Back to Journals » International Medical Case Reports Journal » Volume 19
Severe Respiratory Diphtheria Complicated by Myocarditis-Induced Dilated Cardiomyopathy and Peripheral Neuropathy in a Non-Immunized Two-Year-Old Child from Rural Somalia: A Case Report
Authors Farah SA ![]() , Hassan Orey FA
, Hassan Orey FA ![]() , Elmi AH
, Elmi AH ![]()
Received 7 April 2026
Accepted for publication 13 May 2026
Published 15 May 2026 Volume 2026:19 615193
DOI https://doi.org/10.2147/IMCRJ.S615193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Salad Abdullahi Farah,1 Fartun Abdullahi Hassan Orey,1 Abdullahi Hassan Elmi2
1Department of Pediatrics and Child Health, Dr Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Nursing and Midwifery, Dr Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia
Correspondence: Salad Abdullahi Farah, Email [email protected]
Introduction: Diphtheria remains a serious vaccine-preventable infection, particularly among under-immunized children in fragile and resource-limited settings. In Somalia, gaps in routine immunization, delayed healthcare access, and limited diagnostic and treatment resources may increase the risk of severe toxin-mediated complications. Cardiac and neurological involvement are among the most serious manifestations, and their coexistence in a young child is uncommon.
Case Presentation: We report the case of a non-immunized two-year-old boy from rural Somalia who presented with fever, sore throat, progressive dysphagia, respiratory distress, bull-neck swelling, and a firmly adherent grayish-white pharyngeal pseudomembrane. He developed clinical and echocardiographic evidence of diphtheritic myocarditis complicated by toxin-induced dilated cardiomyopathy, followed by progressive symmetrical limb weakness with markedly reduced deep tendon reflexes, consistent with diphtheritic peripheral neuropathy. He was treated with diphtheria antitoxin, intravenous erythromycin, isolation, cardiac monitoring, heart failure therapy, physiotherapy, and nutritional support. His respiratory, cardiac, and neurological status improved progressively, and at one-month follow-up he had no clinical signs of heart failure and was able to walk with minimal support.
Conclusion: This case highlights that diphtheria remains a life-threatening but preventable multisystem disease among unvaccinated children in fragile settings. Early clinical recognition, prompt antitoxin administration, antimicrobial therapy, cardiac monitoring, and supportive multidisciplinary care are essential. The report also reinforces the urgent need to strengthen routine childhood immunization in Somalia to prevent severe disease and avoidable complications.
Keywords: diphtheria, respiratory diphtheria, diphtheritic myocarditis, dilated cardiomyopathy, peripheral neuropathy, non-immunized child, low-resource setting, Somalia
Introduction
Diphtheria is a serious toxin-mediated bacterial infection caused mainly by Corynebacterium diphtheriae and remains an important vaccine-preventable disease, particularly in children from under-immunized communities.1–3 Although the global burden of diphtheria has declined markedly since the introduction of diphtheria toxoid–containing vaccines, the disease has not been eliminated and continues to occur in regions where vaccination coverage is incomplete and access to healthcare is limited.1,4–7 In these settings, delayed diagnosis and restricted treatment resources can allow otherwise preventable cases to progress to severe and potentially fatal illness.
Although global diphtheria incidence has declined substantially with routine vaccination, the disease continues to persist and surge in settings where immunization coverage is incomplete and health systems are disrupted. In Somalia, prolonged conflict, internal displacement, recurrent climatic shocks, limited access to healthcare, and interruptions in vaccination services create conditions in which unvaccinated children remain vulnerable to severe toxin-mediated disease. These structural factors may also delay clinical recognition, referral, laboratory confirmation, and access to diphtheria antitoxin, increasing the risk of severe respiratory, cardiac, and neurological complications.1,2
Respiratory diphtheria is the most recognized clinical form of the disease and typically presents with fever, sore throat, cervical lymphadenopathy, and the development of a thick, firmly adherent pseudomembrane over the tonsils, pharynx, or larynx.2,3,8 In young children, progressive upper airway involvement may lead to life-threatening obstruction. However, the major danger of diphtheria extends beyond the local respiratory infection. Once absorbed systemically, diphtheria toxin can produce multisystem injury, with the heart and peripheral nervous system among the most severely affected organs.9–12
Myocardial involvement is one of the most feared complications of diphtheria and is a well-established predictor of poor outcome. Cardiac and neurological complications are among the most serious systemic manifestations of diphtheria because diphtheria toxin can affect the myocardium and peripheral nerves after the initial respiratory infection.10,11 Diphtheritic myocarditis may present with conduction disturbances, arrhythmias, ventricular dysfunction, or overt heart failure, and in severe cases may evolve into dilated cardiomyopathy.9,10,13 Functional mitral regurgitation may also occur secondary to ventricular dilatation and impaired cardiac performance, further complicating the clinical course.13,14 Even among survivors, cardiac toxicity can result in substantial morbidity and warrants close monitoring during the acute and recovery phases.
