Back to Journals » Clinical Interventions in Aging » Volume 14
Sex-related differences in homebound advanced Parkinson’s disease patients
Authors Nwabuobi L ![]() , Barbosa W, Sweeney M, Oyler S
, Barbosa W, Sweeney M, Oyler S ![]() , Meisel T, Di Rocco A, Chodosh J, Fleisher JE
, Meisel T, Di Rocco A, Chodosh J, Fleisher JE ![]()
Received 1 February 2019
Accepted for publication 22 May 2019
Published 31 July 2019 Volume 2019:14 Pages 1371—1377
DOI https://doi.org/10.2147/CIA.S203690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Lynda Nwabuobi,1 William Barbosa,2 Meghan Sweeney,3 Sarah Oyler,4 Talia Meisel,5 Alessandro Di Rocco,6 Joshua Chodosh,7,8 Jori E Fleisher9
1Department of Neurology, Movement Disorders Division, Columbia University Medical Center, New York, NY, USA; 2New York University School of Medicine, New York, NY, USA; 3Department of Palliative Care, Kaiser Permanente, Lafayette, CO, USA; 4Intermountain Neurosciences Institute, Intermountain Medical Center, Murray, UT, USA; 5State University of New York Downstate Medical Center College of Medicine, Brooklyn, NY, USA; 6Department of Neurology, Movement Disorders Division, Northwell Health, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Long Island, NY, USA; 7Division of Geriatric Medicine and Palliative Care, New York University Langone Health, New York, NY, USA; 8Veterans Affairs NY Harbor Healthcare System, NY, New York, USA; 9Section of Movement Disorders, Department of Neurological Sciences, Rush Medical College, Rush University, Chicago, IL, USA
Background: Women with Parkinson’s disease (PD) are more likely to be older, have greater disease severity and comorbidities, and yet are less likely to receive care from a neurologist, as compared with men with PD. Within the PD population, homebound individuals are a particularly vulnerable group facing significant barriers to care, yet within this understudied population, sex-related differences have not been reported.
Purpose: To identify and describe differences in homebound men and women with advanced PD and related disorders, participating in an interdisciplinary home visit program.
Patients and methods: This was an exploratory analysis of homebound patients seen between February 2014 and July 2016 using data collected via in-person interviews and chart review.
Results: We enrolled 85 patients, of whom 52% were women. PD was the most common diagnosis (79%), followed by dementia with Lewy bodies (5%), and other atypical parkinsonism (16%). Men were more likely to have a PD dementia diagnosis than women (17.1% vs 2.3%, p=0.03). Women were more likely to live alone (18.1% of women had no caregiver vs 2.4% of men, p=0.05).
Conclusion: The role of the caregiver in facilitating safe aging-in-place is crucial. Among homebound individuals with advanced PD, women were far more likely to live alone. The absence of a spouse or care partner may be due in part to variable sex-based life expectancies. Our findings suggest that homebound women with advanced PD may face greater barriers to accessing support.
Keywords: parkinsonism, gender disparities, caregiver, aging, health services, health disparities
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disorder characterized by both motor and nonmotor symptoms due to loss of dopaminergic neurons in the substantia nigra pars compacta. PD onset is likely from a complicated interplay between genetics and the environment.1 The prevalence of PD increases with age, rising from 41 cases per 100,000 at age 40–49 years to 1903 per 100,000 over age 80 years.2 As patients reach advanced stages of PD, gait, balance, and cognition are most notably affected and complications from dopaminergic therapy may become the focus of treatment.3,4 The combination of advanced PD, older age, and its associated accumulation of comorbidities are negatively reinforcing, rendering many people homebound. Once homebound and disconnected from routine care, this population is at further risk of deterioration and adverse events.
Sex-related differences have been documented in several domains of PD, including clinical features, response to levodopa, non-motor symptoms, and quality of life, among others.5–9 Women are more likely to be older and have greater disease severity and more comorbidities than men despite similar PD duration.10 Women are less likely to be treated by a neurologist or receive surgical interventions like deep brain stimulation in the United States, despite evidence demonstrating the benefits of specialized care and interventions.9,11–13 A recent multicenter international cohort study of patients with PD also showed that women are at higher risk of poor access to caregivers.14 Given these findings of health-related disparities in women with PD in the outpatient setting, we hypothesized that homebound women with PD would be particularly vulnerable to poor care. To understand the interaction between homebound status, sex, and access to care, we conducted an exploratory analysis of baseline characteristics among homebound men and women enrolled in a home visit program (HVP) for individuals with advanced PD and related disorders.
