")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
SGLT2 inhibitors and the changing landscape for treatment of diabetes
Authors Liu S , Lam A , Wazir A , Cheema AN
Received 4 March 2019
Accepted for publication 28 April 2019
Published 9 July 2019 Volume 2019:15 Pages 861—867
DOI https://doi.org/10.2147/TCRM.S207515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Shuangbo Liu,1 Anna Lam,2 Arslan Wazir,1 Asim N Cheema1
1Terrence Donnelly Heart Centre, St Michael’s Hospital, University of Toronto, Toronto, Ontario, Canada; 2Division of Endocrinology, University of Alberta, Edmonton, Alberta, Canada
Abstract: Type 2 diabetes mellitus has become an epidemic with rapidly increasing prevalence worldwide. While strict glycemic control has been shown to reduce the risk of diabetic microvascular complications, its role in preventing cardiovascular disease has been less clear. Indeed, anti-hyperglycemic therapies have historically been neutral for cardiovascular benefit. However, recent cardiovascular outcome trials utilizing sodium glucose transporter 2 inhibitors across a broad spectrum of cardiovascular disease patients have demonstrated significant mortality benefit resulting in a paradigm shift in the approach towards patients with heart disease and diabetes mellitus.
Keywords: diabetes, empagliflozin, SGLT2
Introduction
Type 2 diabetes mellitus (T2DM) has become an epidemic with rapidly increasing prevalence worldwide.1,2 It is associated with microvascular (retinopathy, nephropathy, and neuropathy) and macrovascular (myocardial infarction (MI), congestive heart failure (CHF) and stroke) complications.3 While strict glycemic control has been shown to reduce the risk of diabetic microvascular complications, its role in preventing cardiovascular disease (CVD) has been less clear.4,5 Indeed, anti-hyperglycemic therapies have historically been neutral for cardiovascular (CV) benefit, and all new anti-hyperglycemic agents are evaluated in large clinical trials to ensure CV safety, since observation of increased mortality risk associated with thiazolidinediones use in patients with CVD. Sodium glucose co-transporter 2 inhibitors (SGLT2) are marking a new era in the treatment of T2DM after showing significant mortality benefit in patients with CVD. The objective of this narrative review is to discuss the pathophysiology of how SGLT2 may reduce CV outcomes and provide an overview of the current evidence for this therapy.
Glycemic control in T2DM
The management of patients with diabetes is multifaceted and requires an interdisciplinary approach with lifestyle changes, assessment for micro- and macrovascular complications, prevention of hyperglycemia, and monitoring of CV risk. Suboptimal glycemic control with a glycated hemoglobin (A1C) level >7% is associated with an increase in microvascular and CV complications.6,7 In contrast, strict glycemic control in the UK Prospective Diabetes Study (UKPDS) trial was associated with a significant reduction in the risk of microvascular complications, but had no significant beneficial effect on CV outcomes.6 More recent randomized controlled trials (RCT) such as Action to Control Cardiovascular Risk in Diabetes (ACCORD) and Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation (ADVANCE) confirmed that there was no improvement in CV outcomes with intensive glycemic control.5,8 In the ACCORD trial, intensive glycemic control (A1C<6%) was associated with an increase in mortality (1.41% vs 1.14% per year, hazard ratio (HR)=1.22) compared to standard therapy (A1C=7–7.9%) at 3.5 year follow-up, which led to early study termination.8
Anti-hyperglycemic treatment regimens and targets need to be individualized for each patient. With a growing list of available agents, there are many anti-hyperglycemic combinations to achieve the therapeutic A1C target. Metformin is generally the initial therapy due to its low cost, safety profile, and possible CV benefits, unless there are contraindications.9 If the A1C target is not achieved with monotherapy, a second-line anti-hyperglycemic agent (dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists, SGLT2 inhibitors, insulin secretagogues, thiazolidinediones, and insulin) can be added. The choice of a specific anti-hyperglycemic agent will depend on multiple factors, including the severity of hyperglycemia, patient comorbidities, side-effect profile (such as hypoglycemia, weight gain), cost considerations, and patient preference.
