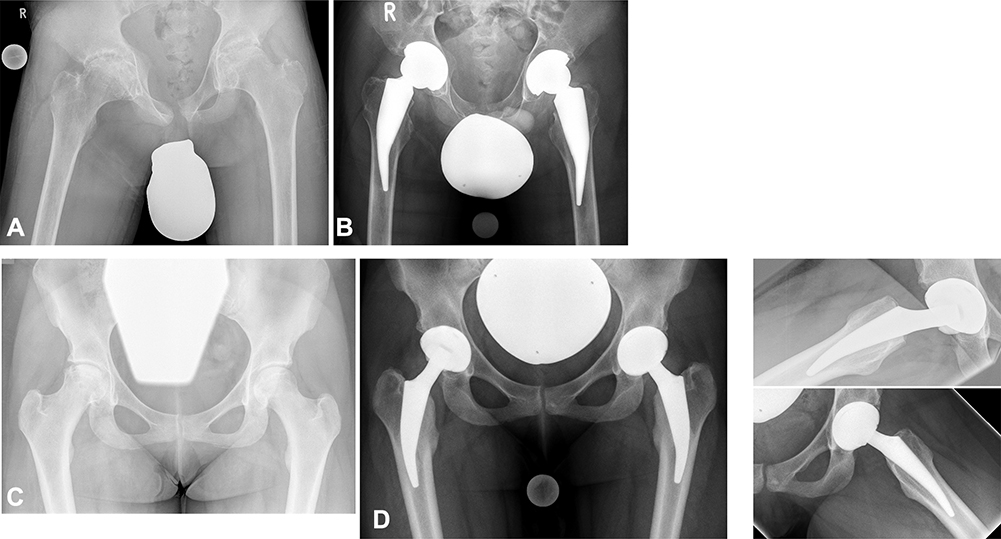 |
Figure 4 14-year-old boy with secondary femoral head necrosis on both sides after chemotherapy and radiotherapy for treating Hodgkin‘s disease (A). Despite the osteopenic bone situation, Metha® prostheses were performed due to the young age (B). 16-year-old girl with secondary femoral head necrosis on both sides following Chemotherapy and long-term cortisone treatment for acute lymphatic leukemia (C). 4-year follow-up after endoprosthetic treatment with Metha® prostheses (D). Data from Ishaque B.13 |
As a general rule, the area affected by the necrosis is removed with the osteotomy. While the earlier reports on results following hip prosthesis implantations with advanced AVN could be classified as sobering, the results and downtimes when using standard prostheses have approximated those of primary coxarthrosis, which can be attributed to improvements in bearing couples, implants and surgical techniques.
While the earlier reports on the results after hip replacement in the case of advanced avascular necrosis are devastating, the analysis of the survival rates when implanting a standard prosthesis approaches those of patients with primary coxarthrosis. Advancements in wearing couples in implants as well as surgery techniques can be seen as an explanation for this improvement.
Schneider and Knahr stated identical survival periods when comparing the initial diagnosis of femoral head necrosis with any other one. They figured out that solely the design of the implant does significantly influence its survival regardless of the initial diagnosis.22 In addition, Kim et al also stated earlier on that cement as well as cement-free implants reached very good results, comparable to those of patients with primary coxarthrosis. They similarly explained these findings with improvements in stem design, cement stems as well as cement-free implants and last but not least a better technique for cementing.23
If and to what extent one will achieve similar long-term results with the femoral neck region preserving short stem implants remains uncertain for now. Nowadays, only a few studies have discussed the usage of these implants in cases of avascular necrosis. However, the few existing reports on the use of these implants to treat AVN are very promising.24,25,26 Our own experiences of implanted short stems in patients with osteonecrosis of the femoral head since 2007 (96 cases with 94 Metha®; 2 Aida® and an average age of 40.5 (14–66 years)) are also very encouraging. In particular, the minimally invasive anterolateral approach (ALMI) was responsible for reaching outstanding clinical results during the three-month follow-up. Additionally, the radiological and DXA-analysis proved a very good osteological integrity of the prosthesis with a gain in bone matrix in Gruen zone 2–6, and a minimal loss in zones 1 and 7 throughout a period of 36 months.27
Merschin et al concluded that, in mid-term observation, the Metha® short-stem prosthesis shows no disadvantage in functional outcome and in survival time compared to a standard hip stem. From their point of view, the Metha® short stem is a valuable option in total hip arthroplasty for younger patients with avascular osteonecrosis of the femoral head, and the evaluation has shown no significant differences between aseptic osteonecrosis and other indications.28
In summary, the previous findings have shown that, in cases of an idiopathic avascular necrosis, the usage of a partially femoral neck preserving implants leads to reproducible results; however, only if the involvement of the femoral neck metaphysis is excluded by MRI. In case of a secondary necrosis, associated with a general reduction in bone metabolism, eg as a result of nephropathy, long-term corticosteroid therapy or immunosuppressive treatments, the use of this group of prostheses is not advisable. In contrast, the involvement of the necrosis zone in the femoral neck is not a contraindication of femoral neck partially preserving prostheses. When treating a patient with a simultaneous general reduction in the bone quality of the proximal femur, the use of these prostheses should depend on a critical evaluation of the femoral geometry as well as the predicted remaining lifespan.
