Back to Journals » Infection and Drug Resistance » Volume 17
Severe Respiratory Syncytial Virus Infections in Elderly Persons During the COVID-19 Pandemic
Received 15 June 2024
Accepted for publication 15 August 2024
Published 24 August 2024 Volume 2024:17 Pages 3669—3675
DOI https://doi.org/10.2147/IDR.S474852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Daishi Shimada,1 Masafumi Seki1,2
1Division of Infectious Diseases, Tohoku Medical and Pharmaceutical University Hospital, Sendai City, Japan; 2Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Hidaka City, Japan
Correspondence: Masafumi Seki, Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Yamane 1397-1, Hidaka City, Saitama, 350-1298, Japan, Tel +81-42-984-4392, Fax +81-42-984-0280, Email [email protected]
Background: Respiratory syncytial virus (RSV) is a pathogenic respiratory virus that is considered to affect not only children but also adults, especially elderly persons aged ≥ 65 years. However, in Japan, the annual epidemic situation and severity of RSV infections in these adults have not yet been clarified, especially during the COVID-19 pandemic.
Methods: The epidemic of RSV, especially the number of adults with RSV infection during the COVID-19 period, was retrospectively analyzed. In addition, the clinical features of patients aged ≥ 65 years (older group) and those aged ≤ 64 years (younger group) were compared.
Results: A total of 58 patients were found to have RSV infections from April to August 2021. Ten were adults, and five each were detected in June and July, respectively. Of the 10 adult patients, three were in the older group and were more often infected by their grandchildren, and seven were in the younger group. All older patients had underlying diseases, including diabetes mellitus. In addition, the older group showed more severe inflammation, such as increased white blood cell counts and C-reactive protein levels, and received antibiotic therapy, whereas no antibiotics were used for the younger group. Two of the three older patients were admitted to our hospital, but survived.
Conclusion: These data suggest that RSV infection in adult patients was related to the increase in pediatric RSV patients and that the infection season had shifted to summer, similar to other countries. Among the adult RSV patients, those aged ≥ 65 years were more often infected by their grandchildren and received antibiotics because of their more severe inflammatory status than patients aged ≤ 64 years during the COVID-19 pandemic in Japan.
Keywords: antibiotic therapy, C-reactive protein, pediatric, underlying disease, viral pneumonia
Introduction
Respiratory syncytial virus (RSV) is considered an important viral pathogen of serious respiratory illness not only in children but also older adults. RSV infection is detected in 3%–7% of healthy adults in the community, 4%–10% of adults with high-risk factors, and 16% of those aged ≥65 years hospitalized due to cardiopulmonary infections.1,2 Furthermore, in the United States, it has been reported that RSV infection is related to approximately 177,000 hospitalizations, 10,000–14,000 deaths, and more than $1 billion dollars in health-care costs per year, mostly among older adults.1,3 Similar data have been reported from European countries.4,5 However, RSV is underestimated clinically by many physicians and health-care staff as a pathogen of lethal respiratory infection for adult patients, although several outbreaks among elderly persons residing in long-term care facilities have been reported.2,3 In addition, pooled estimates were 1.62% for RSV acute respiratory illness (RSV-ARI), 0.15% for hospitalizations, and 7.13% for in-hospital case fatalities in patients aged ≥60 years in a worldwide (including Japan) meta-analysis, and approximately 5.2 million infected cases, 470,000 hospitalizations, and 33,000 in-hospital deaths among ≥60-year-olds in high-income countries.6
In Japan, RSV-ARI was found in 24 of 1000 (2.4%) and RSV lower respiratory tract disease in eight of 1000 (0.8%) persons aged ≥65 years in a multicenter, prospective, observational, cohort study covering 52 weeks during the 2019–2020 season, which also found that all 24 RSV-ARI patients were from outpatient visits, but only one (4.2%) had been admitted to the hospital due to RSV-ARI.7 These findings suggested that RSV was one of the major pathogens of severe respiratory infections in elderly persons in Japan during this period, but very few data have been published and the real-world situation in Japan has remained unclear, because endemic RSV might vary by region, season, and other viral endemic infections, including influenza and COVID-19.8 In this study, the prevalence of RSV during the COVID-19 period was investigated and the clinical characteristics of adult RSV-infected patients compared between patients aged ≥65 years and those aged ≤64 years.