Methods
Participants/setting
We recruited patients with advanced PD and related disorders into the Edmond J. Safra Interdisciplinary Home Visit Program for Advanced Parkinson’s Disease (HVP), which consisted of a movement disorders-trained neurologist, nurse, and social worker evaluating the patient at home every 4 months. We included patients if they had a diagnosis of PD or a related disorder provided by a referring movement disorders specialist, met Medicare homebound criteria, and lived within the five boroughs of New York City.15 Additionally, to be included, participants had to have one or more of the following risk factors for hospitalization or institutionalization: motor fluctuations, multi-morbidity, medication mismanagement, depression, anxiety, frequent hospitalizations, suspected elder abuse, caregiver burnout, or increased falls at home. Further details on the structure and processes of the HVP have been described elsewhere.16
Standard protocol approvals, registrations, and patient consents
The Institutional Review Board of New York University Langone Health approved this study.
Data collection
We conducted a retrospective, exploratory analysis of patients enrolled in the HVP from its inception in February 2014 to July 2016, including data collected via in-person interviews at the time of each initial home visit, and subsequent chart review. We de-identified and maintained all data in an electronic database – REDCap (Research Electronic Data Capture), a secure, web-based application designed to support data capture for research studies.17 We collected information on demographics, social factors, and clinical utilization. The Unified Parkinson’s Disease Rating Scale (UPDRS) and Hoehn & Yahr (H&Y) scores were documented based on examination by a movement disorders specialist during the visit.
Statistical analysis
