")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Severe Vincristine-Induced Neuropathic Pain: A Case Report with Pharmacogenetic Analysis and Literature Review
Authors Hu YH, Li GZ, Long JY, Yang QY, Zhang Y, Chen F, Wang YR
Received 8 September 2022
Accepted for publication 5 December 2022
Published 30 December 2022 Volume 2022:15 Pages 1029—1035
DOI https://doi.org/10.2147/PGPM.S389197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Ya-Hui Hu,1 Gui-Zhou Li,1,2 Jia-Yi Long,1,2 Qing-Yan Yang,1,2 Yong Zhang,1 Feng Chen,1 Yong-Ren Wang3
1Department of Pharmacy, Children’s Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 2School of Basic Medicine and Clinical Pharmacy, China Pharmaceutical University, Nanjing, People’s Republic of China; 3Department of Hematology and Oncology, Children’s Hospital of Nanjing Medical University, Nanjing, People’s Republic of China
Correspondence: Yong-Ren Wang, Children’s Hospital of Nanjing Medical University, 72 Guangzhou Road, Nanjing, 210008, People’s Republic of China, Email [email protected]
Abstract: Vincristine-induced peripheral neuropathy (VIPN) is a common adverse effect of vincristine (VCR) for which there is no preventative or curative treatment. Here, we report a case of a patient suffering from severe VCR-related neurotoxicity. To explore the possible causes of severe VIPN in this patient, a set of genes involved in VCR metabolism, transport or are related to the cytoskeleton, microtubules, and inherited neurological diseases gene polymorphisms were examined via pharmacogenetic analyses. The genotyping results revealed the presence of a complex pattern of polymorphisms in CYP3A5, ABCC2, SYNE2, BAHD1, NPSR1, MTNR1B, CEP72, miR-4481 and miR-3117. A comprehensive understanding of all the pharmacogenetic risk factors for VIPN may explain the occurrence of severe neurotoxicity in our patient. This case brings to light the potential importance of pharmacogenetic testing in clinical practice. It also exemplifies the importance of developing early-detection strategies to optimize treatment regimens through prior risk stratification while reducing adverse drug reactions and personalizing therapy.
Keywords: vincristine, peripheral neuropathy, pharmacogenetics, toxicity, polymorphisms, precision medicine
Introduction
Vincristine (VCR) is a crucial medication in combination chemotherapy regimens for the treatment of most pediatric cancers, such as acute lymphoblastic leukemia (ALL), lymphomas, rhabdomyosarcoma, neuroblastoma, and nephroblastoma.1 The main side-effect of VCR is vincristine-induced peripheral neuropathy (VIPN) which causes peripheral and mostly symmetric sensory-motor neuropathy; these effects limit the dosage, delay treatment cycles, and even lead to discontinuation of chemotherapy.2 Clinical symptoms of VIPN include neuropathic pain, numbness and tingling in the hands and feet, muscle weakness, areflexia, and altered gait, amongst others. Furthermore, it can cause autonomic nerve injury and impaired sight and hearing.3 This debilitating feeling plagues approximately 30% of patients treated with VCR and severely reduces their quality of life.4
Multiple factors may alter the development and severity of VIPN, for example dose, age, gender, combination medicine and genetic variants.3,5 Indeed, the role of genetics in VIPN has been well documented. Pharmacogenomics can detect associations between genetic variation and drug safety, avoiding adverse drug reactions and maximizing drug efficacy.6 Single-nucleotide polymorphisms (SNPs) are the most common genetic variants. In the last decade, several SNPs associated with VIPN have been reported in pharmacogenomic studies through candidate gene studies7–9 or population-based GWAS or EWAS (genome- or exome-wide association studies).4,10 Variations in the expression or sensibility of VCR response-related proteins, such as drug metabolizing enzymes, transporters and therapeutic mechanisms are important sources of interindividual variability in drug response.
Here, we report a case of severe neuropathic pain after VCR chemotherapy in a patient with T-lymphoblastic lymphoma during the induction phase.
