Back to Journals » Infection and Drug Resistance » Volume 12
Shanghai Parents’ Perception And Attitude Towards The Use Of Antibiotics On Children: A Cross-Sectional Study
Authors Wang J, Sheng Y, Ni J, Zhu J, Zhou Z, Liu T, Zhang X, Zhao Q ![]()
Received 12 June 2019
Accepted for publication 28 September 2019
Published 17 October 2019 Volume 2019:12 Pages 3259—3267
DOI https://doi.org/10.2147/IDR.S219287
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Jian Wang,1,* Yuchao Sheng,2,3,* Jun Ni,4 Jianyu Zhu,5 Zhigang Zhou,5 Tianwei Liu,5 Xiaoying Zhang,6 Qi Zhao2,3
1Department of General Practice, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Epidemiology, School of Public Health, Fudan University, Shanghai, People’s Republic of China; 3The Key Laboratory of Public Health Safety of Ministry of Education, Shanghai, People’s Republic of China; 4Vaccination Clinics, Gangyan Community Health Service Center, Shanghai, People’s Republic of China; 5Vaccination Clinics, Tangqiao Community Health Service Center, Shanghai, People’s Republic of China; 6Vaccination Clinics, Huacao Community Health Service Center, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qi Zhao
Department of Epidemiology, School of Public Health, Fudan University, 130 Dongan Road, Xuhui District, Shanghai 200032, People’s Republic of China
Tel/fax +86 21 5423 7335
Email [email protected]
Background: Parents play an important role in the management of their children’s illnesses, including in decisions concerning how and whether to use antibiotics. This study aims to assess the knowledge and attitude towards antibiotics usage among young parents from different areas in Shanghai and to identify contributing factors of antibiotics usage that are comprehensible for parents.
Methods: A cross-sectional study was conducted at vaccination clinics of three community health centers from April to June 2017. Primary guardians who took children for vaccination under the national expanded immunization program were invited to participate.
Results: Of the 1368 young parents interviewed, 78.4% of them have taken their children for medical treatment, and 68.9% of their children have taken antibiotics. Parents with education level of senior high school (OR=1.850, 95% CI: 1.214–2.818), or university/college, or above (OR=3.950, 95% CI: 2.604–5.991), and parents with high-income (OR=1.360, 95% CI: 1.013–1.827) have better comprehension of antibiotics. It is found that parents who deny the existence of antibiotic abuse in China (OR=1.857, 95% CI: 1.100–3.135), who have lower income (OR=1.536, 95% CI: 1.074–2.197) and who have antibiotics prescribed by doctors (OR=1.473, 95% CI: 1.048–2.070) are associated with those incorrect practices.
Conclusion: Lack of knowledge and poor perception of antibiotics usage are found among young parents in Shanghai. Intervention should be conducted to publicize the rational use of antibiotics, reduce the rate of inappropriate behaviors and limit the sale of antibiotics.
Keywords: antimicrobial resistance, KAP, China, urban area
Background
The discovery of antibiotics was a milestone in human history. Countless lives in the previous decades were saved after this medical revolution.1 However, antimicrobial resistance (AMR) is rapidly becoming one of the most serious threats to public health.2 AMR occurs naturally, but the misuse of antibiotics on humans and animals is accelerating the process and occurring everywhere in the world.3 AMR leads to longer hospital stays, higher medical costs, increased mortality, and decreased effectiveness of treatment.4,5 Many of the medical breakthroughs since the last century could be wiped out because of the spreading of AMR. Tackling antibiotic resistance is a high priority for WHO and many governments.6
China is the largest producer and consumer of antibiotics among countries in the world. The total human usage of antibiotics in China was estimated to be approximately 77,760 tons in 2013, which was 23 times more than that in the US.7 As a result of antibiotic abuse and misuse, China has the world’s most rapid growth of antibiotic resistance.8 In 2009, Heddini et al found that more than 60% of Staphylococcus aureus isolated from Chinese patients were methicillin-resistant, much higher than that in 2000 (40%).9 Meanwhile, the proportion of Streptococcus pneumonia isolated from Chinese patients that are resistant to macrolide topped 70%.3 Antibiotics are also regarded as a panacea in many primary health-care centers in China. Doctors might overprescribe antibiotics due to lack of knowledge of its rational use.4 A recent review shows that in China 83.7% of all patients with upper respiratory tract infections (URTI) have been prescribed with antibiotics.10 However, most URTIs are caused by viruses, which do not respond to antibiotics.11
Children are more susceptible to respiratory tract infection and certain other infections.12 In developed countries, a preschool infant experiences an average of 6–10 viral infections annually.13 Parents’ practices on how to use antibiotics have important effects on the management of children’s illnesses.14 For example, parents’ high expectations of quick relief of symptoms and recovery of their children would impose further pressure on doctors to prescribe more antibiotics in order to make treatments more immediately effective.8 Parents’ knowledge and attitudes towards antibiotics usage have huge impact on their practices. Previous studies observed the connection between parents’ low level of knowledge about the use of antibiotics and the high prevalence of parents self-medicating their children with antibiotics in rural China.14,15 However, there is little research on the perception and attitude of parents from more developed areas in China.
This study aims to assess the knowledge and attitude towards antibiotics usage among young parents in different areas in Shanghai, to identify contributing factors of antibiotics usage for parents, and to provide information for further health education in Shanghai.