Metha® in Patients with Rheumatic Diseases
The particular challenge of endoprosthetic treatment in patients suffering rheumatoid arthritis lies in their young age, on the one hand, and their poor bone quality, on the other hand. Additionally, a higher infection risk can definitely not be neglected as the immune system is significantly down regulated through this disease. The pathologically modified biological as well as mechanical bone competence was used as an argument for implanting cemented prostheses for quite a long time. Dangers from using a cement-free system were seen in the modified bone metabolism that might lead to an intra- or postoperative fracture surrounding the prosthesis as well as early aseptic loosening. In addition, the risk of stress shielding, which could contribute to the failure of these prostheses, was used as a contra argument for choosing a cement-free standard implant.
Meanwhile, on the other hand, many studies have shown that, when using cement-free standard straight shafts, reliable osteointegration and a long survival rates can be achieved.29,30 In addition, Eskelinen et al conducted a study of 2557 patients from the Finnish register and found that cement-free implants should be used for the treatment of young patients suffering rheumatoid arthritis.31 So, how can these findings be transferred to the indication of short stem hip systems in patients with rheumatic disease as there is lacking evidence for its success?
Fink et al analyzed the implantation of femoral neck preserving TPPs with metaphyseal anchorage in 42 patients with polyarthritis and an average age of 40.8. A sustainable improvement in the clinical score was depicted, however, alongside a failure of almost 15% during 26.1 months of follow-up. When compared to cementless standard prostheses, the TPP fared worse, so that the authors justified the use of that implant only with the argument of a simple revision.32 However, our own examinations on the same implant have shown that it is not always that simple as the subtrochanteric region is often already weakened by bolts and thrust plates, which is even more important in osteopenic bones and can lead to trochanteric fractures.20 Since femoral neck-preserving implants with purely metaphyseal anchoring depend on the integrity of the biological and mechanical properties of the femoral-neck cancellous bone and cortex, these implants should not be indicated in patients with rheumatic arthritis.
Bause‘s work is nowadays the only one that specifically discusses the implantation of the Metha® hip stem in patients with rheumatoid arthritis. It provides an overview of mid-term results utilizing a total number of 105 Metha® prosthesis.33 In order to successfully apply this system, it is essential to ensure a cortical fit of the prosthesis. The principle of a multiple point anchoring as well as the dorsolateral attachment of the prosthesis against the cortex are basic requirements for achieving a rotationally stable anchoring system and a primary stability overall. In particular, in patients with poor bone quality, a careful bone preparation is required and in addition, the postoperative regime has to address the special needs of patients with a reduced immune response in regard to prosthesis loosening and infection risk. In individual cases, it should be considered to only allow partial weight bearing for a couple of weeks following the intervention.
The question of whether using a cement-free standard system or a Metha® stem can ultimately only be answered during the surgery itself. Since the requirements are generally higher and the error tolerance is reduced, the indication and implantation of a short-stem in patients with rheumatoid arthritis should be reserved for surgeons who are well experienced in handling these prostheses. The advantage of such a treatment can be seen in reduced bone loss, physiological load transfer, as well as reduced soft tissue trauma when compared to a standard stem system.
Metha® in Patients with Developmental Dysplasia of the Hip (DDH)
The treatment of a secondary coxarthrosis following DDH is often challenging, especially for the higher Crowe degrees (II, III, IV). Reasons for this can be found in choosing the right-cup position, as well as in establishing matching stem components. It should also be taken into consideration that sometimes, patients in the middle stage of life underwent corrective surgeries in their youth that sustainably changed the geometry of the hip and bone structure. This is especially crucial when choosing the right prosthesis for the patient. In addition to the restoration of the hip rotation center, the frequently increased anteversion, a high CCD angle and the dysplastic meta-diaphyseal junction must be critically assessed and play an important role in the indication. Femoral neck-preserving short-stem implants with a metaphyseal anchoring philosophy cannot usually be established in the case of increased anteversion (> 20°). A high CCD of >140° must also be viewed as unsuitable for such systems. In addition, past inter-trochanteric varisation- and derotation osteotomies are a relative contraindication. Classical dysplasia prostheses, such as the Wagner cone or the modular SROM system, are preferred in these situations.