Presentation of Case
On January 21, a 10-year-old Chinese boy had numbness of the lips and face accompanied by obvious pain, which was improved after oral administration of ibuprofen. Since his tumor was primary in the neck and mediastinum and required vigilance for central invasion, the lymphoblastic lymphoma was deemed to be stage IV. According to Chinese Children Cancer Group-lymphoblastic lymphoma-2016 (CCCG-LBL-2016) treatment protocols, he began remission induction therapy with VCR, daunorubicin, prednisone, PEG-aspargase and triple it (methotrexate, cytarabine, and dexamethasone, intrathecally). The patient’s height and weight were 145 cm and 54 kg on admission, respectively. Thus, he received 2 mg (maximum dose, but < 1.5 mg/m2) VCR once daily on Days 1, 8, 15, and 22 of induction chemotherapy. In the following days, the child was given recombinant human granulocyte stimulating factor (rhG-CSF) injection to increase the number of neutrophils and voriconazole was used to prevent fungal infection. Three days after receiving the fourth dose of VCR, on February 15, the patient reported mild abdominal pain at night, which was relieved spontaneously. Examination of serum or urine amylase and color ultrasounds of hepatobiliary, pancreatic, and splenic tissues showed no significant abnormality. On the afternoon of February 17, the child cried and complained of pain in both legs, which was scored as 9 using the visual analogue scale (VAS). At night, it developed into systemic pain, mainly in the back, lower limbs and shoulders, which was paroxysmal and not relieved after his parents gave ibuprofen sustained-release capsules orally (dose unknown), with a VAS score of 8. After subsequent oral administration of compound paracetamol tablets (dose unknown) given by parents, the VAS score was 5. The physician considered peripheral neuralgia caused by rhG-CSF-stimulated myeloproliferation and/or VCR, so the patient was given an analgesic pump for intravenous analgesia after consultation with the anesthesiologist on February 18, and on the next day the VAS score decreased to 0. The patient then proceeded with sequential chemotherapy. On February 29, the patient reported transient abdominal pain, which was not severe and was relieved spontaneously. After this adverse event, no similar symptoms occurred during the following chemotherapy courses until the patient received the next dose of VCR.
Four months later, the patient was admitted to the hospital for reinduction chemotherapy with dexamethasone, VCR, epirubicin, PEG-aspargase and triple it (methotrexate, cytarabine, and dexamethasone, intrathecally). At this admission, the patient’s height did not increase, but his weight dropped to 44 kg. He received VCR 1.95 mg (1.51 mg/m2) on July 3, the first day of reinduction chemotherapy. After two days, the child reported pain around the gingiva and soft tissue at night which was accompanied by facial pain and headache when the pain was severe. On examination, significant local tenderness of the gingiva was noted, but there was no significant redness, swelling, suppuration, or dental caries, with a VAS score of 5. The patient’s symptoms did not decrease after oral administration of cefathiamidine and metronidazole for anti-infection, and the VAS score did not change. Therefore, the doctor gave the child compound paracetamol tablets (450 mg) for pain relief. Then the toothache was gradually relieved, and the VAS score decreased to 2 on July 8. However, on July 9, the patient began to experience back pain, which was suspected to be caused by drug toxicity of VCR, and the VAS score was 2. On July 10, while receiving the second dose of 1.95 mg (1.51 mg/m2) VCR, the patient was given mecobalamin to nourish the nerves, but in the following days the back pain persisted. On July 14, the patient received two intravenous bolus doses of tramadol hydrochloride, 50 mg and 100 mg, respectively, owing to body aches, especially in the back. By the night of July 16, the child had systemic pain and shortness of breath when the pain was severe with a VAS score of 3, and the doctor decided to treat him with an analgesic pump for pain relief; then, the VAS score decreased to 1. Since the patient did not appear to tolerate the neurotoxicity of VCR, the VCR in the regimen was replaced with vindesine to continue chemotherapy. On July 22, the systemic pain was improved, but the patient began to experience abdominal pain and urine trypsinogen was positive. Pancreatitis was considered, and chemotherapy was suspended until August 10, during which several episodes of abdominal pain occurred. On August 11, the patient’s condition was improved, and chemotherapy was continued in sequence. Notably, the patient still had occasional back pain for more than twenty days from July 24 to August 13. The chronology of chemotherapy medications and adverse effects is shown in Figure 1.