SGLT2 inhibitors and glucose metabolism
The kidneys play a critical role in glucose regulation via gluconeogenesis and glucose reabsorption from the glomerular filtrate.10 Renal glucose reabsorption occurs via two SGLT channels (SGLT1 and SGLT2) located in the proximal tubule.11 SGLT2 is responsible for approximately 90% of glucose reabsorption, while SGLT1 accounts for the remaining 10%.11 In a healthy kidney, 99% of glucose is reabsorbed and very little is present in the urine.10 However, in patients with T2DM, plasma glucose levels exceed the maximum glucose transport capacity, leading to glycosuria. This results in up-regulated SGLT genes, increased renal glucose reabsorption, and further hyperglycemia, thus making SGLT2 a logical target in the management of T2DM. Currently, three SGLT2 inhibitors are commercially available, and include empagliflozin (Jardiance, Boehringer Ingelheim and Eli Lilly), canagliflozin (Invokana, Janssen), and dapagliflozin (Forxiga, Bristol-Myers Squibb, and AstraZeneca).
EMPA-REG OUTCOME trial
Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) was a large multi-center randomized double-blind, placebo-controlled trial (Table 1)12 designed to examine CV morbidity and mortality outcomes with empagliflozin compared to placebo in patients with T2DM at high risk of CV events. This intention to treat analysis compared pooled empagliflozin (10 mg and 25 mg groups) vs placebo using a four-step hierarchical-testing strategy to assess for non-inferiority and superiority. All eligible patients underwent a 2-week placebo run in period before being randomized to empagliflozin 10 mg once daily, empagliflozin 25 mg once daily, or placebo once daily.
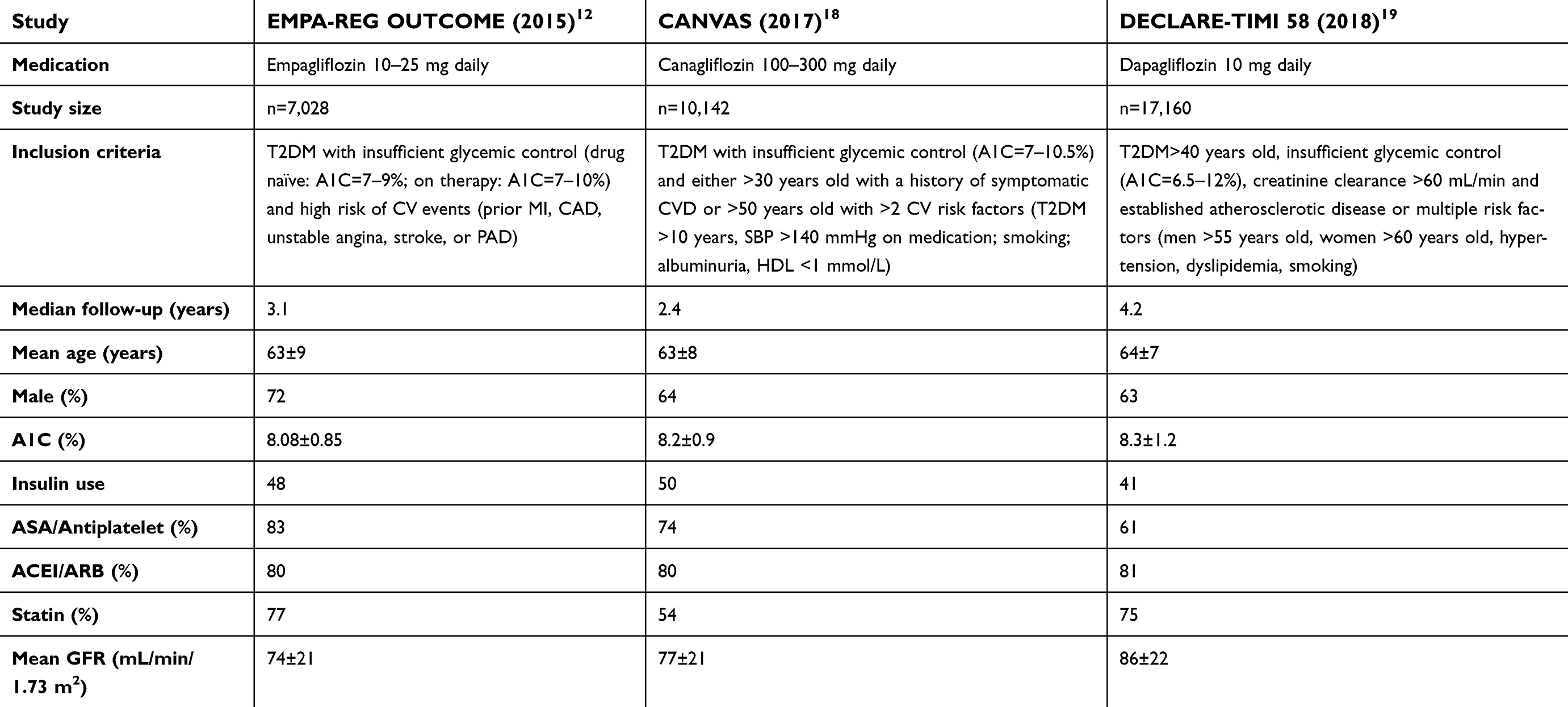 |
Table 1 Inclusion criteria and baseline characteristics of EMPA-REG OUTCOME, CANVAS, and DECLARE-TIMI 58 |
Between 2010–2013, 11,531 patients were assessed for eligibility and 7,028 patients underwent randomization. Of the 39% of potentially eligible patients excluded, 85% did not meet the inclusion/exclusion criteria. The two groups were well-matched with no statistically significant difference in baseline characteristics. The mean age was 63±9 