Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Shared Decision-Making Facilitates Inhaler Choice in Patients with Newly-Diagnosed Chronic Obstructive Pulmonary Disease: A Multicenter Prospective Study
Authors Hsiao YH ![]() , Tseng CM, Sheu CC
, Tseng CM, Sheu CC ![]() , Wang HY, Ko HK, Su KC, Tao CW, Tsai MJ
, Wang HY, Ko HK, Su KC, Tao CW, Tsai MJ ![]() , Chen YF
, Chen YF
Received 11 June 2022
Accepted for publication 22 August 2022
Published 2 September 2022 Volume 2022:17 Pages 2067—2078
DOI https://doi.org/10.2147/COPD.S376547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yi-Han Hsiao,1– 3 Ching-Min Tseng,2,4 Chau-Chyun Sheu,5,6 Hsin-Yi Wang,7,8 Hsin-Kuo Ko,2,9 Kang-Cheng Su,2,10 Chi-Wei Tao,4 Ming-Ju Tsai,5,6,* Yen-Fu Chen7,8,*
1Division of General Chest Medicine, Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 2School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 3Department and Institute of Physiology, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 4Division of Chest Medicine, Department of Internal Medicine, Cheng-Hsin General Hospital, Taipei, Taiwan; 5Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan; 6Department of Internal Medicine, School of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; 7Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, National Taiwan University Hospital Yunlin Branch, Yunlin, Taiwan; 8Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; 9Division of Respiratory Therapy, Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 10Division of Clinical Respiratory Physiology, Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Ming-Ju Tsai, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Kaohsiung Medical University Hospital, No. 100, Tz-You 1st Road, 807, Kaohsiung, Taiwan, Tel +886 7 3121101, Ext. 5651, Fax +886 7 3161210, Email [email protected] Yen-Fu Chen, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, National Taiwan University Hospital Yunlin Branch, Yunlin, Taiwan, Tel +886 5 5323911, Ext. 2501, Email [email protected]
Purpose: Inadequate inhaler technique and nonadherence to therapy are associated with poorer clinical outcomes in chronic obstructive pulmonary disease (COPD). Shared decision-making (SDM), based on clinical evidence, patient goals and preferences, improves quality of care. This study aims to investigate the initial patients’ choices of inhaler devices in patients with newly-diagnosed COPD after an SDM process.
Patients and Methods: We conducted a prospective, observational, multi-center study in four hospitals in Taiwan from December 2019 to July 2021. All treatment-naïve patients with newly-diagnosed COPD who were able to use three different inhalers of dual bronchodilators (Respimat®, Ellipta®, and Breezhaler®) in the outpatient setting were enrolled. After an SDM process, every patient was prescribed with one inhaler chosen by him- or herself. Errors of using inhalers were recorded after prescription of the inhaler, and at the follow-up visit a month later. The patients’ adherence, satisfaction score, and willingness to keep the initially chosen inhaler were investigated.
Results: In 109 enrolled patients, 43, 45, and 21 patients chose Respimat®, Ellipta®, and Breezhaler®, respectively. Patients chose different inhalers had similar rates of critical error on both visits, while the rates greatly decrease on the follow-up visit, no matter which inhaler devices they chose initially. The majority of patients had good adherence (use as the prescription daily, n = 79, 82%), satisfaction (satisfaction score ≥ 4, n = 70, 73%), and strong willingness to keep the initial inhaler (n = 89, 93%) on the follow-up visit regardless of disease severity and their comorbidities.
Conclusion: SDM might facilitate inhaler choosing, reduce inhaler errors (versus baseline) with good adherence, satisfaction and strong willingness to keep the initial inhaler in patients with newly-diagnosed COPD.
Keywords: shared decision-making, inhaler choice, dual bronchodilators, chronic obstructive pulmonary disease
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and airflow limitation due to chronic airway inflammation and remodeling.1,2 Inhaled therapy is the fundamental treatment for COPD patients,1 which provides rapid onset of action and good efficacy in the airways with limited systemic adverse effects.3,4 In addition to the advances in pharmacological compounds, multiple inhaler devices with different handling techniques have been developed.4,5 However, poor inhaler technique and nonadherence of patients may bring great challenges in managing COPD with these devices.6–10
The updated report by Global Initiative for Obstructive Lung Disease (GOLD) highlights the importance to select optimal inhaler based on patient needs, to reassess handling techniques regularly, and to ensure patients’ adherence to the inhaled therapy.1 Many studies have investigated patients’ preferences of different inhalers,11–15 but the decision of selecting inhaler is usually made by the physicians, rather than patients themselves. This unilateral decision process raises the concerns of suboptimal satisfaction and nonadherence of the patients, especially in those who are newly diagnosed and have no experience in using inhalers.
Emerging evidence has demonstrated that a shared-care approach which emphasizes on patients’ goals, preferences, and comprehensive education improves outcomes.12,16,17 This “shared decision-making (SDM)” concept focuses on developing tools, which introduce choices and help patients explore their preferences based on treatment goals, to support patient involvement in deciding optimal treatment.18,19 Nevertheless, whether SDM could facilitate inhaler choice and determine clinical outcomes in patients with newly-diagnosed COPD remains unclear.
This multi-center prospective study aims to investigate the initial choices and handling errors from three inhaler devices (Respimat®, Ellipta®, and Breezhaler®) in patients with newly-diagnosed COPD after a SDM process. The inhaler errors, satisfaction to the device, and willingness to keep using the initial device after one-month are also evaluated.
Materials and Methods
Study Population
This prospective, observational study was conducted in four major hospitals in Taiwan from December 2019 to July 2021. We identified newly-diagnosed COPD patients in the outpatient setting according to the GOLD report1 and were considered eligible to receive a long-acting β2 agonists (LABA) and long-acting muscarinic antagonists (LAMA) fixed-dose combination (FDC) by the pulmonologists. The patients with no experience on any of study inhalers, including Respimat® Soft Mist™ Inhaler (Respimat®; Boehringer Ingelheim, Germany), ELLIPTA® dry powder inhaler (DPI) (Ellipta®; GlaxoSmithKline, Brentford, UK; ELLIPTA® is a trademark of the GSK group of companies), and Breezhaler® DPI (Breezhaler®; Norvatis, Basel, Switzerland) were carefully evaluated by both pulmonologists and certified COPD educators to confirm their capability on communication and ability to operate these devices before enrollment. Patients meeting any of the following criteria were excluded: current diagnosis of asthma without COPD; those obviously unable to use any study inhaler as determined by the pulmonologists (for example, inability to twist Respimat® due to weakness [and no family could help], status post reconstructive oral or maxillofacial surgery causing inability to seal the lips on Ellipta®, inability to insert a capsule into the compartment of Breezhaler® due to hand tremors); patients disagreed to participate; difficulty in communication or conscious disturbance.