Methods
Patients
The data of patients who had eight major respiratory symptoms — cough, chills, dyspnea, fatigue, fever, nasal discharge, sore throat, and sputum — tested using the multiplex polymerase chain reaction (PCR) method (BioFire FilmArray Respiratory 2.1, bioMérieux, Lyon, France) at Tohoku Medical and Pharmaceutical University Hospital from April 1, 2021 to March 31, 2022 were analyzed. Patients whose nasal swabs showed positive RSV genes were included. These patients had visited the outpatient clinic. Those suspected of being infected in the hospital were excluded. Variables assessed included demographics, such as age, male:female ratio, underlying diseases, onset in persons in the family, symptoms, laboratory data, isolated bacteria, and treatment, such as antibiotic use and symptom management. We used antifebrile pills, expectorant, and cough suppressant for symptom management.
Ethics
The Committee for Clinical Scientific Research of Tohoku Medical and Pharmaceutical University Hospital approved this study on February 15, 2021 (ID2021-2-087) as a trial of surveillance for viral respiratory diseases. To have any accompanying images and their case details published, all participants whose specimens were used and all other patients in this study provided written, informed consent at admission. The patients were informed that they could opt out if they preferred not to be involved in these clinical studies. This study was performed according to the Declaration of Helsinki.
Statistical Analysis
Mann–Whitney and χ2 tests were used to compare continuous variables between two groups. Significant differences were defined as p<0.05. StatView software (Abacus Concepts, Cary, NC, USA) was used for all analyses.
Results
RSV Epidemic and Patient Characteristics
During the COVID-19 pandemic, there was an epidemic of RSV from April to September, 2021 (Figure 1). Of the total 58 RSV gene–positive patients, most were children, and the number peaked in July 2021. Ten adult patients were found in June and July, five in each month, in conjunction with the increase in pediatric patients. No pediatric or adult patients who were RSV gene–positive showed coinfection with another respiratory virus by our multiplex PCR detection system.
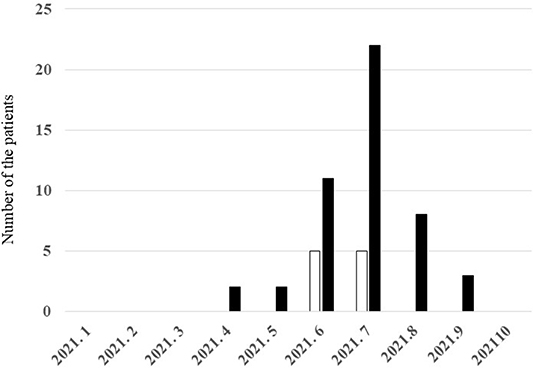 |
Figure 1 Numbers of adult and pediatric patients infected with RSV by month during the COVID-19 pandemic. |
Clinical Features of Adult Patients and Differences Between Those Aged ≥65 Years and Those Aged ≤64 Years
The clinical features of the 10 adult RSV-infected patients in this period are shown in Table 1. Of the 10 adult patients, three were aged ≥65 (median 80.3, range 78–83) years, and the other seven aged ≤64 (median 34.7, range 23–62) years (Table 2). The ages of the two groups were significantly different (p=0.022). The male:female ratio and symptoms were similar, but grandchildren were a significantly more common source of RSV infection in those ≥65 years of age (p=0.015), though more than half of those ≤64 years of age were infected by their children (Table 2). Underlying diseases were also similar: four of the seven patients ≤64 years of age had no underlying diseases, although all the three ≥65 years of age had underlying diseases, including sinusitis, diabetes mellitus, and gastroesophageal reflux disease. In addition, white blood cell counts and CRP levels were higher in those aged ≥65 years than those aged ≤64 years (Table 2). All patients ≥65 years of age received treatment with antibiotics, whereas no patients ≤64 years of age received antibiotics. Although two of the three patients ≥65 years of age admitted to our hospital, the other eight adult patients recovered on outpatient treatments, such as symptom management with/without antibiotics. All of the 10 adult patients, including the two older patients that were admitted, survived.