Neurological complications are another important manifestation of systemic toxin effect and usually appear after the onset of the initial respiratory illness.9,11,12 Diphtheritic neuropathy commonly presents with progressive symmetrical weakness and diminished or absent deep tendon reflexes, with severity ranging from mild motor impairment to extensive neuromuscular dysfunction.9,11,12 The occurrence of both significant cardiac and neurological complications in the same child is uncommon and reflects severe toxin-mediated disease.
Despite major advances in prevention, diphtheria continues to persist and surge in vulnerable populations where routine immunization is incomplete, health systems are disrupted, and access to timely diagnosis, diphtheria antitoxin, and supportive care is limited.1,4–7,15 Reports of severe disease in such contexts remain clinically important because they highlight the persistent consequences of immunization gaps and the challenges of managing toxin-mediated complications in resource-constrained settings.
In this report, we describe a non-immunized two-year-old boy from rural Somalia who presented with severe respiratory diphtheria complicated by myocarditis-induced dilated cardiomyopathy and peripheral neuropathy. This case highlights the continued threat of diphtheria in low-resource settings, the need for early recognition of systemic complications, and the critical importance of strengthening routine childhood immunization to prevent severe and life-threatening disease.
Case Presentation
A 2-year-old non-immunized boy from a rural area of Somalia was admitted with a 7-day history of high-grade fever, sore throat, progressive dysphagia, and worsening respiratory distress. According to his parents, his illness began with fever and throat pain, followed by the development of a thick grayish membrane over the tonsils and pharynx, foul-smelling breath, and painful neck swelling. He had not received any routine childhood immunizations, including diphtheria-containing vaccines.
On admission, the child appeared acutely ill and toxic. He had marked bilateral cervical lymphadenopathy producing the characteristic “bull-neck” appearance. Oropharyngeal examination showed a thick, firmly adherent grayish-white pseudomembrane covering the tonsils and posterior pharyngeal wall, with bleeding on attempted removal. These findings, together with inspiratory stridor, progressive dysphagia, and respiratory distress in a completely non-immunized child, strongly supported the clinical diagnosis of severe respiratory diphtheria. Microbiological confirmation by culture, toxin testing, or polymerase chain reaction was not available at the time of care; therefore, the diagnosis was made clinically based on the characteristic respiratory findings, complete lack of immunization, systemic complications, and response to diphtheria-specific treatment.
Cardiovascular examination revealed tachycardia, a gallop rhythm, and a soft holosystolic murmur best heard at the apex. The liver was palpable 3 cm below the right costal margin, and mild pedal edema was noted, raising concern for early heart failure. Chest auscultation revealed bilateral basal crepitations. Chest radiography was performed and showed no focal lung consolidation, pleural effusion, or other acute parenchymal abnormality (Figure 1).
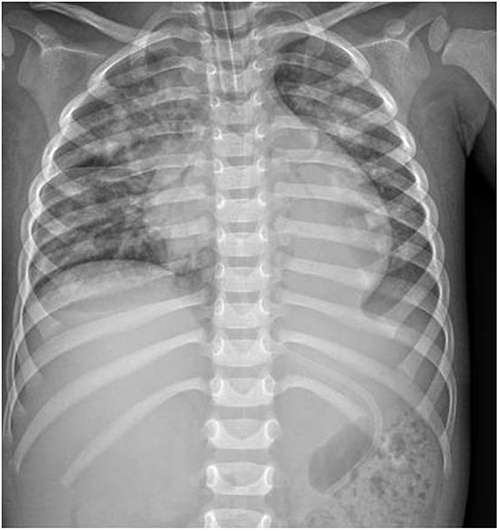 |
Figure 1 Chest radiograph obtained on admission showing no focal pulmonary consolidation, pleural effusion, or acute intrathoracic abnormality. |
Initial laboratory investigations demonstrated leukocytosis, with a white blood cell count of 19.4 × 109/L and neutrophils of 78%. Mild anemia was present, with a hemoglobin level of 9.6 g/dL, while the platelet count remained within normal range. C-reactive protein was elevated at 68 mg/L. Serum electrolytes, urea, and creatinine were within normal limits, with no laboratory evidence of acute kidney injury during admission. Liver enzymes were mildly elevated, with AST 86 U/L and ALT 74 U/L. Cardiac biomarkers showed elevated troponin I (1.6 ng/mL) and CK-MB, supporting myocardial injury (Table 1). Electrocardiography showed sinus tachycardia without significant arrhythmia, conduction block, or ischemic changes.