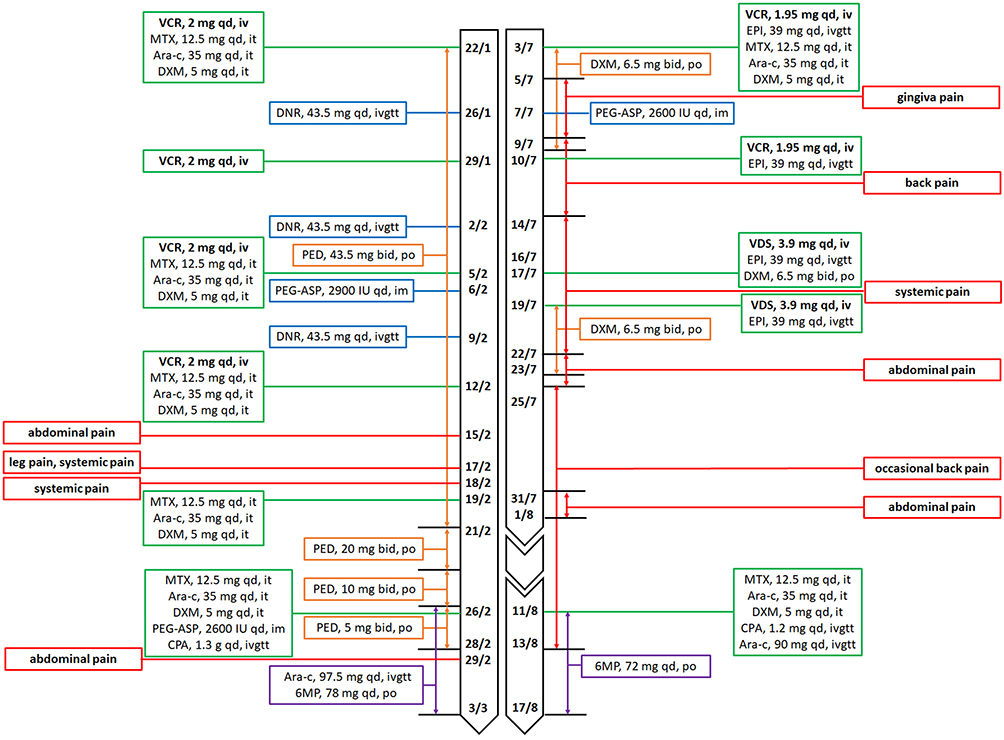 |
Figure 1 Chronology of Chemotherapy Medications and Adverse Effects. Abbreviations: VCR, vincristine; MTX, methotrexate; Ara-c, cytarabine; DXM, dexamethasone; DNR, daunorubicin; PED, prednisone; PEG-ASP, PEG-aspargase; CPA, cyclophosphamide; 6MP, mercaptopurine; EPI, epirubicin; VDS, vindesine; qd, once a day; bid, twice a day; iv, intravenous injection; it, intrathecal injection; ivgtt, intravenous drip; po, oral adminstration; im, intramuscular injection. |
Materials and Methods
To investigate the genetic basis of severe neuropathic pain, we summarized genes that identified by pharmacogenetic studies as responsible for the large interindividual differences in VIPN. Since there were no pharmacogenetic studies on T-lymphoblastic lymphoma with VCR in the database, we searched PubMed with a combination of the keywords “pharmacogenetic” AND “vincristine”. Of those genes, two SNPs in metabolism-associated genes (CYP3A4 and CYP3A5),9 five SNPs in transporter-associated genes (ATP-binding cassette transporter (ABCB1, ABCC1, ABCC2),8 solute carrier family 5 member 7 (SLC5A7)11), six SNPs in cytoskeleton-associated genes (centrosomal protein 72 (CEP72),4 spectrin repeat containing nuclear envelope protein 2 (SYNE2), mitochondrial ribosomal proteins 47 (MRPL47),10 capping actin protein gelsolin (CAPG), actin gamma 1 (ACTG1)7), six SNPs in genes detected by GWAS or EWAS (transmembrane protein 215 (TMEM215), melatonin receptor 1B (MTNR1B), Ewing’s tumor-associated antigen 1 (ETAA1), NADH: ubiquinone oxidoreductase complex assembly factor (NDUFAF6),4 bromo adjacent homology domain containing 1 (BAHD1),10 alpha tocopherol transfer protein (TTPA)11) and two SNPs in miRNA genes (miR–3117 and miR-448112) were reported to be significantly associated with VIPN. In addition, seven SNPs in the neuropeptide S receptor 1 (NPSR1) gene were implicated with recurrent abdominal pain.13 The polymorphisms of above-mentioned genes were examined. The study was performed in accordance with the Helsinki Declaration and the study protocol was approved by the Children’s Hospital of Nanjing Medical University ethics committee (Protocol number 202206117–1).
