Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Sex-Specific Associations Between Serum Phosphate Concentration and Cardiometabolic Disease: A Cohort Study on the Community-Based Older Chinese Population
Authors Lan Q, Zhang Y, Lin F, Meng Q, Buys N ![]() , Fan H, Sun J
, Fan H, Sun J ![]()
Received 22 December 2021
Accepted for publication 8 March 2022
Published 15 March 2022 Volume 2022:15 Pages 813—826
DOI https://doi.org/10.2147/DMSO.S354167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Qin Lan,1,2,* Yuming Zhang,3,* Fang Lin,1,2 Qingshu Meng,1,2 Nicholas Buys,4 Huimin Fan,1,2 Jing Sun3,4
1Shanghai East Hospital, Tongji University, Shanghai, People’s Republic of China; 2School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3School of Medicine and Dentistry, Griffith University, Gold Coast, QLD, Australia; 4Menzies Health Institute Queensland, Griffith University, Gold Coast, QLD, Australia
*These authors contributed equally to this work
Correspondence: Jing Sun, School of Medicine and Dentistry, Griffith University, Gold Coast, QLD, Australia, Tel +61756780924, Fax +61756780303, Email [email protected] Huimin Fan, Shanghai East Hospital, Tongji University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the association between sex-specific baseline serum phosphate and the incidence of new-onset cardiometabolic disease in a cohort of Shanghai-based older Chinese individuals.
Patients and Methods: A community cohort of 5000 disease-free Chinese men and women was recruited in 2013 and followed until 2017 for the development of cardiometabolic disease. Participants underwent index and follow-up health screens at the Tongji Medical School affiliated Shanghai East Hospital, including blood biochemistry analysis, anthropometric measurements, interview on health-related behaviors, and clinical evaluation.
Results: Higher baseline serum phosphate (> 1.25 mmol/L) was significantly associated with new-onset type-2 diabetes mellitus (HR 1.730, 95% CI 1.127– 2.655) and metabolic syndrome (HR 0.640, 95% CI 1.085– 2.155) in women. Baseline serum phosphate was associated with age, BMI, waist circumference, SBP, total calcium, bicarbonate, and total cholesterol in women. The estimated risk of developing diabetes mellitus in women with inorganic phosphate > 1.25 mmol/L was 14.54%. Inorganic phosphate accounted for 9.2% of the variance explained in a total estimated 14.52% of variance attributed to BMI, total cholesterol, total calcium, waist circumference, and inorganic phosphate.
Conclusion: Serum phosphate concentration showed sex-specific associations with diabetes and metabolic syndrome. Higher inorganic phosphate was associated with increased risk of developing diabetes mellitus in women. These findings may be important in the assessment of individualized metabolic risk.
Keywords: inorganic phosphate, diabetes mellitus, metabolic syndrome, older women, cohort study
Introduction
Cardiometabolic disease describes a group of non-communicable diseases, comprising of cardiovascular disease, hypertension, diabetes, metabolic syndrome and chronic kidney disease.1 The global burden of cardiometabolic disease has risen significantly in recent years, with cardiovascular disease being the main contributor of premature mortality in non-high-income countries and premature mortality due to diabetes increasing since 2010.2
China has experienced a marked increase in the prevalence of cardiometabolic disease, with the prevalence of diabetes rising from 3.7% in 1990 to 6.6% in 2016.3 According to the International Diabetes Federation (IDF), China had the largest number of adult population with diabetes in 2019, and is anticipated to remain so until 2045.4 This increase corresponded into a rise in China’s health expenditure, with the highest annual medical expenses attributed to diabetes mellitus, followed by cardiovascular disease.5 This heightens the need for effective prevention strategies acting at the risk factor level.
Serum phosphate has been widely associated with cardiometabolic disease and mortality across a number of populations.6–8 Correlations have been identified between serum phosphate and cardiometabolic risk factors, including central adiposity,9 dyslipidaemia,10 hypertension,11 and insulin sensitivity.7,12,13 Recent studies further propose that high phosphate concentration within the normal range can contribute to cardiometabolic disease through mechanisms such as endothelial thickening and vascular calcification.14,15 However, studies on the Chinese population is limited. Given that metabolic diseases such as diabetes mellitus are known to develop at lower body mass indexes in the Chinese population compared to European populations, studies on the Chinese population are required to confirm current findings from European cohorts.16 Furthermore, sex-specific differences in the association between serum phosphate and cardiometabolic disease remains under-investigated. This is important as sex hormones may alter phosphate metabolism and cardiometabolic disease development.17 Further longitudinal studies are required to bridge this gap in knowledge.
This study tried to fill in the research gap by investigating a large cohort of community-based older Chinese people from Shanghai and followed them over a period of 4 years to examine the prognostic significance of serum phosphate levels on incident cardiometabolic diseases, including heart failure, ischemic heart disease, hypertension, type-2 diabetes mellitus, metabolic syndrome, and chronic kidney disease. It is hypothesized that increased baseline phosphate will predict cardiometabolic disease development.
Materials and Methods
Study Population
The study was conducted at the Tongji Medical School affiliated Shanghai East Hospital in China, from the year 2013 to 2017. It involved a community-based cohort of older individuals from the town of Gaohang, located north-east within the Pudong district of Shanghai city, along the eastern coast of China. Permanent residents of the Gaohang community were invited to participate in the study, resulting in an initial cohort of 5000 individuals. The exclusion criteria included one or more pre-existing cardiometabolic disease at baseline, and missing or invalid data. The final cohort after 2017 included 3027 participants (1290 men and 1737 women), accounting for a retention rate of 60.5%. Those who were lost to follow-up did not show significant differences in demographic characteristics.
The study protocol was approved by the Institutional Review Board of Tongji Medical School affiliated Shanghai East Hospital. Written informed consent was obtained from all participants. All participants were informed about the purpose of the study, in accordance with the Declaration of Helsinki.
Data Collection
Participants attended the Gaohang community medical centre for an index health screen in 2013. All participants arrived in the morning following an overnight fast of at least 10 hours. Blood samples were obtained upon arrival and analyzed at the Tongji Medical School affiliated Shanghai East Hospital within 2 hours. A double-blind approach was taken by the laboratory technicians, and biochemical analyses were performed using standardized automated analyzers. Relevant reference values were determined using the Chinese Health Industry Guideline.18
Information on past medical history, demographic factors and health-related behaviors were collected by trained family doctors using a standardized questionnaire. Smoking status was categorized into non-smoker, current-smoker, or ex-smoker, and likewise with alcohol drinking. Current-smoker was defined as consuming at least one cigarette daily for at least one year. Ex-smoker was defined as previously satisfying the definition of current-smoker, but has ceased at the time of the questionnaire. Current-drinker was defined as average daily intake of at least 50g alcohol for more than a year, and the category encompassed low, moderate, and heavy drinking. Exercise status was categorized into sedentary, light-intensity exercise, and moderate-intensity exercise, defined using the Physical Exercise guideline.19
Anthropometric measurements including blood pressure, weight, height, and waist circumference were obtained. Three measurements of sitting blood pressure were taken using a mercury sphygmomanometer after 5 minutes of rest. The average of three measurements was recorded. The above procedures were repeated at the 2014 and 2017 follow-up visits.