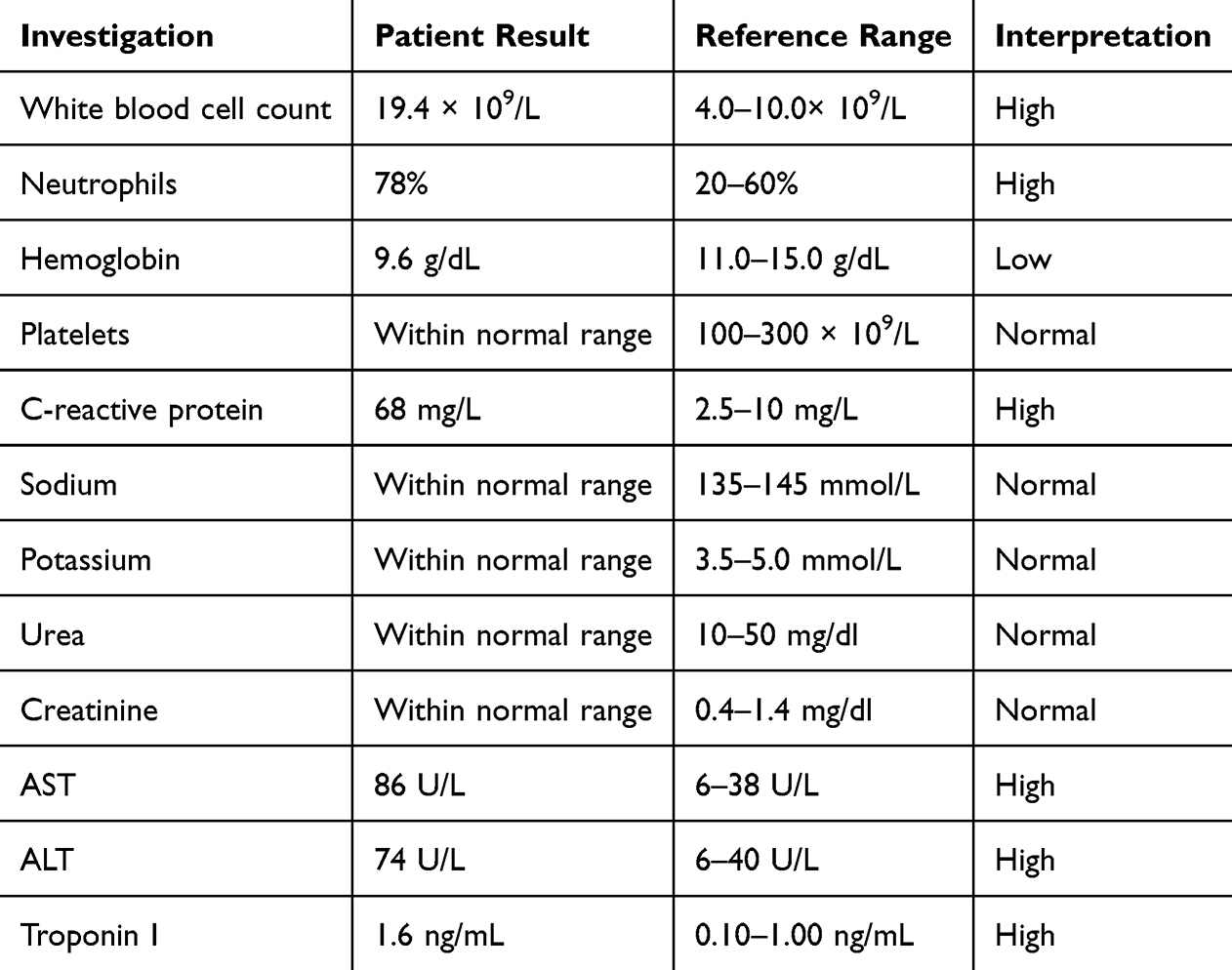 |
Table 1 Laboratory Investigations on Admission |
Transthoracic echocardiography demonstrated a dilated left ventricular cavity with global hypokinesia, mildly reduced left ventricular systolic function with an ejection fraction of approximately 45%, and mild-to-moderate functional mitral regurgitation, without pericardial effusion or intracardiac thrombus. Representative echocardiographic findings are shown in (Figure 2). These findings were consistent with diphtheritic myocarditis complicated by toxin-induced dilated cardiomyopathy (Figure 3).