We exported data to STATA 14 for analysis and used Chi-square and Fischer’s exact test to analyze differences between categorical variables. We used two-sample t-tests to analyze differences between continuous variables. Statistical significance was based on a two-tailed alpha of <0.05. Given the exploratory nature of the analysis, no corrections were made for multiple comparisons.
Results
Demographics
We enrolled 85 patients in the study. Patients received a median of three visits (range 1–7). Women comprised 52% of patients, as shown in Table 1. At visit 1, the median age of the group was 79.6 (range 43.3–93.9, standard deviation 8.7), with no significant sex-related differences (female 79.4 years, male 77.2 years, p=0.25). In terms of self-identified race, 7% each identified as African-American and Asian, respectively, and 15% identified as Hispanic. More women identified as Hispanic compared to men (22.7% vs 7.3%, p=0.07). Of the 49 individuals disclosing their educational attainment, 78% had a college degree or higher, with no significant difference between the sexes (p=0.99).
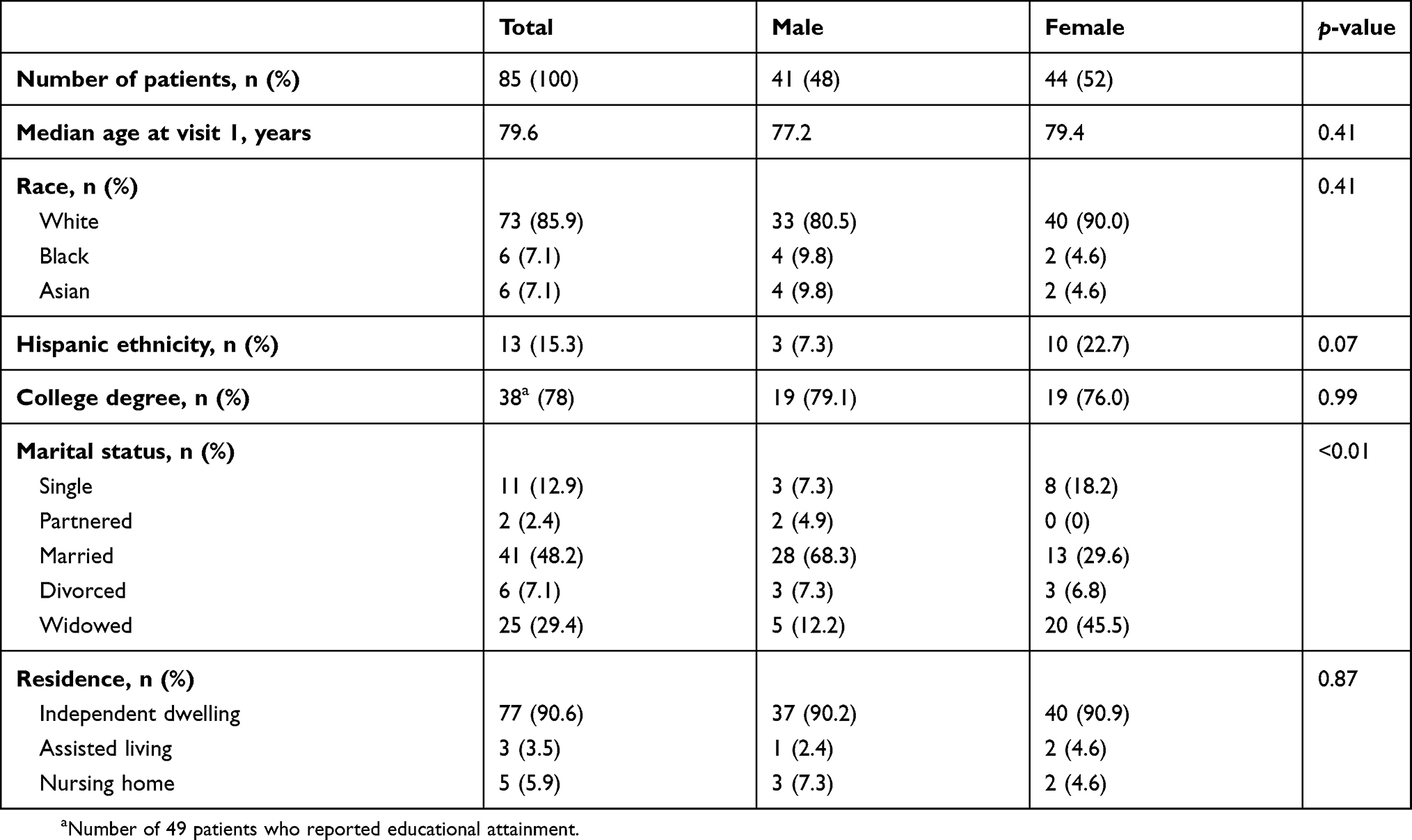 |
Table 1 Baseline demographics of homebound advanced PD patients |
Clinical characteristics
PD was the most common diagnosis among all the patients (79%), followed by dementia with Lewy bodies and progressive supranuclear palsy accounting for 5% each, multiple system atrophy2%, and other atypical parkinsonism 9% (Table 2). Men were more likely to have a PD dementia diagnosis than women (17.1% vs 2.3%, p=0.02). Among the patients with PD, men had a significantly higher mean total UPDRS score compared to women (85.6 vs 71.2, p<0.01). Baseline mean UPDRS-III (motor) score was 46.8 (SD 14.7). Men had more severe motor scores than women (49.9 vs 43.7, p=0.06). There was no significant sex-related difference in the Hoehn & Yahr (H&Y) stage (mean: men 4.1, women 3.9, p=0.22).