According to the manufacturer’s instructions, DNA was extracted from the patient’s peripheral blood using a DNA extraction kit (BioTeke Corporation, Wuxi, China) and stored at −80 ℃. Twenty-eight, relative SNPs were genotyped by direct automated DNA sequencing on an ABI 3730 analyzer after polymerase chain reaction (Applied). The primers used are listed in Supplementary Table S1.
Results
Sequence analysis revealed the presence of a complex pattern of polymorphisms: CYP3A5 rs776746 GG, ABCC2 rs12826 GG, SYNE2 rs2781377 AA, BAHD1 rs3803357 AA, NPSR1 rs887020 AG, miR-4481 rs7896283 GG, miR-3117-3p rs12402181 GA, MTNR1B rs12786200 CT, and CEP72 rs924607 CT (Table 1). Taken together, the genetic profile may be related to the pharmacokinetics and pharmacodynamics of VCR, thus explaining the observed VIPN. The results of all genotypes of the patient are shown in Supplementary Table S2.
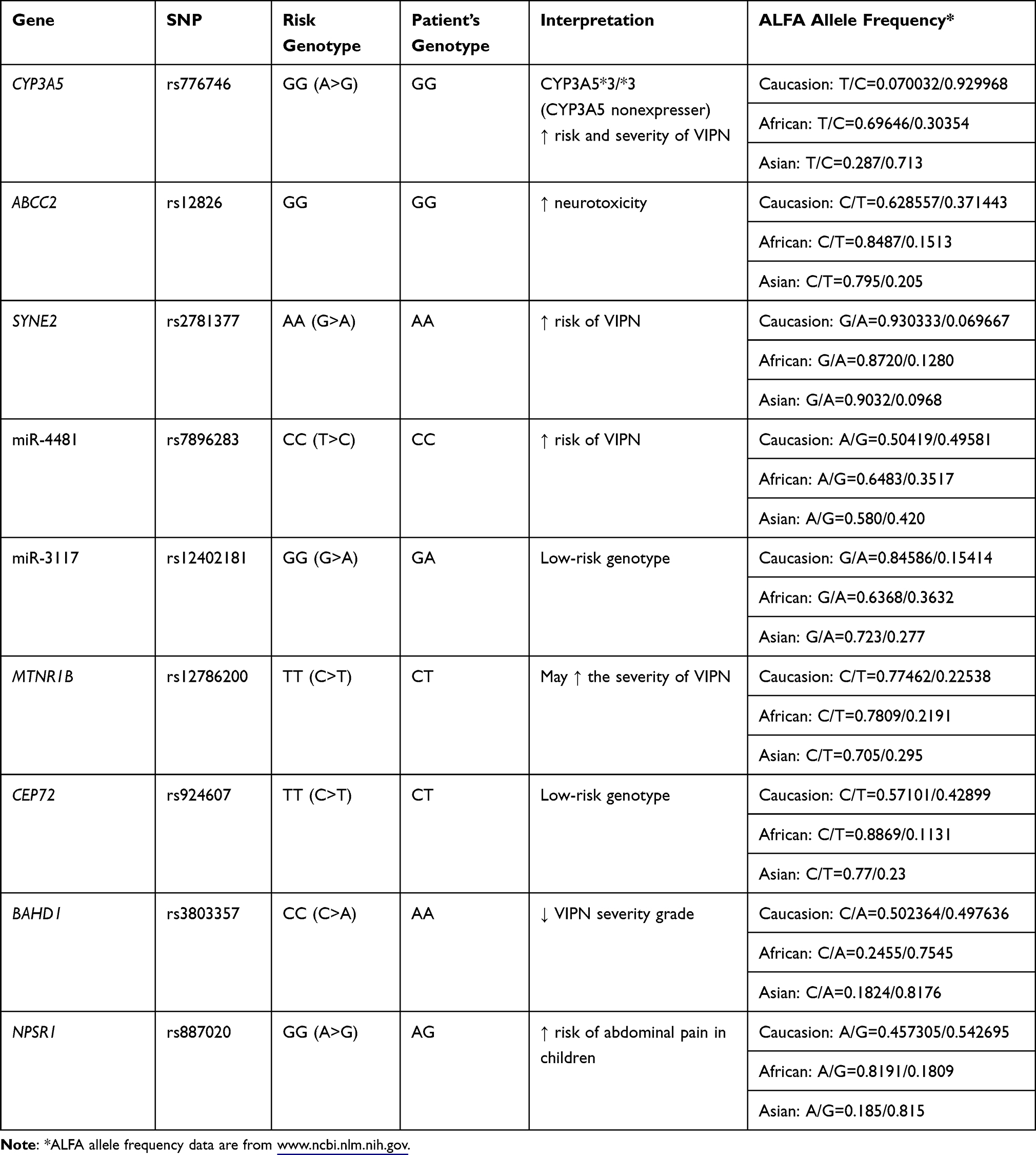 |
Table 1 Patient’s Genotype Results Associated with VIPN and ALFA Allele Frequency |
Discussion
The present case report describes a pediatric patient with T-lymphocytic lymphoma whose complex pattern of genetic polymorphisms may be the cause of severe neuropathic pain.
VCR pharmacokinetics showed large interpatient variability in the pediatric population.14 The genotypes of enzymes involved in VCR metabolism may affect the pharmacokinetic process of VCR. CYP3A family of enzymes is responsible for the metabolism of VCR. In fact, a link between genetic variants in CYP3A enzymes and drug toxicity has been established.15 Of note, CYP3A5 showed higher selective oxidation and 9- to 14-fold intrinsic clearance of VCR than CYP3A4, which was mainly manifested by a higher catalytic formation of primary metabolites (M1).16,17 Furthermore, the M1 plasma concentration was