Back to Journals » International Journal of General Medicine » Volume 18
Shawarma and Salmonella Enteritidis: Tracing a 2020 Foodborne Outbreak in Ain Al-Basha, Jordan
Authors Alsulaiman JW ![]() , Slaihat A, Kheirallah KA
, Slaihat A, Kheirallah KA ![]() , Alrawashdeh A, Haddad SZ, Abdel Al AM
, Alrawashdeh A, Haddad SZ, Abdel Al AM ![]() , Al Bataineh GH, Alazzam RM, Bashyreh MI, Al-Nusair MM
, Al Bataineh GH, Alazzam RM, Bashyreh MI, Al-Nusair MM ![]() , Hulliel AF, Al Zein EI, Bellizzi S, AlZoubi H
, Hulliel AF, Al Zein EI, Bellizzi S, AlZoubi H
Received 9 February 2025
Accepted for publication 14 May 2025
Published 10 June 2025 Volume 2025:18 Pages 3011—3019
DOI https://doi.org/10.2147/IJGM.S517468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Jomana W Alsulaiman,1 Akef Slaihat,2 Khalid A Kheirallah,2 Ahmad Alrawashdeh,3 Said Z Haddad,2 Amjed M Abdel Al,2 Ghaith Hussein Al Bataineh,2 Reem M Alazzam,2 Marah Ibrahim Bashyreh,2 Mohammed M Al-Nusair,2 Atef F Hulliel,2 Eva Inam Al Zein,2 Saverio Bellizzi,4 Hamed AlZoubi2
1Department of Pediatrics, Medical School of Yarmouk University, Irbid, Jordan; 2Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 4World Health Organization (WHO), Jordan Country Office, Amman, Jordan
Correspondence: Khalid A Kheirallah, Department of Public Health, Community Medicine, and Family Medicine, Faculty of Medicine, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel +962 7 9611 9094, Email [email protected]
Background: This study investigated a severe foodborne outbreak in Ain Al-Basha, Jordan, linked to a fast-food restaurant offering chicken shawarma meals. The outbreak highlighted systemic lapses in food safety, particularly in handling and preparing poultry products, underscoring the need for immediate public health intervention.
Methods: Outbreak data collected by rapid response teams from the Jordan Ministry of Health (MOH), were analyzed. A case was defined as any individual who visited healthcare centers within the Al-Balqa Governorate between July 27 and August 2, 2020, presenting with two or more of the following symptoms: fever, diarrhea, vomiting, abdominal pain, or headache. Descriptive statistics were used to summarize demographic, clinical, and exposure characteristics.
Results: A total of 472 confirmed cases were identified, with a mean (standard deviation [SD]) age of 20.8 (13.4) years. The most frequently reported symptoms were fever (98.3%), abdominal pain (96.8%) and vomiting (96.0%). Most cases reported consuming chicken shawarma (86.0%), garlic sauce (83.1%), or French fries (79.9%). Of the 56 stool specimens tested, 100% tested positive for Salmonella enteritidis. Food samples revealed Enterococcus faecalis and Campylobacter spp. contamination in marinated raw chicken, indicating cross-contamination and improper cooking. Salmonella enteritidis was not detected in food items.
Conclusion: This outbreak underscores critical gaps in food safety practices related to shawarma preparation in Jordan. These findings call for stronger regulations, regular inspections, and focused public education on safe food handling, particularly for vulnerable populations. Timely action to enforce stricter protocols is vital to prevent further outbreaks and protect public health.
