Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 16
Severe Hypertensive Response to Atropine Therapy for Bradycardia Associated with Dexmedetomidine: Case Report and Literature Review
Authors Li Y, Gao J, Jiang L, Sun C, Hong H, Yu D
Received 26 September 2023
Accepted for publication 23 December 2023
Published 11 January 2024 Volume 2024:16 Pages 27—31
DOI https://doi.org/10.2147/CPAA.S436188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Yong Li,1 Ju Gao,1 Lin Jiang,2 Canlin Sun,2 Hua Hong,2 Dapeng Yu2
1Department of Anesthesiology, Northern Jiangsu People’s Hospital Affiliated to Yangzhou University, Yangzhou, Jiangsu Province, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu Province, People’s Republic of China
Correspondence: Dapeng Yu, Department of Anesthesiology, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu Province, 225300, People’s Republic of China, Email [email protected]
Abstract: Dexmedetomidine is a selective and potent α2-adrenoceptor agonist used for sedation, analgesia, and anxiolysis, with minimal respiratory depression; therefore, it is widely used in clinical practice. Transient hypertension has been reported to be an indication for the use of dexmedetomidine. The authors report three female patients who experienced hypertensive crisis when used atropine to treat bradycardia caused by dexmedetomidine. The transient hypertension is a relatively common side effect of dexmedetomidine, hypertensive crisis seen with coadministration of atropine is much less frequently reported. This is the first report to describe the use of atropine to treat bradycardia induced by dexmedetomidine, which may cause severe hypertension in female patients. They discuss the reason for and treatment of hypertension caused by administration of atropine and dexmedetomidine together and review the relevant literature.
Keywords: dexmedetomidine, atropine, bradycardia, hypertension
Introduction
Dexmedetomidine is a selective and potent α2-adrenoceptor agonist used for its anxiolytic, sedative, and analgesic properties, with minimal respiratory depression.1 The most common adverse events associated with its use include hypotension, bradycardia, and dry mouth.2 Transient hypertension, which also been reported during the initial phase of infusion, is caused by stimulation of α2-adrenoceptors.1 This usually does not require direct intervention, and simply reducing the infusion rate may be more reasonable. We report three female patients who experienced bradycardia during intravenous (IV) injection of dexmedetomidine during general anesthesia, for which atropine was used to treat ensuing bradycardia, each female patient exhibited resistant, severe hypertension.
Perioperative bradycardia generally refers to a heart rate (HR) <50 beats/min or a decrease in HR to 20% of awake norms. Perioperative hypertension is defined as an increase in blood pressure to >30% of awake norms or systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg. The potential mechanisms underlying hypertension following atropine administration for bradycardia associated with dexmedetomidine infusion remain unclear. The coadministration of IV atropine and dexmedetomidine are suspected to have led to severe hypertension.
Case Descriptions
Case 1
A 43-year-old female, weighing 57 kg, with a maxillary tumor was scheduled for maxillary tumor resection under general anesthesia. She was not taking any medications and her physical examination was unremarkable. She presented in a calm state, with an HR of 69 beats/min, noninvasive blood pressure (NIBP) of 119/70 mmHg (mean arterial pressure [MAP], 86 mmHg), and an oxygen saturation (SpO2) of 100% on room air. An IV bolus of dexmedetomidine (1 µg/kg) was administered over a period of 15 min. Anesthesia induction drugs included lidocaine (100 mg), propofol (75 mg), sufentanil (35 μg), and cisatracurium (10 mg); sufentanil (10 μg) was administered before surgery commenced. Anesthesia maintenance drugs included sevoflurane 1–2.5%, dexmedetomidine 0.25 μg/kg/h, remifentanil 10 μg/kg/h. Five minutes after tracheal intubation, HR exhibited sinus bradycardia (46 beats/min), with a concurrent NIBP of 100/59 (MAP, 73 mmHg), and an SpO2 of 100%. IV administration of atropine (0.5 mg) elicited an immediate HR response to 60, 79, and 85 beats/min at 1, 2, and 5 min, respectively. NIBP and MAP increased to 176/122 and 140 mmHg, respectively. The concentration of sevoflurane was adjusted to 3% and dexmedetomidine infusion was continued. After administration of nitroglycerin (0.5 mg), blood pressure decreased to 163/107 mmHg, with an HR of 79 beats/min. When nitroglycerin (0.5 mg) was administered again, blood pressure decreased further to 142/107 mmHg, with an HR of 72 beats/min. Subsequently, the operation commenced and was completed in 25 min. After a 60 min recovery period, the patient fulfilled discharge criteria and was transferred to the ward with an HR of 62 beats/min and NIBP of 112/82 (MAP, 92 mmHg). No adverse sequelae were noted at discharge or at the 24 h follow-up.