Methods
Study Sites
Shanghai is one of the richest areas in China and its gross domestic product (GDP) ranked 1st in the country in 2016. Three communities, Tangqiao (TQ), Huacao (HC), and Gangyan (GY), were purposefully selected for the study based on their location and economic development level in Shanghai. TQ belongs to Pudong New District and its per capita gross domestic product (GDP) was US$25,365 in 2016. HC belongs to Minhang District and its per capita GDP was US$12,429 in 2016. GY belongs to Chongming District. Chongming District is on the edge of Shanghai and its per capita GDP was US$6,664 in 2016.16
The survey was conducted in the vaccination clinic of community health centers, the only one in each community, in each study site from April to June of 2017. Parents who took children for vaccination under the national expanded immunization program were invited to participate.
Data Instrument And Collection
Face-to-face questionnaire interviews were used to collect data. The questionnaire was developed by Professor Biao Xu and the research team in the School of Public Health of Fudan University in China.14 The questionnaire collected information on: (1) demographic characteristics of the child and socioeconomic information of the parents; (2) the parents’ knowledge and attitudes on antibiotic use, including basic concepts of antibiotics, indications of antibiotic use, administration of antibiotics, AMR and other side effects; (3) parents’ experiences and practices of purchasing antibiotics without a prescription and (4) parents’ experience and practices of self-medicating children with antibiotics. In total, the nine investigators, three physicians from each vaccination clinic, all of whom were responsible for the investigation. All of them had been trained by the School of Public Health of Fudan University before the investigation began.
Data Analysis
Parents’ knowledge on antibiotics was scored from 14 selected questions, with one point for each correct answer. The scores ranged from 0 to 14, with scores above the median score deemed as being knowledgeable about antibiotics. Those who have at least one unfit behavior were defined as having inappropriate practices. To determine unfit behavior, we used the 4 questions below: (1) If I want my child to take antibiotics, I will ask the doctor directly, (2) When I want my child to take antibiotics, the dose is generally smaller than that required by the instructions, (3) When I want my child to take antibiotics, the dose is generally larger than that required by the instructions. (4) I will stock some antibiotics at home for my child.