Keywords: food-borne disease outbreak, chicken shawarma, Salmonella, food safety, Jordan
Introduction
Foodborne illnesses account for more than 200 diseases worldwide, ranging from mild and self-limiting gastrointestinal disturbances to debilitating and life-threatening conditions, which can ultimately lead to death.1–4 Globally, an estimated 600 million individuals, or nearly 1 in 10, fall ill annually from consuming contaminated food, resulting in approximately 420,000 deaths annually and a loss of 33 million healthy life years.5 Within this global context, the Eastern Mediterranean Region (EMR) has the third highest documented burden of foodborne illnesses per population, following Africa and Southeast Asia, with an estimated 100 million people falling ill annually, including 32 million children under five years of age.3 Diarrheal diseases in EMR account for approximately 70% of the burden of foodborne diseases, mainly caused by Escherichia Coli, Norovirus, Campylobacter, and Non-typhoidal Salmonella.3 Nevertheless, the available literature on foodborne illnesses from EMR is scarce, particularly regarding surveillance practices and epidemiological investigations of outbreaks.6 This scarcity may be related to fragile public health infrastructure and poorly developed prevention and control strategies, including insufficient regulatory standards, enforcement, educational interventions, applied research, epidemiological information systems, and adverse environmental and economic conditions exacerbated by conflicts and wars.3,6,7
Previous outbreaks in Jordan and neighboring countries further underscore the vulnerability of the region to foodborne hazards. For instance, in 2003–2004, an estimated 15,000 cases of Salmonella infections were reported in Jordan, linked to contaminated poultry products.8 Similarly, Lebanon documented a significant burden of Salmonella infections, with outbreaks often traced to street food vendors and inadequate food handling practices.9 In Iraq, outbreaks of Brucella and Salmonella have been recurrent, highlighting systemic gaps in food safety regulation and enforcement.3 Despite these challenges, national surveillance programs were in place in Jordan prior to this outbreak, primarily managed by the Ministry of Health (MOH) and the Jordan Food and Drug Administration (JFDA). These programs focused on monitoring foodborne pathogens and conducting outbreak investigations but faced limitations in terms of resource allocation, laboratory capacity, and data integration.
Given the critical public health knowledge gap in systematically reporting foodborne disease investigations, the present study utilized available surveillance data from the Jordan Ministry of Health (MOH) to describe a national foodborne outbreak believed to have originated from a fast-food restaurant offering a Shawarma meal deal on July 24, 2020. Furthermore, this study aimed to describe the epidemiology, clinical presentation, and laboratory findings of a foodborne outbreak in the Ain Al-Basha area of Jordan, thereby highlighting the critical gaps in food safety practices.
Methods
Study Design and Settings
A descriptive cross-sectional outbreak investigation was conducted in Ain Al-Basha, a small town located 20 km from the capital Amman, and administratively part of the Al Balqa Governorate. The estimated population of Ain Al-Basha is approximately 300,000 (Data secured from the Jordan Department of Statistics). At the time of this outbreak, the area included four primary hospitals, 22 pharmacies, and more than 20 primary healthcare centers. Given Ain Al-Basha’s dense population and multiple fast-food outlets, local authorities consider it a high-risk setting for potential foodborne disease outbreaks.
Outbreak Description and Investigation
On July 27, 2020, soon after the strict COVID-19 lockdown in Jordan ended, multiple patients presented to the emergency departments across Ain Al-Basha hospitals, healthcare centers, and private clinics with fever, diarrhea, vomiting, abdominal pain, and headaches. Symptom onset was first reported on July 26, 2020, and medical care was sought on July 27. Rapid response teams from local health directorates were deployed to further investigate the potential outbreaks. These teams interviewed all the patients who visited public healthcare providers (hospitals and health centers) and reported the aforementioned symptoms. A standardized questionnaire was administered to document the signs, symptoms, onset date, and retrospective exposure to the suspected food items. Medical records were reviewed to validate self-reported symptoms and stool, food, and water samples were collected for laboratory testing. Owing to limited resources and ongoing COVID-19 contact tracing, investigations focused solely on Ain Al-Basha and only collected data from cases; that is, no controls were interviewed.