indicated to be negatively correlated with the severity of neuropathy. The CYP3A5*1 allele is required for the production of a functional enzyme. The CYP3A5*3 allele has a SNP in intron 3, resulting in a premature stop codon and no active CYP3A5 enzyme.18 Therefore, the polymorphic expression of CYP3A5 may be an important factor in the individual differences in VCR disposal and toxicity. Subjects with at least one CYP3A5*1 allele are called CYP3A5 expressers. In contrast, people with CYP3A5*3/*3 genotypes are considered CYP3A5 nonexpressers. The predicted intrinsic clearance of VCR was 5-fold higher in CYP3A5 expressers than nonexpressers.16 Compared with CYP3A5 expressers, CYP3A5 nonexpressers metabolize VCR slower (higher [VCR]/[M1] ratios) and experience more severe VIPN.9,15,19,20 However, contradictory results regarding the relationship between the CYP3A5 genotype and VCR-related neurotoxicity have been reported.7,21 In addition, a meta-analysis supported the point that CYP3A5 expression status was not a significant risk factor for the development of VIPN. The authors argued that considering the heterogeneity of the study population, treatment regimens, assessment methods, definitions of VIPN, and interpretation of the results are limited.1 The concentration time curve (AUC) of CYP3A5 nonexpressers was significantly higher than that of expressers.9 There is a statistically considerable association between AUC and the degree of neurotoxicity.22 To explore the relationship between drug exposure and VIPN, the potential of therapeutic drug monitoring (TDM) has therefore been highlighted. In the present case, the patient has the CYP3A5*3/*3 genotype and is a nonexpresser of this enzyme, which may lead to decreased metabolism of VCR and increased risk of drug exposure and VIPN.