years, and 72% were male. The mean A1C was 8.08±0.85%, 57% of patients had diabetes for more than 10 years, and 48% of patients were on insulin. The majority of patients (95%) were treated with anti-hypertensive medications, with 80% on angiotensin-converting enzyme inhibitor or angiotensin receptor blockers. Also, 77% of patients were on statin therapy and 83% were on aspirin.
The primary outcome of CV death, non-fatal MI or non-fatal stroke (Table 2) was significantly reduced in the pooled empagliflozin group (12.1%) compared to placebo (10.5%) with HR=0.86 (95% confidence interval (CI)=0.74–0.99). Based on the Kaplan-Meier curve, the outcomes appear to separate early by 3 months of treatment. When the individual components of the primary outcome are examined, CV mortality was significantly reduced (3.7% empagliflozin vs 5.9% placebo, HR=0.62, 95% CI=0.49–0.77, P<0.001), whereas non-fatal MI (4.5% empagliflozin vs 5.2% placebo, HR=0.87, 95% CI=0.70–1.09, P=0.22) and stroke (3.2% empagliflozin vs 2.6% placebo, HR=1.24, 95% CI=0.92–1.67, P=0.16) were not significantly different. Hospitalization for CHF, (2.7% empagliflozin vs 4.1% placebo, HR=0.65, 95% CI=0.50–0.85, P=0.002) and all-cause mortality (5.7% empagliflozin vs 8.3% placebo, HR=0.68, 95% CI=0.57–0.82, P<0.001) were also significantly reduced with empagliflozin compared to placebo.
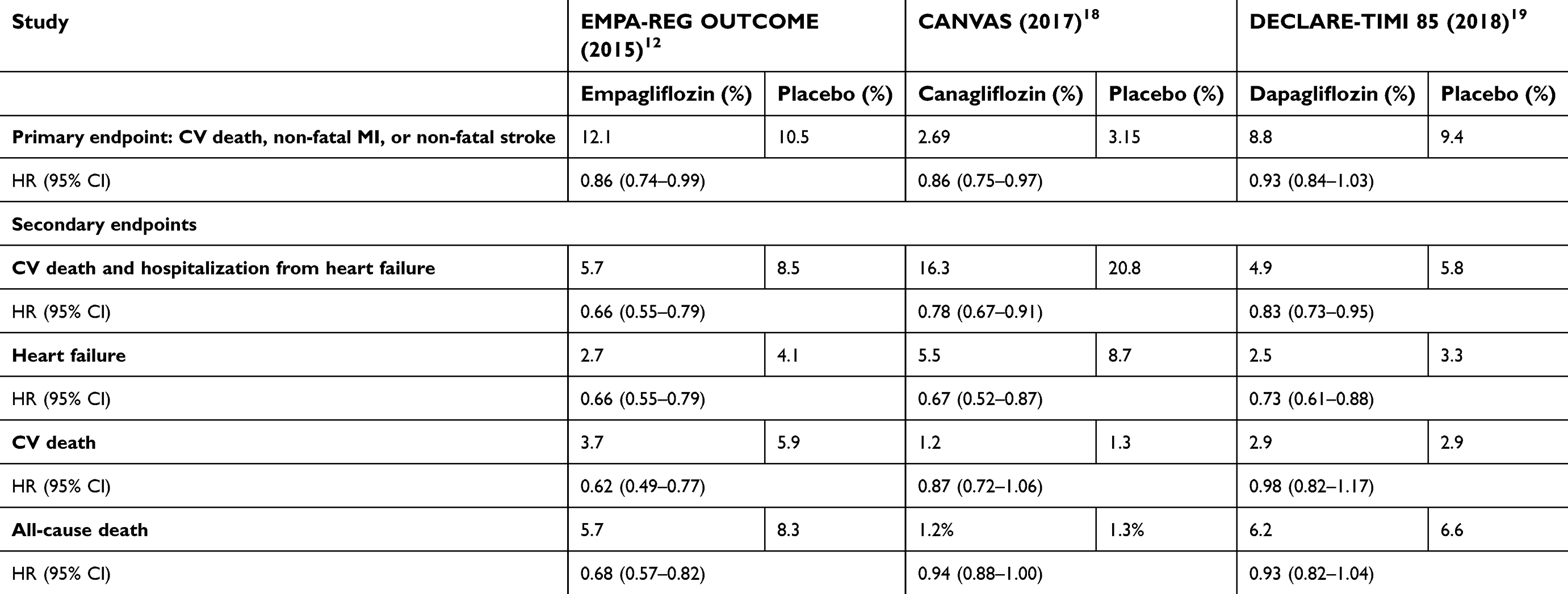 |
Table 2 Study endpoints of EMPA-REG OUTCOME, CANVAS, and DECLARE-TIMI 58 |
The rate of any adverse event in the study was high (90% empagliflozin vs 92% placebo, P<0.001), but rates of adverse events leading to discontinuation of study drug were lower (17% empagliflozin vs 19.4% placebo, P<0.01). Urinary tract infection in female patients (36.4% empagliflozin vs 40.6% in placebo, P<0.05) and genital infections in both genders (6.4% empagliflozin vs 1.8% placebo, P<0.001) occurred more in patients receiving empagliflozin than placebo.