Exposure Assessment
A local fast-food restaurant linked to the reported cases is known to serve shawarma (grilled chicken sandwich), zinger, and broasted/fried chicken as the main dishes, with fries, pickles, garlic sauce, and coleslaw offered as side items. Around the outbreak date, this restaurant offered a 1 JOD (~ 1.4 USD) chicken shawarma meal deal that included French fries, garlic sauce, and pickles, alongside a sliced shawarma sandwich. Preliminary findings suggest that foodborne transmission is associated with fast-food consumption in the same area. Overall, 472 individuals presented with gastrointestinal symptoms.
Case Definition and Ascertainment
During the MOH outbreak investigation, a case was defined as
Any individual who visited local hospitals or healthcare centers within the Al Balqa Governorate between July 27 and August 2, 2020, with two or more of the following five symptoms: fever, diarrhea, vomiting, abdominal pain, and headache.
Cases were identified and enrolled if they met the inclusion criteria. The interview data included demographics, date and time of the first clinical manifestation, and food exposure at the suspected restaurant.
The selection of these symptoms—fever, diarrhea, vomiting, abdominal pain, and headache—was based on their alignment with the clinical presentation of common foodborne illnesses, particularly those caused by Salmonella and other enteric pathogens. These symptoms are consistent with WHO guidelines for investigating foodborne disease outbreaks, which emphasize the inclusion of gastrointestinal and systemic symptoms commonly associated with bacterial and viral foodborne infections.1 Additionally, the case definition was informed by previous outbreak investigations in Jordan and neighboring countries, where similar symptom profiles were observed in cases linked to contaminated food sources.8,9 While the case definition was not derived from a single source, it reflects a combination of clinical experience, epidemiological evidence, and standard practices for identifying potential cases during foodborne disease outbreaks.
Laboratory Investigations
Stool specimens were analyzed for common foodborne pathogens, including Salmonella, Shigella, and other enteric bacteria, following the standard protocols of the MOH. Samples of raw chicken, prepared shawarma, and water were subjected to microbiological testing by accredited laboratories associated with the Jordan Food and Drug Administration (JFDA) and the MOH. The analysis included culture-based methods and biochemical testing to identify Salmonella spp. and other organisms. The testing procedures adhered to JFDA standards and were supplemented by further environmental assessments of food handling and storage practices.
Pathogen Isolation and Identification
Culture Media
Stool samples were inoculated onto selective and differential media, including Xylose Lysine Deoxycholate (XLD) agar and MacConkey agar, to isolate Salmonella and Shigella. For Campylobacter spp., stool samples were cultured on Skirrow agar and Campylobacter Blood-Free Selective Agar (CCDA) under microaerophilic conditions at 42°C for 48 hours. Raw chicken samples were enriched in Bolton broth prior to plating on CCDA to enhance recovery of Campylobacter spp.
Biochemical Tests
Presumptive colonies were further characterized using biochemical tests. Salmonella isolates were confirmed using triple sugar iron (TSI) agar, urease test, lysine iron agar (LIA), and indole production tests. Campylobacter spp. were identified based on their characteristic morphology, oxidase and catalase positivity, and inability to ferment carbohydrates.
Confirmatory Methods
While molecular techniques such as polymerase chain reaction (PCR) or serotyping were not utilized due to resource constraints, isolates were presumptively identified as Salmonella enteritidis based on biochemical profiles and agglutination tests using commercially available antisera.
The analysis included culture-based methods and biochemical testing to identify Salmonella spp. and other organisms. The testing procedures adhered to JFDA standards and were supplemented by further environmental assessments of food handling and storage practices.
While molecular techniques such as PCR are increasingly used for confirming pathogen identity with high sensitivity and specificity, they were not utilized in this investigation due to resource constraints and the reliance on existing laboratory infrastructure. Traditional culture-based methods remain the standard in many low- and middle-income settings, including Jordan, due to their cost-effectiveness and widespread availability. However, these methods may have limitations, particularly in cases where pathogens are present in low concentrations or are overgrown by competing background microbiota. To mitigate the risk of false negatives, the laboratories followed strict quality control measures, including the use of selective media and enrichment broths designed to enhance the recovery of target pathogens. Despite these precautions, the possibility of under-detection cannot be entirely ruled out, especially for transient or low-abundance contaminants.
