Back to Journals » International Journal of General Medicine » Volume 17
Severe Vitamin D Deficiency is Associated with Mortality Risk in Critically Ill Patients with Acute Kidney Injury
Authors Shen B, Liu B, Wang Y, Wang R, Gu D
Received 7 July 2024
Accepted for publication 8 October 2024
Published 9 November 2024 Volume 2024:17 Pages 5153—5162
DOI https://doi.org/10.2147/IJGM.S477114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor David E. Stec
Beili Shen, Bianling Liu, Yanhui Wang, Rui Wang, Dongfeng Gu
The Fifth Clinical Medical College of Henan University of Chinese Medicine (Zhengzhou People’s Hospital), Zhengzhou, Henan, 450003, People’s Republic of China
Correspondence: Dongfeng Gu, Department of Nephrology, The Fifth Clinical Medical College of Henan University of Chinese Medicine (Zhengzhou People’s Hospital), No. 33 Huanghe Road, Zhengzhou, Henan, 450003, People’s Republic of China, Tel +86-371-67077643, Email [email protected]
Purpose: Deficiency in vitamin D is associated with adverse outcomes in several health conditions. However, the specific impact of vitamin D levels on mortality in acute kidney injury (AKI) patients remains inadequately explored. This study aims to investigate the association between serum vitamin D concentrations and mortality risk in critically ill patients diagnosed with AKI. We hypothesize that severe vitamin D deficiency is associated with an increased risk of 90-day all-cause mortality in these patients.
Patients and Methods: This study retrospectively enrolled 259 adult AKI patients admitted to the intensive care unit (ICU) at The Fifth Clinical Medical College of Henan University of Chinese Medicine (Zhengzhou People’s Hospital) between July 2021 and June 2023. Based on 25-hydroxyvitamin D (25-OHD) levels, they were categorized into 4 groups: severe deficiency (< 10 ng/mL), deficiency (10– 20 ng/mL), insufficiency (20– 30 ng/mL), and sufficiency (> 30 ng/mL). Multivariate survival analysis using Cox’s regression model was used to analyze the impact of vitamin D concentrations on the 90-day all-cause mortality risk after controlling for potential confounders.
Results: The 90-day all-cause mortality rate was the highest in patients with severe deficiency (50.8%), followed by those with deficiency (35.0%), insufficiency (23.9%), and sufficiency (12.2%). Multivariate Cox regression showed that compared with sufficiency, severe deficiency (HR=3.34, 95% CI: 1.14– 9.77; P=0.03) was independently associated with a higher risk of 90-day all-cause mortality, but deficiency and insufficiency were not significantly associated with 90-day all-cause mortality risk.
Conclusion: Severe vitamin D deficiency (< 10 ng/mL) significantly increases the risk of mortality in AKI patients, underlining the need for monitoring and potentially supplementing vitamin D in this population.
Keywords: acute kidney injury, vitamin D deficiency, mortality, prognosis
Introduction
Acute kidney injury (AKI) encompasses a diverse range of conditions characterized by a sudden decline in glomerular filtration rate (GFR), an increase in serum creatinine concentration (SCC), or reduced urine output (oliguria).1 This condition affects over 50% of critically ill patients worldwide, leading to higher mortality rates, longer hospital stays, and a greater risk of long-term complications.2–5 Moreover, AKI survivors are particularly vulnerable to progressive kidney function decline and the onset of end-stage renal disease.6–8 Therefore, identifying risk factors for mortality among AKI patients is essential for improving their outcomes.