Case 2
A 47-year-old female, weighing 51 kg, with multiple uterine fibroids was scheduled to undergo uterine fibroid resection under general anesthesia. She was not taking any medications and her physical examination was unremarkable. She presented in a calm state, with an HR of 82 beats/min, a respiratory rate (RR) of 16 breaths/min, an NIBP of 110/59 (MAP, 76 mm Hg), and an SpO2 of 98% on room air. After placement of an IV catheter, dexmedetomidine (1 µg/kg) was administered over a 15 min period. Anesthesia induction drugs included lidocaine (100 mg), propofol (75 mg), sufentanil (40 μg), and cisatracurium (10 mg). Anesthesia maintenance drugs included sevoflurane 1–2% and dexmedetomidine 0.5 μg/kg/h. Twenty-five minutes after tracheal intubation, HR exhibited sinus bradycardia (46 beats/min), with a concurrent NIBP of 90/42 mmHg (MAP, 58 mm Hg), and an SpO2 of 100%. IV atropine (0.5 mg) was administered and HR responded within 3 min. Five minutes later, HR was 96 beats/min, with an NIBP of 171/110 mmHg (MAP 130 mmHg). The concentration of sevoflurane was adjusted to 3%, dexmedetomidine infusion was discontinued, and IV labetalol (10 mg) was administered. After repeat administration of IV labetalol (10 mg), blood pressure immediately decreased, but then increased to 130/97 mmHg. Blood pressure was stable until the conclusion of surgery, with HR of 80 beats/min and NIBP of 126/79 mmHg (MAP, 100 mmHg). After a 40 min recovery period, the patient fulfilled discharge criteria and was transferred to the ward with an HR of 79 beats/min and an NIBP of 103/52 mmHg (MAP, 69 mmHg). No adverse sequelae were noted at discharge or at the 24 h follow-up.
Case 3
A 29-year-old female, weighing 53 kg, with acute mastitis was scheduled to undergo local breast resection under general anesthesia. She was not taking any medications and her physical examination was unremarkable. She presented in a calm state, with an HR of 86 beats/min, an RR of 17 breaths/min, an NIBP of 138/79 mmHg (MAP, 99 mmHg), and an SpO2 of 100% on room air. After placement of an IV catheter, dexmedetomidine (1 µg/kg) was infused over a 15 min period. Anesthesia induction drugs included lidocaine (100 mg), propofol (75 mg, sufentanil 40 μg, cisatracurium (15 mg)). Anesthesia maintenance drugs included sevoflurane 1–2%, dexmedetomidine 0.5 μg/kg/h. Five minutes after surgery began, HR exhibited sinus bradycardia at 46 beats/min with a concurrent NIBP of 109/58 (MAP, 75 mmHg), and an SpO2 of 100%. IV atropine 0.5 mg was administered and her HR responded within 3 min. Five minutes later, HR was 120 beats/min, with an NIBP of 178/111 mmHg (MAP, 134 mmHg). The concentration of sevoflurane was adjusted to 3% and 50 mg of IV propofol was administered. After IV administration of neostigmine (0.5 mg), blood pressure decreased to 141/100 mmHg (MAP, 103 mmHg), with an HR of 105 beats/min. Infusion of dexmedetomidine was not discontinued until the conclusion of surgery. Blood pressure continued to decline slowly to 122/69 mmHg (MAP, 87 mmHg), with an HR of 83 beats/min. When all anesthesia drugs were discontinued, HR was 64 beats/min with an NIBP of 104/62 mmHg (MAP, 75 mmHg). After a 25 min recovery period, the patient fulfilled discharge criteria and was transferred to the ward with an HR of 79 beats/min and an NIBP of 103/64 mmHg (MAP, 77 mmHg). No adverse sequelae were noted at discharge or at the 24 h follow-up.