In the case of femoral neck partial-preserving short stem prostheses that anchor according to the Mayo principle – like the Metha® stem – and have a clear tapering shaft geometry in the distal direction, the anteversion can be corrected within certain limits with the help of a posteriorly sloping osteotomy (Figure 5).
 |
Figure 5 42-year old woman with dysplasia coxartrosis following Salter procedure and derotation osteotomy in childhood (A). Leg length and offset could be successfully reconstructed with the short stem (B). The increased anteversion was corrected by a slight posterior tilt of the osteotomy (yellow line) (C). |
The surgeon should be aware that the increased shaft anteversion with partial retention of the femoral neck harbors the risk of causing dorsomedial cortical penetration with a via falsa and also predisposes the narrow femoral neck to fissures. On the other hand, since achieving a good fit and fill is very important, the femoral neck resection must be carried out close to the base, but with a circumferentially closed cortical ring. The anchoring of the Metha® stem then shifts more in the direction of the diaphysis, but compared with standard diaphyseal prostheses, a more proximal application of load is generated and cortical hypertrophies and thigh pain syndromes, as they are known from the conical prosthesis, among others, are avoided. A high CCD angle (up to 140°) often poses no problems for such short-stem systems and the dysplastic meta-diaphyseal junction and narrow medullary canal do not even allow the implantation of a standard prosthesis in some cases, so that either an individualized stem-anchoring prosthesis has to be made, but it is better to use a suitable short-stem prosthesis system. Our own observations have shown that aligning the top of the stem towards the medial side when treating valgus deformities did not lead to any disadvantage later on. Suksathien et al evaluated promising results in patients with developmental hip dysplasia (Crowe I and II) after receiving a Metha® short stem. In comparison to conventional stems, short stem showed less thigh-pain, slightly more natural joint feeling and more patients’ preferred hip. Furthermore, the short stem provided more favorable results for proximal load transfer and less stress shielding.34
Jerosch was the first who even reported about the treatment of severe developmental dysplasia of the hip (DDH Crowe type IV) using a short stem (MiniHip® prosthesis) and saw an advantage of the system especially in the tapering of the prosthesis in the distal direction and the relation to the narrow diaphysis as an advantage of the system compared to standard prosthesis, which is often seen reaming of the medullary canal becomes necessary.
After the short-stem prosthesis had been implanted, the shortening and derotation osteotomy was placed below the stem tip and secured with an angle locking plate.35 The same procedure in the case of developmental high hip dislocation was performed using Metha® short stem by the author of this review (Figure 6).
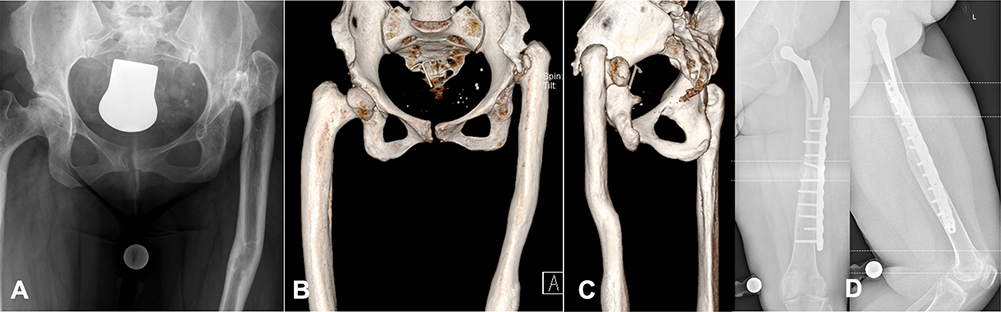 |
Figure 6 High hip developmental dislocation (Crowe IV) (A). An Ilizarov leg lengthening procedure was performed years ago with the result of a massive curvature of the diaphysis (B and C). Metha® short stem was established after a diaphyseal shortening and derotation osteotomy which was secured by an angle locking plate (D). |
Our own experiences with dysplasia coxarthrosis using the Metha® prosthesis can also be rated as consistently positive. Since 2007, 106 cases with an average age of 52 years (19–71) have been successfully treated. An intraoperative fissure in the area of the calcar femoris was treated without additional cerclage with partial weight bearing for 6-weeks.