Shared Decision-Making (SDM) Process
Before enrollment of patients, all pulmonologists and certified COPD educators in four hospitals were invited to a consensus meeting, and a standardized SDM protocol was established (Figure S1 in the Supplementary Data). All patients received the protocolized approach from the pulmonologists and educators, who provided a comprehensive education after understanding patients’ goals. In brief, an educator introduced three inhalers with a SDM leaflet (See “Patient Information” in the Supplementary Data) and demonstrated the steps of using them with placebo devices. The order of introducing and demonstrating to each patient was randomized according to a random number table. After being fully understood, the patients chose one inhaler by their preference and the reasons of choosing that device were recorded (see “Educator’s checklist” in the Supplementary Data). The pulmonologists then prescribed one of the LABA/LAMA FDCs, including olodaterol/tiotropium bromide (Spiolto® Respimat®), vilanterol trifenatate/umeclidinium bromide (Anoro® Ellipta®), and indacaterol maleate/glycopyrronium (Ultibro® Breezhaler®), according to the patient’s choice. The educators demonstrated that inhaler again to the patients. After these two times of demonstration, the patients were asked to demonstrate how to use the inhaler independently. The visit 1 would be ended if the patients operate the inhaler completely correctly. If any error was observed by the educators, the patients would be re-educated until they could use the inhaler without any error. The times of error(s) that required re-education in each step of the inhaler were recorded before the end of visit 1. One month later, the patients were arranged to follow up (visit 2) and were asked to operate the inhaler independently again. If the patients operate the inhaler correctly, they were asked to complete a questionnaire regarding the adherence, satisfaction score and willingness to keep the initial inhaler before meeting the physicians. If any error was observed by the educators, the patients would be re-educated again until they could use the inhaler without any error. The times of error(s) that required re-education in each step of the inhaler were recorded as well.
Data Collection and Outcome Measurements
Baseline demographic variables, including sex, age, education level, smoking history, comorbidities, spirometry parameters, exacerbation history in the past year, COPD assessment test (CAT) score, and modified medical research council (mMRC) dyspnea scale were collected. All patients were arranged to follow up a month later (visit 2), and the CAT score, mMRC dyspnea scale, adherence, satisfaction score, willingness to keep the initial inhaler were assessed. The times of error(s) that required re-education in each step of the inhaler were recorded and summarized at both visits.
At visit 2, adherence was evaluated by a patient-reported questionnaire from good (use as the prescription daily), fair (use in 5–6 days per week), to poor (use ≤4 days per week). The patients were also asked to answer a five-point scale satisfaction score which ranged from (1) very unsatisfied, (2) unsatisfied, (3) fair, (4) satisfied, to (5) very satisfied. A satisfaction score ≥4 was considered that the patient had good satisfaction to the device from the SDM process.
The numbers of critical errors, which were defined as any action critically affecting the lung deposition of inhaled drug including critical preparation errors and critical delivery errors, were also calculated.8 The critical preparation errors included the following: did not twist the base one half-turn (Respimat®), did not open the device correctly, did not place capsule in the chamber (Breezhaler®), did not close the mouthpiece (Breezhaler®), or did not press button to pierce the capsule (Breezhaler®). The critical delivery errors included the following: did not seal lips around mouthpiece during inhalation, synchronize actuation and inhalation (Respimat®), inhale slowly (Respimat®)/forcefully (Ellipta®)/quickly (Breezhaler®) and deeply, hold breath after inhalation, or did not remove capsule and check for powder residue (Breezhaler®).
The primary outcome of this study was the times of error(s) that required re-education in each step of the inhaler. The secondary outcomes included the adherence, satisfaction score and willingness to keep the initial inhaler at the end of the study.
Statistical Analysis
The categorical and continuous variables were presented using frequencies with percentages and median with interquartile ranges (IQR), respectively. Variables were compared between groups using Fisher’s exact test (for categorical variables) or Kruskal–Wallis test (for continuous variables). Variables were compared between two visits with Wilcoxon signed-rank test. The effects of various factors on a specific outcome variable were assessed with Logistic regression analyses. All variables in the univariate analysis were included in the multivariable Logistic regression models, and odds ratios (ORs) or adjusted ORs (aORs) with 95% confidence intervals (95% CI) were calculated. Statistical significance was set at a two-tailed p value of less than 0.05. All analyses were performed using SAS system (version 9.4 for Windows, SAS Institute Inc., Cary, NC).
Results
Baseline Characteristics and the Choices of Devices
A total of 109 treatment-naïve patients with newly-diagnosed COPD and good ability to use all three inhalers were enrolled (Figure 1). Through an SDM approach, 43 (39%) patients chose Respimat®, 45 (41%) patients chose Ellipta®, and 21 (19%) chose Breezhaler® initially. A total of 96 patients completed visit 2 after 1-month treatment, and the numbers (%) of patients who want to keep their initial inhaler were 35 (81%), 38 (84%), and 17 (81%) for those choosing Respimat®, Ellipta®, and Breezhaler® at visit 1, respectively. Six patients decided to change their inhaler on visit 2, including one from Respimat® to Ellipta®, two from Breezhaler® to Ellipta®, and three from Ellipta® to Respimat®.
 |
Figure 1 (A) Flowchart showing the enrollment of patients. (B) Bullseye plot showing the numbers of patients choosing different inhalers on the visit 1 (inner circle) and the decision of keeping or changing inhalers on the visit 2 (outer circle). |
Table 1 shows the demographic and certain baseline characteristics of patients who completed two visits (n = 96). The median (IQR) age was 67 (61.5–72) years; 90 (94%) patients were male; 45 (47%) patients had an education level of senior high school or higher; 90 (94%) patients were ever smoker; 86 (90%) patients had at least one comorbidity. Most patients had mild (GOLD grade 1, n = 29, 30%,) or moderate (GOLD grade 2, n = 53, 55%) airflow limitation. The patients had a median (IQR) CAT score of 7 (4–11) and mMRC dyspnea scale of 2 (1–2); 87 (91%) patients had no acute exacerbation in the past year. Most patients were in GOLD group A (n = 30, 31%) and GOLD group B (n = 63, 66%). There were no significant differences in these baseline characteristics, lung function, symptom scores, exacerbation history, or GOLD group between groups (Table 1 and Table S1 in the Supplementary Data). After 1-month of treatment, there were significant improvements in CAT score (Figure S2A–C in the Supplementary Data) and mMRC dyspnea scale (Figure S3A–C in the Supplementary Data) compared with those at the initial visit. The improvement of symptoms showed no significant difference between groups (Figures S2D and S3D in the Supplementary Data).