Data Analysis
The surveillance data lacked control or unexposed groups for the comparative analysis. Therefore, only descriptive statistics including frequencies, percentages, means, and standard deviations were computed. Given the absence of a control group, we were unable to perform comparative analyses including calculating risk and relative probability.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of the MOH (IRB number: MOH/REC/2021/230−17,527). This study was conducted in accordance with the 1975 Declaration of Helsinki, revised in 2008, and its later ethical standards. The surveillance data used in this study were anonymous and information confidentiality was ensured.
Results
The MOH surveillance data included 472 foodborne illness cases that were interviewed by the rapid response teams. The mean age was 20.8 (SD±13.4) years (median: 17.0 years, range: 3–80 years). Overall, the majority of individuals (72.3%) were between 3 and 30 years of age, with age groups 3–10, 10–20, and 20–30 years accounting for 23.7%, 27.7%, and 20.9% of the total cases, respectively. No major gender differences were reported.
The epidemic curve (Figure 1) suggests that the outbreak began on July 27 and ended on August 1. Most cases first reported their symptoms on July 27 (n=46, 9.8%), July 28 (n=301, 63.8%), or July 29 (n=75, 15.8%). A few new cases were noted on subsequent days, indicating a single-source exposure.
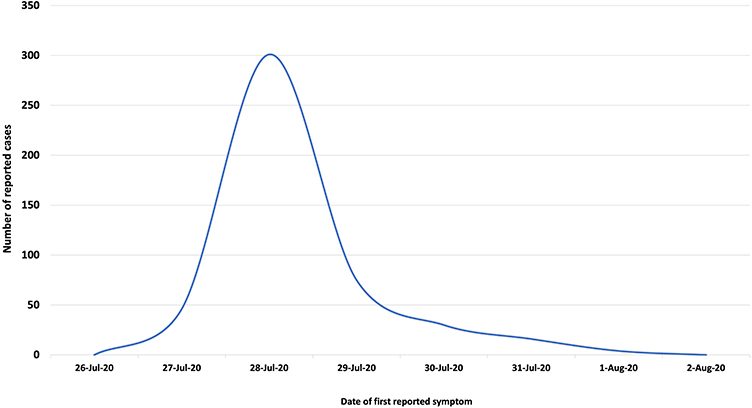 |
Figure 1 Epidemic Curve of the Chicken Shawarma-Associated Foodborne Outbreak, Ain Al-Basha, Jordan, July–August 2020. |
Symptom Profile
More than two-fifths of cases (42.1%) developed all five symptoms (diarrhea, vomiting, fever, headache, and abdominal pain). Four symptoms were experienced by 40.0% of cases, three by 16.7%, and two by 15.0% (Table 1). The most frequent symptoms were fever (98.3%), abdominal pain (96.8%) and vomiting (96.0%). Among the 472 total cases, seven required intensive care unit admission and two died (one aged three years and the other 40 years).