Study Outcomes
Heart failure, ischemic heart disease and chronic kidney disease were defined using codes I50, I20-I25 and N18.2-N18.5 from the tenth edition of the International Classification of Diseases (ICD-10) and relevant hospital records. Hypertension was defined as systolic blood pressure ≥130 mmHg and/or diastolic pressure ≥80 mmHg, as per the 2017 American Heart Association Guideline.20 Diabetes mellitus was defined as fasting plasma glucose >7.0 mmol/L, based on recommendations by the Chinese Diabetes Society.21 Metabolic syndrome was defined using the revised National Cholesterol Education Program Adult Treatment panel III (NCEP ATP III) criteria, where clinical diagnosis of metabolic syndrome requires 3 of 5 constitute diagnosis of: waist circumference ≥90 cm in Asian men and ≥80 cm in Asian women; triglyceride ≥1.7 mmol/L or on medication for elevated triglycerides; HDL <1.03 mmol/L in men and <1.3 mmol/L in women or on medication for reduced HDL; systolic blood pressure ≥130 mmHg or diastolic pressure ≥85 mmHg or on antihypertensive drug; fasting glucose ≥100 mg/dL or on medication for elevated glucose.22
Statistical Analysis
Statistical analysis was performed using SPSS® 26.0 (SPSS, Chicago, IL, USA). Continuous variables were presented as mean and standard deviation, while categorical variables were presented as number and percentage.
Baseline inorganic phosphate was categorized into sex-specific quartiles to account for the effect of sex on serum phosphate. Baseline biochemical variables, including BMI, waist circumference, SBP, creatinine, total calcium, bicarbonate, fasting glucose, HbA1c, total cholesterol (TC), triglyceride (TG), and low-density lipoprotein (LDL), were compared against inorganic phosphate quartiles using the ANOVA analysis. The Kruskal–Wallis H-test was used for non-parametric variables. Demographical characteristics, including occupation, education, income, disease history, smoking status and alcohol status were compared against inorganic phosphate quartiles using the χ2 test. Variables with statistically significant difference across phosphate quartiles were included in subsequent multivariable analyses as potential confounders.
Cox proportional hazards regression analysis was used to identify the association between sex-specific inorganic phosphate quartiles and incidence of cardiometabolic disease. Significant associations will be investigated further using the machine learning analysis. Statistical significance was set at P<0.05 for all analyses.
Machine Learning Analysis
Partition analysis was performed using JMP® 16 (SAS Institute Inc., Cary, NC, USA). Recursive partitions, or splits, were performed to divide the study population into subgroups based on the optimal outcome predictors. The optimal number of splits was determined based on the Akaike’s Information Criterion score (AICs), with the smallest AICs selected. The R2, RASE, column contribution and prediction profiles were reported.
A second model was performed using the bootstrap forest method. This method combines the predictions from multiple trees together to provide an averaging model. For each outcome, 100 smaller trees were performed, with a minimum of 5 splits and maximum of 10 splits. The best decision tree was selected based on having the lowest Out-of-Bag (OOB) loss. The R2, RASE, column contribution and prediction profiles are reported. All models were performed with 20% validation.
Results
Population Characteristics
The study population at baseline consisted of 1743 (44.1%) men and 2205 (55.8%) women. Most participants were aged between 66 and 70 years (32.4%), worked as farmers (59.7%), and earned below 1500 CNY (36.4%). Only 4.6% has an education background of college or above. The prevalence of positive disease history is low. Kidney disease history was the most prevalent (6.3%) followed by liver disease (1.8%). The majority did not smoke or drink alcohol (98.7% and 98.6% respectively).
Baseline Population Demography by Inorganic Phosphate Quartile
Baseline demographical variables associated with inorganic phosphate quartiles are presented in Table 1. Participants were classified into four sex-specific quartiles using baseline inorganic phosphate concentration. For men, the lowest quartile included values below 0.91 mmol/L (n=455), the second quartile included values between 0.91 and 1.01 mmol/L (n=466), the third quartile included values between 1.01 and 1.11 mmol/L (n=425), and the highest quartile included values above 1.11 mmol/L (n=397). For women, the lowest quartile included values below 1.07 mmol/L (n=601), the second quartile included values between 1.07 and 1.16 mmol/L (n=562), the third quartile included values between 1.16 and 1.25 mmol/L (n=523), and the highest quartile included values above 1.25 mmol/L (n=519).
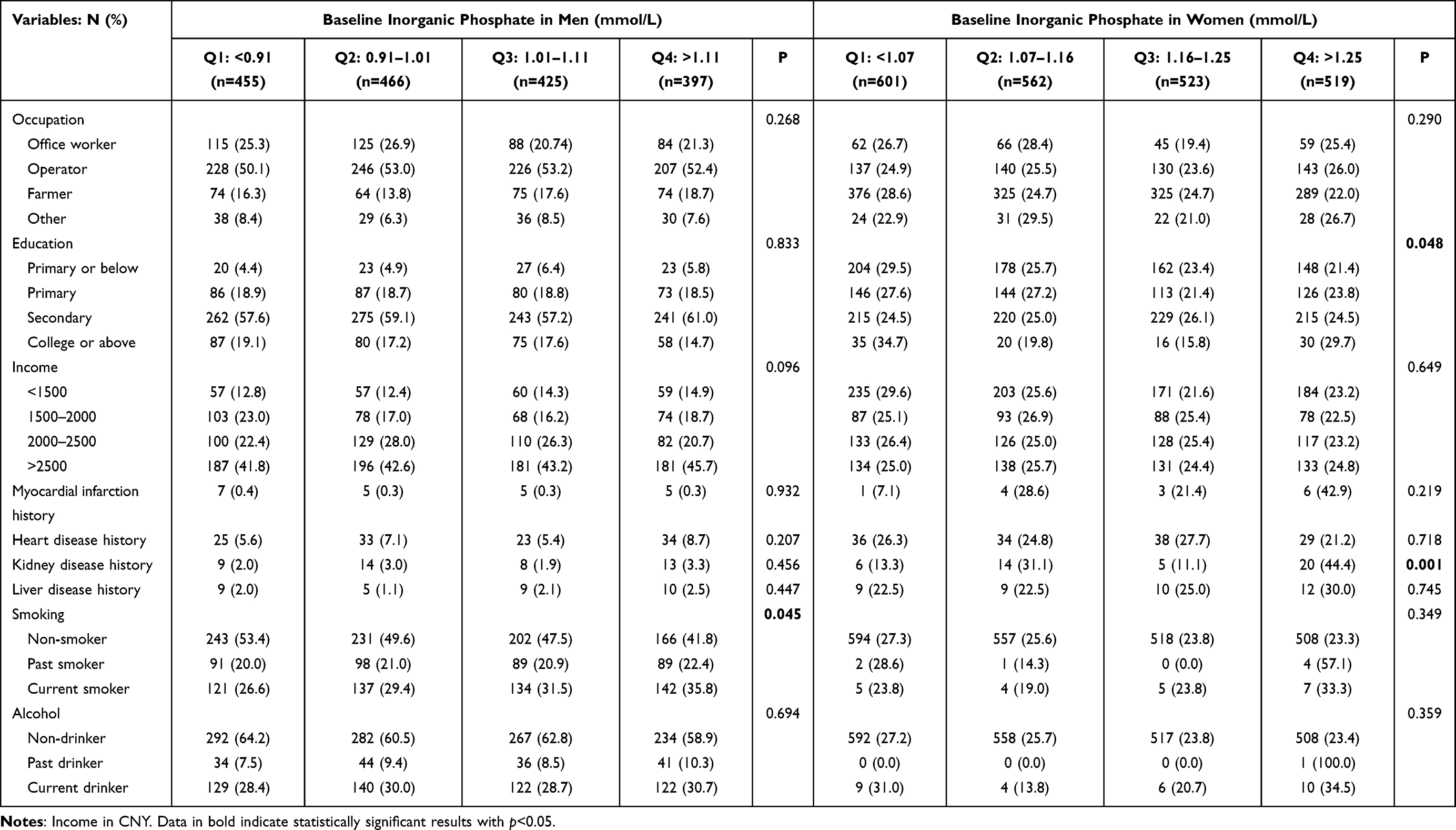 |
Table 1 Baseline Demography Based on Inorganic Phosphate Quartiles |
Among men, smoking status showed significant difference across inorganic phosphate quartiles. The highest quartile showed the greatest proportion of current smokers (35.8%).