The database was established using Epidata 3.0.1. SPSS for Windows ver. 17.0 (SPSS, Chicago, IL, USA) issued for data analysis. Means, medians, proportions and 95% confidence intervals (95% CIs) are calculated as descriptive statistics. The student’s t-test, ANOVA and Chi-square test were used to compare the differences among subgroups. Logistic regression analysis was used to identify the factors associated with knowledge level and behavior. Confounding variables were defined as those resulting in ≥10% of change in the parameter with the estimation of the variable of interest when the potential confounder is added to the logistic regression model. Statistical significance is considered to be at p<0.05.
Ethical Statement
Written consent was obtained from all participants after the study was described in the initial face-to-face interview. Approval of this study was obtained from the Ethics Committee of Zhongshan Hospital, Fudan University (B2017-036).
Results
Characteristics Of Participants
A total of 1423 questionnaires were collected and 55 questionnaires were excluded because their completion rate was less than 90%. In the remaining 1368 questionnaires, 482 (33.9%) were from TQ, 481 (33.8%) were from HC, and 405 (32.3%) were from GY. Among the respondents, 33.1% were male, with the mean age being 33.2 years old. Parents from TQ had higher educational level and higher income level compared with those from HC and GY. The coverage of health insurance was higher in TQ than in HC (97.3% vs 91.7%, P<0.001) and GY (97.3% vs 93.8%, P=0.011). Parents from HC are more likely to have more than one child than those from TQ (43.6% vs 23.3%, P<0.001) and GY (43.6% vs 22.6%, P<0.001) (Table 1).
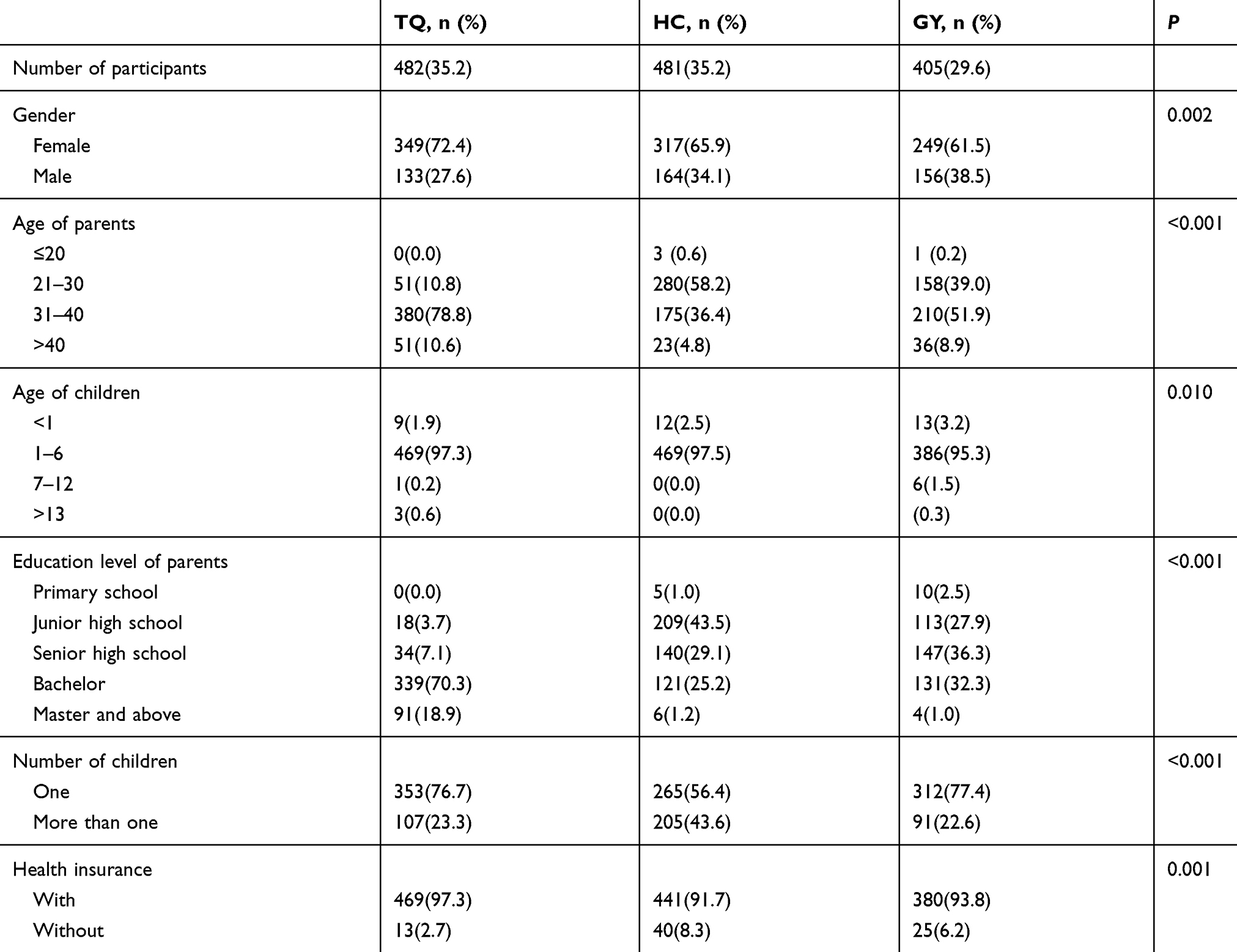 |
Table 1 Characteristics Of Participants |
Use Of Antibiotics
In the six months before the interview, 78.4% of the respondents had taken their children to hospital. The median number of medical treatments received was 2, varying from 1 to 3. In those past six months, 68.9% of the respondents said that a doctor had prescribed antibiotics for their children, with the median number of prescriptions being 1 and varying from 0 to 2. As high as 27.2% of the parents had purchased antibiotics by themselves in the past 12 months and retail pharmacy (62.2%) was the main channel for them. As high as 41.8% of the parents had self-medicated their children with antibiotics without prescriptions from doctors in the last 12 months. The main reasons cited for parents to self-medicate their children were: “Some antibiotics previously prescribed by physicians for the similar symptoms were left over at home (55.9%)” and “Children’s condition was not serious enough (38.3%)”. Parents who had purchased antibiotics by themselves were also more likely to self-medicate their children (49.0% vs 11.1%, P<0.001)