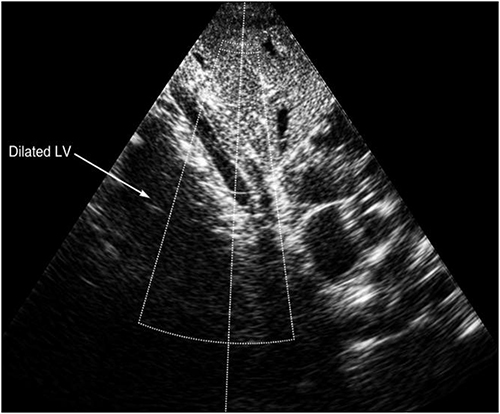 |
Figure 2 Transthoracic echocardiographic image showing left ventricular dilatation with global hypokinesia and mildly reduced systolic function, consistent with diphtheritic myocarditis complicated by toxin-induced dilated cardiomyopathy. |
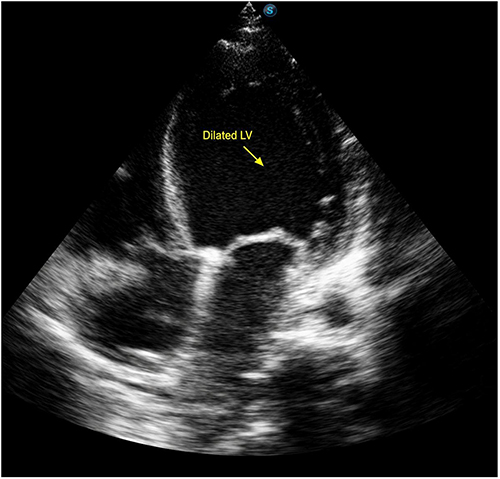 |
Figure 3 Transthoracic echocardiographic image demonstrating dilated cardiac chambers and reduced systolic function, supporting toxin-induced dilated cardiomyopathy secondary to diphtheritic myocarditis. |
On the fifth hospital day, after initial stabilization, the child developed progressive symmetrical weakness involving both the upper and lower limbs. He became unable to sit unsupported and was unable to stand. Deep tendon reflexes were markedly diminished, although sensation remained preserved. Cranial nerve examination was normal, with no evidence of bulbar palsy or ophthalmoplegia. In the absence of nerve conduction studies, which were not available in our setting, the clinical picture strongly suggested diphtheritic peripheral neuropathy secondary to systemic toxin-mediated nerve injury.
Given the strong clinical suspicion of severe respiratory diphtheria, the child was transferred to the pediatric high-dependency unit and placed in isolation. Following a negative sensitivity test, equine diphtheria antitoxin was administered intravenously at a dose appropriate for severe respiratory disease. Intravenous erythromycin at 40 mg/kg/day was initiated and continued for 14 days to eradicate Corynebacterium diphtheriae and halt further toxin production.
Because of the evidence of cardiac involvement, continuous cardiac monitoring was instituted. The child was managed for heart failure with supplemental oxygen, intravenous furosemide, and a low-dose angiotensin-converting enzyme inhibitor. Fluid balance was closely monitored throughout hospitalization. No significant arrhythmias or high-grade atrioventricular block were observed.
Supportive care was provided for the neurological complication, including early physiotherapy with daily passive and active limb exercises to prevent contractures and support recovery. Nutritional rehabilitation and multivitamin supplementation were also given.
Over the next 10 to 14 days, the child showed progressive clinical improvement. Fever subsided, respiratory distress resolved, and the pseudomembrane gradually disappeared. Limb strength improved steadily, and deep tendon reflexes began to return. He was discharged on oral heart failure medications with close follow-up planned in both cardiology and neurology clinics. At the 1-month follow-up visit, he was able to walk with minimal support and had no clinical signs of heart failure.