EMPA-REG OUTCOME was a well-designed RCT, and its results have been practice changing specifically as it relates to the management of CV risk in patients with T2DM. This study showed significant mortality benefit (both CV and all-cause) as well as a reduction in hospitalization for CHF. The number needed to treat for the primary outcome (composite of CV death, non-fatal MI, and stroke) was 63 patients over 3.1 years, a benefit mainly driven by reduction of CV death. Similarly, the HR for hospitalization from CHF was significantly lower (HR=0.66, 95% CI=0.55–0.79) with an absolute risk reduction of 1.4% and a number needed to treat of 71 over 3.1 years.
The mechanism of CV benefit with SGLT2 inhibitors
It is interesting to note that the clinical benefit of SGLT2 inhibitors in reducing CV morbidity and mortality was seen early after treatment initiation and exceeds the benefit expected from modest improvement observed in the metabolic profile of treated patients. In addition to a 0.3% difference of A1C levels between the study and the control arm at study end, the empagliflozin group in the EMPA-REG OUTCOME trial demonstrated only a mild reduction in systolic and diastolic blood pressure measurements, moderate weight reduction, and lower uric acid levels throughout the study period. However, the clinical benefit of empagliflozin was seen as early as 3 months after initiation of treatment, strongly suggesting an independent mechanism of cardio-protection in treated patients.
Proposed mechanisms for the cardioprotective of empagliflozin include reduction in cardiac inflammation,13 decreased cardiac oxidative stress,14 decreased cardiac apoptosis,15 and improved cardiac mitochondrial function.14 Recently reported results from the Effects of Empagliflozin on Cardiac Structure in Patients with Type 2 Diabetes (EMPA-HEART) trial identified a significant reduction in left ventricular mass index on cardiac magnetic resonance at 6 months in the empagliflozin group compared to placebo (−2.6 vs −0.01 gm/m2, P=0.01) suggesting the beneficial effects on left ventricular remodeling.16 In addition, treatment with empagliflozin may also improve cardiac energy metabolism via increased glucose and fatty acid oxidation translating into a cardioprotective effect for patients with heart failure.17 However, further mechanistic studies are needed to better elucidate the remarkable results observed in the EMPA-REG OUTCOME trial.