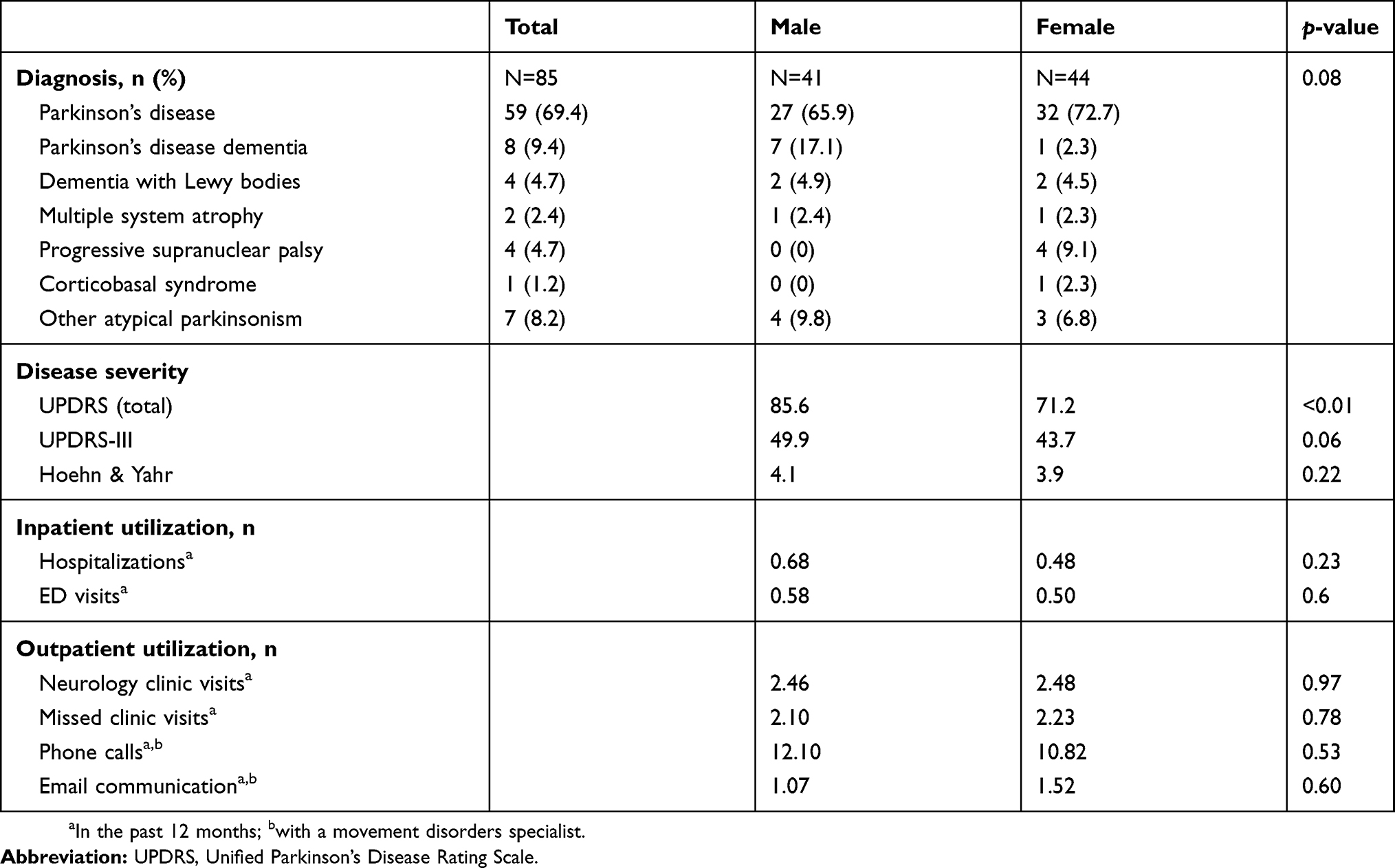 |
Table 2 Baseline clinical characteristics of homebound advanced PD patients |
Regarding access to health care, there were no significant sex-related differences in the number of hospitalizations or emergency department visits in the 12 months prior to the initial home visit (t-test, p=0.23, p=0.68, respectively). Similarly, we found no differences in outpatient utilization, specifically the number of attended outpatient neurology visits (p=0.97), missed visits (p=0.78), phone calls to the movement disorders specialist (t-test, p=0.53), or emails to the movement disorders specialist (p=0.60).
Social impact
We found significant sex-related differences in marital status, with a significantly higher proportion of women being widowed (45.5% vs 12.2%) or single (18.2% vs 7.3%) compared to men (p<0.01 for both) (Figure 1). Men were 2.3 times more likely to be married (68.3% vs 29.6%). As shown in Table 3, compared to men, women were less likely to have any caregiver present (18.1% of the women were alone vs 2.4% of the men, p<0.01). Comparing caregiver types, 70.7% of men identified a spouse, partner, or significant other serving as a caregiver compared to only 27.3% of women (p<0.01). There was no significant difference among those who identified an adult child (p=0.08), other family members (p=1.00), or a neighbor/friend (p=1.00) as their primary caregivers. Many subjects endorsed having home health aides (HHAs), with 48.2% having a part-time HHA and 21.2% having a full-time HHA, without statistically significant sex-related differences (p=0.10, p=0.43, respectively). Most visits were conducted in the home of the patient (90.6%) as opposed to an assisted living or skilled nursing facility (Table 1), and there were no sex-related differences in place of residence (p=0.87).