Vitamin D is widely recognized for its role in calcium and phosphate metabolism, but its effects extend far beyond bone health.9 In AKI, the kidneys’ diminished capacity to produce calcitriol exacerbates the detrimental consequences of vitamin D deficiency.10,11 Vitamin D receptors are present in renal tissues, indicating its direct influence on kidney function. Several mechanisms link vitamin D deficiency to the development of AKI, including the upregulation of the renin–angiotensin–aldosterone system, increased renal vascular renin expression, and immune system dysregulation. This deficiency may worsen renal vascular health, hinder recovery from renal ischemia-reperfusion injury (IRI), and accelerate the progression from AKI to chronic kidney disease (CKD).12
Vitamin D deficiency affects more than 20% of the population and has emerged as a serious public health concern.13 Among critically ill patients, the prevalence of vitamin D deficiency is even higher, with studies showing that 40%–70% of these patients have insufficient vitamin D levels.14 Furthermore, Cameron et al reported that serum 1.25(OH)2D levels were significantly lower in critically ill patients with AKI than those than those without AKI (54 vs 41 pmol/L), significantly contributing to worse clinical outcomes.15 Evidence suggests that critically ill patients with vitamin D deficiency are more likely to develop AKI and require renal replacement therapy (RRT) compared to those with adequate vitamin D levels.10,16,17 Despite these findings, the relationship between vitamin D status and mortality in AKI patients remains underexplored.18
This research aims to assess the association of serum vitamin D concentrations with 90-day all-cause mortality among critically ill patients with AKI. The 90-day period was selected as it captures both immediate and delayed effects of AKI and is a commonly used timeframe in similar research,19,20 facilitating consistent comparisons.
Materials and Methods
Patients
This research involved a retrospective analysis of all adult patients (≥18 years) diagnosed with AKI in our ICU from July 2021 to June 2023. We used the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines for AKI diagnosis, which define AKI based on an increase in serum creatinine by ≥0.3 mg/dL within 48 hours or an increase to ≥1.5 times baseline within the prior 7 days, or urine output <0.5 mL/kg/h for 6 hours.21 Exclusion criteria included pregnant women, and individuals with conditions such as malabsorption, hyperparathyroidism, hyperthyroidism, chronic renal failure, or granulomatous disorders. Patients undergoing antiepileptic or antiretroviral treatment, those taking vitamin D supplements, or medications affecting bone metabolism (eg, bisphosphonates) were also excluded from the study.
The Ethical Committee of The Fifth Clinical Medical College of Henan University of Chinese Medicine (Zhengzhou People’s Hospital) (approval number: 2023016) reviewed and approved this study. All procedures involving human subjects adhered to the 1964 Declaration of Helsinki and its subsequent amendments or equivalent ethical standards. Given the retrospective nature of the study, informed consent was waived by the Ethical Committee of The Fifth Clinical Medical College of Henan University of Chinese Medicine (Zhengzhou People’s Hospital). All data were stored securely, and confidentiality was maintained throughout the study.
Data Collection
Patient data were collected from electronic medical records. A standardized medical record abstraction form was developed to systematically collect patients’ baseline characteristics within 24 hours of ICU admission, including demographic data (age, gender, body mass index [BMI]), reasons for admittance to the ICU, comorbidities, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, Sequential Organ Failure Assessment (SOFA) scores, KDIGO stage, and laboratory results such as 25-hydroxyvitamin D (25-OHD), serum calcium, albumin, creatinine, and parathyroid hormone (PTH) levels. Medical charts were reviewed by two individual researchers, and discrepancies between researchers were adjudicated by means of consensus. All collected data were anonymized to maintain patient confidentiality.
The 25-OHD levels were quantified using the radioimmunoassay kit (Liaison; DiaSorin, Shanghai, China). Patients were categorized into four groups based on the Endocrine Society guidelines for vitamin D levels: severe deficiency (<10 ng/mL), deficiency (10–20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (>30 ng/mL).22
The primary outcome measured was 90-day all-cause mortality. Survival outcomes were obtained from medical records or through telephone interviews as needed. Secondary outcome was the recovery kidney function, which was assessed comparing the discharge and baseline creatinine and categorized as full recovery (within 20% above baseline creatinine), 20%-60% above baseline creatinine, or greater than 60% above baseline creatinine. Baseline creatinine was defined as the last available measurement from 365 to 7 days before hospital admission. Where baseline creatinine was not available, hospital admission creatinine was used as baseline. Discharge creatinine was the last measurement before hospital discharge.
Statistical Analysis
A one-way design with four groups was employed to assess whether differences exist among the group proportions. The comparison was conducted using a likelihood ratio chi-square test with three degrees of freedom. A sample size of 45 patients per group was determined to provide over 80% power, with an alpha level of 5%, to detect 90-day mortality rates of 50%, 35%, 25%, and 20%.