VCR transport and clearance are mainly contributed by the ABC family, which consists of transmembrane proteins that mediate VCR efflux across cell membranes. Several SNPs of ABCB1, ABCC1 and ABCC2 were found to be significantly correlated with VIPN.7,8 ABCC1 is responsible for transporting VCR into the blood whereas ABCB1 and ABCC2 play a critical role in the biliary elimination of VCR.8 In this case, we found that the patient carried the wild-type homozygote in ABCC2 12826 GG after analyzing the SNPs in the above related genes. A retrospective study suggested that the GG genotype was most strongly associated with an increase in neurotoxicity, which remained statistically significant after false discovery rate (FDR) correction. The minor allele showed a dominant protective effect.8 The function of ABCC2 (also known as multidrug-resistance protein 2, MRP2) has been shown to be related to VCR resistance or sensitivity in several cell line studies.23,24 rs12826 is a downstream SNP with a predicted role at the transcriptional regulation level. This SNP may affect the general expression or function of ABCC2 in some way, resulting in changes in VCR clearance. However, the absence of mutation carriers may be accompanied by an accumulation of VCR in cells, leading to increased intracellular concentrations, thus explaining the association with neurotoxicity.
The cellular cytoskeleton-associated gene SYNE2, which encodes the Nesprin-2 protein, interacts with the nuclear lamina and plays a critical role in neuronal migration and neural development.25,26 Abaji et al identified that the AA allele of rs2781377 in the SYNE2 gene had an increased risk of high-grade VIPN by combining whole-exome sequencing (WES) and an exome-wide association study (EWAS) strategy.10
Accumulated evidence has shown that microRNAs (miRNAs) mediate posttranscriptional regulation involved in drug pharmacokinetics and pharmacodynamics directly or indirectly27 Gutierrez-Camino et al observed that CC alleles of rs7896283 CC/miR-4481 increased the risk of VCR-induced neurotoxicity by 2.6-fold (p = 0.017). In contrast, only the AA alleles of rs12402181/miR-3117 significantly decreased the risk of grade 1–4 neurotoxicity (p = 0.00042).12 It is worth noting that the pathway enrichment analysis revealed that rs7896283 in miR-4481 may be significantly related to the nervous system.12 Genetic variants in miR-4481 could alter miRNA levels and consequently, decrease the expression of genes involved in peripheral nerve regeneration and leading to an increase in peripheral neuropathy.
CEP72 gene is involved in the formation of microtubules and has been shown to be associated with VCR sensitivity. Diouf et al took a genome-wide approach and revealed that patients carrying the TT allele in CEP72 rs924607 had a higher incidence of VIPN than CC/CT patients,4 which was confirmed by two subsequent studies.11,28 Therefore, the CT genotype in this case cannot explain the observed neurotoxicity. Furthermore, genetic variants in MTNR1B rs12786200 may be correlated with the severity of VIPN based on the univariate, meta-analytic p-values from a North American cohort in this study.4
Interestingly, among the detected SNPs, a C to A polymorphism in the BAHD1 gene was identified as protective against high-grade VIPN. The CA/AA genotypes of rs3803357 were associated with a lower incidence of toxicity of VCR.10 BAHD1 is a heterochromatinization factor that may lead to neuropsychiatric disorders due to abnormal epigenetic features,29 which in itself, is linked to sensory and autonomic neuropathy.
Neuropeptide S receptor 1 (NPSR1) is a G protein-coupled receptor (GPCR) that is expressed in various regions of the brain and enteroendocrine cells in the gut and regulates several, physiological processes, including inflammation and pain.30 Considering the frequent occurrence of abdominal pain in our patient, seven SNPs in NPSR1 associated with recurrent abdominal pain13 were genotyped. NPSR1 polymorphisms may modulate abdominal pain by impacting its expression.
Conclusions
In conclusion, the severe VIPN developed in this patient might be associated with a complex pattern of polymorphisms. This case highlights the potential importance of pharmacogenetic testing in clinical practice. Unfortunately, there are no widely accepted genetic biomarkers. Therefore, further investigations in this field are needed to identify high-risk patients. Comprehensive risk assessments of pharmacogenomic factors may allow a safer, personalized approach to VCR-based chemotherapy in children.