Knowledge Around The Appropriate Use Of Antibiotics And Antibiotics Resistance
As shown in Table 2, 46.5% of the participants think that antibiotics and anti-inflammatory drugs are same drugs. Only 27.4% of the participants know that antibiotics could not cure infections caused by viruses. The majority of participants (83.5%) believe that common cold does not require using antibiotics while 81.2% feel that antibiotics is not necessary when a child has a fever. More than half (60.6%) of the parents believe that antibiotics should be withdrawn as soon as the symptoms disappear. As high as 36.7% of the parents think that administration of multiple antibiotics would have better effects than a single one, and 24.6% of the parents prefer expensive antibiotics. About 29.2% of the parents believe that antibiotics can prevent the common cold.
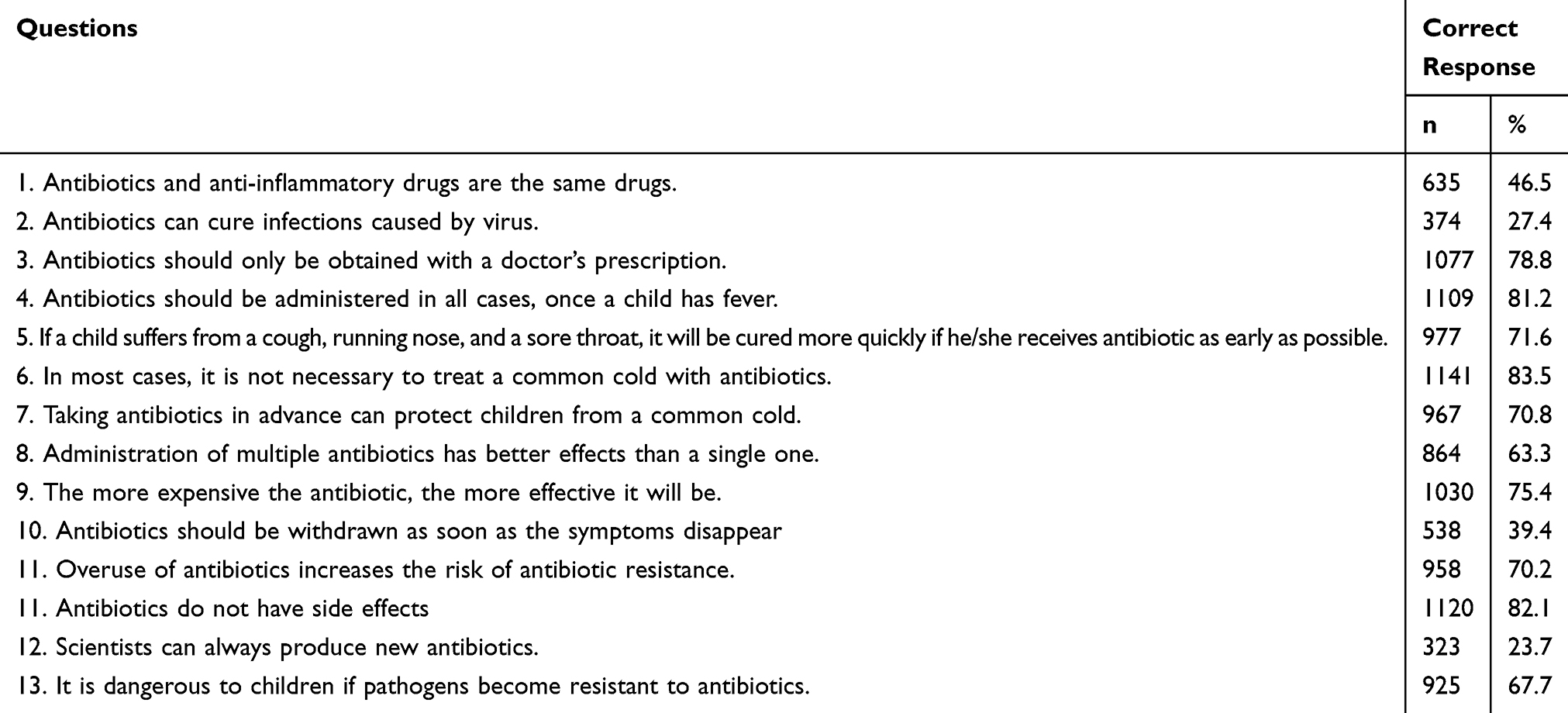 |
Table 2 Parents’ Correct Response To Questions Related To Knowledge Of Antibiotic Use |
The median score of parents for the 14 questions about antibiotics knowledge is 10, and 36% of them have higher levels of antibiotics usage knowledge. The proportion of parents with better antibiotics usage knowledge in TQ is significantly higher (51.7%) compared to those in HC (25.6%, P<0.001) and GY (29.6%, P<0.001). From multiple logistic regression analysis, we identified that parents with senior high school education (OR=1.850, 95% CI: 1.214–2.818) or college/university education and above (OR=3.950, 95% CI: 2.604–5.991) are more likely to have better knowledge of antibiotics usage than those with junior high school education or below. That is to say, the higher the parents’ education level, the higher their level of knowledge about antibiotics usage will be. High-income parents also tend to have better knowledge of antibiotics (OR=1.360, 95% CI: 1.013–1.827) (Table 3).
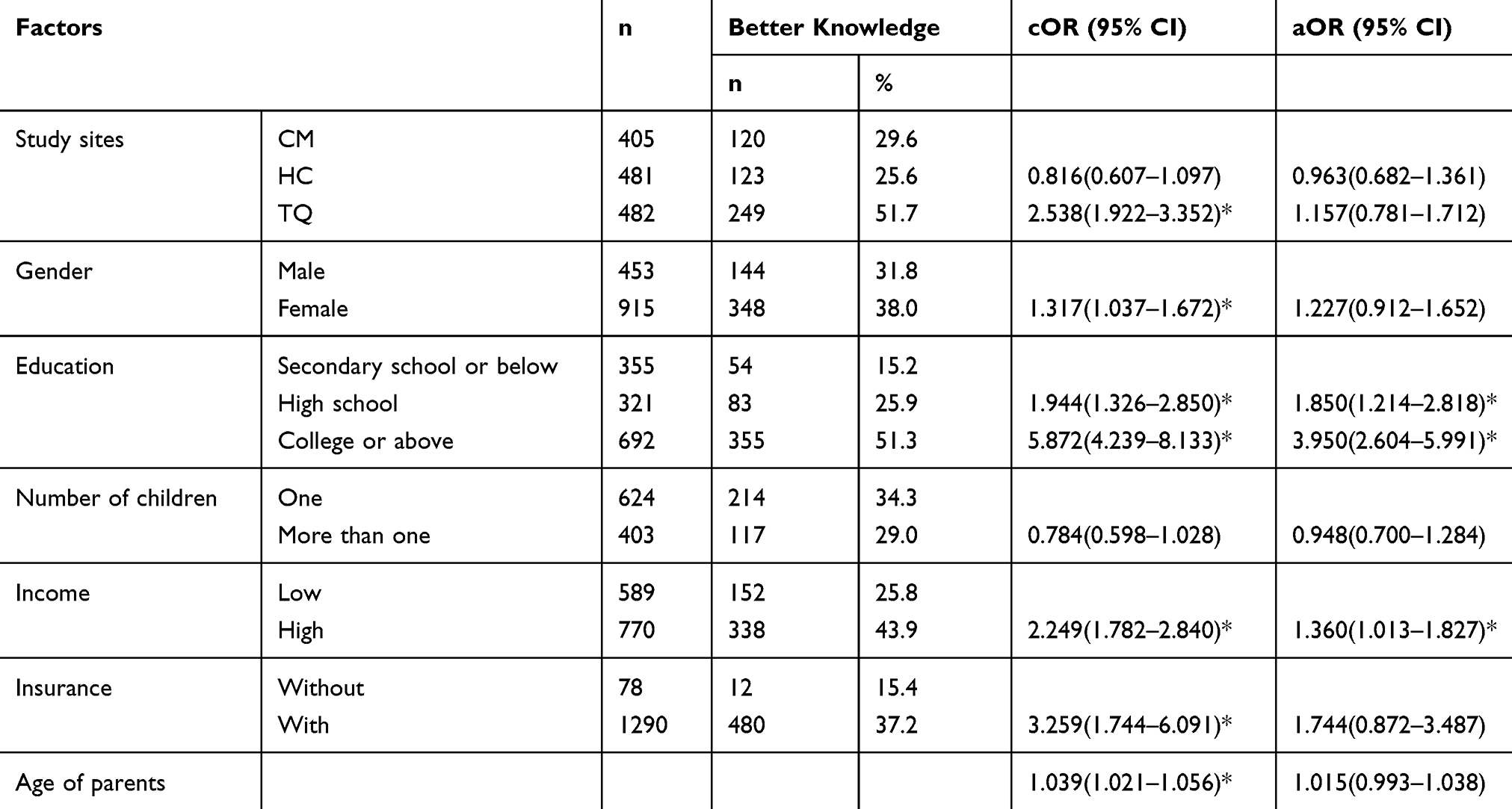 |
Table 3 Factors Associated With Better Knowledge Of The Uses Of Antibiotics |
Awareness And Attitudes Towards Antibiotics
As high as 71.6% of the parents agree that overuse of antibiotics does exist in China. Only 22.8% of the parents think that they are very knowledgeable about antibiotics while more than nine out of ten (90.4%) respondents are willing to receive more guidance on how to use antibiotics correctly. Most of the parents (71.1%) are willing to follow doctors’ advice completely. Only a few parents (9.0%) are dissatisfied if the doctors do not prescribe antibiotics. As high as 9.7% of the respondents are willing to use antibiotics by intravenous infusion. A majority of parents (90.6%) think that doctors should determine the etiological agent before prescribing (Figure 1).