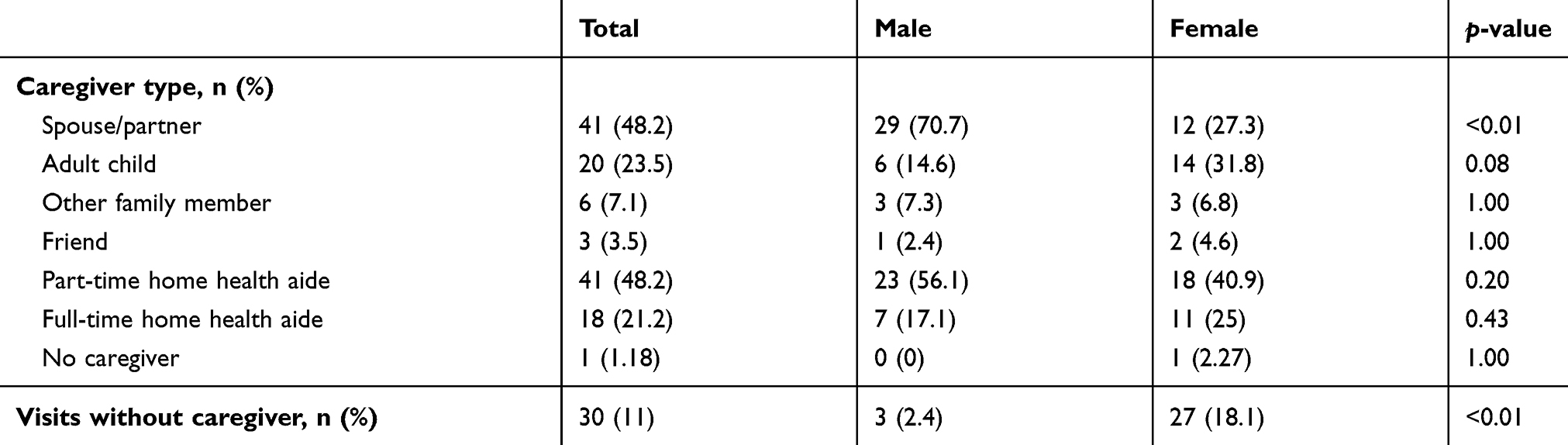 |
Table 3 Caregiver types and presence at visits |
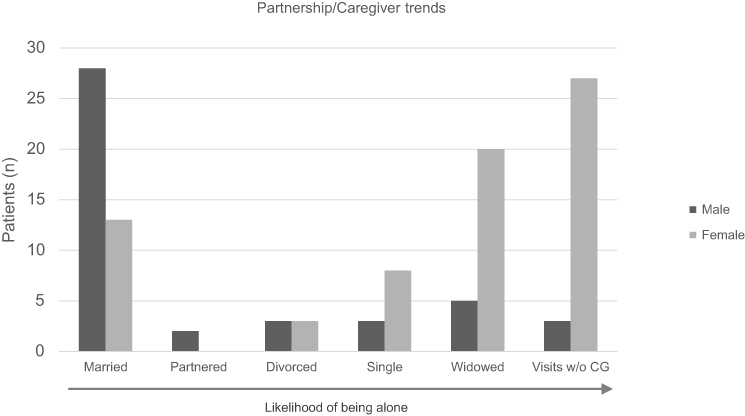 |
Figure 1 Partnerships and caregiver trends in homebound advanced PD patients. Abbreviations: CG, caregiver; PD, Parkinson’s disease. |
Discussion
To our knowledge, ours is the first study to specifically explore the sex-related differences beyond disease progression in a homebound PD population. Despite the higher prevalence of PD in men in most studies conducted in outpatient settings, women comprised more than half of this homebound advanced PD group (44 women vs 41 men), and were more likely to be single or widowed, and to lack any caregiver.18
In the early phase of PD, women exhibit a milder disease phenotype and present at an older age compared to men. This may be possibly due to neuroprotective effects of estrogen.5,19,20 However, once the disease fully manifests, this slight advantage seen in women is no longer apparent.5 The longer life expectancy for women in the general population may explain the shift in distribution to an increasing prevalence of homebound women with advanced PD. As the disease progresses, women may be at increased risk for homebound status and hence, dependence on a caregiver and/or facility placement compared to men.