Acknowledgments
Written informed consent to publish this case report was obtained from the patient and his guardian.
Funding
This work was supported by Grants from the National Natural Science Foundation (No. 81803642), the Jiangsu Research Hospital Association for Precision Medication (No. JY202010) and the Specially Appointed Medical Expert Project of Jiangsu Commission of Health (2019).
Disclosure
Gui-Zhou Li, Jia-Yi Long, and Qing-Yan Yang are visiting graduate students from China Pharmaceutical University. The authors declare no conflict of interest.
References
1. Uittenboogaard A, Neutel C, Ket J, et al. Pharmacogenomics of vincristine-induced peripheral neuropathy in children with cancer: a systematic review and meta-analysis. Cancers. 2022;14:612. doi:10.3390/cancers14030612
2. Triarico S, Romano A, Attinà G, et al. Vincristine-Induced Peripheral Neuropathy (VIPN) in pediatric tumors: mechanisms, risk factors, strategies of prevention and treatment. Int J Mol Sci. 2021;22:4112. doi:10.3390/ijms22084112
3. Li GZ, Hu YH, Li DY, et al. Vincristine-induced peripheral neuropathy: a mini-review. Neurotoxicology. 2020;81:161–171. doi:10.1016/j.neuro.2020.10.004
4. Diouf B, Crews KR, Lew G, et al. Association of an inherited genetic variant with vincristine-related peripheral neuropathy in children with acute lymphoblastic leukemia. JAMA. 2015;313:815–823. doi:10.1001/jama.2015.0894
5. Yang Q-Y, Hu Y-H, Guo H-L, et al. Vincristine-induced peripheral neuropathy in childhood acute lymphoblastic leukemia: genetic variation as a potential risk factor. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.771487
6. Weinshilboum R, Wang L. Pharmacogenomics: precision medicine and drug response. Mayo Clin Proc. 2017;92:1711–1722. doi:10.1016/j.mayocp.2017.09.001
7. Ceppi F, Langlois-Pelletier C, Gagne V, et al. Polymorphisms of the vincristine pathway and response to treatment in children with childhood acute lymphoblastic leukemia. Pharmacogenomics. 2014;15:1105–1116.
8. Lopez-Lopez E, Gutierrez-Camino A, Astigarraga I, et al. Vincristine pharmacokinetics pathway and neurotoxicity during early phases of treatment in pediatric acute lymphoblastic leukemia. Pharmacogenomics. 2016;17:731–741. doi:10.2217/pgs-2016-0001
9. Skiles J, Chiang C, Li C, et al. CYP3A5 genotype and its impact on vincristine pharmacokinetics and development of neuropathy in Kenyan children with cancer. Pediatr Blood Cancer. 2018;65:e26854. doi:10.1002/pbc.26854
10. Abaji R, Ceppi F, Patel S, et al. Genetic risk factors for VIPN in childhood acute lymphoblastic leukemia patients identified using whole-exome sequencing. Pharmacogenomics. 2018;19:1181–1193. doi:10.2217/pgs-2018-0093
11. Wright G, Amstutz U, Drögemöller B, et al. Pharmacogenomics of vincristine-induced peripheral neuropathy implicates pharmacokinetic and inherited neuropathy genes. Clin Pharmacol Ther. 2019;105:402–410. doi:10.1002/cpt.1179
12. Gutierrez-Camino A, Umerez M, Martin-Guerrero I, et al. Mir-pharmacogenetics of vincristine and peripheral neurotoxicity in childhood B-cell acute lymphoblastic leukemia. Pharmacogenomics J. 2018;18:704–712. doi:10.1038/s41397-017-0003-3
13. Henström M, Zucchelli M, Söderhäll C, et al. NPSR1 polymorphisms influence recurrent abdominal pain in children: a population-based study. Neurogastroenterol Motil. 2014;26:1417–1425. doi:10.1111/nmo.12401