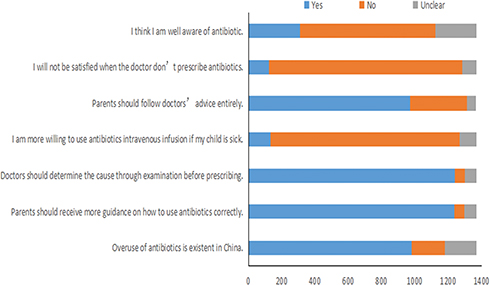 |
Figure 1 Parents’ attitude towards antibiotics. |
Practices Of Using Antibiotics
As high as 19.3% of the respondents would ask doctors to prescribe antibiotics. Nearly half (48.5%) of the parents would use lower dose of antibiotics than required by the instructions with consideration of safety, while 8.9% of the parents would choose a higher dose. More than a third of the respondents (35.9%) are likely to store antibiotics at home. Parents who would use a lower dose of antibiotics than required by the instructions (48.1% vs 24.3%, P<0.001) are more likely to store antibiotics at home.
We divided parents into two groups: Group One includes those report no use of antibiotics on their children and Group Two includes those with at least one instance of antibiotic use on their children. Multiple logistic regression results showed that the probability of having one or more instances of antibiotic use among parents from HC is 2.054 (OR=2.054, 95% CI: 1.217–3.467) times higher than parents from TQ. Denying the existence of antibiotic abuse in China (OR=1.857, 95% CI: 1.100–3.135), lower income (OR=1.536, 95% CI: 1.074–2.197) and having received prescription of antibiotics from doctors (OR= 1.473, 95% CI: 1.048–2.070) are risk factors for those practices (Table 4).
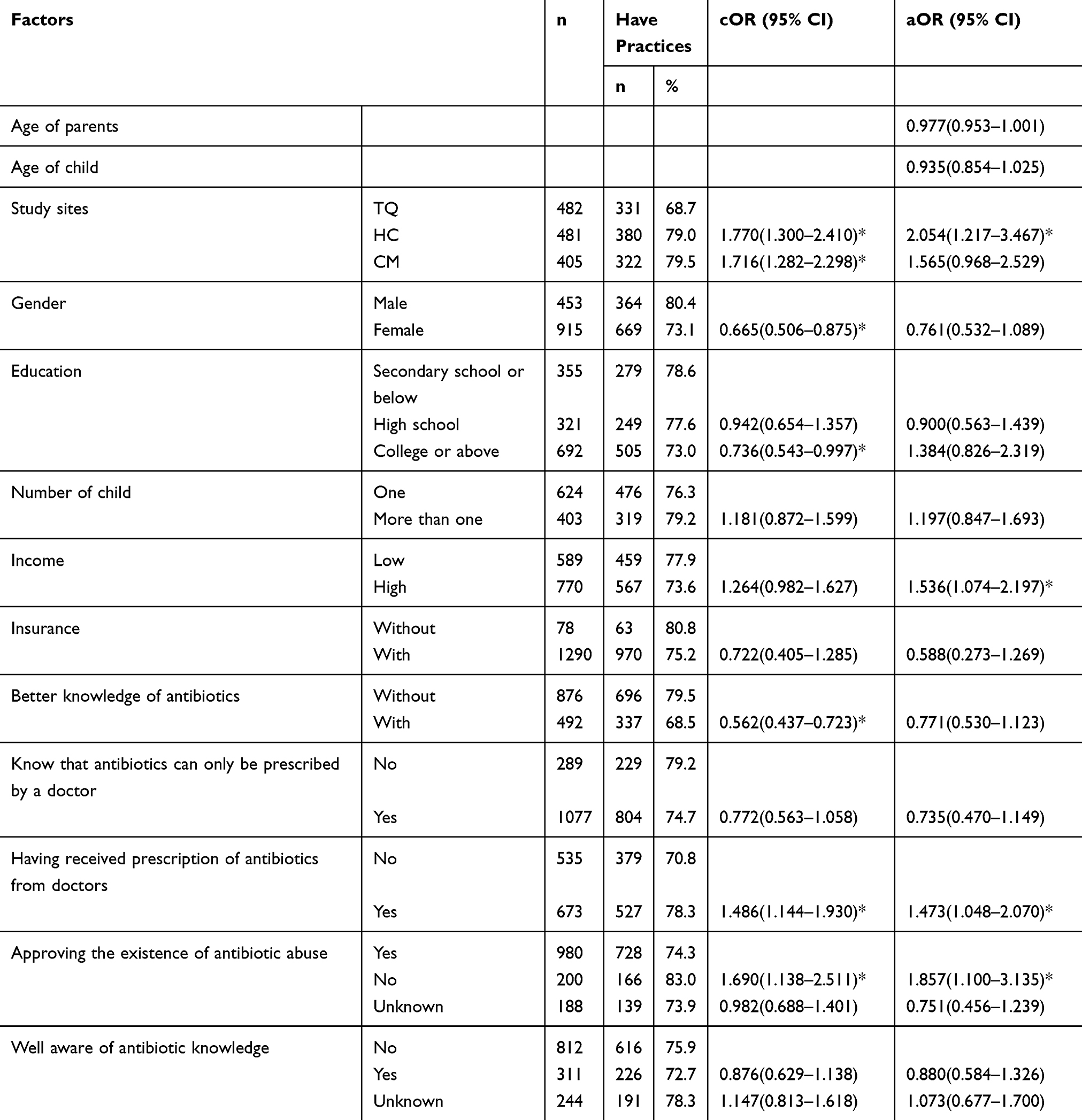 |
Table 4 Factors Associated With Practices Of Incorrect Uses Of Antibiotics |
Discussion
From our study, we found that there are misconceptions and lack of basic knowledge about the antibiotic resistance and the usage and administration of antibiotics.