Among women, baseline inorganic phosphate was significantly associated with education (p=0.048) and history of kidney disease (p=0.001). Educational attainment equivalent to primary or below primary education was more prevalent in participants with lower quartiles (29.5% and 25.7%) compared to higher quartiles of inorganic phosphate (23.4% and 21.4%). History of kidney disease was more prevalent in the highest quartile (44.4%). No significant difference was observed for occupation, income, other disease histories, smoking status and alcohol status.
Baseline Biochemical Profile by Inorganic Phosphate Quartile
Baseline biochemical variables associated with inorganic phosphate quartile are presented in Table 2. For men, statistically significant differences were observed in SBP (p=0.004), total calcium (p<0.001), bicarbonate (p<0.001), fasting glucose (p<0.001), HbA1c (p<0.001), and TC (p=0.032) across inorganic phosphate quartiles. Compared to men with lower phosphate quartiles, the highest quartile was associated with lower SBP (137.23±16.71mmHg), greater total calcium (2.312±0.108mmol/L), lower bicarbonate (26.375±2.937mmol/L), greater fasting glucose and HbA1c (5.927±2.059mmol/L and 6.309±1.281%), and greater total cholesterol (4.783±0.918mmol/L).
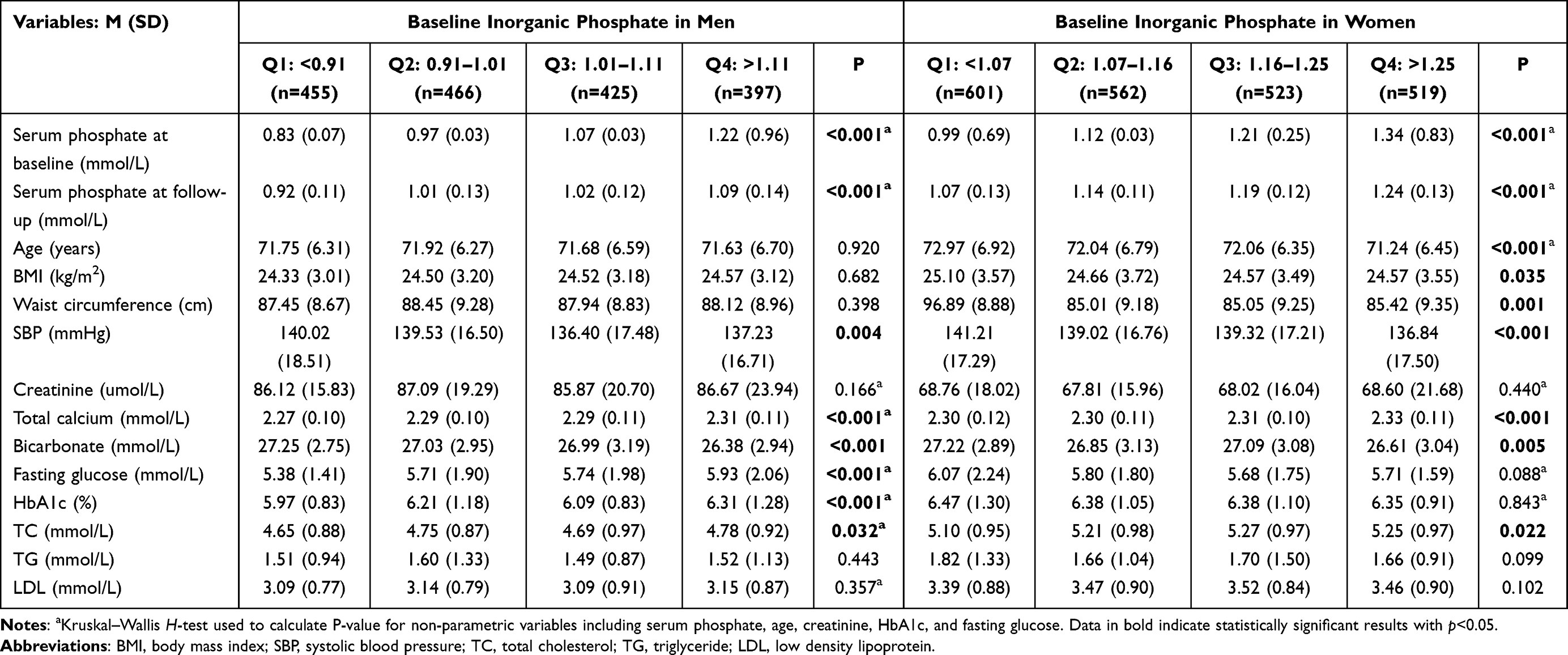 |
Table 2 Biochemical Variables Associated with Inorganic Phosphate Quartiles |
Among women, there were significant differences between inorganic phosphate quartiles and age (p<0.001), BMI (p=0.035), waist circumference (p=0.001), SBP (p<0.001), total calcium (p<0.001), bicarbonate (p=0.005), and TC (p=0.022). Compared to lower quartiles, the highest quartile of inorganic phosphate was associated with younger age (71.24±6.454 years), lower BMI (24.569±3.553kg/m2), lower SBP (136.84±17.503mmHg), higher total calcium (2.330±0.112mmol/L), lower bicarbonate (26.605±3.040mmol/L), and higher TC (5.248±0.973mmol/L). No significant associations were observed between inorganic phosphate and variables such as creatinine, fasting glucose, HbA1c, TG, and LDL (all p>0.05).
Inorganic Phosphate and Disease Incidence
During the follow-up period, 1856 of the 3027 subjects developed at least one cardiometabolic outcome (61.3%). In total, there were 811 cases of incident heart failure (25.8%), 371 cases ischemic heart disease (11.6%), 609 cases of hypertension (19.2%), 233 cases of diabetes mellitus (7.3%), 389 cases of metabolic syndrome (12.4%), and 384 cases of chronic kidney disease (12.2%).
Adjusted hazard ratios with 95% confidence interval are shown in Table 3. For both sexes, the lower quartiles (≤1.20 mmol/L) were used as the reference group. The model was adjusted for SBP, total calcium, bicarbonate, fasting glucose, HbA1c, TC and smoking status in men, and age, BMI, waist circumference, SBP, total calcium, bicarbonate, TC, education and kidney disease history in women.