Discussion
Dexmedetomidine is a selective and potent α2-adrenoceptor agonist that has recently gained popularity as an anxiolytic, sedative, and analgesic agent. It has been registered for use in the United States since 1999 and since 2009 in China. It was approved for IV administration for sedation of mechanically ventilated adult patients during surgery. Dexmedetomidine is commercially available as a water-soluble HCl salt, which contains a concentration of dexmedetomidine hydrochloride equivalent to 200 μg/mL dexmedetomidine. According to clinical application guidelines in China, dexmedetomidine hydrochloride is diluted to 4 μg/mL in 0.9% sodium chloride before IV injection. The guidelines recommend an initial infusion rate of 0.5–1 μg/kg, with a loading dose delivered over 10–15 min, followed by titration to the desired effect using a dose range of 0.2–0.5 μg/kg/h while adjusting the concentration of inhaled anesthetic. Dexmedetomidine can cause hemodynamic changes including hypertension and bradycardia.
Hypertension can occur during the initial phase of infusion and last for a short time owing to α2b-receptor activation, which causes vasoconstriction and systemic and pulmonary hypertension.3 Dexmedetomidine causes hypertension at high plasma concentrations and hypotension at lower plasma concentrations, producing a typical biphasic hemodynamic response.3,4 Nevertheless, this initial response can be overcome by stimulation of central α2 adrenoceptors to continue the infusion.5 In clinical practice, the infusion dose is generally reduced to address this situation. The high blood pressure reflex causes bradycardia, and central α2 adrenoceptors prevent the release of norepinephrine, thereby causing bradycardia. This can also be attributed to the combined properties of volatile anesthetics (vasodilation and myocardial depression) and opioids. Therefore, we used atropine to improve HR.
There have been some reports addressing dexmedetomidine-induced hypertension in literature (Table 1). Erkonen et al reported a 2-year-old boy who experienced traumatic brain injury and developed hypertension following dexmedetomidine infusion at 4 µg/kg/h for several hours.6 Shah et al reported a 70 kg 18-year-old male with acute transverse myelitis with severe hypertension and bradycardia after a loading dose of dexmedetomidine for sedation to undergo magnetic resonance imaging.7 Mason et al reported bradycardia in three boys after administering high-dose dexmedetomidine as sedation, which was treated with IV glycopyrrolate (5.0 μg/kg) for cases of marked bradycardia; each child responded to glycopyrrolate with immediate, exaggerated hypertension.8 Kukoyi et al reported two cases of adult female patients who