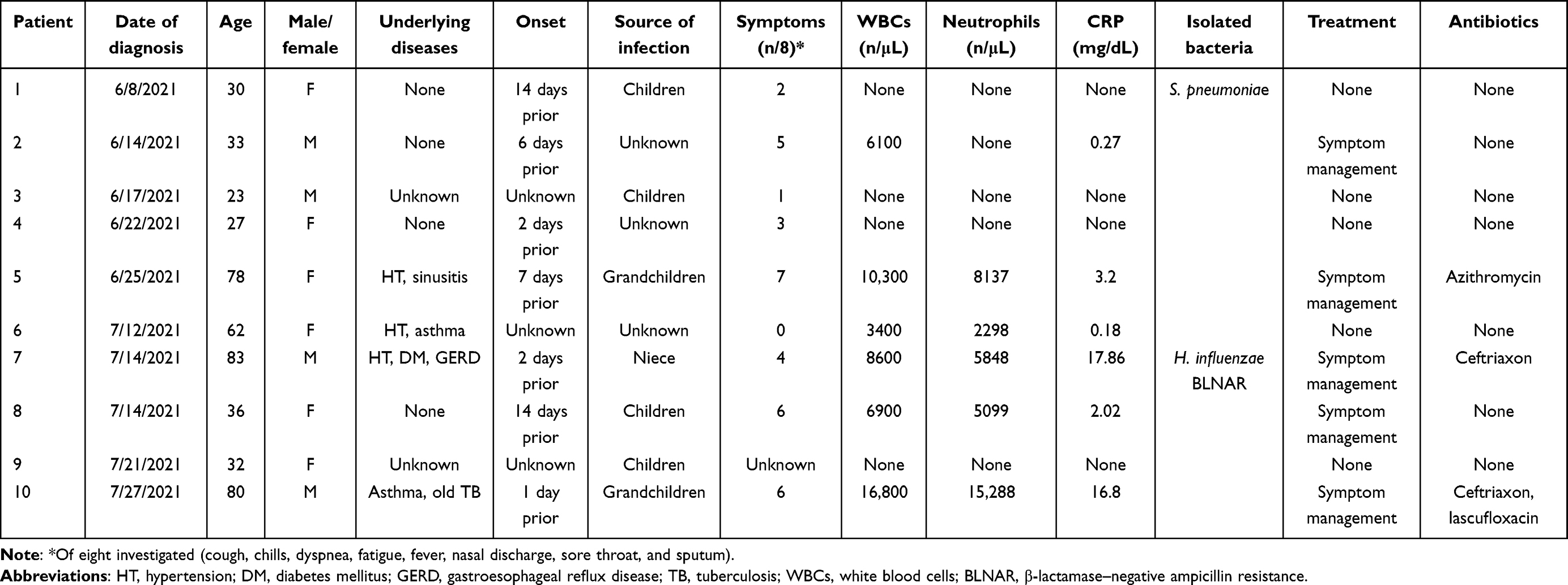 |
Table 1 Clinical characteristics of 10 adult patients infected with RSV during the COVID-19 epidemic |
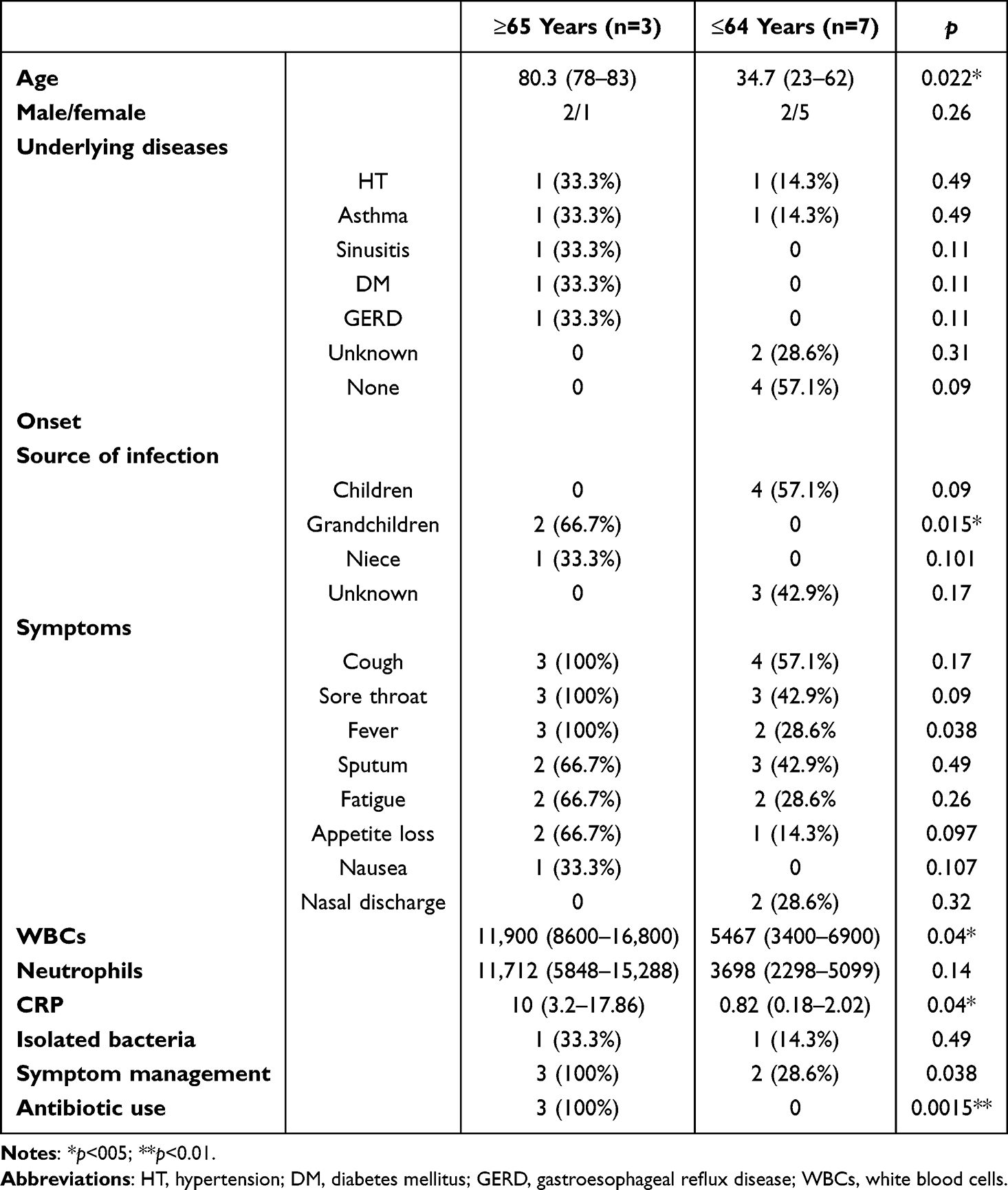 |
Table 2 Differences between RSV-infected adult patients aged ≥65 years and ≤64 years during the COVID-19 pandemic |
Discussion
In this study, the RSV epidemic that occurred in the period of COVID-19 pandemic was investigated, and it was found that RSV infections in adults occurred in association with the increase in pediatric RSV infections in Japan. The RSV epidemic occurred from spring to autumn and peaked in the summer of 2021, during the COVID-19 pandemic. Previously, RSV epidemics were thought to occur in winter or autumn before the influenza season,9 but this epidemic of RSV occurred in the summer. In the SARS-CoV-2–dominant period, the other respiratory viruses, including RSV, disappeared temporarily, and the majority of patients lost their immunity to RSV, thus leading to their easy infection with RSV.7,9,10 The role of nucleotide-binding oligomerization domain (NOD) 2 signaling in SARS-CoV-2 infection remains altogether unknown up to now; however, NOD2 has been reported to sense single-strand RNA from RSV to stimulate IFN responses through mitochondrial membrane–anchored proteins.11 Host miRNAs, a type of noncoding RNA, play a crucial role in the viral life cycle, influencing viral replication and the host immunoresponse directly or indirectly. One study focused specifically on miRNAs with documented expression in SARS-CoV-2 target cells, with an additional focus on miRNAs that have been reported in other viral infections, including RSV.12 Although trained immunity and immunological modifications have been suggested, these mechanisms might not work sufficiently to protect against the RSV endemic.