Normally distributed variables were presented as mean ± standard deviation (SD) and analyzed using one-way analysis of variance (ANOVA), followed by post hoc Tukey’s Honestly Significant Difference (HSD) testing to determine pairwise differences between groups. Non-normally distributed variables were described as medians with interquartile ranges and assessed using the Kruskal–Wallis test, followed by post-hoc Dunn’s multiple comparison test. Categorical variables were reported as percentages and compared using either Pearson’s chi-square test or Fisher’s exact test. The association between vitamin D levels and 90-day all-cause mortality risk was evaluated using multivariate Cox regression, controlling for potential confounding factors including age, gender, BMI, primary reason for admittance to the ICU, sepsis at admission to ICU, mechanical ventilation, comorbidities, APACHE II scores, SOFA scores, KDIGO stage, serum calcium, serum albumin, serum creatinine, and PTH levels. For missing laboratory values or clinical data, we employed multiple imputation methods where applicable to minimize potential bias. All analyses were two-sided, and significance was set at a P value less than 0.05.
Statistical analyses were conducted using SPSS version 20.0 for Windows (IBM Corp., Armonk, NY). The custom scripts for multivariate Cox regression and post-hoc testing is available upon request. Additionally, all statistical methods adhered to established guidelines for handling clinical datasets, with detailed coding available to ensure transparency.
Results
The flowchart of study population selection was shown in Figure 1. From July 2021 to June 2023, a total of 423 patients diagnosed with AKI in our ICU were recorded. After excluding 164 patients, the remaining 259 patients were included in the analysis and categorized based on their vitamin D status. Severe vitamin D deficiency was observed in 63 patients (24.3%), deficiency in 80 patients (30.9%), insufficiency in 67 patients (25.9%), and sufficient levels in 49 patients (18.9%). Table 1 presents the baseline demographics and clinical profiles of these groups. Significant differences were found in APACHE II scores, SOFA scores, 25-OHD levels, and PTH levels (all P<0.05, Figure 2), while no significant differences were noted in age, sex, BMI, admission diagnosis, sepsis occurrence, calcium, and albumin.
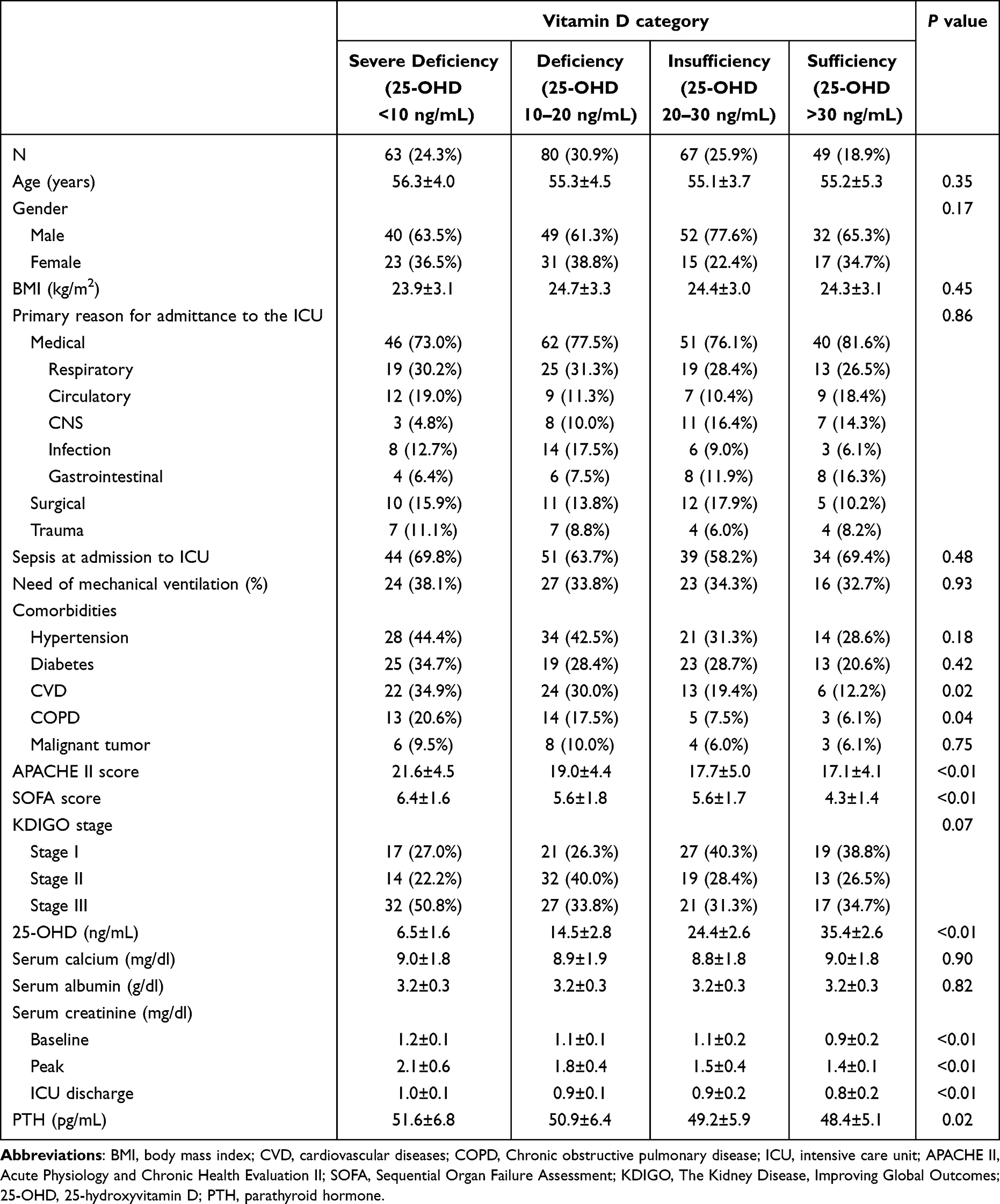 |
Table 1 Patients’ Baseline Demographics and Clinical Characteristics |
 |