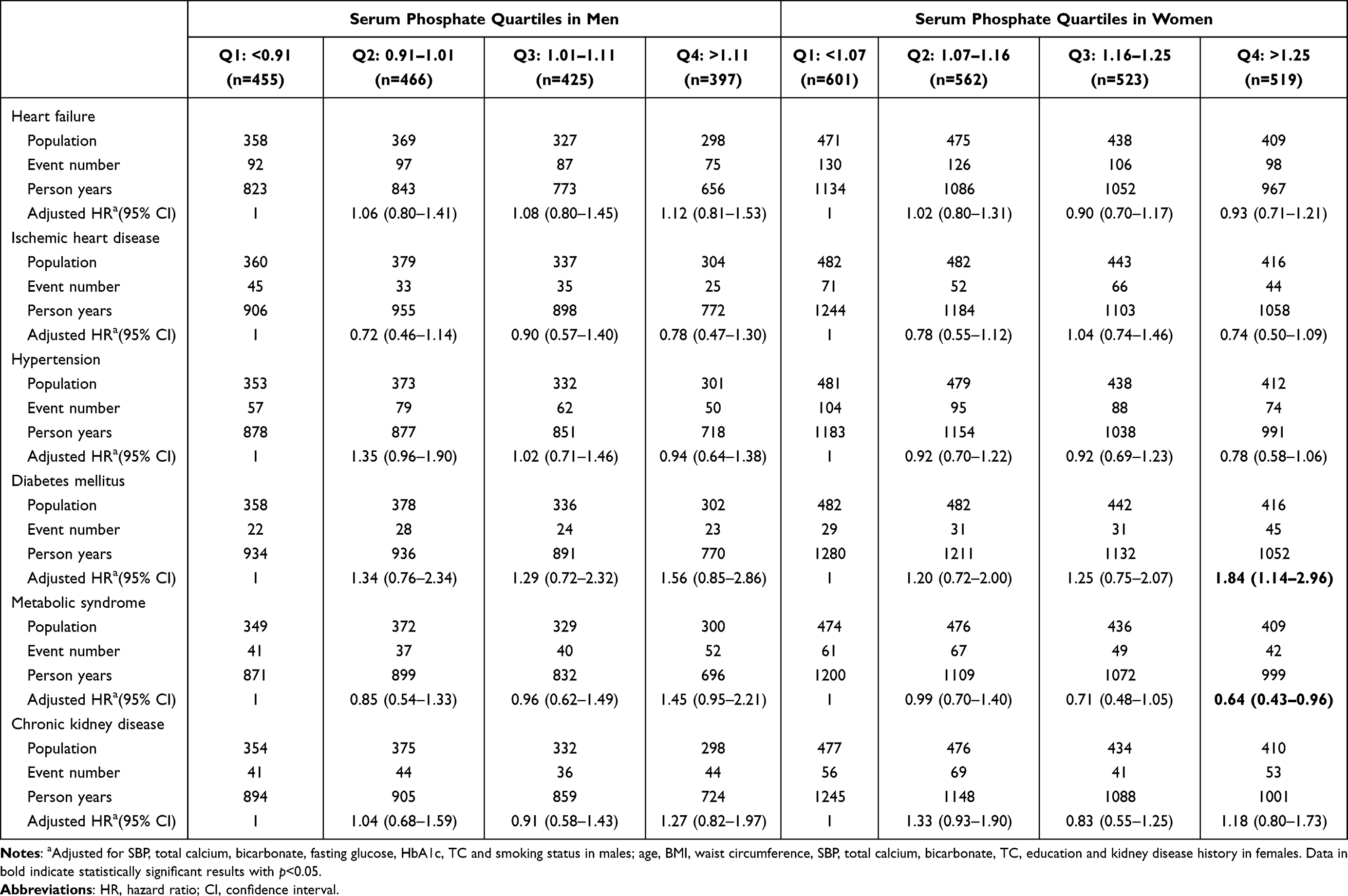 |
Table 3 Risk of Cardiometabolic Diseases by Baseline Phosphate Quartiles in Men and Women |
When compared using phosphate quartiles, there was a statistically significant difference in the incidence of diabetes mellitus and metabolic syndrome among women (p=0.013 and p=0.030 respectively). Women with serum phosphate greater than 1.25 mmol/L were 1.835 times more likely to develop diabetes mellitus compared to women with levels less than 1.07 mmol/L (95% CI 1.139–2.957). The risk of developing metabolic syndrome is 0.360 times lower in women with the highest level of inorganic phosphate compared to the lowest quartile (95% CI 0.428–0.957).
For men, higher phosphate quartiles were associated with increased risk of developing diabetes and metabolic syndrome. Compared to men in the lowest phosphate quartile, men with phosphate greater than 1.11 mmol/L were 1.453 times more likely to develop metabolic syndrome (95% CI 0.954–2.213). Similarly, the risk of developing metabolic syndrome was 1.561 times greater in the highest quartile (95% CI 0.853–2.856). However, these associations were marginal (p=0.082 and p=0.149).
Machine Learning Analysis
Partition analysis and bootstrap forest analysis were performed for diabetes mellitus and metabolic syndrome development in women. Confounding variables identified in the bivariate analysis are included in the models. Fasting glucose was removed for diabetes mellitus as it was part of the diagnostic criteria. Similarly, waist circumference, SBP, HbA1c, TC and TG were not included as they define metabolic syndrome.
For diabetes mellitus, the bootstrap forest model explained 12.2% of the variance observed in disease outcome with an estimated error of 0.248, compared to the partition model which explained 6.5% with a higher estimated error of 0.264. For metabolic syndrome, the bootstrap forest model accounted for 16.2% of the observed variance with an estimated error of 0.309, whereas the partition model explained 9.5% of the disease outcome with an estimated error of 0.321. Therefore, the bootstrap forest model was chosen for both outcomes.
The best decision tree for predicting the 4-year probability of developing diabetes mellitus was selected using the smallest out-of-bag (OOB) loss. It used seven variables (inorganic phosphate, waist circumference, bicarbonate, BMI, TC, education status, and total calcium) to perform 19 splits. The overall probability of developing diabetes mellitus in all female participants was 7.96%. The highest quartile of inorganic phosphate (>1.25mmol/L) was identified as the most significant predictor, with a 4-year risk of 14.54%.
For metabolic syndrome, the overall probability of developing metabolic syndrome in all female participants was 14.8%. A total of 19 splits were performed using BMI, total calcium, bicarbonate, kidney disease history, age, occupation, inorganic phosphate, education, and alcohol use as predictors. The most significant predictor of metabolic syndrome was BMI.
Table 4 shows the decision rules and subgroups, or terminal nodes, identified by the decision tree. High inorganic phosphate (>1.25mmol/L) was the most significant predictor of 4-year diabetes mellitus development. In females with high inorganic phosphate (>1.25mmol/L), bicarbonate was the next predictor. The probabilities of developing diabetes mellitus in females with high inorganic phosphate who has bicarbonate ≥24.1mmol/L and <24.1mmol/L were 12.6% and 24.1% respectively. Among females with lower quartiles of inorganic phosphate, those with waist circumference greater than 86cm, and TC <3.14mmol/L had the highest probability of developing diabetes mellitus (50.0%).