This study showed that while a spouse or partner is the most likely individual to serve as a caregiver, homebound women were more likely to be single or widowed compared to men. They were also more likely to lack any caregiver. Hariz et al showed a similar finding in a group of PD patients who underwent pallidotomy, thalamotomy, or deep brain stimulation in which women were more likely to be living without a spouse (50% women vs 20% men).21 Dahodwala et al reported that women have fewer informal caregivers and were more likely to use formal caregivers compared to men, despite greater strain reported by caregivers of men with PD.14 Similarly, Fullard et al found that women used HHAs and skilled nursing facilities more than men and also had less outpatient physician contact compared to men.22 This suggests that women with advanced PD who are homebound are an especially vulnerable group due to a relative lack of caregivers/partners, and are therefore at risk of loss to follow up. Once neurologic follow-up is lost, these women may be at increased risk of hospitalizations, nursing facility placement, and poorer quality of life.11,23 A growing body of literature reports that women with PD are more likely to be institutionalized compared to men, possibly due to disparities in caregiver presence and type, or greater psychological distress, and institutionalization is associated with increased mortality.22,24–28 This further highlights the importance of caregivers in preventing premature institutionalization and excess mortality in women with PD.
Men in this cohort had greater disease severity as evidenced by the higher mean total UPDRS score, and a higher rate of PD dementia. This is comparable to findings in other studies even after adjustment for age and disease duration.21,23,24,29–31 One explanation is that the equivalently impaired women either have been institutionalized or died rather than remain in the community, due to a lack of caregivers. These impairments also likely facilitate greater use of caregivers in men. Women historically play the role of caregiver, may have better symptom coping skills, and may not seek potentially helpful care. Lubomski et al demonstrated that women with PD are more likely to believe that they did not require support from an appointed caregiver.29 Education on the risks of poor continuity of care and the need to advocate for assistance may be an important intervention.
Identifying patients at risk for homebound status creates an opportunity for clinicians to intervene, tailoring treatment strategies toward transition to said homebound status. The increased risk of homebound status among women and among individuals with severe disease should be discussed with these patients in advance so that they can identify and mobilize friends, family, and community resources for support in the future.
A limitation of this study is that findings are from a convenience sample in New York and are not necessarily generalizable. Some of the observed differences or lack thereof could be attributable to access to the HVP itself. This study also focused primarily on the social impact of PD in the homebound patient and did not capture other measures that may contribute to sex-related differences in this population (eg, levodopa equivalent dose, disease duration, nonmotor symptoms, etc.). Future population-based studies that capture a larger sample of patients outside of an HVP setting will be useful to further evaluate and understand the observed sex differences and improve generalizability. A larger, ongoing adaptation of the HVP outside of New York, with matched controls, will start to answer these questions.
Conclusion
This study highlights the relative lack of caregivers among homebound women with advanced PD and emphasizes the vulnerability of this group of patients to interruptions in continuity of care. With additional understanding of barriers to care, clinicians can further individualize treatment strategies, counseling, and care planning based on these sex-related differences. Health systems opportunities to support individuals with PD are essential to improving care.
Acknowledgments
This work was supported by the Edmond J. Safra Philanthropic Foundation, the National Parkinson Foundation, the Parkinson Alliance, the Doris Duke Fund to Retain Clinical Scientists, the Feldstein Medical Foundation; and the National Institutes of Health (2L30NS084235-02, 2L30NS084235-03, 2L30NS084235-04, and 1K23NS097615.). None of the funding sources were involved in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work. Lynda Nwabuobi contributed to concept, analysis and interpretation of data, literature search, drafting, and revision of the manuscript. William Barbosa, Meghan Sweeney, Sarah Oyler, alia Meisel contributed to data acquisition, revision, and critique of the manuscript. Alessandro Di Rocco and Joshua Chodosh contributed to conception and design of study, revision, and critique of the manuscript. Jori E Fleisher contributed to conception and design of study, project organization, data acquisition, statistical analysis and interpretation of data, revision, and critique of the manuscript.