Discussion
This case illustrates a severe and uncommon presentation of respiratory diphtheria in a non-immunized young child, complicated by two major toxin-mediated sequelae: myocarditis with dilated cardiomyopathy and peripheral neuropathy. Although diphtheria is now preventable through routine vaccination, it continues to cause serious illness in under-immunized populations, particularly in low-resource settings where delayed presentation and limited access to specialized care may worsen outcome.1,11–15 The present case is clinically important because it demonstrates the classical local manifestations of severe respiratory diphtheria together with early cardiac involvement and subsequent neurological complications in the same patient.
The initial presentation was highly consistent with severe upper respiratory diphtheria, including fever, sore throat, a thick adherent pharyngeal pseudomembrane, cervical lymphadenopathy with “bull-neck” appearance, stridor, and respiratory distress. These findings are well recognized features of toxic respiratory diphtheria and should prompt urgent clinical suspicion, particularly in an unvaccinated child.2,3,9 In many resource-constrained settings, diagnosis remains primarily clinical because bacteriological confirmation may be delayed or unavailable. Under such circumstances, timely recognition is essential, as delayed treatment increases the likelihood of systemic toxin absorption and organ injury.12,15
Cardiac involvement is among the most serious complications of diphtheria and remains a major predictor of mortality.4,5 In this patient, tachycardia, gallop rhythm, hepatomegaly, edema, elevated cardiac biomarkers, and echocardiographic evidence of left ventricular dilatation with global hypokinesia strongly supported diphtheritic myocarditis. The presence of reduced systolic function and functional mitral regurgitation further suggested clinically significant myocardial injury with secondary ventricular remodeling.4–7 Previous studies have shown that diphtheritic cardiomyopathy may develop early in the disease course and may range from mild ventricular dysfunction to fulminant heart failure, malignant arrhythmias, and conduction block.4,5 Although our patient did not develop major arrhythmias or advanced atrioventricular block, the cardiac findings indicated severe toxin-mediated myocardial involvement that required close monitoring and heart failure management.
The echocardiographic findings in this case are particularly noteworthy. Left ventricular dilatation with global hypokinesia and mildly reduced ejection fraction are consistent with diffuse myocardial toxicity rather than focal ischemic injury. The associated mild-to-moderate mitral regurgitation can reasonably be explained as functional regurgitation secondary to left ventricular dilatation and impaired contractile performance, a mechanism well described in heart failure syndromes.6
Neurological complications of diphtheria are also well documented, although they tend to occur later than respiratory manifestations and may be overlooked during the early phase of treatment.8,9 In this child, progressive symmetrical limb weakness with depressed deep tendon reflexes developed on the fifth hospital day after initial stabilization, while sensation and cranial nerve function remained preserved. This pattern is compatible with diphtheritic peripheral neuropathy, which is believed to result from toxin-mediated demyelinating injury affecting peripheral nerves.8,9 Although nerve conduction studies were not available in our setting, the clinical picture and temporal relationship to severe diphtheria strongly support this diagnosis. The absence of ophthalmoplegia, bulbar dysfunction, and sensory loss suggests a predominantly motor neuropathic process at the time of assessment.
An important strength of this case is the temporal evolution of complications. The child first presented with classical severe respiratory disease, then showed evidence of myocarditis, followed by the later appearance of peripheral neuropathy. This sequence closely reflects the known pathophysiology of diphtheria toxin, in which local infection is followed by systemic dissemination and delayed injury to highly vulnerable tissues, particularly the myocardium and peripheral nerves.4,8,9 The coexistence of both cardiac and neurological complications in such a young child underscores the severity of toxin exposure and highlights the need for continued surveillance even after the airway and pharyngeal findings begin to improve.
Management in this case followed the core principles of severe diphtheria care: isolation, prompt administration of diphtheria antitoxin, antibiotic therapy to eradicate the organism and prevent further toxin production, and aggressive supportive management of organ-specific complications.12 Because antitoxin neutralizes only circulating unbound toxin, its early use is critical and may reduce progression of systemic injury, although it does not reverse established tissue damage.9 The child also received erythromycin, cardiac monitoring, heart failure treatment, physiotherapy, and nutritional support, all of which likely contributed to the favorable short-term outcome. The observed improvement in respiratory status, neurological function, and echocardiographic parameters before discharge reflects the value of early recognition and multidisciplinary supportive care even in a resource-limited environment.