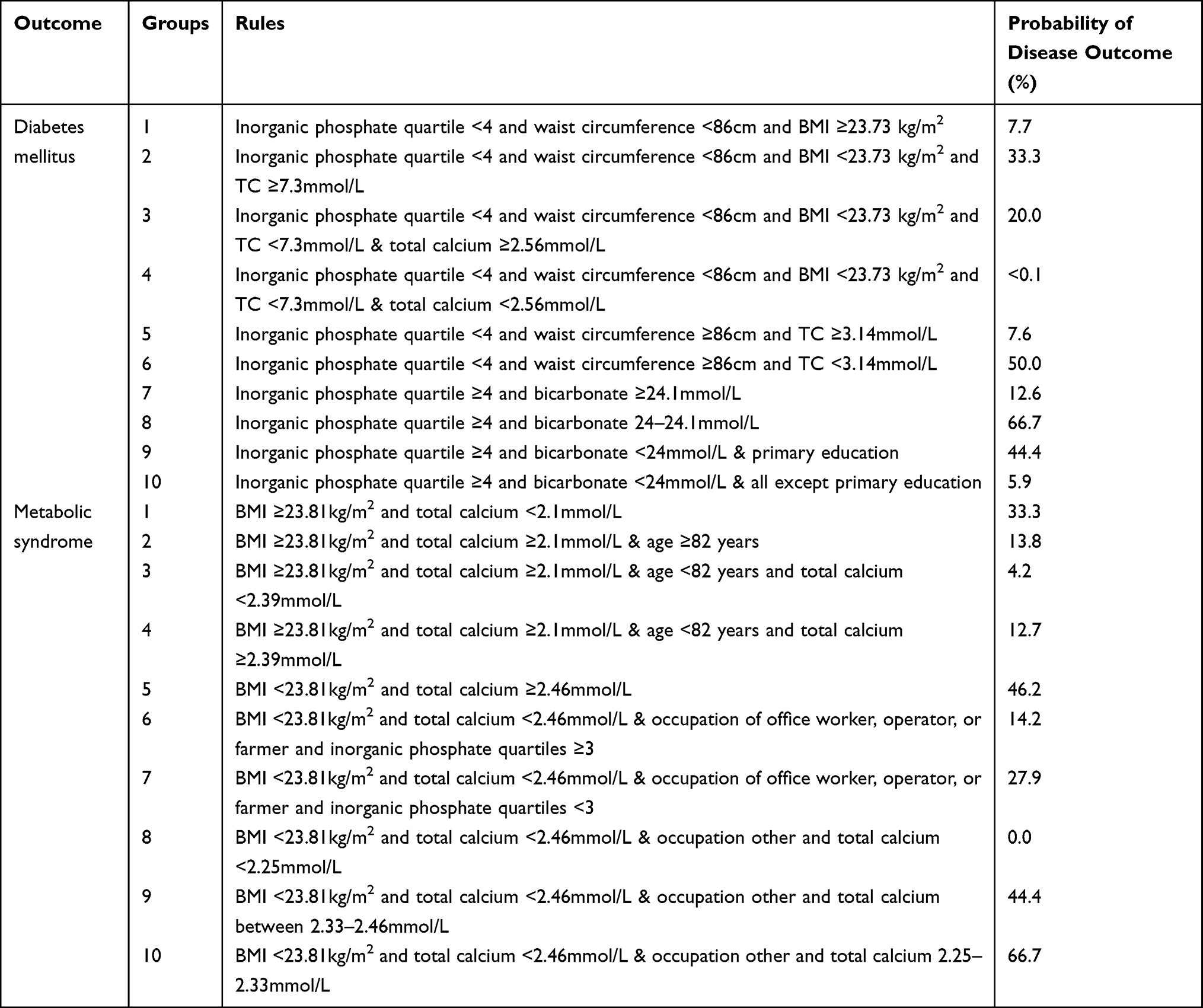 |
Table 4 Rules Identified by Decision Tree to Determine Metabolic Disease Outcomes |
For metabolic syndrome, the greatest risk was associated with having a BMI <23.81kg/m2 (24.6%). The next best predictor was total calcium. The highest risk was estimated in females with BMI <23.81kg/m2, other occupations, and total calcium 2.25–2.33mmol/L (66.7%).
As shown in Table 5, inorganic phosphate quartiles contributed 9.2% to the variance explained for diabetes mellitus. BMI was the greatest predictor, accounting for 24.0%, followed by TC (19.9%), total calcium (11.3%), waist circumference (10.1%), bicarbonate (8.5%), education (7.1%), and SBP (6.9%). Age and history of kidney disease contributed negligible amounts to the 4-year risk of developing diabetes mellitus (2.2% and 0.7% respectively).
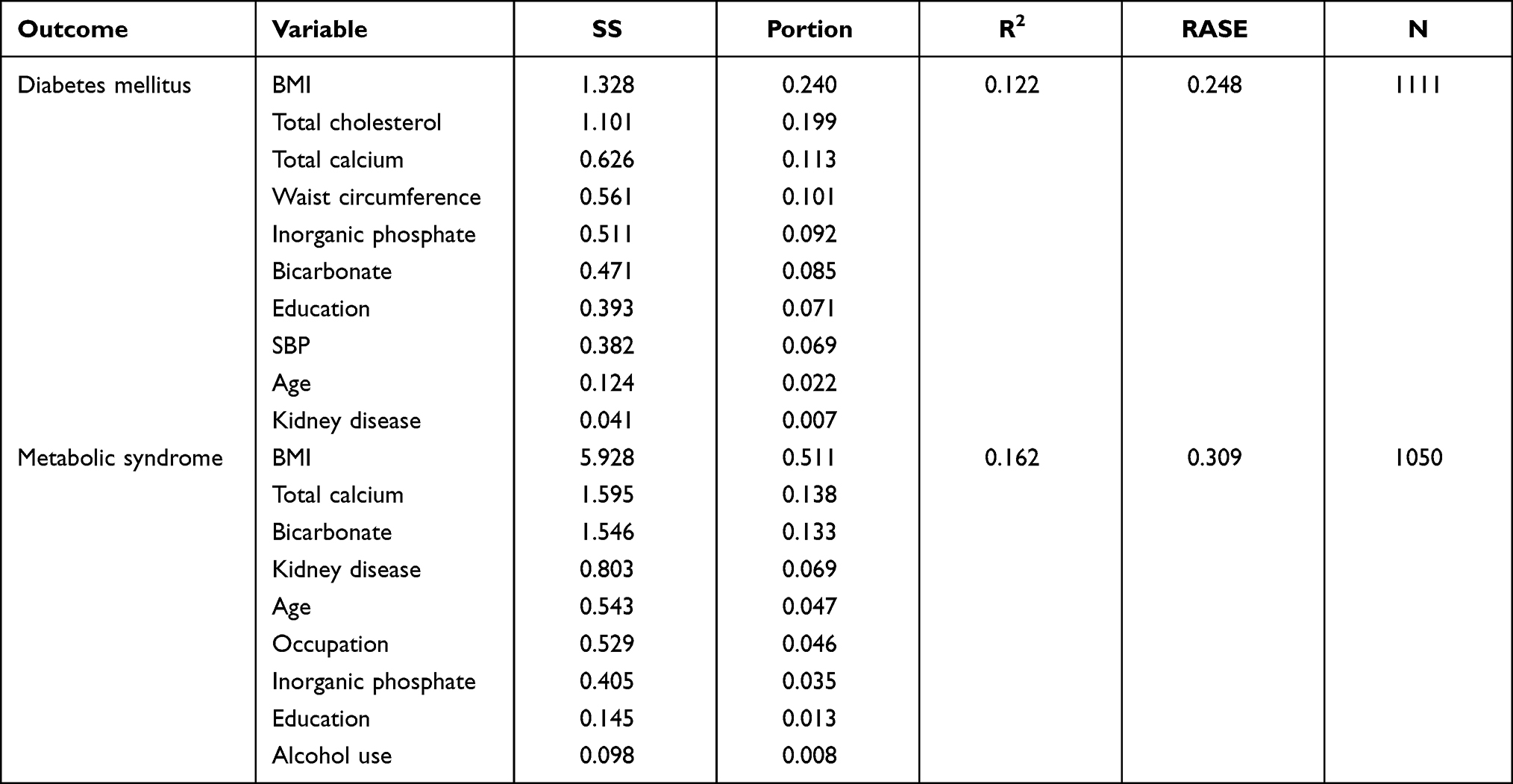 |
Table 5 Variable Contributions for the Development Metabolic Disease Outcomes |
Inorganic phosphate quartile was not a significant contributor to the development of metabolic syndrome (3.5%). BMI was again the most significant contributor, accounting for 51.1% of the variance explained by the model. The second greatest contributor total calcium (13.8%) and bicarbonate (13.3%), followed by kidney disease history (6.9%). Age (4.7%), occupation (4.6%) did not contribute significantly. Lastly, education and alcohol use had negligible effects on the risks of developing metabolic syndrome (1.3% and 0.8% respectively).