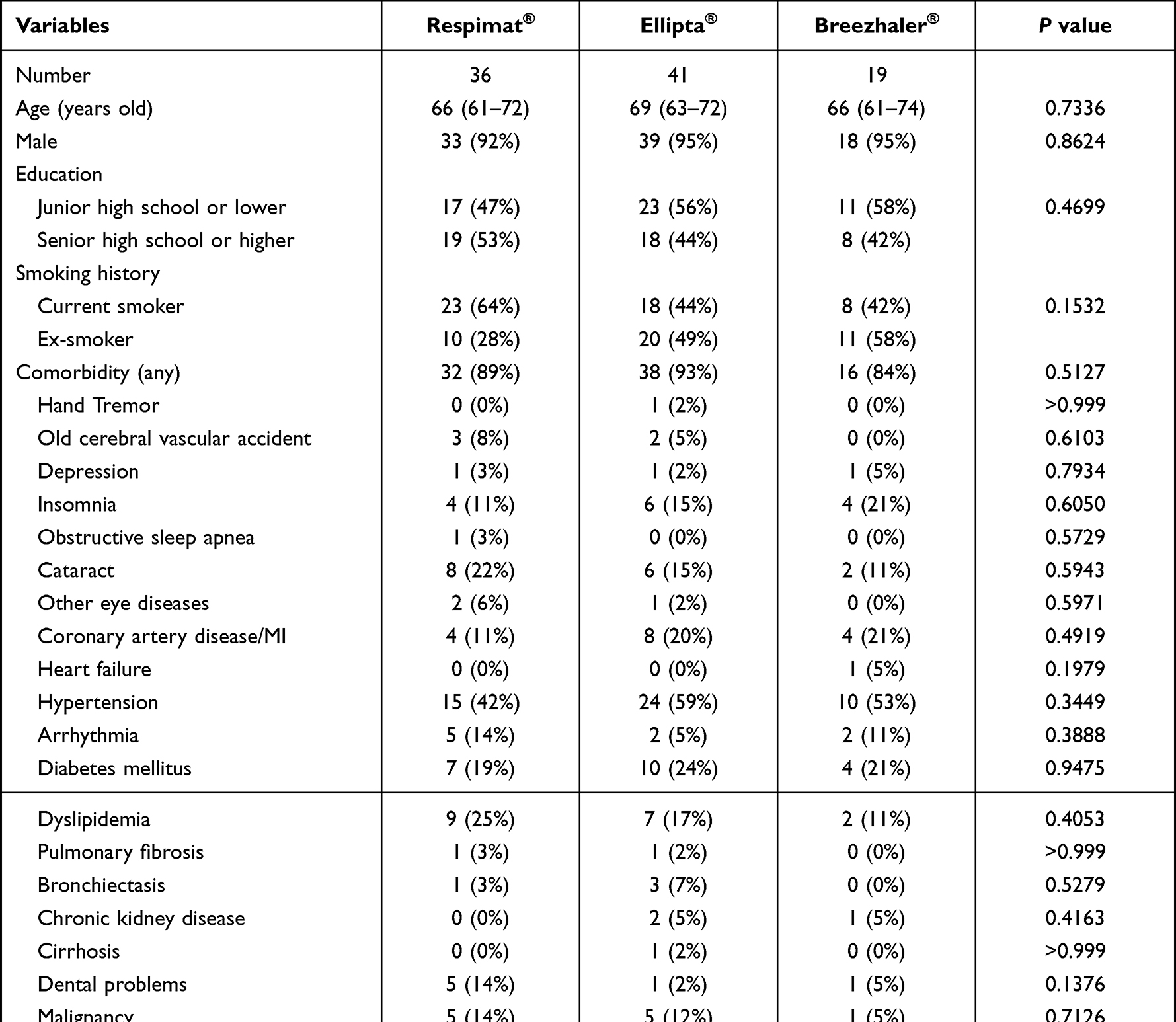 |
Table 1 Baseline Characteristics of Patients Completed Two Visits |
The order of demonstration showed no significant difference between groups (Tables S2 and S3 in the Supplementary data) because of the randomized design. In regard to the reasons of choosing the inhaler, more patients chose Breezhaler® because of the visibility of inhaled medication and the device appeared delicate and textured; more patients chose Ellipta® because of simple using. Six patients chose Respimat® because of worrying about potential choking sensation or cough induced by dry powders; two patients chose Respimat® because of feeling easy to inhale the soft mist while the others appeared requiring more force to inhale.
Errors in Using the Inhalers
The primary outcome of the study, which was the times of error(s) that required re-education in each step of the inhaler, and the numbers of patients with any error(s) are shown in Table 2, as well as Table S4 and Figure S4 in the Supplementary Data. The detailed errors by steps in three inhalers based on patients’ initial choices are shown in Tables S5–S7 in the Supplementary Data. Although the Respimat® group appeared having more errors in terms of the number of patients with any error(s) and the error times per step (Table 2; Table S4 and Figure S4A–E in the Supplementary Data), the numbers of patients with critical error, either in preparation or delivery aspect, showed no difference between groups in both visits. The educators re-educated the patients until they can use the inhaler with zero error before the end of visit 1. No inhaler device education was given to the patients between two visits. When the patients came back to the clinic a month later (visit 2), the numbers of errors at visit 2 were found not zero, and therefore re-education was needed. However, the errors at visit 2 were significantly decreased compared to those at visit 1, in terms of decreased number of patients with any error (visit 1 vs visit 2: 76% vs 38%, p < 0.0001) or any critical error (72% vs 29%, p < 0.0001) and the median error times per step (0.3 vs 0.0, p<0.0001) (Table S8 and Figure S4A–C in the Supplementary Data). The improvement between two visits showed no difference in three groups (Table 2 and Figure S4F in the Supplementary Data).