Small prosthesis sizes were used in about two thirds of all cases. Depending on the needs, a certain correction regarding leg length and offset could be achieved by selecting different CCD variants of the implant. None of the patients had to be revised in the previous follow-up and the regular clinical, radiological and osteo-densitometric examinations showed excellent results with occasional signs of mild stress shielding grade 1 according to Engh (Calcar Rounding).
In summary, it can be stated that a femoral neck partial-preserving short-stem prosthesis is a good alternative to a standard implant in the endoprosthetic treatment of dysplasia coxarthrosis. Essential requirement is the exact assessment of the existing geometry as well as the preoperative planning. Furthermore, the femoral neck osteotomy is of great importance so that the indication and usage of such a short-stem belongs in the hands of those being experienced.
Metha® in the Elderly Patient Group
Regarding the epidemiological development as well as the knowledge that increased activity levels lead to increased stress on the joint with the consequence of increased revision rates among under 50-year-olds and furthermore the demand for a soft tissue-gentle, bone-saving primary care is growing, short stem prosthetics have meanwhile become firmly established for the endoprosthetic treatment of younger patients.36 The question therefore arises as to whether the advantages that lie in this care strategy can also be transferred to the elderly patient population and whether the use of these prosthesis systems can be recommended and indicated. In general, until recently, the implantation of a short-stem prosthesis should be reserved for younger patients, also against the background that the bone quality declines with increasing age and the manufacturer’s recommendations were formulated accordingly.
For femoral neck-preserving short stem prostheses with a solely metaphyseal anchoring philosophy, which are dependent on the load-bearing capacity of the femoral neck cancellous bone, the use in older patients seems to be unsafe. Long-term examinations of the TPP have shown that when compared to patients under and over 50 years of age, the younger patient group achieved significantly better survival rates (94% for 13.6 years versus 87% for 13.1 years).37 There is enough evidence to achieve survival rates of 15 years in 95% when implanting a standard prosthesis in older patients. There are not enough advantages by using a short stem system to justify its implantation as most of these patients will not survive a revision surgery.
The Metha® stem that preserves the femoral neck partially and that achieves meta-diaphyseal anchoring according to the multi-point principle and cortical support is, according to the current data, equivalent to cementless standard stems in terms of its primary stability.38 With regard to its secondary stability and peri-prosthetic bone remodeling processes, the stem cannot achieve physiological conditions, but causes a proximal load transfer and thus significantly lower signs of stress shielding than cement-free standard stems. Our own DXA studies of the Metha® stem show in the course of the first 12 months that in patients over 65 years of age, the changes in bone density regarding their amplitudes are weakened in both positive and negative directions and a significant difference compared to only in green zone 2 under 65-year-old patients.39,12
Jakubowitz et al were able to refute the argument that the implantation of these short-stem prostheses would be associated with a greater risk of developing intra- or post-operative fractures in their bio-mechanical study and found an equally high risk of such fractures when choosing the CLS or Mayo shaft.40 In this respect, the usage of such prostheses in the treatment of elderly patients is only opposed to shorter follow-up periods, and longer-term survival time analyses that are not yet available. However, the medium-term results available so far are so encouraging that in one’s own routine the use of the Metha® short stem prosthesis is made dependent less on the numerical age than on the biological age and then ultimately on the advantages associated with the soft tissue-sparing surgical technique justify the implantation, even if, in view of the implant prices, this usually entails higher costs. We usually use cemented standard stems for patients who have advanced both age-numerically and biologically.
The previously mentioned relationships also seem to apply to femoral neck-resecting short stem prostheses. So, Kim et al came to the result that the use of the femoral neck resecting short stem prosthesis Proxima leads to stable anchoring in both younger and older patients and osteointegration was recorded in every case. The follow-up period in the group of older patients (mean age 78.9 years) was a maximum of 9 years. None of the 114 prostheses had to be revised during this period.41
Our own study group examined the clinical results and the age-related osteointegration of the Metha® short stem in a 24 months follow-up. We saw no significant differences or any influences of osseointegration and clinical outcome of the short hip stem in older patients and concluded that the Metha® prosthesis seems to be an adequate treatment for THA also for older patients.42
In summary, the higher numerical age does not represent a general exclusion criterion for the indication of a short-stem prosthesis.