Additional studies examining the efficacy and safety of other SGLT2 inhibitors, canagliflozin18 and dapagliflozin,19 have demonstrated CV outcome benefits that are consistent with the EMPA-REG OUTCOME study confirming that CV protection is indeed a class effect rather than characteristic of a specific compound.
CANVAS and DECLARE trials
Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes (CANVAS)18 integrated data from two RCTs (CANVAS and CANVAS-R) to examine the effects of treatment with canagliflozin on 10,142 patients with T2DM and high risk of CVD. Baseline characteristics are shown in Table 1. The primary outcome (composite of death from CV cause, non-fatal MI, or non-fatal stroke) was lower with canagliflozin than placebo (2.69% vs 3.15%, HR=0.86, 95% CI=0.75–0.97). Similar to EMPA-REG OUTCOME, there was a reduction in CHF with canagliflozin compared to placebo (0.55% vs 0.87%, HR=0.67, 95% CI=0.52–0.87), but, unlike EMPA-REG OUTCOME, CV death (1.2% vs 1.3%, HR=0.87, 95% CI=0.72–1.06) and all-cause death (1.2% vs 1.3%, HR=0.94, 95% CI=0.88–1.00) were not reduced. This is likely due to differences in the inclusion criteria – EMPA-REG OUTCOME included patients with established CVD, whereas CANVAS included patients without symptomatic CVD but at least two CV risk factors. This lower risk patient population led to lower event rates and, overall, less power to detect a difference between the two groups. Treatment with canagliflozin was associated with an increase in rate of amputation (0.63% vs 0.34%, P<0.001) and bone fracture (1.54% vs 1.19%, P<0.02). Also, canagliflozin was associated with an increase in infection of male genitalia (3.49% vs 1.08%, P<0.001), mycotic genital infection in women (6.88% vs 1.75%, P<0.001), osmotic diuresis (3.45% vs 1.33%, P<0.001), and volume depletion (2.6% vs 1.85%, P=0.009).
In the Dapagliflozin Effect on Cardiovascular Events (DECLARE TIMI 58) study,19 17,160 patients with T2DM and a history or at risk of CV disease were randomized to either dapagliflozin or placebo. Dapagliflozin did not reduce the primary endpoint (CV death, non-fatal MI, or stroke) compared to placebo (8.8% vs 9.4%, HR=0.93, 95% CI=0.84–1.03). The rates of CV death (2.9% vs 2.9%, HR=0.98, 95% CI=0.82–1.17) and all-cause death (6.2% vs 6.6%, HR=0.93, 95% CI=0.82–1.04) were similar between the two groups. Approximately 60% of the included patients did not have atherosclerotic CVD, and therefore the patient population is lower risk than EMPA-REG OUTCOME, which could contribute to the lower event rates and lack of statistical difference. Similar to EMPA-REG OUTCOME and CANVAS, DECLARE TIMI 58 demonstrated a reduction in hospitalization for CHF (2.5% vs 3.3%, HR=0.73, 95% CI=0.61–0.88). Dapagliflozin was associated with an increase in the rate of diabetic ketoacidosis (0.3% vs 0.1%, P=0.02) and genital infection (0.9% vs 0.1%, P<0.0001). Rates of acute kidney injury were reduced with dapagliflozin compared to placebo (1.5% vs 2.0%, P=0.002).
A network meta-analysis of nine large CV outcome trials of new antidiabetic drugs included two SGLT2 trials (EMPA-REG OUTCOME and CANVAS), but not the more recent DECLARE TIMI 58.20 The meta-analysis demonstrated a 28% reduction in CHF hospitalization events with SGLT2 therapy compared to placebo (risk ratio=0.72, 95% CI=0.6–0.86). Ranking for the network meta-analysis showed empagliflozin ranked first in reducing major adverse cardiovascular events, CV death, non-fatal MI, death from any cause and CHF hospitalizations, compared to canagliflozin. Another meta-analysis included all three SGLT2 RCTs, but only assessed CHF outcomes which demonstrated a significant reduction in hospitalizations for CHF (odds ratio=0.70, 95% CI=0.61–0.79).21 However, an updated meta-analysis including all SGLT2 RCTs would be helpful to assess the potential benefits for important clinical outcomes.