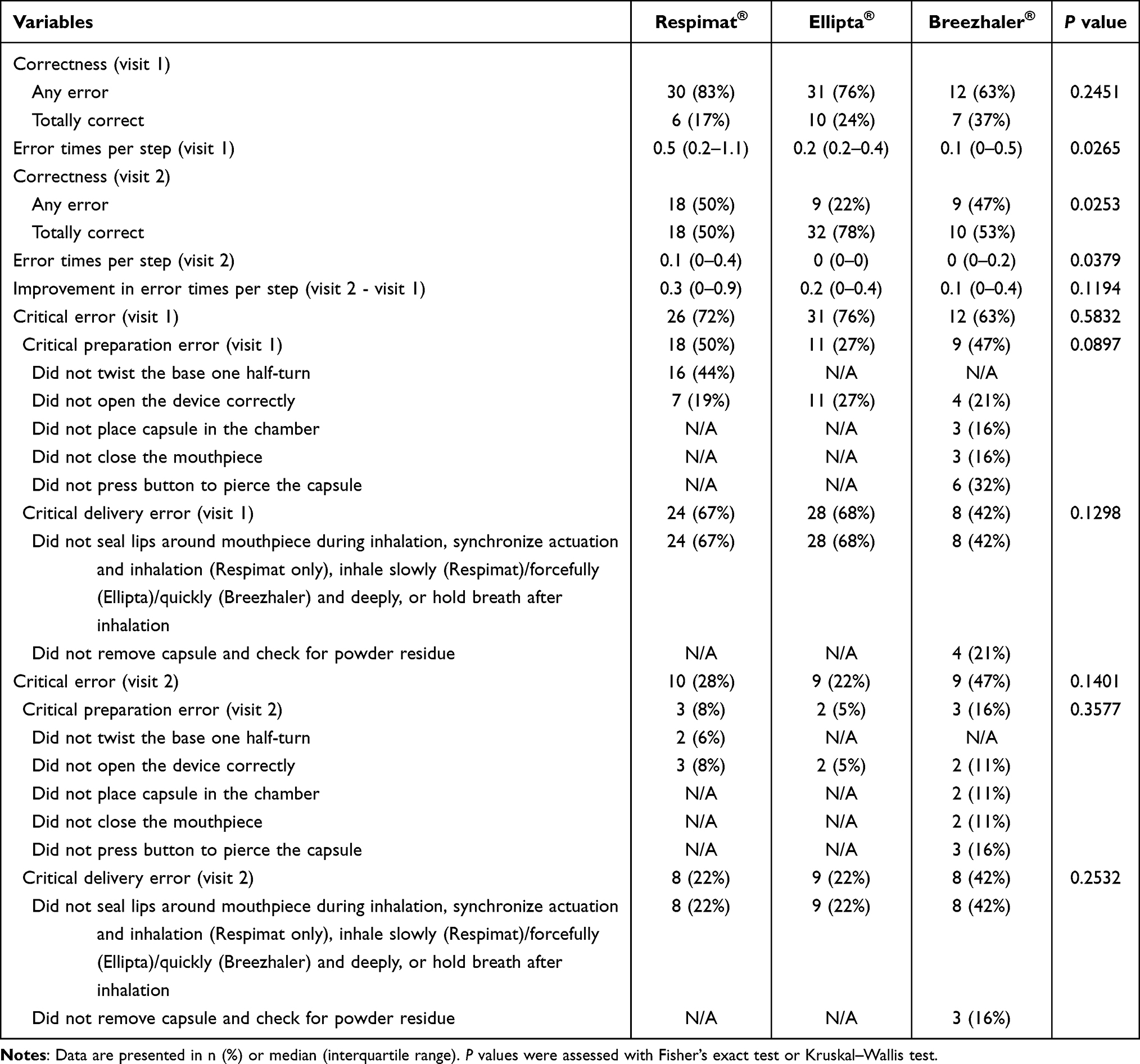 |
Table 2 Number of Patients with Error(s) and Times of Error(s) That Required Re-Education in Patients Completed Two Visits |
Logistic regression analyses found none of the variables assessed, including initial inhaler choice, age, sex, education level, smoking history, comorbidity, severities of airflow limitation, acute exacerbation history and CAT score, as a risk factor for any critical error on both visits (Tables S9 and S10 in the Supplementary data).
Adherence, Satisfaction Score and Willingness Scale to Keep Initial Inhaler
In regard to the secondary outcomes of the study, the majority of patients had good adherence (use as the prescription daily, n = 79, 82%), satisfaction (satisfaction score ≥4, n = 70, 73%), and strong willingness to keep the initial inhaler (n = 89, 93%) on visit 2 (Table 3). There were no differences in adherence, satisfaction score, and willingness scale to keep the initial inhaler between groups.