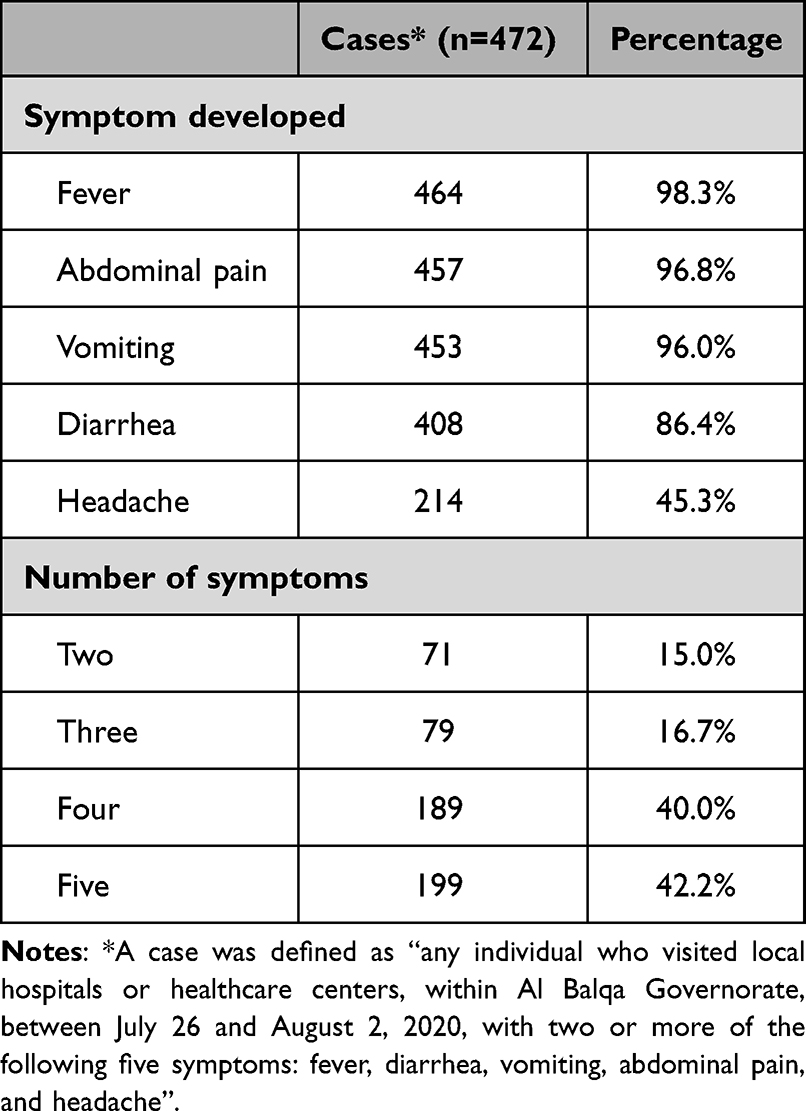 |
Table 1 Distribution of Cases by Symptom* |
Food Exposures
The majority (86.0%) of cases consumed chicken shawarma sandwiches. Similar consumption percentages were reported for garlic sauce (83.0%) and French fries (79.9%) (Table 2). Among those who had chicken shawarma (n=406), 1.0% (n=4) also reported eating broasted chicken, 92.6% (n=376) garlic sauce, 89.2% (n=362) French fries, 47.0% (n=191) pickles, 0.5% (n=2) zinger, and 40.1% (n=163) coleslaw. No other major exposure sources were identified.
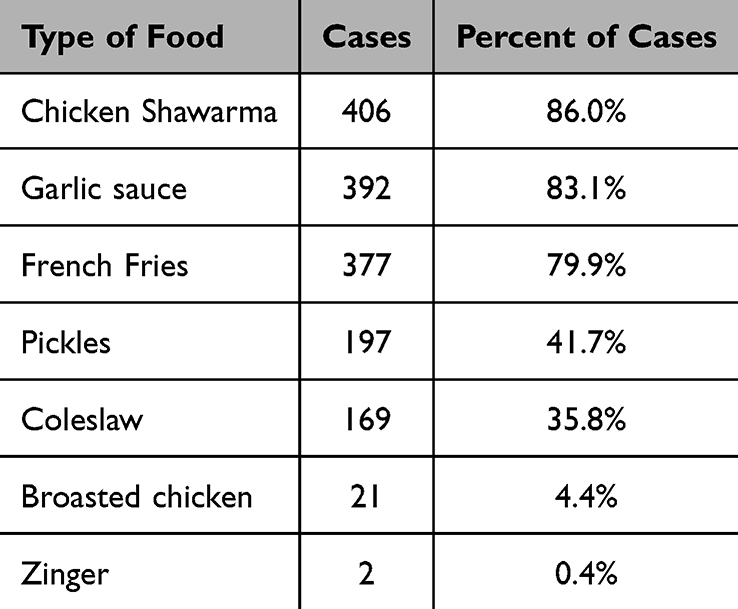 |
Table 2 Distribution of Cases by Food Items Consumed |
Laboratory Findings
Of the 472 total cases, stool specimens were collected from 56 individuals for laboratory analysis. All 56 (100%) tested positive for Salmonella enteritidis and 10 (17.9%) tested positive for Rotavirus, suggesting possible co-infection in these samples. All the food handlers tested negative for Shigella spp.