Furthermore, because it has been suggested that RSV interferes with the influenza virus,8 which also disappeared during the COVID-19 pandemic, RSV could have easily prevailed regardless of the season. Similar trends emerged worldwide, with delays in the expected RSV season ranging from 13 weeks in France to 88 weeks in South Korea, and a particularly large spike in cases in the 2022–2023 season were also found in the US.13 These data also suggested dynamic changes in RSV infection and transmission epidemiologically and immunologically.
Elderly patients started to be infected by RSV after the RSV epidemic in children started to appear from April 2021, and these infected children were identified after the RSV infections in adult patients disappeared. These data suggested that children were the source of the RSV infection and that adults might be infected by children in the community and/or homes in the situations investigated.14 In addition, in the present study, patients aged ≥65 years were infected more often by grandchildren than those aged ≤64 years, being a parent generation that was mostly infected by their children. These data also suggest that patients who were aged ≥65 years were infected by their grandchildren, and thus most adult patients might have been infected in their homes by children in general in Japan.
In the adult patients of the present study, those aged ≥65 years developed a more severe inflammatory status and received antibiotic treatment more often than those aged ≤64 years. It has been reported that the clinical outcome of 243 RSV-infected adults aged ≥60 years was 17% (n=41) mild, 64% (n=155) moderate, and 19% (n=41) serious.15 Moderate patients included those given a new antibiotic prescription (n=144), and serious patients included those admitted to hospital (n=29) and emergency department visits (n=13). These data also suggested that RSV infections were common in elderly persons, were of moderate–severe status, and needed more intensive treatment than symptom management alone, although no patients aged ≥65 years died, and RSV, unlike influenza, was not associated with underlying diseases, such as congestive heart failure or chronic pulmonary disease, in contrast toa previous report.16 In our cohort, four of seven RSV patients ≤64 years of age had no underlying diseases, although all three patients ≥65 years of age had underlying diseases, but these differences were not significant statistically, and none of the patients died.
The mechanisms by which RSV infection leads to severe inflammation in elderly persons are unclear, but significant increases in serum neutralization titers, IgG concentrations and local upregulation of IFNβ, IFNλ1, IFNγ, IL1β, TNFα, IL6, IL10, CXCL8, and CXCL10 based on assessment of antibody and local cytokine responses to RSV infection have been reported in older adults (≥60 years of age).17 IFNβ, IFNλ1, CXCL8, and CXCL10 are also upregulated in the epithelial model by RSV infection.18 This increased inflammatory status may lead to severe status in adults, especially those ≥65 years of age with RSV infection.