Figure 1 Flowchart of study population selection. |
 |
Figure 2 Box plots of 25-OHD levels (A), PTH levels (B), APACHE II scores (C), and SOFA scores (D) across different vitamin D groups. *P <0.05 vs 25-OHD 10–20; #P <0.05 vs 25-OHD 20–30; ^P<0.05 vs 25-OHD >30. Abbreviations: 25-OHD, 25-hydroxyvitamin D; PTH, parathyroid hormone; APACHE II, Acute Physiology and Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment. |
Within the 90-day follow-up period, 82 patients (31.7%) died. The mortality rate over 90 days was highest in the severe vitamin D deficiency group (50.8%), followed by the deficiency group (35.0%), insufficiency group (23.9%), and sufficiency group (12.2%). Kaplan-Meier survival analysis (Figure 3) showed that patients with severe vitamin D deficiency had a significantly higher risk of 90-day all-cause mortality compared to those with sufficient levels (HR=5.75, 95% CI: 2.40–13.76; P<0.01), as did those with vitamin D deficiency (HR=3.25, 95% CI: 1.35–7.85; P =0.01).
 |
Figure 3 Kaplan-Meier survival curves comparing 90-day mortality across vitamin D groups in critically ill patients with acute kidney injury. |
Multivariate Cox regression analysis (Table 2) identified severe vitamin D deficiency (HR=3.34, 95% CI: 1.14–9.77; P=0.03) as a significant predictor of increased 90-day all-cause mortality risk. However, vitamin D deficiency and insufficiency did not significantly impact the 90-day all-cause mortality risk. Additionally, higher APACHE II scores (HR=1.07, 95% CI: 1.01–1.13; P=0.03) and SOFA scores (HR=1.22, 95% CI: 1.04–1.43; P=0.02), and KDIGO stage III (HR=2.11, 95% CI: 1.14–3.93; P=0.02) were associated with an elevated risk of 90-day mortality.
 |
Table 2 Univariate and Multivariate Cox Regression Analysis to Evaluate the Association Between Vitamin D Levels and 90-Day Mortality in Critically Ill Patients with Acute Kidney Injury |
The proportions of renal function recovery for each group are presented in Figure 4. The data show that the proportion of full recovery is significantly lower in patients with severe vitamin deficiency (65.1%) compared to those with sufficient levels (91.8%) and insufficient levels (82.1%) (P < 0.01).
 |
Figure 4 Association of vitamin D levels with renal function recovery. |
Discussion
AKI is a prevalent and multifaceted condition seen in critically ill patients. This study found that in critically ill patients with AKI, severe vitamin D deficiency was significantly associated with a higher risk of 90-day all-cause mortality.