Water samples (tanks, tap water, and household sources) conformed to JS 286/1997 standards and were deemed fit for human consumption. Food samples tested by the JFDA revealed Enterococcus faecalis, indicating poor hygiene, and Campylobacter spp. in raw marinated chicken used for shawarma preparation. However, the JFDA report did not detail the specific tests run on each item, and only a summary of the results was provided to the MOH.
Discussion
Rapid demographic and dietary changes in developing countries have amplified the risk of foodborne hazards, often overwhelming the existing food safety systems.10 While these risks are believed to be high in EMR, limited scientific research on the specific pathogens involved persists.3 The resulting under-detection and under-reporting of outbreaks pose a critical public health challenge.11 In this study, we used Jordanian MOH surveillance data to describe an extensive foodborne outbreak in a major Jordanian city, where 472 symptomatic individuals sought care after consuming food from a single source. However, the true burden is likely to be higher given the possibility of underreporting (eg, individuals treated at home, private clinics, outside the geographic area investigated, or not seeking care). Epidemiological investigations strongly implicated chicken shawarma as the primary culprit, as the majority of cases reported its consumption.
Shawarma, a popular dish in Jordan, typically includes marinated and spit-roasted chicken wrapped in thin bread, along with French fries, garlic sauce, pickles, and coleslaw. Raw poultry is frequently contaminated with Campylobacter during slaughter and carcass processing.12 Environmental assessments in this study revealed cross-contamination and inadequate cooking methods for chickens, highlighting deficiencies in safe handling practices. The detection of Campylobacter spp. in raw chicken supports this conclusion, whereas the isolation of Salmonella enteritidis in ready-to-eat items suggests improper temperature control and “temperature abuse” during food storage or holding.
Still, the absence of Salmonella enteritidis in the food samples, despite its presence in stool specimens, can be explained by several factors, particularly given the delay in the investigation and the perishable nature of the food items. Accordingly, by the time food samples were collected, the specific batches of food responsible for the outbreak may no longer have been accessible, leading to a failure to detect Salmonella enteritidis in food. As well, contamination might have been localized to specific portions of the raw chicken or prepared shawarma and cross-contamination during food preparation could have affected only certain servings of the meal. Other reasons may also include time lag between exposure and outbreak investigation, inadequate sampling, environmental degradation of the pathogens, or the longer survival dynamics of the pathogen in stool compared to food. Regardless, our results underscore the importance of rapid outbreak investigations and comprehensive sampling strategies to identify the source of contamination effectively.
Possible Risk Factors
Notably, the JFDA regulations published in 2017 do not explicitly require the absence of Campylobacter in raw or marinated chicken products, although tracing back to chicken suppliers was part of the investigation. Matching clinical isolates with food isolates proved unfeasible, likely because of uneven pathogen distribution, inadequate sampling, or inherent challenges in detecting transient contamination. Despite these limitations, our findings suggest the presence of multiple risk factors. These include the consumption of garlic sauce, French fries, and occasionally pickles or coleslaw, although their smaller share in meals suggests that they were less central than shawarma itself. The isolation of Enterococcus faecalis from food samples further indicated inadequate hygiene practices.