Metha® in Obese Patients
The probability of intra- and postoperative complications is generally increased in patients with high body weight and high body mass index (BMI). Traina et al found that the BMI was less than the increased absolute weight (> 80 kg) in combination with the male gender that had a negative impact on the survival of prosthesis.43 Chammai and Brax compared the medium-term results of patients with BMI over and under 30kg/m2 after treatment with the Metha® short-stem prosthesis and found somewhat poorer absolute results of the HHS in the group of obese patients, but the gain was identical in both groups and the mean prosthesis life was the same in both groups (96%/50 months). Due to the risk of cone fracture, modular prostheses should not be used in patients over 100 kg.44
Reviewing our own files of more than 900 cases of femoral neck partial preserving short stems shows that every fourth patient had an absolute weight of 90 kg and more and every second of these weighed > 100 kg. A related prosthesis-specific problem has not yet been objectified. While a postoperative partial weight bearing of 3–6 weeks was specified for these patients in the course of the learning curve at the beginning, the postoperative treatment regime provides for immediate full weight bearing in the meantime.
Experience to date suggests that obesity is not a contraindication for femoral neck partial preserving or neck resecting monobloc implants with meta and (short) diaphyseal anchoring like the Metha® stem. Achieving an adequate fit and fill is crucial to secure a primary stability and subsequent osteointegration of such short-stem prostheses. In this respect, there are no differences to standard prostheses with regard to the indication. In general, however, in the case of extreme obesity (BMI > 40 kg/m2), it must be clarified whether measures to reduce weight should not be realized prior to any endoprosthetic treatment.
Metha® in Patients with Post-Traumatic-, Post-Perthes Disease or Other Deformities of the Hip
Regardless of the etiology, in some cases, malposition of the proximal femur can be addressed very comfortably and with significantly less effort than with a standard prosthesis. This applies in particular to axial deformities of the proximal femoral diaphysis, in which a revision osteotomy is necessary to implant standard prostheses and the use of modular revision systems is then often unavoidable. Even in the case of remaining osteosynthesis materials that obstruct diaphysis, the use of short-stem prostheses can have a positive effect. For example, Mont et al published on the use of the neck-preserving MiniHip® in a patient who had received retrograde nailing seven years earlier due to a femoral fracture and who explicitly did not want any additional surgery to remove the material.45
For the treatment of an aged femoral neck fracture, the use of a femoral neck partial preserving short stem prosthesis like Metha® can be particularly useful when the patient is still comparatively young and stable primary anchoring is achieved intraoperatively.
Various patients with post-traumatic deformities, post-Perthes condition and post-ECF situation have already been successfully supplied with the Metha® short stem in our own patients, so that it can be regarded as the implant of first choice in some of these cases (Figure 7).
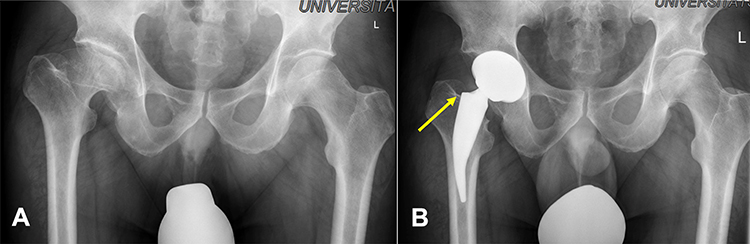 |
Figure 7 Coxarthrosis after Perthes’ disease (A). Metha® stem could be successfully established due to a closed cortical femoral neck ring (yellow arrow) (B). |
Learning Curve
As with any new prosthetic system, the surgeon goes through a learning curve on the way to reproducible results. This could be determined for the THA but exemplary, as well as for ankle prosthetics.46,47 The primary anchorage is particularly important for the successful and permanent fixation of the Metha® prosthesis. This requires cortical clamping of the prosthesis in the closed femoral neck ring as well as a good fit and fill. In the course of an initial learning curve, errors can arise here.
On the one hand, when performing the femoral neck resection, there is a risk that the resection will be too deep and the ring structure of the femoral neck will be lost, which then no longer allows the Metha® short stem to be established. On the other hand, if you choose an oversized prosthesis, there is a potential danger of fractures. A total of three fissural fractures occurred in our own collective, two of which could be healed with cerclage and one other conservatively.
On the other hand, there is a risk of not establishing a sufficient fit and fill due to an undersized prosthesis, which can subsequently lead to a caudally directed migration of the prosthesis.
In our own group of patients, it was shown that femoral neck resections became more reproducible with an increasing number of surgical treatments and that the fit and fill also improved. In addition, the operating times could be reduced. With increasing expertise, it is possible to expand the range of indications.