Discussion
Diabetes Mellitus
The present study demonstrates the importance of inorganic phosphate in the development of type-2 diabetes mellitus among a population of older Chinese women. Serum phosphate greater than 1.25 mmol/L showed an estimated risk of 14.54%, compared to 5.88% observed in lower quartiles. This finding is contrary to previous studies which identified lower serum phosphate in subjects with type-2 diabetes mellitus compared to non-diabetic subjects.23 Similarly, lower, rather than higher, serum phosphate has been associated with impaired glucose tolerance and insulin sensitivity.7,12,24,25
However, similar findings have been reported in some population studies. The IRAS (Insulin Resistance Atherosclerosis Study) investigated African-American, Hispanic, and non-Hispanic individuals, with serum phosphate concentration greater than 1.20 mmol/L associated with 2.24 times greater risk of developing diabetes compared to individuals with serum phosphate lower than 1.00 mmol/L, independent of glucose tolerance and insulin parameters.26 Similarly, high serum phosphate was associated with increased risk of diabetes mellitus in a population of Taiwanese individuals aged over 60 years (HR 1.49, 95% CI 1.15–1.92).27 Such heterogeneity may suggest ethnic- or culture-specific associations. Alternatively, as our cohort consisted of older post-menopausal women, it is possible that increased serum phosphate observed at baseline was reflective of bone health rather than glucose metabolism.
Several mechanisms have been proposed for the interaction between serum phosphate and diabetes development. One mechanism is the involvement of phosphate in regulating energy balance and oxygen consumption.28 Phosphate is heavily implicated in both gluconeogenesis and glycolysis through its role in the phosphorylation of carbohydrate intermediates.12 Haglin et al hypothesized that higher serum phosphate may be associated with depletion of intracellular phosphate.10 Depletion of intracellular phosphate may lead to a lack of substrate for phosphorylation, which inhibits the peripheral utilization of glucose and subsequently results in impaired insulin secretion and glucose tolerance.29,30 Studies of phosphate metabolism in diabetic patients have also suggested that higher oxygen consumption was associated with lower concentrations of inorganic phosphate.31
Another mechanism is the positive effects of serum phosphate on insulin secretion and sensitivity. Hypophosphatemia, not hyperphosphatemia, has been associated with impaired insulin sensitivity in both hyperglycemic and euglycemic states.7 This is hypothesized to be due to insulin’s capacity to stimulate intracellular phosphate uptake via insulin-dependent transporters and phosphorylation of metabolic intermediates, which exacerbates hypophosphatemia and results in further hyperinsulinaemia.8
Lastly, changes in serum phosphate reflects impaired renal reabsorption. Higher serum phosphate has been associated with increased HOMA-IR in non-diabetic participants with impaired renal function.32 Hyperphosphatemia has also been noted in diabetes, especially in the context of diabetic nephropathy.33 Therefore, poor renal function may have a mediating effect between phosphate retention and insulin resistance. However, although this study found a significant association between higher serum phosphate and existing kidney disease in women (p<0.001), serum phosphate was not associated with kidney disease development (p=0.411), nor was baseline kidney disease a significant contributor to diabetes (p=0.526). These findings suggest serum phosphate may increase the risk of type-2 diabetes mellitus through an unclear mechanism that is independent of kidney disease.
Metabolic Syndrome
Although inorganic phosphate above 1.25 mmol/L was significantly associated with lower risks of metabolic syndrome development in the multiple regression model (HR 0.640, 95% CI 0.428–0.957), it had a negligible contribution in the bootstrap model (3.5%). BMI was the greatest contributor (51.1%), which may be explained by its close relation to waist circumference, a diagnostic criterion of metabolic syndrome. Overall, this finding supports previous cohort studies, which identified significant associations between inorganic phosphate and metabolic diseases. Jhuang et al identified a positive association between serum phosphate at baseline and development of metabolic syndrome in those aged above 60 years (HR 1.39, 95% CI 1.11–1.74).27 They reported no significant association in those aged below 60, likely due to lower baseline serum phosphate compared to those aged over 60, which is consistent with the findings of this study. However, the sex-specific differences identified in our cohort was not reported. A cross-sectional study performed by Shimodaira et al on the older Japanese population identified contrary sex-specific differences.24 Among 16,041 participants (9076 men and 6965 women), low serum phosphate was associated with metabolic syndrome in men, whereas high serum phosphate was associated with metabolic syndrome in women.24 In a cohort of middle-aged British men, lower rather than higher baseline serum phosphate was associated with increased components of metabolic syndrome.8 The mechanism behind this disparity remains unclear. However, the effect of age cannot be excluded, as our study cohort had a mean age of around 70 years at follow-up, while the latter two studies included participants aged around 50 and 60 years respectively.8,24 Moreover, ethnicity and cultural differences may have contributed, as the development of metabolic syndrome varies due to gene-environmental interactions.34 Overall, our results suggest that low serum phosphate is significantly associated with risk of metabolic syndrome in older Chinese women.
Low phosphate has been linked to obesity. Obeid argued that reduction in intracellular phosphate availability causes low thermogenesis secondary to reduced ATP production.35 Thermogenesis has been shown to affect weight control, with low thermogenesis associated with greater predisposition to gain weight.36 This is possibly due to the effects of low thermogenesis on hunger and appetite.37 In support of this hypothesis, a randomized controlled trial has demonstrated that phosphorous supplementation reduces body weight, BMI and waist circumference, as well as subjective appetite.38
Furthermore, low serum phosphate may be an indicator of poor diet. Stoian et al suggested that altered phosphate levels may result from changes in intestinal absorption and internal redistribution.39 Diets high in carbohydrate and low in protein provide limited dietary phosphate. Low protein and high carbohydrate diets have been associated with three-times greater odds of metabolic syndrome in elderly women, as well as increased central adiposity and dyslipidaemia.40 Furthermore, serum phosphate can predict blood pressure elevations. A possible mechanism is its role in promoting sympathoadrenal activity through increasing plasma adrenaline.8 Higher serum phosphate has been shown to contribute towards vascular and soft-tissue calcification,14 which increases arterial wall stiffness and predisposes to hypertension and cardiovascular disease.41 However, the mechanism behind significantly lower blood pressure observed in the women of this study remains unclear.