In conclusion, similar to other countries an epidemic of RSV infection was identified in the summer of 2021 during the COVID-19 pandemic in Japan, and the increase in adult patients matched the increase in pediatric patients. Coinfections with other respiratory viruses were not found. In adult patients infected with RSV, those aged ≥65 years were more often infected by their grandchildren and showed more severe inflammation status than those aged ≤64 years infected with RSV. The older patients had underlying diseases, but all adult patients finally survived. More extensive care and treatments, including antibiotic treatment, should be considered for elderly patients infected with RSV.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005;352(17):1749–1759. doi:10.1056/NEJMoa043951
2. Branche AR, Saiman L, Walsh EE, et al. Incidence of respiratory syncytial virus infection among hospitalized adults, 2017-2020. Clin Infect Dis. 2022;74(6):1004–1011. doi:10.1093/cid/ciab595
3. Ackerson B, Tseng HF, Sy LS, et al. Severe morbidity and mortality associated with respiratory syncytial virus versus influenza infection in hospitalized older adults. Clin Infect Dis. 2019;69(2):197–203. doi:10.1093/cid/ciy991
4. Boattini M, Almeida A, Christaki E, et al. Influenza and respiratory syncytial virus infections in the oldest-old continent. Eur J Clin Microbiol Infect Dis. 2020;39(11):2085–2090. doi:10.1007/s10096-020-03959-9
5. Boattini M, Charrier L, Almeida A, et al. Burden of primary influenza and respiratory syncytial virus pneumonia in hospitalised adults: insights from a 2-year multi-centre cohort study (2017-2018). Intern Med J. 2023;53(3):404–408. doi:10.1111/imj.15583
6. Savic M, Penders Y, Shi T, Branche A, Pirçon JY. Respiratory syncytial virus disease burden in adults aged 60 years and older in high-income countries: a systematic literature review and meta-analysis. Influenza Other Respir Viruses. 2023;17(1):e13031. doi:10.1111/irv.13031
7. Kurai D, Natori M, Yamada M, Zheng R, Saito Y, Takahashi H. Occurrence and disease burden of respiratory syncytial virus and other respiratory pathogens in adults aged ≥65 years in community: a prospective cohort study in Japan. Influenza Other Respir Viruses. 2021;16(2):298–307. doi:10.1111/irv.12928
8. Nickbakhsh S, Mair C, Matthews L, et al. Virus-virus interactions impact the population dynamics of influenza and the common cold. Proc Natl Acad Sci U S A. 2019;116(52):27142–27150. doi:10.1073/pnas.1911083116
9. Staadegaard L, Caini S, Wangchuk S, et al. Defining the seasonality of respiratory syncytial virus around the world: national and subnational surveillance data from 12 countries. Influenza Other Respir Viruses. 2021;15(6):732–741. doi:10.1111/irv.12885
10. Centers for Disease Control and Prevention. Respiratory syncytial virus infection (RSV). 2024: Available from: https://www.cdc.gov/rsv/index.html.
11. Wannigama DL, Jacquet A. NOD2-dependent BCG-induced trained immunity: a way to regulate innate responses to SARS-CoV2? Int J Infect Dis. 2020;101:52–55. doi:10.1016/j.ijid.2020.09.1429
12. Rad S, Wannigama DL, Hirankarn N, McLellan AD. The impact of non-synonymous mutations on miRNA binding sites within the SARS-CoV-2 NSP3 and NSP4 genes. Sci Rep. 2023;13(1):16945. doi:10.1038/s41598-023-44219-y
13. Rios-Guzman E, Simons LM, Dean TJ, et al. Deviations in RSV epidemiological patterns and population structures in the United States following the COVID-19 pandemic. Nat Commun. 2024;15(1):3374. doi:10.1038/s41467-024-47757-9
14. McClure DL, Kieke BA, Sundaram ME, et al. Seasonal incidence of medically attended respiratory syncytial virus infection in a community cohort of adults ≥50 years old. PLoS One. 2014;9(7):e102586. doi:10.1371/journal.pone.0102586
15. Belongia EA, King JP, Kieke BA, et al. Clinical features, severity, and incidence of rsv illness during 12 consecutive seasons in a community cohort of adults ≥60 years old. Open Forum Infect Dis. 2018;5(12). doi:10.1093/ofid/ofy316
16. Sundaram ME, Meece JK, Sifakis F, Gasser RA Jr, Belongia EA. Medically attended respiratory syncytial virus infections in adults aged ≥ 50 years: clinical characteristics and outcomes. Clin Infect Dis. 2014;58(3):342–349. doi:10.1093/cid/cit767
17. Yu X, Lakerveld AJ, Imholz S, et al. Antibody and local cytokine response to respiratory syncytial virus infection in community-dwelling older adults. mSphere. 2020;5(5):e00577–20. doi:10.1128/mSphere.00577-20
18. Dee K, Schultz V, Haney J, Bissett LA, Magill C, Murcia PR. Influenza A and respiratory syncytial virus trigger a cellular response that blocks severe acute respiratory syndrome virus 2 infection in the respiratory tract. J Infect Dis. 2023;227(12):1396–1406. doi:10.1093/infdis/jiac494
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.