Compounding these risks, the rapid reopening of restaurants after Jordan’s COVID-19 lockdown and low-cost shawarma deals may have created a high volume catering environment with limited staff. Such conditions can lead to improper food handling, reflecting the crucial role of food handlers in transmitting infections.11 Hence, the JFDA, along with food sector unions, must strengthen its oversight and training to maintain rigorous standards at every point of sale. Strengthening training programs for food handlers on proper hygiene and food safety practices is essential to mitigate such risks.
Public Health Implications
Bacteria such as Salmonella spp., E. coli, Bacillus cereus, and Campylobacter spp. pose ongoing challenges to food safety.13 Campylobacter in poultry remains a major concern because widely consumed poultry products are powerful vehicles for infection.14 Although campylobacteriosis is not often cited as a leading cause of foodborne diseases in the region,11 this underreporting might be attributable to suboptimal surveillance systems. Our data highlights the overlap between these pathogens. Nevertheless, the variety of isolated pathogens underscores the need for a comprehensive hazard analysis.
In Jordan, multiple agencies have coordinated food safety. The JFDA was established in 2008 as the national authority, while the MOH led outbreak investigations and collaborated with the JFDA to regulate and inspect implicated establishments. This partnership helped identify sources of contamination in the current outbreak, reinforcing the value of an integrated approach. However, some EMR countries lack a single robust agency, diffusing responsibilities among different ministries and complicating surveillance. Exclusive food safety authorities in such settings could unify farm-to-fork strategies, bolster outbreak detection, and promote evidence-based decision making.
Population at Risk
Our results indicate that the most affected individuals were under 30 years of age, including many children. Additionally, seven admissions to the intensive care unit and two deaths reflected a disproportionate burden on children and vulnerable populations (eg, the elderly, pregnant women, or immunocompromised individuals). These groups face heightened risk of severe complications, underscoring the moral and regulatory obligations of food services to ensure stringent safety protocols. National food safety systems should prioritize identifying at-risk groups and communicating the importance of safe diets and hygienic preparation methods.15 Risk communication via mass media may help both the public and policymakers to respond more effectively when hazards emerge.
Study Limitations
Although this study combined epidemiological and laboratory components to identify the drivers of this outbreak, it has several limitations. First, the reliance on secondary data from the rapid response teams restricted our ability to analyze potential exposures in an analytic manner, as no control or unexposed groups were included. The absence of a control group limits our ability to calculate relative risks and draw definitive conclusions about the association between specific food items and illness. Future studies should incorporate control groups to strengthen the epidemiological rigor of outbreak investigations. Second, the timing and uneven distribution of pathogens may have precluded the finding of a direct match between clinical and food isolates. Third, the narrow geographic focus could exclude cases that sought care in neighboring governorates, further contributing to the underestimation of the extent of the outbreak. Finally, food-specific microbiological testing data were not available as this was under the control of the JFDA, and reliance on critical decisions was based on narratives provided to the MOH. Future food-borne investigations should ensure compliance with epidemiological standards for all datasets and support access to data to facilitate reporting of the burden of foodborne diseases.
Conclusion
This outbreak, tied to chicken shawarma in Jordan, highlighted systemic lapses in food safety, resulting in severe illnesses and tragic fatalities. Reopening restaurants post-COVID-19, combined with inadequate food handling, created conditions that rapidly escalated contamination and disease transmission. Our findings highlight the pressing need for stronger regulations, regular inspections, and targeted education of food handlers. Protecting children and immunocompromised groups from similar incidents is a national priority. Ultimately, guaranteeing safe and hygienic food extends beyond mere regulation. It is a core public health responsibility that demands collective action from regulatory authorities and industry stakeholders to the consuming public.
Data Sharing Statement
The datasets generated during this study are available from the corresponding author (e-mail: [email protected]). The data will be provided with proper approval from the Jordan Ministry of Health, upon reasonable request.