Vitamin D deficiency plays a crucial role in renal recovery following AKI. It influences key biological processes involved in renal function, such as immune regulation, endothelial stability, and calcium metabolism.15 The bidirectional relationship between vitamin D and renal health is evident—AKI impairs vitamin D metabolism by reducing nephron function, specifically through decreased 1-alpha hydroxylase activity, which is responsible for converting 25-hydroxyvitamin D into its active form.23 Conversely, vitamin D deficiency may impair renal recovery mechanisms, including the renin-angiotensin-aldosterone system and renal vascular function.24 This deficiency can exacerbate ischemia-reperfusion injury (IRI) and hinder the repair process, thereby reducing the likelihood of full renal function recovery and potentially accelerating progression to CKD.25 Our study’s results, which show a significantly lower renal recovery rate in patients with severe vitamin D deficiency, support this hypothesis.
In the last decade, a number of studies have examined the possible association between low vitamin D levels and mortality among critical patients, with contradictory results. Vijayan’s study found that vitamin D levels were higher in non-survivors than survivors, however, on multivariate linear regression analysis, no association between vitamin D levels and mortality in critically ill AKI patients after adjusting for age and APACHE II score (β=0.29, 95% CI: 0.000–0.009, P=0.069).26 This lack of statistical significance may be attributed to their use of linear regression analysis, which may not accurately reflect the impact of severe vitamin D deficiency on mortality. This method could overlook the nonlinear relationships and complexities involved in the association between vitamin D levels and outcomes in critically ill patients. Leaf’s study did not give quantitative vitamin D data. They divided AKI patients into different groups according to medium vitamin D concentrations and concluded that no association exists between the serum vitamin D levels and all-cause mortality.27 Contrary to these findings, Zapatero et al identified an independent association between serum 25-OHD levels and 28-day mortality (OR=2.86, 95% CI: 1.05–7.86, P=0.04). The study highlighted a cut-off point of 10.9 ng/mL, which closely aligns with the definition of severe vitamin D deficiency.28 This result supports the hypothesis that a threshold effect exists, where extreme deficiency, rather than moderate deficiency, may play a crucial role in mortality risk. Our findings further support this view, demonstrating that severe vitamin D deficiency, in contrast to milder forms of deficiency, independently correlates with 90-day all-cause mortality. This association remains significant even after adjusting for APACHE II, SOFA scores, and KDIGO stages, emphasizing the potential for severe vitamin D deficiency to serve as a predictive marker for mortality in AKI patients.
Despite the significant findings, this study has certain limitations. One of the key challenges is the potential presence of confounding factors that could have influenced the outcomes. In particular, variables such as comorbid conditions and laboratory data may have affected the relationship between vitamin D levels and all-cause mortality. To address these confounders, we employed multivariable Cox regression models to adjust for their impact, thereby enhancing the accuracy and credibility of our results. However, residual confounding due to unmeasured or unknown factors remains a possibility and should be considered when interpreting the findings. For instance, serum Fibroblast Growth Factor 23 (FGF-23) was not measured in this study, which is a hormone produced by osteocytes and osteoblasts that plays a critical role in phosphate and vitamin D metabolism. Elevated FGF-23 levels might reflect disturbances in phosphate metabolism and could be a marker of adverse outcomes in critically ill patients. Including FGF-23 measurements in future prospective research could provide additional insights into its role and potential interactions with vitamin D levels and outcomes. Additionally, we did not measure vitamin D levels after discharge, which limits our understanding of the long-term implications of vitamin D deficiency in this patient group. Moreover, the single-center design and relatively small sample size limit the generalizability of our results to other regions. Furthermore, we assessed all-cause mortality rather than cause-specific death. While this provides a broad assessment of patient outcomes, it may obscure specific factors contributing to mortality in different patient subgroups. To address the limitations of our study, including residual confounding and sample size constraints, larger and multicenter studies are warranted. Such studies could incorporate more comprehensive data collection methods, including more genetic and biomarkers as well as cause-of-death data, to provide a clearer understanding of the relationship between vitamin D and AKI outcomes. By addressing these gaps, future research can further substantiate the clinical relevance of vitamin D status in managing AKI patients.