This case also highlights several realities of case management in low-resource settings. Advanced microbiological confirmation, nerve conduction studies, and broader cardiac investigations were not available, yet the diagnosis and treatment decisions had to be made promptly on clinical grounds. Such constraints are common in many settings where vaccine-preventable diseases still persist. For that reason, carefully documented case reports remain valuable, as they provide practical clinical lessons for frontline physicians who must often diagnose and manage severe diphtheria without access to extensive diagnostic tools. In addition, this report reinforces the wider public health message that severe diphtheria continues to occur where immunization gaps remain.1,11,13–15
This case should also be interpreted within the broader Somali context, where prolonged conflict, internal displacement, recurrent climatic shocks, and strained health services continue to affect routine immunization and timely access to care.1 In such settings, children from rural and underserved communities may remain unvaccinated or incompletely vaccinated, increasing their vulnerability to vaccine-preventable infections such as diphtheria. Limited laboratory capacity, delayed referral, and inconsistent access to diphtheria antitoxin may further complicate early diagnosis and treatment. Therefore, this case reflects not only the severe multisystem toxicity of diphtheria but also the wider public-health consequences of persistent immunization gaps in fragile settings.1,2,4,7,9
The patient’s non-immunized status is central to the significance of this case. Diphtheria is largely preventable through routine childhood vaccination, and persistent cases in young children reflect missed opportunities for primary prevention.1,2,11,13 In fragile and underserved settings, interrupted vaccine access, low coverage, and delayed healthcare seeking may combine to increase the risk of severe disease and its complications. This case therefore carries both clinical and public health relevance: it demonstrates not only the multisystem toxicity of diphtheria, but also the consequences of inadequate immunization coverage in vulnerable communities.
This report has some limitations. Microbiological confirmation of Corynebacterium diphtheriae by culture, toxin testing, or polymerase chain reaction was not available at the time of care, and electrophysiological testing for neuropathy could not be performed. Therefore, the diagnosis relied on the characteristic clinical presentation, including an adherent pharyngeal pseudomembrane, bull-neck appearance, non-immunized status, elevated cardiac biomarkers, echocardiographic myocardial dysfunction, subsequent symmetrical motor weakness, and clinical response to treatment. Although the absence of microbiological confirmation limits diagnostic certainty, the overall clinical picture strongly supported severe toxin-mediated diphtheria.1,4
This case emphasizes that diphtheria should still be considered in unvaccinated children presenting with membranous pharyngitis and respiratory distress, especially in low-resource settings. It also demonstrates that myocarditis and peripheral neuropathy may occur sequentially during the same illness and require continued clinical vigilance beyond the initial airway emergency. Early antitoxin administration, antibiotics, close cardiac monitoring, and comprehensive supportive care are essential to improving outcomes, while strengthening routine immunization remains the most effective strategy for preventing such life-threatening presentations.1,12–15
Conclusion
This case highlights the continued clinical importance of diphtheria as a severe but preventable infection among under-immunized children in Somalia. In this non-immunized two-year-old child from a rural community, respiratory diphtheria progressed beyond local airway disease and caused two serious toxin-mediated complications: myocarditis with dilated cardiomyopathy and peripheral neuropathy. The case demonstrates how missed immunization opportunities, delayed presentation, and limited access to timely diagnostic and treatment resources can contribute to severe and avoidable complications.
Early clinical recognition, prompt diphtheria antitoxin administration, appropriate antimicrobial therapy, close cardiac monitoring, and supportive multidisciplinary care remain essential for improving outcomes. In settings where advanced diagnostic tools are limited, clinicians must rely on careful recognition of classical clinical features and early anticipation of systemic complications.
Most importantly, this report reinforces that routine childhood immunization remains the most effective strategy for preventing diphtheria and its severe toxin-mediated complications. Strengthening vaccination coverage, improving outreach to rural and displaced communities, and ensuring early access to care are essential to reducing preventable morbidity and mortality among vulnerable children in Somalia.
Ethics and Consent
Written informed consent for publication of this case report and the accompanying images was obtained from the patient’s parent/legal guardian because the patient was younger than 18 years. Institutional ethical review was waived by Dr. Sumait Hospital/SIMAD University for this single-patient case report because no experimental intervention was performed and no identifiable patient information is disclosed. The waiver documentation is available upon request.