Conclusion
Recent trials that included T2DM patients across a spectrum of CV risk have demonstrated significant CV benefit with SGLT2 inhibitors resulting in a paradigm shift for the management of these high risk patients. Although additional studies are required to better understand the mechanism underlying observed CV risk modification, the clinical implications for an individual patient cannot be ignored. Therefore, SGLT2 inhibitors should be a part of the therapeutic regimen for all eligible T2DM patients with established CVD and strongly considered for those T2DM patients at high risk of future CV events.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64:1929–1949. doi:10.1016/j.jacc.2014.07.017
2. International Diabetes Federation IDF Diabetes Atlas, 8th edn. Brussels, Belgium: International Diabetes Federation, 2017. Available from: http://www.diabetesatlas.org. Accessed December 1, 2018.
3. Public Health Agency of Canada, Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011. Available from: https://www.canada.ca/content/dam/phac-aspc/migration/phac-aspc/cd-mc/publications/diabetes-diabete/facts-figures-faits-chiffres-2011/pdf/facts-figures-faits-chiffres-eng.pdf. Accessed December 1, 2018.
4. Gerstein HC, Miller ME, Genuth S, et al. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011;364:818–828. doi:10.1056/NEJMoa1006524
5. Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–2572. doi:10.1056/NEJMoa0802987
6. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet (London, England). 1998;352:837–853.
7. The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes. 1995;44:968–983.
8. Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose lowering in Type 2 diabetes. N Engl J Med. 2008;358:2545–2559. doi:10.1056/NEJMoa0802743
9. Lipscombe L, Booth G, Butalia S, et al. Pharmacologic glycemic management of Type 2 diabetes in adults. Can J Diabetes. 2018;42(Suppl 1):S88–s103. doi:10.1016/j.jcjd.2017.10.034
10. Gerich JE. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: therapeutic implications. Diabetic Med. 2010;27:136–142. doi:10.1111/j.1464-5491.2009.02894.x
11. Wright EM. Renal Na(+)-glucose cotransporters. Am J Physiol Renal Physiol. 2001;280:F10–8. doi:10.1152/ajprenal.2001.280.1.F10
12. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373:2117–2128. doi:10.1056/NEJMoa1504720
13. Lin B, Koibuchi N, Hasegawa Y, et al. Glycemic control with empagliflozin, a novel selective SGLT2 inhibitor, ameliorates cardiovascular injury and cognitive dysfunction in obese and type 2 diabetic mice. Cardiovasc Diabetol. 2014;13:148. doi:10.1186/1475-2840-13-80
14. Habibi J, Aroor AR, Sowers JR, et al. Sodium glucose transporter 2 (SGLT2) inhibition with empagliflozin improves cardiac diastolic function in a female rodent model of diabetes. Cardiovasc Diabetol. 2017;16:9. doi:10.1186/s12933-017-0624-5
15. Hammoudi N, Jeong D, Singh R, et al. Empagliflozin improves left ventricular diastolic dysfunction in a genetic model of Type 2 diabetes. Cardiovasc Drug Ther. 2017;31:233–246. doi:10.1007/s10557-017-6734-1
16. Verma S, Mazer CDYan AT
17. Verma S, Rawat S, Ho KL, et al. Empagliflozin increases cardiac energy production in diabetes: novel translational insights into the heart failure benefits of SGLT2 inhibitors. JACC. 2018;3:575–587. doi:10.1016/j.jacbts.2018.07.006
18. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in Type 2 diabetes. N Engl J Med. 2017;377:644–657. doi:10.1056/NEJMoa1611925
19. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in Type 2 diabetes. N Engl J Med. 2019;380(4):347–357.
20. Alfayez OM, Al Yami MS, Alshibani M, et al. Network meta-analysis of nine large cardiovascular outcome trials of new antidiabetic drugs. Prim Care Diabetes. 2019;13:204–211. doi:10.1016/j.pcd.2019.01.003
21. Singh AK, Singh R. Heart failure hospitalization with SGLT-2 inhibitors: a systematic review and meta-analysis of randomized controlled and observational studies. Expert Rev Clin Pharmacol. 2019;12:299–308. doi:10.1080/17512433.2019.1588110
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.