Use Of Antibiotics
In our study, we find that antibiotics use is widespread over all three study sites. As high as 68.9% of the respondents claimed that they had received antibiotics from doctors in the previous 6 months. Although recall bias might impact our result, we still believe that the improper prescription of antibiotics is a severe problem in Shanghai.
As high as 41.8% of the parents had self-medicated their children with antibiotics without prescription from doctors in the last 12 months. This rate is lower than that conducted in a previous study in rural China (62.0%),14 but higher than that in a research in Lithuania (31.0%).17 The main reasons are: “The situation is not serious enough.” and “Some antibiotics previously prescribed by doctors are left over”. Only a few parents chose reasons like “do not have enough money to go to hospital”, which is comparable to results found in a previous study in Thailand.18 As high as 27.2% of the parents had purchased antibiotics by themselves in the last 12 months. A recent study in Saudi Arabia found that due to insufficient policies, 63.6% of the participants were reported to have purchased antibiotics without prescriptions from doctors at a rate higher than that found in our study (27.2%).19 Although antibiotic sales in retail pharmacies are not within the jurisdiction of government regulation,20 retail pharmacy is still the main channel for parents to purchase antibiotics in China. Both self-medication and purchase of antibiotics without a prescription would cause irrational use of antibiotics. It is essential to publicize the harm of self-medication, to strengthen the supervision of pharmacies and to limit the sale of antibiotics.
Misconception Of Antibiotics
Our study shows that parents in Shanghai are not quite knowledgeable about antibiotic usage. Only 36.0% of them answered more than 10 questions correctly, and some of them had misinterpretation about the use of antibiotics. It is a major misconception that antibiotics can treat viral infections. Previous research in Poland found that the vast majority of respondents (80%) thought that antibiotics “kill” bacteria while at the same time 60% of the respondents believed that antibiotics “kill” viruses as well.21 Hawking et al found in their qualitative study22 that most parents could not tell the difference between viral and bacterial infections. In our study, we also found that 72.7% of the parents believed that antibiotics could treat viral infections. Thus, it is essential for us to strengthen the public knowledge of the difference between viral and bacterial infection for parents.
WHO suggests that patients should always take the full prescription, even if they feel better earlier.6 However, our study found that more than 60% of the participants reported believing that antibiotics should be withdrawn as soon as the symptoms disappear. A similar finding was reported by WHO in 2015, citing that Chinese respondents (53%) are more likely to stop taking antibiotics when they feel better.6 A previous study conducted at Xi’an Jiaotong University found that more than 50% of the students agreed that the use of antibiotics could be stopped as soon as symptoms disappear and nearly 30% of the students were uncertain about the answer to this question.23
Another interesting finding is that the majority of the respondents (76.3%) think that new antibiotics can always be developed by scientists. However, low return of the investment, unpredictable and often arduous pathways of approval by regulatory agencies have caused many pharmaceutical companies to leave the antibiotics market.24 The Infectious Disease Society of America (IDSA) reported that only a single new antibiotic had been approved by the Food and Drug Administration (FDA) since 2010.25 As the development of new antibiotics is not optimistic, the thought that ‘new antibiotics can always be developed by scientists’ should be corrected.
On multivariate regression, the results show that the higher the educational level of parents, the higher level of their antibiotic knowledge; this is comparable to the results of many other studies.26–30 The possible reason might be that parents with higher levels of education have more access to knowledge and information. Furthermore, parents with higher educational levels have more opportunities to learn about the use of antibiotics. On the other hand, parents with lower educational levels have fewer opportunities to acquire knowledge on and information about antibiotic use. In our study, the respondents with higher income are shown to have a higher level of antibiotic knowledge, which is similar to the findings of a previous study.27 Compared with parents from TQ and GY, the rate of correct answers to questions related to knowledge of antibiotic use among parents from HC is the lowest. We found that the rate of correct answers from parents in TQ was lower than that of GY, which might be due to the fact that HC community has more immigrant communities compared to GY.