experienced sudden onset of hypertension, tachycardia, agitation, and anxiety after rapid discontinuation of prolonged (5–7 days) infusions of dexmedetomidine in the intensive care unit.9 Muthiah et al reported a case involving a 34-year-old male patient who was scheduled to undergo general anesthesia with a conscious fiber-guided nasotracheal tube because of a fractured mandible. The initial infusion rate of 1 µg/kg/h dexmedetomidine was used as the loading dose for 20 min. The patient’s blood pressure progressively increased from 128/86 mmHg to 200/110 mmHg, and he complained of severe headache.10
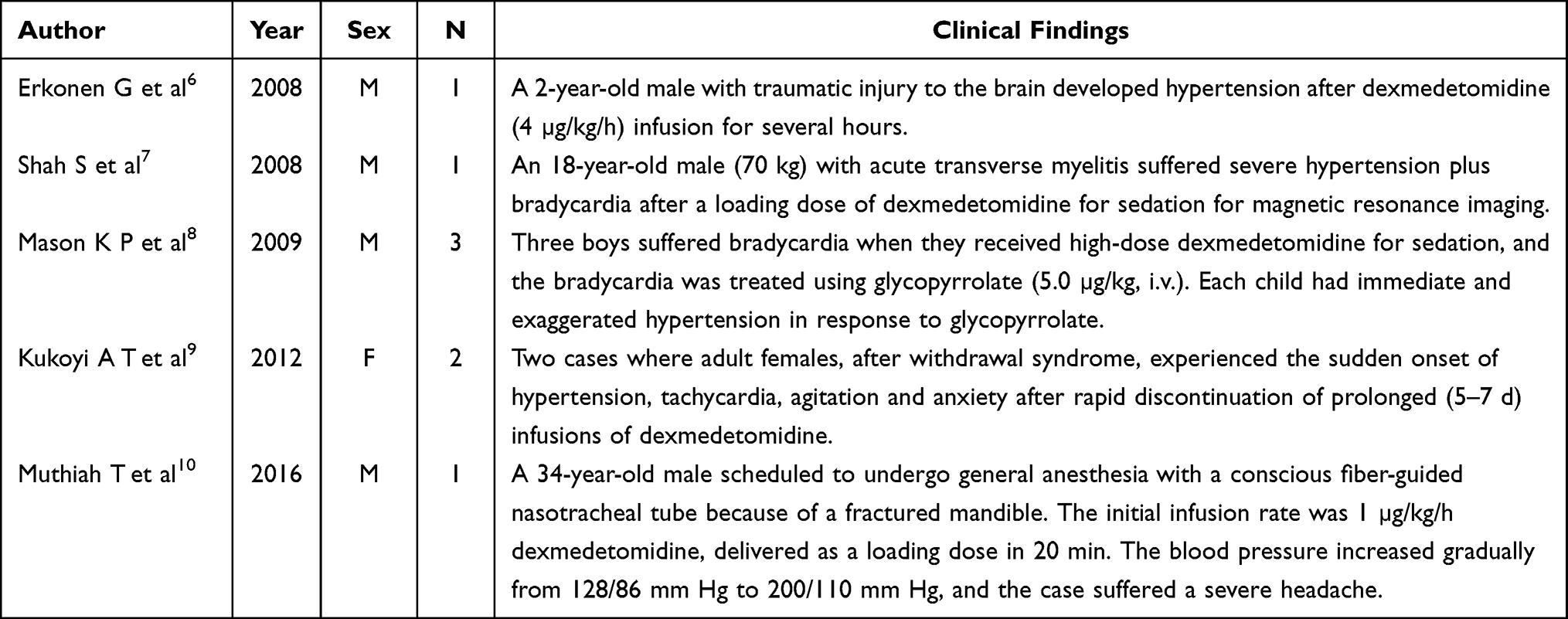 |
Table 1 Overview of Published Dexmedetomidine-Induced Hypertension |
We analyzed the similarities among the patients described in the present article to determine the underlying mechanisms. All patients were female, all of whom were administered a bolus infusion of dexmedetomidine (1 µg/kg) for 15 min. Severe hypertension did not occur during the initial phase of infusion, but did occur after surgery commenced. After administration of atropine, the patients experienced severe hypertension. Other studies have reported that cases usually occur in occidental males, except in the study by Kukoyi et al. We found that only female patients experienced severe hypertension after a loading dose of dexmedetomidine, and other anesthesiologists have previously reported similar situations in virtually all female patients. Not all patients experience hypertension in their daily lives.
To our knowledge, this is the first report to describe the use of atropine to treat bradycardia induced by dexmedetomidine, which may cause severe hypertension in female patients. Why are females more prone to this situation? Flieller et al11 reported that a history of hypertension and shorter weaning duration appear to be associated with an increased risk for rebound hypertension with discontinuation of dexmedetomidine. In a study investigating hypertension after discontinuation of dexmedetomidine infusion, Salah et al12 reported that a medical history of hypertension was the only independent risk factor for hypertension or tachycardia with discontinuation. The patients in the present study had no history of hypertension.
Resistant and severe hypertension is not a stress response caused by surgical stimulation, and increasing the concentration of inhaled anesthetic did not change this situation; moreover, we used sufficient analgesic drugs. We observed that after atropine was administered, HR accelerated and blood pressure increased significantly. Hence, we believe that atropine administration for bradycardia associated with dexmedetomidine infusion may induce resistant and severe hypertension.