Disclosure
Dr Di Rocco has received grant support from the Parkinson Alliance, Parkinson Foundation, and Edmond J. Safra Philanthropic Foundation.
Dr Chodosh has received research support from the National Institutes of Health, New York State Department of Health, and Independence at Home, Long Beach, CA, USA; has received honoraria from Gerontological Society of America; serves on the advisory board of Aging in New York Fund; and has no personal conflicts to disclose.
Dr Fleisher has received research support from the Feldstein Medical Foundation, Doris Duke Charitable Foundation Fund to Retain Clinical Scientists, National Institutes of Health/National Institute of Neurological Disorders and Stroke, CurePSP, and Biogen. She has received honoraria from Parkinson’s Foundation and royalties from UpToDate.
The other authors report no conflicts of interest in this work.
References
1. Kalia LV, Lang AE. Parkinson’s disease. Lancet. 2015;386(9996):896–912. doi:10.1016/S0140-6736(14)61393-3
2. Pringsheim T, Jette N, Frolkis A, Steeves TD. The prevalence of Parkinson’s disease: a systematic review and meta-analysis. Mov Disord. 2014;29(13):1583–1590. doi:10.1002/mds.25945
3. Fahn S, Jankovic J, Hallett M. Principles and Practice of Movement Disorders.
4. Coelho M, Ferreira JJ. Late-stage Parkinson disease. Nat Rev Neurol. 2012;8(8):435–442. doi:10.1038/nrneurol.2012.126
5. Haaxma CA, Bloem BR, Borm GF, et al. Gender differences in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2007;78(8):819–824. doi:10.1136/jnnp.2006.103788
6. Kumagai T, Nagayama H, Ota T, Nishiyama Y, Mishina M, Ueda M. Sex differences in the pharmacokinetics of levodopa in elderly patients with Parkinson disease. Clin Neuropharmacol. 2014;37(6):173–176. doi:10.1097/WNF.0000000000000051
7. Martinez-Martin P, Pecurariu CG, Odin P, et al. Gender-related differences in the burden of non-motor symptoms in Parkinson’s disease. J Neurol. 2012;259(8):1639–1647. doi:10.1007/s00415-011-6392-3
8. Nicoletti A, Vasta R, Mostile G, et al. Gender effect on non-motor symptoms in Parkinson’s disease: are men more at risk? Parkinsonism Relat Disord. 2017;35:69–74. doi:10.1016/j.parkreldis.2016.12.008
9. Pavon JM, Whitson HE, Okun MS. Parkinson’s disease in women: a call for improved clinical studies and for comparative effectiveness research. Maturitas. 2010;65(4):352–358. doi:10.1016/j.maturitas.2010.01.001
10. Dahodwala N, Pei Q, Schmidt P. Sex differences in the clinical progression of Parkinson’s disease. J Obstet Gynecol Neonatal Nurs. 2016;45(5):749–756. doi:10.1016/j.jogn.2016.05.002
11. Willis AW, Schootman M, Evanoff BA, Perlmutter JS, Racette BA. Neurologist care in Parkinson disease: a utilization, outcomes, and survival study. Neurology. 2011;77(9):851–857. doi:10.1212/WNL.0b013e31822c9123
12. Willis AW, Schootman M, Kung N, Wang XY, Perlmutter JS, Racette BA. Disparities in deep brain stimulation surgery among insured elders with Parkinson disease. Neurology. 2014;82(2):163–171. doi:10.1212/WNL.0000000000000017
13. Willis AW, Schootman M, Tran R, et al. Neurologist-associated reduction in PD-related hospitalizations and health care expenditures. Neurology. 2012;79(17):1774–1780. doi:10.1212/WNL.0b013e3182703f92
14. Dahodwala N, Shah K, He Y, et al. Sex disparities in access to caregiving in Parkinson disease. Neurology. 2018;90(1):e48–e54. doi:10.1212/WNL.0000000000004764
15. Department of Health and Human Services. Pub 100-02 Medicare Benefit Policy: clarification of the confined to the home definition in Chapter 15, Covered Medical and Other Health Services, of the Medicare Benefit Policy Manual. In: Department of Health & Human Services (DHHS) CfMMSC. 2019. Vol. Transmittal 192, Change Request 88182014.