Acknowledgments
This research was supported by SIMAD University, Mogadishu, Somalia. We gratefully acknowledge the Center for Research and Development at SIMAD University for its valuable guidance and insightful recommendations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. Orey FAH, Elmi AH, Farah SA. Breakthrough diphtheria in a fully immunized child in a resource-limited setting: a case report from Somalia. IDCases. 2026;44:e02557. doi:10.1016/j.idcr.2026.e02557
2. World Health Organization. Diphtheria vaccine: WHO position paper. Wkly Epidemiol Rec. 2017;92:417–8.
3. Tiwari TSP, Wharton M. Diphtheria toxoid. In: Plotkin SA, Orenstein WA, Offit PA, editors. Vaccines.
4. Efstratiou A, George RC. Microbiology and epidemiology of diphtheria. Revi Res Med Microbiol. 1996;7(1):31–42.
5. Galazka A. The changing epidemiology of diphtheria in the vaccine era. J Infect Dis. 2000;181(1):S2–9. doi:10.1086/315533. PMID: 10657184.
6. Clarke KEN, MacNeil A, Hadler S, Scott C, Tiwari TSP, Cherian T. Global Epidemiology of Diphtheria, 2000–2017. Emerg Infect Dis. 2019;25(10):1834–1842. doi:10.3201/eid2510.190271. PMID: 31538559; PMCID: PMC6759252.
7. Wagner KS, White JM, Lucenko I, et al. Diphtheria Surveillance Network. Diphtheria in the postepidemic period, Europe, 2000–2009. Emerging Infectious Diseases. 2012;18(2):217–225. doi:10.3201/eid1802.110987
8. Wiedermann BL. Diphtheria in the 21st Century: new Insights and a Wake-up Call. Clin Infect Dis. 2020;71(1):98–99. doi:10.1093/cid/ciz813. PMID: 31425579.
9. Mohanta KD, Parija AC. Neurological complications of diphtheria. Indian J Pediatr. 1974;41(318):237–243. doi:10.1007/BF02829276. PMID: 4426658.
10. Kneen R, Nguyen MD, Solomon T, et al. Clinical features and predictors of diphtheritic cardiomyopathy in Vietnamese children. Clin Infect Dis. 2004;39(11):1591–1598. doi:10.1086/425305. Epub 2004 Nov 8. PMID: 15578357.
11. Samdani S, Jain A, Meena V, Meena CB. Cardiac complications in diphtheria and predictors of outcomes. Int J Pediatr Otorhinolaryngol. 2018;104:76–78. doi:10.1016/j.ijporl.2017.10.032. Epub 2017 Oct 31. PMID: 29287886.
12. Kurdi A, Abdul-Kader M. Clinical and electrophysiological studies of diphtheritic neuritis in Jordan. J Neurol Sci. 1979;42(2):243–250. doi:10.1016/0022-510x(79)90055-8. PMID: 479913.
13. Groundstroem KW, Molnar G, Lumio J. Echocardiographic follow-up of diphtheric myocarditis. Cardiology. 1996;87(1):79–81. doi:10.1159/000177065. PMID: 8631051.
14. Pino PG, Galati A, Terranova A. Functional mitral regurgitation in heart failure. J Cardiovasc Med. 2006;7(7):514–523. doi:10.2459/01.JCM.0000234770.88701.75. PMID: 16801813.
15. Stübgen JP. Drug-induced dysimmune demyelinating neuropathies. J Neurol Sci. 2011;307(1–2):1–8. doi:10.1016/j.jns.2011.05.010. Epub 2011 May 31. PMID: 21621795.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diphtheria with Measles Co-Infection in a Severely Malnourished, Unvaccinated Child: A Case Report from a Resource-Limited Setting
Mohamud KH, Hassan FA, Hussein AM, Mudei NM, Hassan RA, Abdi AA, Muhumed SM
Infection and Drug Resistance 2026, 19:596410
Published Date: 30 March 2026
Severe Antepartum Eclampsia Complicated by Intrauterine Fetal Demise and Pulmonary Edema: A Case Report
Abdulle AM, Hussein AM, Adawe MMM, Ibrahim FH, Mudei NM, Ali HA
International Journal of Women's Health 2026, 18:613673
Published Date: 20 June 2026