Our study shows that 71.6% of the parents believe that overuse of antibiotics does exist in China; this rate is higher than that from previous researches conducted in rural China (61.0%)14 and in Malaysia (67.5%),27 but lower than that from a study in Sweden (94.0%).31 This rate is alarming because Shanghai is one of the richest areas in China and the situation might be more serious in other areas.
As high as 70.2% of the parents agree that antibiotics resistance is caused by excessive use of antibiotics. Antibiotics resistance will lead to longer hospital stays, increased patient mortality and increased health-care costs, especially for children.32 In addition, children are more vulnerable than adults, and more than two-thirds of childhood mortality is related to infections.5 Unfortunately, one-third of parents do not think that it is dangerous if the pathogens become resistant to antibiotics. It is essential to increase awareness of the seriousness of antibiotics resistance, especially in parents.
Awareness And Practices Of Antibiotics Use
In general, it is reported that AMR mainly results from incompliance with treatment, uncompleted treatment, irregular treatment, and inadequate dosage.33 In our research, a higher percentage of parents choose a lower dose of antibiotics compared to those who choose a higher dose of antibiotics to treat their child. This result is comparable to that of a previous study in Shandong province, China.15 The result may be attributed to a Chinese traditional concept that any drug does harm to people’s health to some extent. However, lower dose of antibiotics will prolong the treatment course, increase the risk of AMR and treatment failure. A total of 35.9% of the parents had stored antibiotics at home for future need. In addition, we found that parents who use a lower dose of antibiotics than that required by the instructions have a higher probability of storing antibiotics at home. Thus, antibiotics would be left over due to the lower dose used, and then these left-over antibiotics would be stored at home for future, unprescribed use. Therefore, it is essential to ask parents to follow the correct dose on the instructions. After adjusting the confounding factors, logistic regression analysis found that parents from HC are more likely to have irrational practices than parents from TQ. This is in line with the above result of parents’ knowledge of antibiotic and the main reason is that HC has one of the largest immigrant communities in Shanghai. Parents who have received prescriptions of antibiotics from doctors in the previous 6 months are more likely to have those behaviors, which indicates that it is essential to restrict the prescriptions of antibiotics. Reducing the opportunity of parents’ contact with antibiotics may be an effective way to decrease the rate of irrational antibiotic usage.
Conclusion
In conclusion, this study revealed incomplete knowledge and poor understanding of antibiotic usage among parents in Shanghai, especially in the HC area. The prescription of antibiotics from doctors may impact parents’ practice of using antibiotics on children. Intervention should be conducted to regulate the prescriptions of antibiotics, advocate for rational use of antibiotics by parents to reduce inappropriate behaviors and limit the sale of antibiotics in retail pharmacies.
Abbreviations
AMR, antimicrobial resistance; cOR, crude odds ratio; aOR, adjusted odds ratio; CI, confidence interval; TQ, Tangqiao; HC, Huacao; GY, Gangyan.
Availability Of Data And Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval And Consent Of Participant
Written consent was obtained from all participants after the study was described in the initial face-to-face interview. Approval of this study was obtained from the Ethics Committee of Zhongshan Hospital, Fudan University (B2017-036).
Acknowledgments
The author is grateful to those staff members from the three community health centers for their help in conducting the questionnaire. We greatly appreciate April Ai-Rou Qian (a rising Junior in the Molecular Biology and Biochemistry department at Middlebury College, USA) for her time and efforts to revise the manuscript.
Author Contributions
Jian Wang, Yuchao Sheng and Qi Zhao participated in the study design, data collection, analysis and the writing of manuscript. Jun Ni, Jianyu Zhu, Zhigang Zhou, Tianwei Liu, and Xiaoying Zhang participated in the data collection. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol R. 2010;74(3):417–433. doi:10.1128/MMBR.00016-10
2. World Health Organization. Antimicrobial Resistance: Global Report on Surveillance. Geneva: WHO; 2014.
3. Hvistendahl M. China takes aim at rampant antibiotic resistance. Science. 2012;336(6083):795. doi:10.1126/science.336.6083.795
4. Li Y. China’s misuse of antibiotics should be curbed. BMJ. 2014;348(feb125):g1083. doi:10.1136/bmj.g1083
5. Laxminarayan R, Duse A, Wattal C, et al. Antibiotic resistance-the need for global solutions. Lancet Infect Dis. 2013;13(12):1057–1098. doi:10.1016/S1473-3099(13)70318-9