Conclusion
Severe vitamin D deficiency (25-OHD <10 ng/mL) is a strong predictor of 90-day all-cause mortality in AKI patients. Although recommendations for vitamin D supplementation vary by country and age, all guidelines consistently agree that serum 25-OHD levels below 10 ng/mL should be avoided at any age.29 Therefore, it is advised to supplement vitamin D in AKI patients with deficiency, particularly severe deficiency. A combination of D3 (cholecalciferol) and calcifediol is recommended, with D3 providing medium-term benefits due to its efficacy in raising serum 25-OHD levels, while calcifediol offers an immediate effect.30
To enhance clinical practice, regular assessment of vitamin D levels in AKI patients is essential to tailor supplementation strategies effectively. Future research should focus on multicenter trials to explore optimal dosing regimens and the impact of vitamin D supplementation on patient outcomes across diverse populations, addressing the limitations identified in this study and bridging existing knowledge gaps.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Levey AS, James MT. Acute Kidney Injury. Ann Intern Med. 2017;167(9):ITC66–ITC80. doi:10.7326/AITC201711070
2. Girling BJ, Channon SW, Haines RW, Prowle JR. Acute kidney injury and adverse outcomes of critical illness: correlation or causation? Clin Kidney J. 2020;13(2):133–141. doi:10.1093/ckj/sfz158
3. Tan L, Chen L, Jia Y, et al. Impact of diabetes mellitus on short-term prognosis, length of stay, and costs in patients with acute kidney injury: a nationwide survey in China. PLoS One. 2021;16(5):e0250934. doi:10.1371/journal.pone.0250934
4. Melo FAF, Macedo E, Fonseca Bezerra AC, et al. A systematic review and meta-analysis of acute kidney injury in the intensive care units of developed and developing countries. PLoS One. 2020;15(1):e0226325. doi:10.1371/journal.pone.0226325
5. Erfurt S, Hoffmeister M, Oess S, et al. Soluble IL-33 receptor predicts survival in acute kidney injury. J Circ Biomark. 2022;11:28–35. doi:10.33393/jcb.2022.2386
6. Gao XP, Zheng CF, Liao MQ, et al. Admission serum sodium and potassium levels predict survival among critically ill patients with acute kidney injury: a cohort study. BMC Nephrol. 2019;20(1):311. doi:10.1186/s12882-019-1505-9
7. Ishani A, Xue JL, Himmelfarb J, et al. Acute kidney injury increases risk of ESRD among elderly. J Am Soc Nephrol. 2009;20(1):223–228. doi:10.1681/ASN.2007080837
8. Lo LJ, Go AS, Chertow GM, et al. Dialysis-requiring acute renal failure increases the risk of progressive chronic kidney disease. Kidney Int. 2009;76(8):893–899. doi:10.1038/ki.2009.289
9. Qi Y, Chai J, Zhang L, Chen Y. Preoperative vitamin D level is significantly associated with hypocalcemia after total thyroidectomy. BMC Musculoskelet Disord. 2022;23(1):1118. doi:10.1186/s12891-022-05977-4
10. Ganimusa I, Chew E, Lu EM. Vitamin D Deficiency, Chronic Kidney Disease and Periodontitis. Medicina. 2024;60(3):420. doi:10.3390/medicina60030420
11. Dusso AS, Tokumoto M. Defective renal maintenance of the vitamin D endocrine system impairs vitamin D renoprotection: a downward spiral in kidney disease. Kidney Int. 2011;79(7):715–729. doi:10.1038/ki.2010.543
12. Yu W, Ying Q, Zhu W, Huang L, Hou Q. Vitamin D status was associated with sepsis in critically ill children: a PRISMA compliant systematic review and meta-analysis. Medicine. 2021;100(2):e23827. doi:10.1097/MD.0000000000023827
13. Liu W, Hu J, Fang Y, Wang P, Lu Y, Shen N. Vitamin D status in Mainland of China: a systematic review and meta-analysis. EClinicalMedicine. 2021;38:101017. doi:10.1016/j.eclinm.2021.101017