Conclusion
Short stem endoprosthesis, using the Metha® prosthesis, has developed into a good and safe alternative to the cementless standard endoprosthesis over the past 15 years. Malahias et al concluded that all mean clinical outcome scores that were used in various studies illustrated significant postoperative improvement when compared with the respective initial values. The revision rate of the Metha® stem for component-related reasons was 2.5%, while the rate of major complications not requiring revision of the Metha® stem was 2.8%.48
Advantages can be seen especially in soft tissue-sparing and bone-saving implantation technique, high primary stability and good osteointegration as well as a wide range of indications. However, as a requirement for a successful use of the prosthesis, a good fit and fill with cortical anchoring in the closed femoral neck ring is extremely important. Precise preoperative planning and exact surgical technique are crucial.
The demanding relative indications described above, such as congenital dysplasia hip or other hip deformities, should only be addressed after a successful learning curve. Even though the short- and medium-term results are promising and the Metha® hip stem shows some advantages in comparison to conventional stems, further studies are needed to evaluate long-term results.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Iorio R, Healy WL, Presutti AH. A prospective outcomes analysis of femoral component fixation in revision total hip arthroplasty. J Arthroplasty. 2008;23:662–669. doi:10.1016/j.arth.2007.06.009
2. Wengler A, Nimptsch U, Mansky T. Hip and knee replacement in Germany and the USA – analysis of individual in patient data from German and US Hospitals for the years 2005 to 2011. Dtsch Arztebl Int. 2014;111:407–416. doi:10.3238/arztebl.2014.0407
3. Springer BD, Fehring TK, Griffin WL, Odum SM, Masonis JL. Why revision total hip arthroplasty fails. Clin Orthop. 2009;467:166–173. doi:10.1007/s11999-008-0566-z
4. Thorey F, Lerch M, Kiel H, von Lewinski G, Stukenborg-Colsman C, Windhagen H. Revision total hip arthroplasty with an uncemented primary stem in 79 patients. Arch Orthop Trauma Surg. 2008;128:673–678. doi:10.1007/s00402-007-0462-0
5. Schnurr C, Schellen B, Dargel J, Beckmann J, Eysel P, Steffen R. Low short-stem revision rates: 1–11 year results from 1888 total hip arthroplasties. J Arthroplasty. 2017;32:487–493. doi:10.1016/j.arth.2016.08.009
6. Wittenberg R, Steffen R, Windhagen H, Bücking P, Wilcke A. Five-year results of a cementless short-hip-stem prosthesis. Orthop Rev. 2013;19:16–22.
7. Jerosch J. Ist kürzer wirklich besser? Philosophie der Kurzschaftendoprothesen Orthopäde [Is shorter really better? Philosophy of short stem prosthesis designs]. 2011;40:1075–1083.
8. Whiteside LA, White SE, McCarthy DS. Effect of neck resection on torsional stability of cementless total hip replacement. Am J Orthop. 1995;24:766–770.
9. Schmidutz F, Steinbrück A, Wanke-Jellinek L, Pietschmann M, Jansson V, Fottner A. The accuracy of digital templating: a comparison of short-stem total hip arthroplasty and conventional total hip arthroplasty. Int Orthop. 2012;36(9):1767–1772. doi:10.1007/s00264-012-1532-7
10. Noble PC, Alexander JW, Lindahl LJ, Yew DT, Granberry WM, Tullos HS. The anatomic basis of femoral component design. Clin Orthop Relat Res. 1988;235:148–165. doi:10.1097/00003086-198810000-00015
11. Issa K, Pivec R, Wuestemann T, Tatevossian T, Nevelos J, Mont MA. Radiographic fit and fill analysis of a new second- generation proximally coated cementless stem compared to its predicate design. J Arthroplasty. 2014;29(1):192–198. doi:10.1016/j.arth.2013.04.029
12. Jahnke A, Engl S, Seeger JB, Basad E, Rickert M, Ishaque BA. Influence of fit and fill following hip arthroplasty using a cementless short-stem prosthesis. Arch Orthop Trauma Surg. 2015;135(11):1609–1614. doi:10.1007/s00402-015-2302-y
13. Ishaque B. Indikationen für die Kurzschaftendoprothetik. [Indications for short-stem arthroplasty]. In: Jerosch J, editor. Kurzschaftendoprothesen an der Hüfte. Springer Verlag Deutschland; 2017:45–59.
14. Gardeniers J. A new international classification of osteonecrosis of the ARCO (Association Research Circulation Osseous) Committee. ARCO-News. 1992;4:41–46.