Ethics Approval
All procedures performed in this study involving human participants were reviewed and ethically approved by the Institutional Review Board (IRB) at the Jordan Ministry of Health (IRB number: MOH/REC/2021/230−17527). This study was conducted following the 1975 helsinki declaration, revised in 2008, and its later amendments or comparable ethical standards.
Consent to Participate
Written informed consent was obtained from all the participants included in the study. A parent, or legal guardian, of patients under 18 years of age provided informed consent.
Acknowledgments
The authors thank the outbreak rapid response teams at the Ministry of Health (MOH) and Jordan Food and Drug Administration (JFDA) for their dedication and prompt responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any grants from funding agencies in the public, commercial, or not-for-profit sector.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Foodborne disease outbreaks: guidelines for investigation and control. World Health Organization; 2008.
2. Pires SM, Desta BN, Mughini-Gras L, et al. Burden of foodborne diseases: think global, act local. Curr Opin Food Sci. 2021;39:152–159. doi:10.1016/j.cofs.2021.01.006
3. Todd ECD. Foodborne disease in the middle east. In: Murad S, Baydoun E, Daghir N, editors. Water, Energy & Food Sustainability in the Middle East. Cham: Springer; 2017. doi:10.1007/978-3-319-48920-9_17
4. World Health Organization. WHO estimates of the global burden of foodborne diseases: executive summary. World Health Organization; 2015.
5. Havelaar AH, Kirk MD, Torgerson PR, et al. World Health Organization global estimates and regional comparisons of the burden of foodborne disease in 2010. PLoS Med. 2015;12(12):e1001923. doi:10.1371/journal.pmed.1001923
6. Faour-Klingbeil D, Todd ECD. Prevention and control of foodborne diseases in Middle-East North African countries: review of national control systems. Int J Environ Res Public Health. 2020;17(1):70. doi:10.3390/ijerph17010070
7. FAO. Near East and North Africa – regional overview of food security and nutrition 2021: statistics and trends. Cairo; 2021. Available from: https://doi.org/10.4060/cb7495en.
8. Gargouri N, Walke H, Belbeisi A, et al. Estimated burden of human Salmonella, Shigella, and Brucella infections in Jordan, 2003–2004. Foodborne Pathogens Dis. 2009;6(4):481–486. doi:10.1089/fpd.2008.0192
9. Malaeb M, Bizri AR, Ghosn N, Berry A, Musharrafieh U. Salmonella burden in Lebanon. Epidemiol Infect. 2016;144(8):1761–1769. doi:10.1017/S0950268815003076
10. World Bank. Food-Borne Illnesses Cost US $110 Billion per year in Low-and Middle-Income Countries. WorldBank Washington, DC, USA; 2018.
11. Greig JD, Todd EC, Bartleson CA, Michaels BS. Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 1. Description of the problem, methods, and agents involved. Journal of Food Protection. 2007;70(7):1752–1761. doi:10.4315/0362-028X-70.7.1752
12. Wieczorek K, Denis E, Osek J. Comparative analysis of antimicrobial resistance and genetic diversity of Campylobacter from broilers slaughtered in Poland. Int J Food Microbiol. 2015;210:24–32. doi:10.1016/j.ijfoodmicro.2015.06.006
13. Sagoo SK, Little CL, Greenwood M, et al. Assessment of the microbiological safety of dried spices and herbs from production and retail premises in the United Kingdom. Food Microbiol. 2009;26(1):39–43. doi:10.1016/j.fm.2008.07.005
14. Wensley A, Coole L. Cohort study of a dual-pathogen point source outbreak associated with the consumption of chicken liver pâté, UK, October 2009. J Public Health. 2013;35(4):585–589. doi:10.1093/pubmed/fdt020
15. World Health Organization. WHO global strategy for food safety 2022–2030: towards stronger food safety systems and global cooperation. World Health Organization; 2022.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.