Sex-Specific Association Between Inorganic Phosphate and Biochemical Risk Factors
In women, high serum phosphate was associated with age, BMI, waist circumference, SBP, total calcium, bicarbonate, and total cholesterol. This was largely consistent with previous studies, which reported significant associations between high serum phosphate and lower systolic blood pressure, lower waist circumference.9,15,42,43 The associations with lower triglyceride and fasting blood glucose were not significant in our study population. A possible explanation is variation in the distribution of serum phosphate measurements, which resulted in different cut-off values. For example, Park et al used 5.0 mg/dL to define high serum phosphate,42 which was considerably higher than the values used by this study. Age differences may also have contributed to this, as previous studies were conducted on younger cohorts aged around 40 years. A recent study by Yoo et al suggested that serum phosphate in women increases until age 60 and decreases thereafter.44 This could have accounted for the lower serum phosphate and subsequent lack of association seen in our cohort. The decrease in serum phosphate after age 60 may also explain why our results showed an inverse association with age, contrary to previous studies conducted on younger women.15,44
In men, high serum phosphate at baseline was positively associated with systolic blood pressure, total calcium, bicarbonate, fasting glucose, HbA1c, and total cholesterol. Elevated blood glucose and cholesterol are established risk factors for cardiometabolic disease.45,46 Previous studies have reported similar sex-specific differences in lipid profiles, where serum phosphate was positively correlated with total cholesterol and increased cholesterol-to-HDL ratio.47 While this study supported previous associations between phosphate in men and altered lipid profiles, the association with greater glucose and HbA1c was contradictory to previous studies. Cohort studies conducted on older Japanese,24 Dutch,44 and New Zealand9 men have observed lower fasting glucose with higher serum phosphate. Differences in baseline characteristics such as age may have contributed to this disparity, as older age has been linked to progressively worse plasma glucose control.48 Fat mass has also been suggested to mediate the relationship between serum phosphate and glucose.9 As our cohort consisted of leaner rather than obese men by BMI, this may have contributed to the contradictory findings. Lastly, the possibility of this association being unique to Chinese men cannot be ruled out.
Strengths and Limitations
Our study expanded on current understandings of serum phosphate and metabolic disease by investigating a population with limited previous insight. Furthermore, we investigated sex-specific differences within this population, which has not been previously reported in the Chinese population. Second, although dietary information was recorded, it did not specify the amount of protein intake. Thus, we could not analyze whether dietary phosphate intake impacted on the findings. Third, although conventional confounding factors were identified and included in the multivariate analysis, some factors such as FGF23 and activated vitamin D were not included in the study. Future study involving large number of participants and long-term follow up will be conducted to confirm the study findings.
Conclusion
In conclusion, baseline serum phosphate greater than 1.25 mmol/L was significantly associated with increased risk of type-2 diabetes mellitus, and decreased risk of metabolic syndrome in older Chinese women. The 4-year risk of developing diabetes mellitus in women with the highest phosphate quartile was 14.54%, with inorganic phosphate contributing to 9.2% of the variance explained by the model. Our results suggest the presence of sex-specific associations between serum phosphate and diabetes mellitus, possibly explained by the difference in risk factor profile. This finding may be important due to its potential prognostic value in assessing metabolic risk among disease-free older individuals. However, further longitudinal studies are required to validate the observed associations.
Funding
This work was supported by National Nature Science Foundation of China (81670458, 81470393, and 81370434), Shanghai Three year plan on promoting TCM development (ZY(2018-2020)-FWTX-2007), Key Discipline of the Health Industry Project of Pudong Health Bureau of Shanghai (PWZxk2017-01), Three year plan of Pudong Health Bureau of Shanghai (PWYgf2018-05), Three-year plan on TCM of Pudong Health Bureau of Shanghai (PDZY-2018-0603), The National Key Research and Development Program of China (2017YFA0105600), The Science and Technology Commission of Shanghai Municipality(17431906600),The Health Industry Project of Pudong Health Bureau of Shanghai (no. PW2013E-1).
Disclosure
Qin Lan and Yuming Zhang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Ndisang JF, Rastogi S. Cardiometabolic diseases and related complications: current status and future perspective. Biomed Res Int. 2013;2013:467682. doi:10.1155/2013/467682
2. World Health Organisation. World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals. World Health Organisation; 2020.
3. Liu M, Liu S-W, Wang L-J, et al. Burden of diabetes, hyperglycaemia in China from to 2016: findings from the 1990 to 2016, global burden of disease study. Diabetes Metab. 2019;45(3):286–293. doi:10.1016/j.diabet.2018.08.008
4. International Diabetes Federation. IDF Diabetes Atlas.
5. Mao W, Yip C-MW, Chen W. Complications of diabetes in China: health system and economic implications. BMC Public Health. 2019;19:269. doi:10.1186/s12889-019-6569-8
6. Levy J, Stern Z, Gutman A, Naparstek Y, Avioli LV, Avioli LV. Plasma calcium and phosphate levels in an adult noninsulin-dependent diabetic population. Calcif Tissue Int. 1986;39:316–318. doi:10.1007/BF02555197
7. DeFronzo RA, Lang R. Hypophosphatemia and glucose intolerance: evidence for tissue insensitivity to insulin. N Eng J Med. 1980;303(22):1259–1263. doi:10.1056/NEJM198011273032203
8. Gudmundsdottir H, Strand AH, Kjeldsen SE, Høieggen A, Os I. Serum phosphate, blood pressure, and the metabolic syndrome—20‐year follow‐up of middle‐aged men. J Clin Hypertens. 2008;10(11):814–821. doi:10.1111/j.1751-7176.2008.00032.x
9. Billington EO, Gamble GD, Bristow S, Reid IR. Serum phosphate is related to adiposity in healthy adults. Eur J Clin Invest. 2017;47(7):486–493. doi:10.1111/eci.12769
10. Håglin LM, Törnkvist B, Bäckman LO. High serum phosphate and triglyceride levels in smoking women and men with CVD risk and type 2 diabetes. Diabetol Metab Syndr. 2014;6:39. doi:10.1186/1758-5996-6-39
11. Huang CX, Plantinga LC, Fink NE, Melamed ML, Coresh J, Powe NR. Phosphate levels and blood pressure in incident hemodialysis patients: a longitudinal study. Adv Chronic Kidney Dis. 2008;15(3):321–331. doi:10.1053/j.ackd.2008.04.012
12. Haap M, Heller E, Thamer C, Tschritter O, Stefan N, Fritsche A. Association of serum phosphate levels with glucose tolerance, insulin sensitivity and insulin secretion in non-diabetic subjects. Eur J Clin Nutr. 2006;60:734–739. doi:10.1038/sj.ejcn.1602375
13. Nowicki M, Fliser D, Fode P, Ritz E. Changes in plasma phosphate levels influence insulin sensitivity under euglycemic conditions. J Clin Endocrinol Metab. 1996;81:156–159. doi:10.1210/jcem.81.1.8550745
14. Park KS, Park J, Choi SH, et al. Serum phosphorus concentration and coronary artery calcification in subjects without renal dysfunction. PLoS One. 2016;11(3):e0151007. doi:10.1371/journal.pone.0151007
15. Onufrak SJ, Bellasi A, Cardarelli F, et al. Investigation of gender heterogeneity in the associations of serum phosphorus with incident coronary artery disease and all-cause mortality. Am J Epidemiol. 2009;169(1):67–77. doi:10.1093/aje/kwn285
16. Hu C, Jia W. Diabetes in China: epidemiology and genetic risk factors and their clinical utility in personalized medication. Diabetes. 2018;67(1):3–11. doi:10.2337/dbi17-0013
17. Gerdts E, Regitz-Zagrosek V. Sex differences in cardiometabolic disorders. Nat Med. 2019;25:1657–1666. doi:10.1038/s41591-019-0643-8
18. Ministry of Health PRC. Reference Intervals for Common Clinical Biochemistry Tests. Vol WS/T 404. National Health and Family Planning Commission PRC; 2015.