16. Fleisher JE, Barbosa W, Sweeney MM, et al. Interdisciplinary home visits for individuals with advanced Parkinson’s disease and related disorders. J Am Geriatr Soc. 2018;66(6):1226–1232. doi:10.1111/jgs.15337
17. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
18. Wooten GF, Currie LJ, Bovbjerg VE, Lee JK, Patrie J. Are men at greater risk for Parkinson’s disease than women? J Neurol Neurosurg Psychiatry. 2004;75(4):637–639. doi:10.1136/jnnp.2003.020982
19. Gillies GE, McArthur S. Independent influences of sex steroids of systemic and central origin in a rat model of Parkinson’s disease: a contribution to sex-specific neuroprotection by estrogens. Horm Behav. 2010;57(1):23–34. doi:10.1016/j.yhbeh.2009.06.002
20. Ragonese P, D’Amelio M, Salemi G, et al. Risk of Parkinson disease in women: effect of reproductive characteristics. Neurology. 2004;62(11):2010–2014. doi:10.1212/wnl.62.11.2010
21. Hariz GM, Lindberg M, Hariz MI, Bergenheim AT. Gender differences in disability and health-related quality of life in patients with Parkinson’s disease treated with stereotactic surgery. Acta Neurol Scand. 2003;108(1):28–37.
22. Fullard ME, Thibault DP, Todaro V, et al. Sex disparities in health and health care utilization after Parkinson diagnosis: rethinking PD associated disability. Parkinsonism Relat Disord. 2018;48:45–50. doi:10.1016/j.parkreldis.2017.12.012
23. Calder SA, Ebmeier KP, Stewart L, Crawford JR, Besson JAO. The prediction of stress in carers: the role of behavior, reported self care and dementia in patients with idiopathic Parkinson’s disease. Int J Geriatr Psychiatry. 1991;6(10):737–742. doi:10.1002/gps.930061008
24. Carrozzino D, Morberg BM, Siri C, Pezzoli G, Bech P. Evaluating psychiatric symptoms in Parkinson’s disease by a clinimetric analysis of the Hopkins symptom checklist (SCL-90-R). Prog Neuropsychopharmacol Biol Psychiatry. 2018;81:131–137. doi:10.1016/j.pnpbp.2017.10.024
25. Anang JB, Gagnon JF, Bertrand JA, et al. Predictors of dementia in Parkinson disease: a prospective cohort study. Neurology. 2014;83(14):1253–1260. doi:10.1212/WNL.0000000000000842
26. Safarpour D, Thibault DP, DeSanto CL, et al. Nursing home and end-of-life care in Parkinson disease. Neurology. 2015;85(5):413–419. doi:10.1212/WNL.0000000000001715
27. Nihtila EK, Martikainen PT, Koskinen SV, Reunanen AR, Noro AM, Hakkinen UT. Chronic conditions and the risk of long-term institutionalization among older people. Eur J Public Health. 2008;18(1):77–84. doi:10.1093/eurpub/ckm025
28. Ibrahim JE, Bugeja L, Willoughby M, et al. Premature deaths of nursing home residents: an epidemiological analysis. Med J Aust. 2017;206(10):442–447.
29. Lubomski M, Louise RR, Lee W, Bertram KL, Williams DR. Sex differences in Parkinson’s disease. J Clin Neurosci. 2014;21(9):1503–1506. doi:10.1016/j.jocn.2013.12.016
30. Lyons KE, Hubble JP, Tröster AI, Pahwa R, Koller WC. Gender differences in Parkinson’s disease. Clin Neuropharmacol. 1998;21(2):118–121.
31. Shulman LM. Gender differences in Parkinson’s disease. Gend Med. 2007;4(1):8–18.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.