15. Smith SW, Fehring TK, Griffin WL, Beaver WB. Core decompression of the osteonecrotic femoral head. J Bone Joint Surg Am. 1995;77:674–680. doi:10.2106/00004623-199505000-00003
16. Fink B, Rüther W. Teil- und Totalgelenkersatz bei Hüftkopfnekrosen. Orthopäde. 2000;29:449–456. doi:10.1007/s001320050466
17. Tingart M, Beckmann J, Opolka A, et al. Analysis of bone matrix composition and trabecular microarchitecture of the femoral metaphysis in patients with osteonecrosis of the femoral head. J Orthop Res. 2009;27(9):1175–1181. doi:10.1002/jor.20873
18. Fink B, Schneider T, Conrad S, Jaeger M, Protzen M, Ruther W. The thrust plate prosthesis in patients with aseptic osteonecrosis of the femoral head. Arch Orthop Trauma Surg. 2002;122:499–505. doi:10.1007/s00402-002-0422-7
19. Yasunaga Y, Goto T, Hisatome T, Tanaka R, Yamasaki T, Ochi M. Bone-preserving prosthesis with a single axis for treating osteonecrosis of the femoral head: midterm results for the thrust plate hip prosthesis. J Orthop Sci. 2003;8:818–822. doi:10.1007/s00776-003-0710-2
20. Ishaque BA, Gils J, Wienbeck S, Donle E, Basad E, Stürz H. Ergebnisse nach Wechsel von Schenkelhalsprothesen – Druckscheibenprothese versus ESKA-Cut-Prothese [Results after replacement of femoral neck prostheses - Thrust-plate prosthesis (TPP) versus ESKA-Cut prosthesis]. Z Orthop Unfall. 2009;147:79–88. doi:10.1055/s-2008-1038992
21. Ishaque BA, Wienbeck S, Basad E, Stürz H. Klinische und radiologische Ergebnisse bei Patienten mit Druckscheibenprothese (DSP) bei Patienten mit Femurkopfnekrose [Clinical and radiological results of the Thrust plate prosthesis (TPP) in patients with aseptic necrosis of the femoral head]. Z Orthop Unfall. 2005;143:622–630. doi:10.1055/s-2005-918187
22. Schneider W, Knahr K. Total hip replacement in younger patients – survival rate after avascular necrosis of the femoral head. Acta Orthop Scand. 2004;75(2):142–146. doi:10.1080/00016470412331294385
23. Kim YH, Oh JH, Oh SH. Cementless total hip arthroplasty in patients with osteonecrosis of the femoral head. Clin Orthop. 1995;320:73–78.
24. Floerkemeier T, Budde S, Gronewold J, et al. Cementless short stem hip arthroplasty METHA as an encouraging option in adults with osteonecrosis of the femoral head. Arch Orthop Trauma Surg. 2012;132:1125–1131. doi:10.1007/s00402-012-1524-5
25. Jerosch J, Grasselli C, Kothny C. Is there an indication for a partial neck preserving short stem (MiniHip) in patients with an avascular necrosis of the femoral head? OUP. 2014;4:178–183.
26. Zeh A, Weise A, Vasarhelyi A, Bach AG, Wohlrab D. Medium-term results of the Mayo short-stem hip prosthesis after avascular necrosis of the femoral head. Z Orthop Unfall. 2011;149:200–205. doi:10.1055/s-0030-1270710
27. Basad E, Ishaque BA, Stürz H, Jerosch J. The anterolateral minimally invasive approach for total hip arthroplasty: technique, pitfalls, and way out. Orthop Clin North Am. 2009;40:473–478. doi:10.1016/j.ocl.2009.05.001
28. Merschin D, Häne R, Tohidnezhad M, Pufe T, Drescher W. Bone-preserving total hip arthroplasty in avascular necrosis of the hip-a matched-pairs analysis. Int Orthop. 2018;42(7):1509–1516. doi:10.1007/s00264-018-3896-9
29. Loehr JF, Munzinger U, Tibesku C. Uncemented total hip arthroplasty in patients with rheumatoid arthritis. Uncemented total hip arthroplasty in patients with rheumatoid arthritis. Clin Orthop Relat Res. 1999;366:31–38. doi:10.1097/00003086-199909000-00005
30. Zwartele R, Peters A, Brouwers J, Olsthoorn P, Brand R, Doets C. Long-term results of cementless primary total hip arthroplasty with a threaded cup and a tapered, rectangular titanium stem in rheumatoid arthritis and osteoarthritis. Int Orthop. 2008;32:581–587. doi:10.1007/s00264-007-0383-0
31. Eskelinen A, Paavolainen P, Helenius I, Pulkkinen P, Remes V. Total hip arthroplasty for rheumatoid arthritis in younger patients: 2557 replacements in the Finnish arthroplasty register followed for 0–24 years. Acta Orthopaedica. 2006;77:853–865. doi:10.1080/17453670610013132
32. Fink B, Siegmüller C, Schneider T, Conrad S, Schmielau G, Rüther W. Short- and medium-term results of the thrust plate prosthesis in patients with polyarthritis. Arch Orthop Trauma Surg. 2000;120:294–298. doi:10.1007/s004020050468
33. Bause L. Short stem hip arthroplasty in patients with rheumatoid arthritis. Orthopaedics. 2015;38(3):46–50. doi:10.3928/01477447-20150215-56
34. Suksathien Y, Suarjui J, Ruangboon C, Akkrasaeng T. Mid-term results of short versus conventional cementless femoral stems in patients with bilateral osteonecrosis of the femoral head. Eur J Orthop Surg Traumatol. 2021;31(2):319–325. doi:10.1007/s00590-020-02777-1
35. Jerosch J. MiniHip. In: Jerosch J, editor. Kurzschaftendoprothesen Wo liegen die Unterschiede [Short stem endoprostheses. What are the differences?]. Deutscher Ärzte-Verlag; 2013:139–170.