14. Chen KW, Chen CW, Yuan KC, et al. Prevalence of Vitamin D Deficiency and Associated Factors in Critically Ill Patients: a Multicenter Observational Study. Front Nutr. 2021;8:768804. doi:10.3389/fnut.2021.768804
15. Cameron LK, Ledwaba-Chapman L, Voong K, et al. Vitamin D metabolism in critically ill patients with acute kidney injury: a prospective observational study. Crit Care. 2024;28(1):108. doi:10.1186/s13054-024-04869-4
16. Ala-Kokko TI, Mutt SJ, Nisula S, et al. Vitamin D deficiency at admission is not associated with 90-day mortality in patients with severe sepsis or septic shock: observational FINNAKI cohort study. Ann Med. 2016;48(1–2):67–75. doi:10.3109/07853890.2015.1134807
17. Braun AB, Litonjua AA, Moromizato T, Gibbons FK, Giovannucci E, Christopher KB. Association of low serum 25-hydroxyvitamin D levels and acute kidney injury in the critically ill. Crit Care Med. 2012;40(12):3170–3179. doi:10.1097/CCM.0b013e318260c928
18. Zhang H, Jiang Y, Shi N, Lu YQ. Serum vitamin D levels and acute kidney injury: a systemic review and meta-analysis. Sci Rep. 2022;12(1):20365. doi:10.1038/s41598-022-24560-4
19. Quraishi SA, Bittner EA, Blum L, McCarthy CM, Bhan I, Camargo CA. Prospective study of vitamin D status at initiation of care in critically ill surgical patients and risk of 90-day mortality. Crit Care Med. 2014;42(6):1365–1371. doi:10.1097/CCM.0000000000000210
20. Malinverni S, Ochogavia Q, Lecrenier S, et al. Severe vitamin D deficiency in patients admitted to the emergency department with severe sepsis is associated with an increased 90-day mortality. Emerg Med J. 2023;40(1):36–41. doi:10.1136/emermed-2021-211973
21. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–84. doi:10.1159/000339789
22. Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008;87(4):1080S–6S. doi:10.1093/ajcn/87.4.1080S
23. Graidis S, Papavramidis TS, Papaioannou M. Vitamin D and Acute Kidney Injury: a Two-Way Causality Relation and a Predictive, Prognostic, and Therapeutic Role of Vitamin D. Front Nutr. 2020;7:630951. doi:10.3389/fnut.2020.630951
24. Zhang Y, Kong J, Deb DK, Chang A, Li YC. Vitamin D receptor attenuates renal fibrosis by suppressing the renin-angiotensin system. J Am Soc Nephrol. 2010;21(6):966–973. doi:10.1681/ASN.2009080872
25. Goncalves JG, de Braganca AC, Canale D, et al. Vitamin D deficiency aggravates chronic kidney disease progression after ischemic acute kidney injury. PLoS One. 2014;9(9):e107228. doi:10.1371/journal.pone.0107228
26. Vijayan A, Li T, Dusso A, Jain S, Coyne DW. Relationship of 1,25 dihydroxy Vitamin D Levels to Clinical Outcomes in Critically Ill Patients with Acute Kidney Injury. J Nephrol Ther. 2015;5(1). doi:10.4172/2161-0959.1000190
27. Leaf DE, Wolf M, Waikar SS, et al. FGF-23 levels in patients with AKI and risk of adverse outcomes. Clin J Am Soc Nephrol. 2012;7(8):1217–1223. doi:10.2215/CJN.00550112
28. Bouillon R. Comparative analysis of nutritional guidelines for vitamin D. Nat Rev Endocrinol. 2017;13(8):466–479. doi:10.1038/nrendo.2017.31
29. Zapatero A, Dot I, Diaz Y, et al. Severe vitamin D deficiency upon admission in critically ill patients is related to acute kidney injury and a poor prognosis. Med Intensiva. 2018;42(4):216–224. doi:10.1016/j.medin.2017.07.004
30. Wimalawansa SJ. Rapidly Increasing Serum 25(OH)D Boosts the Immune System, against Infections-Sepsis and COVID-19. Nutrients. 2022;14(14):2997. doi:10.3390/nu14142997
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.