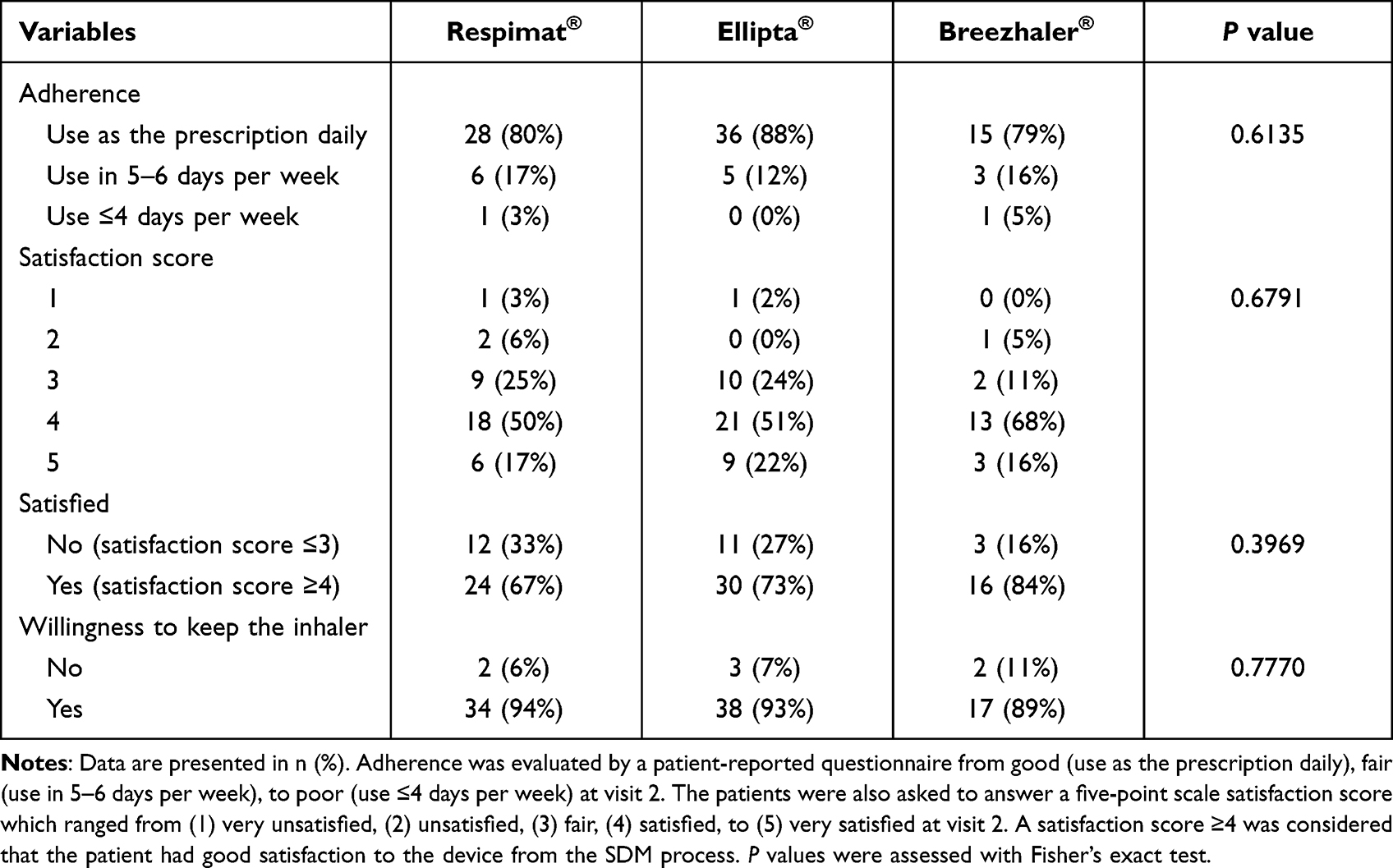 |
Table 3 Adherence, Satisfaction Score, and Willingness to Keep the Inhaler |
Logistic regression analyses were used to identify any factors associated with satisfaction (satisfaction score ≥4), willingness to continue use of the initial inhaler, and significant symptom improvement (CAT score ≥2) (Table 4). Multivariable logistic regression analyses showed that presence of comorbidity (aOR [95% CI]: 6.2 [1.1–33.7]) and acute exacerbation in the previous year (aOR [95% CI]: 16.5 [1.4–200.1]) were associated with higher satisfaction, while severe airflow limitation (GOLD grade 3 and 4, aOR [95% CI]: 0.2 [0.0–0.8]) and symptom burden (CAT score ≥10, aOR [95% CI]: 0.3 [0.1–0.8]) were associated with lower satisfaction. No independent predicting factor was identified in association with the willingness to continue use of the initial inhaler. In regard to symptom improvement, being more symptomatic (CAT score ≥10) at baseline was associated with a significant improvement (CAT score decrease ≥2) after 1-month of LABA/LAMA FDC treatment (aOR [95% CI]: 7.0 [2.4–20.6]).
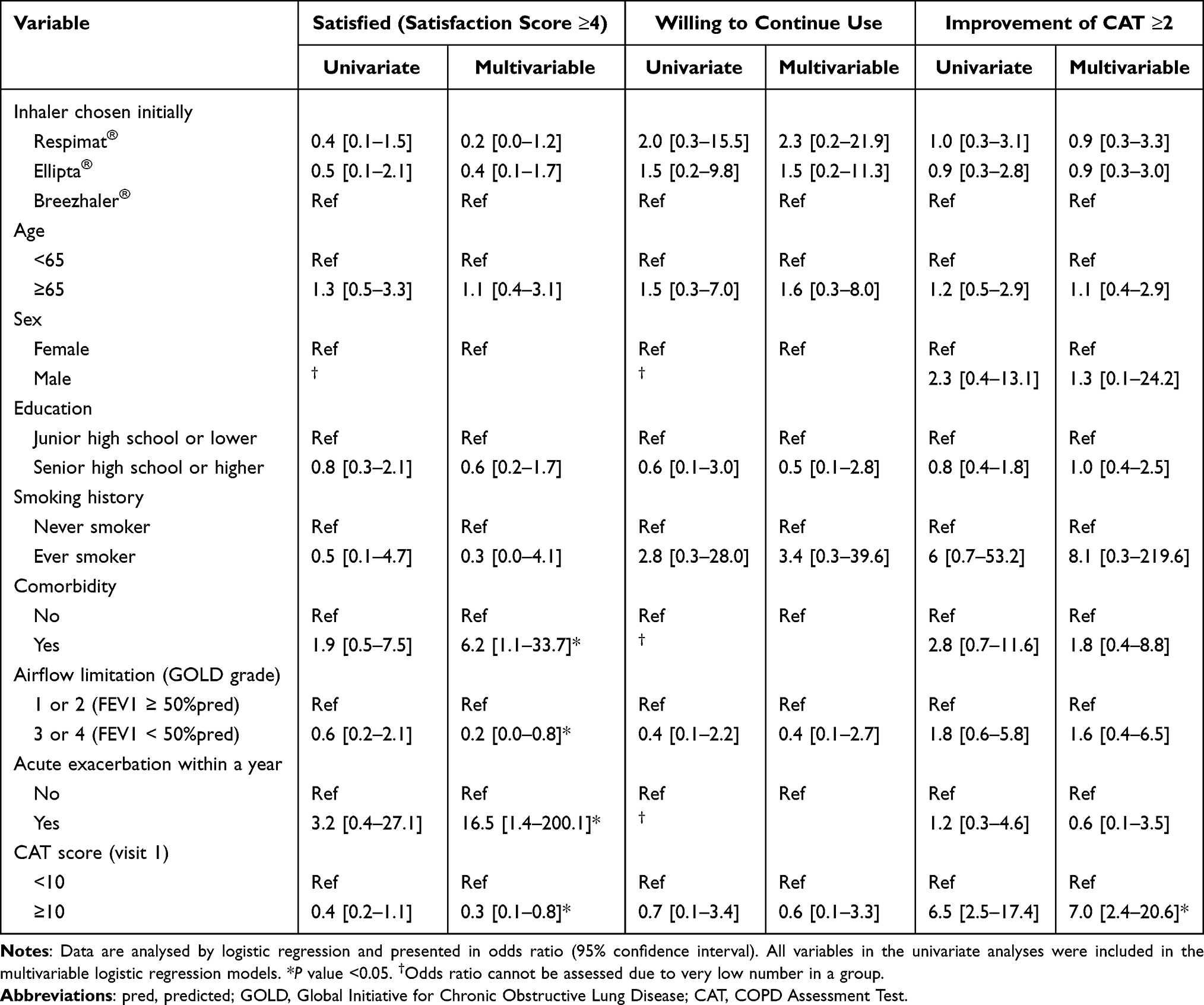 |
Table 4 Factors Associated with Satisfaction, Willingness to Continue Use, and Symptom Improvement in Patients Completed Two Visits |
Discussion
In this multi-center, prospective study, we investigated the patients’ choices of inhaler device after an SDM process in newly-diagnosed COPD patients, showing Ellipta® and Respimat® were more popular than Breezhaler®. The symptoms significantly improved after 1-month treatment with LABA/LAMA FDCs. The inhaler errors markedly reduced at the end of study compared with baseline and the critical errors showed no differences between three devices. Most patients reported great adherence, satisfaction, and strong willingness to keep using the inhalers, which all demonstrated no difference between three devices.
Previous study investigating over 7000 patients worldwide showed that dry power inhalers (DPIs) were the mostly prescribed inhaler, and ease of use was the key factor from both patients’ and physicians’ perspective in selecting inhalers for COPD.20 The results supported our study showing a majority (41%) of patients chose Ellipta® because of the simplicity of operating the inhaler. Interestingly, our study demonstrated a similar percentage (39%) of patients chose Respimat® through SDM, and the reasons unmasked concerns of patients, worrying about potential choking sensation or cough induced by dry powders, and their favors in soft-mist spray to reduce inhalation difficulty. The results may suggest that SDM could be helpful in discovering the unmet needs in choosing optimal devices for COPD patients compared with the traditional unilateral decision process by the physicians.