36. McAuley JP, Szuszczewicz ES, Young A, et al. Total hip arthroplasty in patients 50 years and younger. Clin Orthop Relat Res. 2004;418:119–125. doi:10.1097/00003086-200401000-00019
37. Wienbeck S, Osada H, Stürz H, Ishaque BA, Ishaque BA. Langfristige Analyse der Druckscheibenprothese Vergleich von Patienten unter und über 50 Jahren [Long-term results of the thrust plate prosthesis: comparison of patients younger than and older than 50 years]. Orthopäde. 2011;40:206–216. doi:10.1007/s00132-010-1728-8
38. Jerosch J. Wieviel Stabilität kann man von Kurzschaftendoprothesen an der Hüfte erwarten? [How much stability can you expect from short-stem hip arthroplasty?]. MOT. 2015;4:16–18.
39. Gils J, Koblitz F, Seeger J, Ahmed G, Basad E, Ishaque B. Die Metha Prothese bei Patienten über 65 Jahre: eine 1 Jahres Kontrolle [Metha prosthesis in patients over 65 years: a 1-year follow-up]. DKOU. 2014. doi:10.3205/14dkou183
40. Jakubowitz E, Seeger JB, Lee C, Heisel C, Kretzer JP, Thomsen MN. Do short-stemmed-prostheses induce periprosthetic fractures earlier than standard hip stems? A biomechanical ex-vivo study of two diVerent stem designs. Arch Orthop Trauma Surg. 2008;7:653–659.
41. Kim YH, Park JW, Kim JS. Behaviour of the ultra-short anatomic cementless femoral stem in young and elderly patients. Int Orthop. 2013;37:2323–2330. doi:10.1007/s00264-013-2044-9
42. Boller S, Jahnke A, Augustin L, Ahmed A, Rickert M, Ishaque BA. Age-related osteointegration of a short hip stem: a clinical and radiological 24 months follow-up. Arch Orthop Trauma Surg. 2019;139:405–410. doi:10.1007/s00402-018-3082-y
43. Traina F, Bordini B, De Fine M, Toni A. Patient weight more than body mass index influences total hip arthroplasty long term survival. Hip Int. 2011;21:694–699. doi:10.5301/HIP.2011.8879
44. Chammai Y, Brax M. Medium-term comparison of results in obese patients and non- obese hip prostheses with Metha short stem. Eur J Orthop Surg Traumatol. 2015;25:503–508. doi:10.1007/s00590-014-1574-1
45. Mont MA, Pivec R, Issa K, Harwin SF. Short stem option for total hip arthroplasty with retained hardware. Orthopedics. 2013;36:770–772. doi:10.3928/01477447-20130920-04
46. Maccario C, Tan EW, Di Silvestri CA, Indino C, Kang HP, Usuelli FG. Learning curve for total ankle replacement using transfibular approach. Foot Ankle Surg. 2021;27(2):129–137. doi:10.1016/j.fas.2020.03.005
47. Padilla JA, Anoushiravani AA, Feng J, Schwarzkopf R, Slover J, Scott M. The learning curve following adoption of a novel short-stem prosthesis in total hip arthroplasty: implications on short term patient outcomes. Eur J Orthop Surg Traumatol. 2019;29:819–825. doi:10.1007/s00590-018-2355-z
48. Malahias M-A, Tejaswi P, Chytas D, Kadu V, Karanikas D, Thorey F. The clinical outcome of the Metha short hip stem: a systematic scoping review. Hip Int. 2021;31:24–33. doi:10.1177/1120700020903719
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.