6. World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. Geneva: WHO; 2015.
7. Zhang Q, Ying G, Pan C, Liu Y, Zhao J. Comprehensive evaluation of antibiotics emission and fate in the river basins of China: source analysis, multimedia modeling, and linkage to bacterial resistance. Environ Sci Technol. 2015;49(11):6772–6782. doi:10.1021/acs.est.5b00729
8. Quan-Cheng K, Jian-Guo W, Xiang-Hua L, Zhen-Zhen L. Inappropriate use of antibiotics in children in China. Lancet. 2016;387(10025):1273–1274. doi:10.1016/S0140-6736(16)30019-8
9. Heddini A, Cars O, Qiang S, Tomson G. Antibiotic resistance in China–a major future challenge. Lancet. 2009;373(9657):30. doi:10.1016/S0140-6736(08)61956-X
10. Li J, Song X, Yang T, et al. A systematic review of antibiotic prescription associated with upper respiratory tract infections in China. Medicine. 2016;95(19):e3587. doi:10.1097/MD.0000000000004864
11. O’Sullivan JW, Harvey RT, Glasziou PP, McCullough A. Written information for patients (or parents of child patients) to reduce the use of antibiotics for acute upper respiratory tract infections in primary care. Cochrane Database Syst Rev. 2016;11:D11360. doi:10.1002/14651858.CD011360.pub2
12. Wang H, Wang B, Zhao Q, et al. Antibiotic body burden of chinese school children: a multisite biomonitoring-based study. Environ Sci Technol. 2015;49(8):5070–5079. doi:10.1021/es5059428
13. Pavia AT. Viral infections of the lower respiratory tract: old viruses, new viruses, and the role of diagnosis. Clin Infect Dis. 2011;52(Supplement 4):S284–S289. doi:10.1093/cid/cir043
14. Yu M, Zhao G, Stalsby LC, Zhu Y, Zhao Q, Xu B. Knowledge, attitudes, and practices of parents in rural China on the use of antibiotics in children: a cross-sectional study. BMC Infect Dis. 2014;14:112. doi:10.1186/1471-2334-14-112
15. Ding L, Sun Q, Sun W, et al. Antibiotic use in rural China: a cross-sectional survey of knowledge, attitudes and self-reported practices among caregivers in Shandong province. BMC Infect Dis. 2015;15:1. doi:10.1186/s12879-015-1323-z
16. 2016 Shanghai GDP and GDP rankings by region. Available from: http://www.chyxx.com/industry/201708/554713.html. Accessed Dec 20, 2017.
17. Pavyd E, Veikutis V, Ma Iulien A, et al. Beliefs and behavior on antibiotic use and self-medication in Lithuania. Int J Env Res Pub He. 2015;12(6):7002–7016. doi:10.3390/ijerph120607002
18. Treesirichod A, Chaithirayanon S, Chansakulporn S. Self-medication for dermatologic diseases among children treated at the HRH Princess Maha Chakri Sirindhorn Medical Center. J Med Assoc Thai. 2015;98(Suppl 9):S135–S139.
19. El Zowalaty ME, Belkina T, Bahashwan SA, et al. Knowledge, awareness, and attitudes toward antibiotic use and antimicrobial resistance among Saudi population. Int J Clin Pharm Net. 2016;38(5):1261–1268. doi:10.1007/s11096-016-0362-x
20. Xiao Y, Li L. Legislation of clinical antibiotic use in China. Lancet Infect Dis. 2013;13(3):189–191. doi:10.1016/S1473-3099(13)70011-2
21. Mazi Ska B, Stru Ycka I, Hryniewicz W. Surveys of public knowledge and attitudes with regard to antibiotics in Poland: did the European Antibiotic Awareness Day campaigns change attitudes? PLoS One. 2017;12(2):e172146.
22. Hawking MK, Lecky DM, Touboul Lundgren P, et al. Attitudes and behaviours of adolescents towards antibiotics and self-care for respiratory tract infections: a qualitative study. BMJ Open. 2017;7(5):e15308. doi:10.1136/bmjopen-2016-015308
23. Lv B, Zhou Z, Xu G, et al. Knowledge, attitudes and practices concerning self-medication with antibiotics among university students in western China. Trop Med Int Health. 2014;19(7):769–779. doi:10.1111/tmi.12322
24. Bassetti M, Merelli M, Temperoni C, Astilean A. New antibiotics for bad bugs: where are we? Ann Clin Microbiol Antimicrob 2013;12(1):22.
25. Boucher HW, Talbot GH, Benjamin DK, et al. 10 x ‘20 progress–development of new drugs active against gram-negative bacilli: an update from the infectious diseases society of America. Clin Infect Dis. 2013;56(12):1685–1694. doi:10.1093/cid/cit152
26. Panagakou SG, Papaevangelou V, Chadjipanayis A, Syrogiannopoulos GA, Theodoridou M, Hadjichristodoulou CS. Risk factors of antibiotic misuse for upper respiratory tract infections in children: results from a cross-sectional knowledge-attitude-practice study in Greece. ISRN Pediatr. 2012;2012:1–8. doi:10.5402/2012/685302
27. Teck KC, Ghazi HF, Bin Ahmad MI, et al. Knowledge, attitude, and practice of parents regarding antibiotic usage in treating childrens upper respiratory tract infection at primary health clinic in Kuala Lumpur, Malaysia: pilot study. Health Serv Res Manag Epidemiol. 2016;3:233339281664372. doi:10.1177/2333392816643720
28. Pan DST, Huang JH, Lee MHM, et al. Knowledge, attitudes and practices towards antibiotic use in upper respiratory tract infections among patients seeking primary health care in Singapore. BMC Fam Pract. 2016;17(1). doi:10.1186/s12875-016-0547-3
29. Dunn-Navarra A, Stockwell MS, Meyer D, Larson E. Parental health literacy, knowledge and beliefs regarding upper respiratory infections (URI) in an urban latino immigrant population. J Urban Health. 2012;89(5):848–860. doi:10.1007/s11524-012-9692-8
30. Agarwal S. Antibiotics use and misuse in children: a knowledge, attitude and practice survey of parents in India. J Clin Diagn Res. 2015. doi:10.7860/JCDR/2015/14933.6819
31. Vallin M, Polyzoi M, Marrone G, Rosales-Klintz S, Tegmark Wisell K, Stålsby Lundborg C. Knowledge and attitudes towards antibiotic use and resistance - a latent class analysis of a swedish population-based sample. PLoS One. 2016;11(4):e152160. doi:10.1371/journal.pone.0152160
32. Principi N, Esposito S. Antimicrobial stewardship in paediatrics. BMC Infect Dis. 2016;16(1). doi:10.1186/s12879-016-1987-z
33. Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309–318. doi:10.1179/2047773215Y.0000000030
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.