It is well known that inhaler errors were associated with poor clinical outcomes and non-adherence in COPD.7,9,10,21 However, more than half of COPD patients were reported to have handling errors regardless of the device used,7 and the misuse rates were even higher (65–88%) in elderly patients with COPD in Taiwan.6 It seems reasonable to change device once the current inhaler seemed ineffective, but studies showed that using different inhaler devices may damage patient’s adherence.22,23 In our study, patients who chose Respimat® had more errors compared with other two devices, but no difference in critical errors. Given the patient’s preference of Respimat® shown in this study and clinical benefit of olodaterol/tiotropium bromide,24 we should think more about reducing errors and enhancing adherence of patients rather than switching to other devices. Through the SDM process, our patients achieved less inhaler errors versus baseline with good adherence, high satisfaction level, and a high proportion of patients willing to keep on their initially chosen inhaler device. Hand-on education, ie, asking the patients to operate the inhaler independently followed by re-education, instead of mere demonstration by educators, might greatly improve the learning outcomes with reduced inhaler errors. As shown in Table S8, a majority of patients (76%) had at least one inhaler error at visit 1 after two times of demonstration by educators. Operating the inhaler by patients themselves helped discover the errors that required re-education, and all errors were corrected before the end of the visit. A significantly less proportion (38%) of patients had at least one inhaler error at visit 2. Our findings were supported by several studies revealed greater efficient learning by repeated education about the instruction of inhaler use accompanied with demonstration by patients themselves, rather than video demonstration or leaflets.22,25,26 In addition, our well-established SDM protocol provided sufficient information to improve the patients’ knowledge and motivation, supporting them to choose the optimal inhaler device in their minds, resulting in good adherence and satisfaction. In a study enrolled patients with COPD receiving dual bronchodilator treatment as the initial therapy, the proportion of adherent patients (proportion of days covered ≥0.8) was 22.0%.27 The results suggested that only 22% of patients used filled prescriptions in more than 80% of study period. Our study showed that up to 82% of patients used their LABA/LAMA FDCs in every single day during the study period. Taken together, the results of significant reduction in inhaler errors versus baseline as well as good adherence at the end of study supported the benefits of SDM in facing this challenge in COPD management.
Most patients in our study reported good satisfaction, and several predicting factors were identified, including presence of comorbidity, positive exacerbation history, less severe airflow limitation, and less symptom burden. A study from Miravitlles et al showed that the satisfaction scores were similar in different age, smoking status and time since diagnosis of COPD either in patients using Respimat® or Breezhaler®.28 Another study showed patients with severe COPD tended to have higher satisfaction than those with mild/moderate disease during 4-week observation irrespective of different DPIs used.29 Since satisfaction is a subjective feeling, diverse results may be presented in different groups of patients.