14. Frost B, Lönnerholm G, Koopmans P, et al. Vincristine in childhood leukaemia: no pharmacokinetic rationale for dose reduction in adolescents. Acta paediatr. 2003;92:551–557. doi:10.1111/j.1651-2227.2003.tb02505.x
15. Egbelakin A, Ferguson M, MacGill E, et al. Increased risk of vincristine neurotoxicity associated with low CYP3A5 expression genotype in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2011;56:361–367. doi:10.1002/pbc.22845
16. Dennison J, Jones D, Renbarger J, Hall S. Effect of CYP3A5 expression on vincristine metabolism with human liver microsomes. J Pharmacol Exp Ther. 2007;321:553–563. doi:10.1124/jpet.106.118471
17. Dennison J, Kulanthaivel P, Barbuch R, Renbarger J, Ehlhardt W, Hall S. Selective metabolism of vincristine in vitro by CYP3A5. Drug Metab Dispos. 2006;34:1317–1327. doi:10.1124/dmd.106.009902
18. Kuehl P, Zhang J, Lin Y, et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat Genet. 2001;27:383–391. doi:10.1038/86882
19. McClain C, Bernhardt M, Berger A, et al. Pharmacogenetic association with neurotoxicity in Hispanic children with acute lymphoblastic leukaemia. Br J Haematol. 2018;181:684–687. doi:10.1111/bjh.14678
20. Sims R. The effect of race on the CYP3A-mediated metabolism of vincristine in pediatric patients with acute lymphoblastic leukemia. J Oncol Pharm Pract. 2016;22:76–81. doi:10.1177/1078155214553143
21. Guilhaumou R, Solas C, Bourgarel-Rey V, et al. Impact of plasma and intracellular exposure and CYP3A4, CYP3A5, and ABCB1 genetic polymorphisms on vincristine-induced neurotoxicity. Cancer Chemother Pharmacol. 2011;68:1633–1638. doi:10.1007/s00280-011-1745-2
22. Desai Z, Van den Berg H, Bridges J, Shanks R. Can severe vincristine neurotoxicity be prevented? Cancer Chemother Pharmacol. 1982;8:211–214. doi:10.1007/BF00255486
23. Cui Y, König J, Buchholz J, Spring H, Leier I, Keppler D. Drug resistance and ATP-dependent conjugate transport mediated by the apical multidrug resistance protein, MRP2, permanently expressed in human and canine cells. Mol Pharmacol. 1999;55:929–937.
24. Liu Z, Qiu M, Tang Q, Liu M, Lang N, Bi F. Establishment and biological characteristics of oxaliplatin-resistant human colon cancer cell lines. Chin J Cancer. 2010;29:661–667. doi:10.5732/cjc.009.10666
25. Gonçalves J, Quintremil S, Yi J, Vallee R. Nesprin-2 recruitment of BicD2 to the nuclear envelope controls dynein/kinesin-mediated neuronal migration in vivo. CB. 2020;30:3116–3129.e4. doi:10.1016/j.cub.2020.05.091
26. Young N, Asif M, Jackson M, et al. SYNE2Biallelic missense mutations leading to nesprin-2 giant hypo-expression are associated with intellectual disability and autism. Genes. 2021;12:1294. doi:10.3390/genes12091294
27. Li M, Hu Y, Hu X, et al. MiRNAs and miRNA polymorphisms modify drug response. Int J Environ Res Public Health. 2016;13:1096. doi:10.3390/ijerph13111096
28. Stock W, Diouf B, Crews K, et al. An inherited genetic variant in CEP72 promoter predisposes to vincristine-induced peripheral neuropathy in adults with acute lymphoblastic leukemia. Clin Pharmacol Ther. 2017;101:391–395. doi:10.1002/cpt.506
29. Pourpre R, Naudon L, Meziane H, et al. BAHD1 haploinsufficiency results in anxiety-like phenotypes in male mice. PLoS One. 2020;15:e0232789. doi:10.1371/journal.pone.0232789
30. Tapmeier T, Rahmioglu N, Lin J, et al. Neuropeptide S receptor 1 is a nonhormonal treatment target in endometriosis. Sci Transl Med. 2021;13. doi:10.1126/scitranslmed.abd6469
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.