19. US Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans.
20. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Hypertension. 2017;71:e13–e115. doi:10.1161/HYP.0000000000000065
21. Chinese Diabetes Society. Guidelines for prevention and treatment of type 2 diabetes in China. Chin J Diabetes. 2018;10(1):4–67.
22. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
23. Fang L, Li X. [Level of serum phosphorus and adult type 2 diabetes mellitus]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2016;41(5):502–506. Chinese. doi:10.11817/j.issn.1672-7347.2016.05.009
24. Shimodaira M, Okaniwa S, Nakayama T. Reduced serum phosphorus levels were associated with metabolic syndrome in men but not in women: a cross-sectional study among the Japanese population. Ann Nutr Metab. 2017;71:150–156. doi:10.1159/000480354
25. Akter S, Eguchi M, Kochi T, Kabe I, Nanri A, Mizoue T. Association of serum calcium and phosphate concentrations with glucose metabolism markers: the Furukawa Nutrition and Health Study. Nutrients. 2020;12(8):2344. doi:10.3390/nu12082344
26. Lorenzo C, Hanley AJ, Rewers MJ, Haffner SM. Calcium and phosphate concentrations and future development of type 2 diabetes: the Insulin Resistance Atherosclerosis Study. Diabetologia. 2014;57(7):1366–1374. doi:10.1007/s00125-014-3241-9
27. Jhuang YH, Kao TW, Peng TC, Chen WL, Chang PK, Wu LW. Serum phosphorus as a risk factor of metabolic syndrome in the elderly in Taiwan: a Large-Population Cohort Study. Nutrients. 2019;11(10):2340. doi:10.3390/nu11102340
28. Johnson MA, Tekkanat K, Schmaltz SP, Fox IH. Adenosine triphosphate turnover in humans. Decreased degradation during relative hyperphosphatemia. J Clin Invest. 1989;84(3):990–995. doi:10.1172/JCI114263
29. Khattab M, Abi-Rashed C, Ghattas H, Hlais S, Obeid O. Phosphorus ingestion improves oral glucose tolerance of healthy male subjects: a crossover experiment. Nutr J. 2015;14:112. doi:10.1186/s12937-015-0101-5
30. Paula FJ, Plens AE, Foss MC. Effects of hypophosphatemia on glucose tolerance and insulin secretion. Horm Metab Res. 1998;30(5):281–284. doi:10.1055/s-2007-978884
31. Ditzel J, Lervang -H-H. Disturbance of inorganic phosphate metabolism in diabetes mellitus: its impact on the development of diabetic late complications. Curr Diabetes Rev. 2010;6(5):323–333. doi:10.2174/157339910793360833
32. Raikou VD, Kyriaki D, Gavriil S. Importance of serum phosphate in elderly patients with diabetes mellitus. World J Diabetes. 2020;11(10):416–424. doi:10.4239/wjd.v11.i10.416
33. van der Vaart A, Yeung S, van Dijk P, Bakker S, de Borst M. Phosphate and fibroblast growth factor 23 in diabetes. Clin Sci (Lond). 2021;135(14):1669–1687. doi:10.1042/CS20201290
34. Rakugi H, Ogihara T. The metabolic syndrome in the Asian population. Curr Hypertens Rep. 2005;7:103–109. doi:10.1007/s11906-005-0082-4
35. Obeid OA. Low phosphorus status might contribute to the onset of obesity. Obes Rev. 2013;14(8):659–664. doi:10.1111/obr.12039
36. Tremblay A, Royer -M-M, Chaput J-P, Doucet É. Adaptive thermogenesis can make a difference in the ability of obese individuals to lose body weight. Int J Obes (Lond). 2012;37:759–764. doi:10.1038/ijo.2012.124
37. Jung RT, Shetty PS, James WPT, Barrand MA, Callingham BA. Reduced thermogenesis in obesity. Nature. 1979;279:322–323. doi:10.1038/279322a0
38. Ayoub JJ, Samra MJA, Hlais SA, Bassil MS, Obeid OA. Effect of phosphorus supplementation on weight gain and waist circumference of overweight/obese adults: a randomized clinical trial. Nutr Diabetes. 2015;5:e189. doi:10.1038/nutd.2015.38
39. Stoian M, Stoica V. The role of disturbances of phosphate metabolism in metabolic syndrome. Maedica (Bucur). 2014;9(3):255–260.
40. Nabuco HCG, Tomeleri CM, Junior PS, et al. Lower protein and higher carbohydrate intake are related with altering metabolic syndrome components in elderly women: a cross-sectional study. Exp Gerontol. 2018;103:132–137. doi:10.1016/j.exger.2018.01.013
41. Ix JH, De Boer IH, Peralta CA. Serum phosphorus concentrations and arterial stiffness among individuals with normal kidney function to moderate kidney disease in Mesa. Clin J Am Soc Nephrol. 2009;4(3):609–615. doi:10.2215/CJN.04100808
42. Park W, Kim BS, Lee JE, et al. Serum phosphate levels and the risk of cardiovascular disease and metabolic syndrome: a double-edged sword. Diabetes Res Clin Pract. 2009;83(1):119–125. doi:10.1016/j.diabres.2008.08.018
43. Haglin L, Lindblad A, Bygren L. Original communication hypophosphataemia in the metabolic syndrome. Gender differences in body weight and blood glucose. Eur J Clin Nutr. 2001;55:493–498. doi:10.1038/sj.ejcn.1601209
44. Yoo KD, Kang S, Choi Y, et al. Sex, age, and the association of serum phosphorus with all-cause mortality in adults with normal kidney function. Am J Kidney Dis. 2015;67(1):79–88. doi:10.1053/j.ajkd.2015.06.027
45. Castelli WP. Epidemiology of coronary heart disease: the Framingham study. Am J Med. 1984;76(2):4–12. doi:10.1016/0002-9343(84)90952-5
46. Sigdel M, Kumar A, Gyawali P, Shrestha R, Tuladhar ET, Jha B. Association of high sensitivity C-reactive protein with the components of metabolic syndrome in diabetic and non-diabetic individuals. J Clin Diagn Res. 2014;8(6):11–13. doi:10.7860/JCDR/2014/8085.4522
47. Campos-Obando N, Lahousse L, Brusselle G, et al. Serum phosphate levels are related to all-cause, cardiovascular and COPD mortality in men. Eur J Epidemiol. 2018;33(9):859–871. doi:10.1007/s10654-018-0407-7
48. Ko GT, Wai HP, Tang JS. Effects of age on plasma glucose levels in non-diabetic Hong Hong Chinese. Croat Med J. 2006;47(5):709–713.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.