In regard to the symptom improvement, the medium (IQR) improvement of CAT score after 1-month dual bronchodilator treatment was 2.0 (0.5–5.0) and there was no significant difference between three inhaler groups (p = 0.6877) (Figure S2 in the Supplementary Data). A previous study investigating the efficacy of once-daily dual bronchodilator treatment in symptomatic COPD patients showed the mean CAT score reduction after four weeks treatment was 1.60 in umeclidinium/vilanterol and 1.01 in tiotropium/olodaterol, respectively.30 Because of the study populations were different and symptom improvement was not the primary outcome in both studies, it is difficult to infer that SDM contributed to improved symptom control. However, greater symptom improvement was observed in patients with higher baseline CAT score in our study. This result is consistent with a previous study, which showed patients with higher baseline CAT scores had greater improvement in the St. George’s Respiratory Questionnaire score, rescue medication use, and exacerbation rate after 24-week LABA/LAMA FDCs treatment.31
In our study, 30 patients (31%) were in GOLD group A and received LABA/LAMA FDCs. The majority of them had a moderate to severe airflow limitation in the baseline spirometry, which might contribute to the physicians’ decision of choosing LABA/LAMA FDCs. In recent systematic reviews and meta-analyses enrolling COPD patients with a baseline FEV1 of less than 80% of predicted (at least moderate airflow limitation), LABA/LAMA combination therapy improved lung function, quality of life, reduced rescue medication uses and COPD exacerbation versus single long-acting bronchodilators alone, without compromising safety.32,33 Nevertheless, whether our findings can be generalized to the majority of patients following the GOLD report requires further studies.
Limitations existed in this study. Firstly, our study had no controlled group which had no SDM process. In addition, evidence regarding the efficacy of SDM process on reducing inhaler errors or improving adherence in patients with newly-diagnosed COPD is still lacking. It is therefore difficult to estimate the sample size for the present study. Considering the capacity of four study sites, the duration of enrollment, and the budgets of the study, we arbitrarily estimate a number of around 100 patients for this proof-of-concept study. Future randomized controlled trials comparing SDM-facilitated device selection and usual care without an SDM process may help to directly evaluate the effects of SDM. Secondly, our study investigated outcomes in only one-month period. Further evidence is warranted to determine the long-term benefits of applying SDM before selecting the initial inhaler. Thirdly, our study did not measure the inspiratory flow rate for the patient, which might raise concerns about the adequacy of using DPIs like Ellipta® or Breezhaler®. However, the adequacy of using DPIs was evaluated by both pulmonologists and certified COPD educators. Those who obviously unable to use any study inhaler as determined by the pulmonologists and educators were excluded. In a previous study evaluated the PIFRs against different internal resistances of DPIs for COPD patients in Taiwan, insufficient PIFRs were found infrequent, mostly happened in those who were older than 75 years against medium-high resistance.34 The percentage of insufficient PIFRs against medium-low (ie, Ellipta®) and low (ie, Breezhaler®) resistance was less than 5% in the comparable group (age and severity of airflow limitation) of our study patients.34 Fourthly, we did not provide booster education between two visits. Although all errors were corrected before the end of visit 1, a proportion (38%) of patients had errors at visit 2, showing that errors might emerge. Repeated booster education might be considered while designing further studies. Lastly, patients with unstable condition, severe COPD or those unlikely to use inhalers correctly were excluded from our study. This selection bias might prevent us to study the effects of SDM in these high-risk populations.
Conclusion
In summary, our study demonstrated the feasibility of implementing SDM which might facilitate inhaler choice in patients with newly-diagnosed COPD, achieving less inhaler errors versus baseline with good adherence, high satisfaction level, and a high proportion of patients willing to keep on their initially chosen inhaler devices. Further research for evaluating long-term effect of implementing SDM to COPD patients are warranted.
Abbreviations
aORs, Adjusted odds ratios; CAT, COPD assessment test; CI, Confidence intervals; COPD, Chronic obstructive pulmonary disease; FDC, Fixed-dose combination; GOLD, Global Initiative for Obstructive Lung Disease; IQR, Interquartile ranges; LABA, Long-acting β2 agonists; LAMA, Long-acting muscarinic antagonists; mMRC, Modified medical research council; ORs, Odds ratios; SDM, Shared decision-making.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Taipei Veterans General Hospital (VGHTPE-IRB No. 2019-08-009BC), Cheng-Hsin General Hospital (CHGH-IRB (711)108B-27), National Taiwan University Hospital Yunlin Branch (201907106RINC), and Kaohsiung Medical University Hospital (KMUHIRB-E(I)-20190252). Written informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to thank all patients and educators, Ying-Ju Lin, Chun-Mei Chiu, Min-Shan Yeh, and Shiao-Yun Wu, participating in this study, James Pang from BalDr Strategic Consulting (Hong Kong) Ltd. Taiwan Branch, and Dr. Jen-Yu Hung and Tse-Kuang Kai from Kaohsiung Medical University Hospital for their assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was partially funded by grants from the Ministry of Science and Technology, Taiwan (MOST-109-2314-B-075-065 to Y.H.H. and MOST-108-2314-B-037-097-MY3 to M.J.T.), Taipei Veterans General Hospital (V111B-013 to Y.H.H.), and Kaohsiung Medical University Hospital (KMUH110-0R16 and KMUH-DK(B)11003-3 to M.J.T.). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Disclosure
C.C.S. has received speaker fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis and Pfizer, and has acted as an investigator for trials sponsored by AstraZeneca, Novartis, Roche, Sanofi-Regeneron, Galapagos, Shionogi, Aridis, Bristol Myers Squibb, Insmed and Horizon Therapeutics. H.Y.W has received honorariums for lectures from Boehringer Ingelheim, GlaxoSmithKline, Novartis and AstraZeneca. All other authors have received honorariums for lectures from Boehringer Ingelheim, GlaxoSmithKline, Novartis, AstraZeneca, and Orient EuroPharma. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Obstructive Lung Disease (GOLD). Global Strategy for Diagnosis, Management, and Prevention of COPD. Global Initiative for Obstructive Lung Disease; 2022.
2. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
3. Laube BL. The expanding role of aerosols in systemic drug delivery, gene therapy and vaccination: an update. Transl Respir Med. 2014;23. doi:10.1186/2213-0802-2-3
4. Lavorini F. Inhaled drug delivery in the hands of the patient. J Aerosol Med Pulm Drug Deliv. 2014;27(6):414–418. doi:10.1089/jamp.2014.1132
5. Lavorini F, Fontana GA, Usmani OS. New inhaler devices - the good, the bad and the ugly. Respiration. 2014;88(1):3–15. doi:10.1159/000363390
6. Liang CY, Chen YJ, Sheu SM, et al. Misuse of inhalers among COPD patients in a community hospital in Taiwan. Int J Chron Obstruct Pulmon Dis. 2018:131309–131316. doi:10.2147/COPD.S158864
7. Molimard M, Raherison C, Lignot S, et al. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49(2). doi:10.1183/13993003.01794-2016
8. Usmani OS, Lavorini F, Marshall J, et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes. Respir Res. 2018;19(1):10. doi:10.1186/s12931-017-0710-y
9. Sanduzzi A, Balbo P, Candoli P, et al. COPD: adherence to therapy. Multidiscip Respir Med. 2014;9(1):60. doi:10.1186/2049-6958-9-60
10. Sulaiman I, Cushen B, Greene G, et al. Objective assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(10):1333–1343. doi:10.1164/rccm.201604-0733OC
11. Dekhuijzen PN, Lavorini F, Usmani OS. Patients’ perspectives and preferences in the choice of inhalers: the case for Respimat((R)) or HandiHaler((R)). Patient Prefer Adherence. 2016;101561–101572. doi:10.2147/PPA.S82857
12. Kaplan A, Price D. Matching inhaler devices with patients: the role of the primary care physician. Can Respir J. 2018;2018:9473051. doi:10.1155/2018/9473051
13. Hodder R, Price D. Patient preferences for inhaler devices in chronic obstructive pulmonary disease: experience with Respimat Soft Mist inhaler. Int J Chron Obstruct Pulmon Dis. 2009;4381–4390. doi:10.2147/copd.s3391
14. Chorao P, Pereira AM, Fonseca JA. Inhaler devices in asthma and COPD – an assessment of inhaler technique and patient preferences. Respir Med. 2014;108(7):968–975. doi:10.1016/j.rmed.2014.04.019
15. Molimard M, Colthorpe P. Inhaler devices for chronic obstructive pulmonary disease: insights from patients and healthcare practitioners. J Aerosol Med Pulm Drug Deliv. 2015;28(3):219–228. doi:10.1089/jamp.2014.1142
16. Wilson SR, Strub P, Buist AS, et al. Shared treatment decision making improves adherence and outcomes in poorly controlled asthma. Am J Respir Crit Care Med. 2010;181(6):566–577. doi:10.1164/rccm.200906-0907OC
17. Inhaler Error Steering C, Price D. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107(1):37–46. doi:10.1016/j.rmed.2012.09.017
18. Elwyn G, Laitner S, Coulter A, et al. Implementing shared decision making in the NHS. BMJ. 2010:341c5146. doi:10.1136/bmj.c5146
19. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
20. Ding B, Small M, Scheffel G, et al. Maintenance inhaler preference, attribute importance, and satisfaction in prescribing physicians and patients with asthma, COPD, or asthma-COPD overlap syndrome consulting for routine care. Int J Chron Obstruct Pulmon Dis. 2018:13927–13936. doi:10.2147/COPD.S154525
21. Gregoriano C, Dieterle T, Breitenstein AL, et al. Use and inhalation technique of inhaled medication in patients with asthma and COPD: data from a randomized controlled trial. Respir Res. 2018;19(1):237. doi:10.1186/s12931-018-0936-3
22. Price D, Keininger DL, Viswanad B, et al. Factors associated with appropriate inhaler use in patients with COPD - lessons from the REAL survey. Int J Chron Obstruct Pulmon Dis. 2018:13695–13702. doi:10.2147/COPD.S149404
23. Bjermer L. The importance of continuity in inhaler device choice for asthma and chronic obstructive pulmonary disease. Respiration. 2014;88(4):346–352. doi:10.1159/000363771
24. Cheng SL. Comparison of effectiveness using different dual bronchodilator agents in chronic obstructive pulmonary disease treatment. J Clin Med. 2021;10(12). doi:10.3390/jcm10122649
25. Takaku Y, Kurashima K, Ohta C, et al. How many instructions are required to correct inhalation errors in patients with asthma and chronic obstructive pulmonary disease? Respir Med. 2017:123110–123115. doi:10.1016/j.rmed.2016.12.012
26. Dudvarski Ilic A, Zugic V, Zvezdin B, et al. Influence of inhaler technique on asthma and COPD control: a multicenter experience. Int J Chron Obstruct Pulmon Dis. 2016:112509–112517. doi:10.2147/COPD.S114576
27. Slade D, Ray R, Moretz C, et al. Time-to-first exacerbation, adherence, and medical costs among US patients receiving umeclidinium/vilanterol or tiotropium as initial maintenance therapy for chronic obstructive pulmonary disease: a retrospective cohort study. BMC Pulm Med. 2021;21(1):253. doi:10.1186/s12890-021-01612-5
28. Miravitlles M, Montero-Caballero J, Richard F, et al. A cross-sectional study to assess inhalation device handling and patient satisfaction in COPD. Int J Chron Obstruct Pulmon Dis. 2016:11407–11415. doi:10.2147/COPD.S91118
29. Zervas E, Samitas K, Gaga M. Assessment of satisfaction with different dry powder inhalation devices in Greek patients with COPD and asthma: the ANASA study. Int J Chron Obstruct Pulmon Dis. 2016;111845–111855. doi:10.2147/COPD.S113870
30. Feldman GJ, Sousa AR, Lipson DA, et al. Comparative efficacy of once-daily umeclidinium/vilanterol and tiotropium/olodaterol therapy in symptomatic chronic obstructive pulmonary disease: a randomized study. Adv Ther. 2017;34(11):2518–2533. doi:10.1007/s12325-017-0626-4
31. Martinez FJ, Fabbri LM, Ferguson GT, et al. Baseline symptom score impact on benefits of glycopyrrolate/formoterol metered dose inhaler in COPD. Chest. 2017;152(6):1169–1178. doi:10.1016/j.chest.2017.07.007
32. Han MK, Ray R, Foo J, et al. Systematic literature review and meta-analysis of US-approved LAMA/LABA therapies versus tiotropium in moderate-to-severe COPD. NPJ Prim Care Respir Med. 2018;28(1):32. doi:10.1038/s41533-018-0099-1
33. Oba Y, Keeney E, Ghatehorde N, et al. Dual combination therapy versus long-acting bronchodilators alone for chronic obstructive pulmonary disease (COPD): a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2018:12CD012620. doi:10.1002/14651858.CD012620.pub2
34. Chen SY, Huang CK, Peng HC, et al. Inappropriate peak inspiratory flow rate with dry powder inhaler in chronic obstructive pulmonary disease. Sci Rep. 2020;10(1):7271. doi:10.1038/s41598-020-64235-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.