Bolus administration of dexmedetomidine with a high plasma concentration3,4 results in α2b-receptor activation in the vascular smooth muscles, causing peripheral vasoconstriction and hypertension. As with the initial high plasma concentrations after an IV bolus, higher maintenance doses are associated with progressive increases in MAP.3 Together with presynaptic α2-adrenoreceptors, they inhibit the sympathetic release of catecholamines and increase vagal activity. These hypotensive effects overcome hypertensive effects, resulting in hypotension. Atropine is an anticholinergic alkaloid that acts as an antiarrhythmic, preanesthetic to reduce secretion, and a cholinesterase inhibitor. IV atropine has been reported to significantly increased HR, MAP, and cardiac output.13,14 Atropine and dexmedetomidine work synergistically, and the hypertensive effects overcome the hypotensive effects causing high blood pressure but not only through dexmedetomidine alone. Similar to Mason et al,8 who treated bradycardia using IV glycopyrrolate for bradycardia caused by dexmedetomidine, each child responded to immediate exaggerated hypertension.
In conclusion, the increase in arterial blood pressure observed in our patients after atropine administration was presumably secondary to an HR-induced increase in cardiac output in the setting of elevated systemic vascular resistance due to the sustained effect of higher concentrations of dexmedetomidine on the α2-receptors in the peripheral vascular smooth muscles.
It is crucial to carefully choose the appropriate treatment drugs for hypertension caused by atropine and dexmedetomidine. When we encountered this situation for the first time, we chose to increase the concentration of inhaled anesthetics and nitroglycerin; however, the effect of this strategy on reducing blood pressure was not favorable. Currently, we know that hypertension following dexmedetomidine administration is caused by α2-adrenoceptor stimulation, and atropine increases cardiac output; therefore, the use of α-adrenoceptor blockers should be a reasonable choice. We chose labetalol, a combined α- and β-blocker, to treat hypertension and control blood pressure.10 The pure α-blocker phentolamine appears to be a reasonable choice for treating such cases. It should be noted that the administration of a selective β-blocker will result in no antagonistic α-receptor stimulation, which may worsen hypertension. It is interesting that we used a small dose of IV neostigmine (0.5 mg) and controlled blood pressure while slowing HR; however, more attention should be devoted to monitoring muscle relaxation and airway secretions. Neostigmine is a cholinesterase inhibitor that is used as a standard drug to reverse the effects of muscle relaxants at the conclusion of surgery. It indirectly increases acetylcholine levels, which are mediated via muscarinic receptors, leading to bradycardia and hypotension.15 Neostigmine is very effective in this situation because it slows HR and reduces heart output, which offsets the effects of atropine. Fortunately, all patients described in this article returned to the ward, and no adverse sequelae were noted at discharge or at the 24 h follow-up.
Based on our experience, we recommend infusion of low-dose dexmedetomidine under general anesthesia. We recommend to treat bradycardia caused by dexmedetomidine with low-dose atropine or use other drugs, such as ephedrine. Once atropine and dexmedetomidine induced hypertension, infusion of dexmedetomidine was discontinued, and the appropriate antihypertensive drugs were carefully chosen.
Patient Informed Consent to Publish
The patients gave the consents for the Material about them/the patients to appear in a publication. The case details can be publish without institutional approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors do not have any possible conflicts of interest.
References
1. Belleville JP, Ward DS, Bloor BC, et al. Effects of intravenous dexmedetomidine in humans. I. Sedation, ventilation, and metabolic rate. Anesthesiology. 1992;77(6):1125–1133. doi:10.1097/00000542-199212000-00013
2. Ahmed S, Murugan R. Dexmedetomidine use in the ICU: are we there yet? Crit Care. 2013;17(3):320. doi:10.1186/cc12707
3. Ebert TJ, Hall JE, Barney JA, et al. The effects of increasing plasma concentrations of dexmedetomidine in humans. J Am Soc Anesthesiologists. 2000;93(2):382–394.
4. Bloor BC, Ward DS, Belleville JP, Maze M. Effects of intravenous dexmedetomidine in humans. II. Hemodynamic changes. Anesthesiology. 1992;77(6):1134–1142. doi:10.1097/00000542-199212000-00014
5. Kaur M, Singh PM. Current role of dexmedetomidine in clinical anesthesia and intensive care. Anesthesia. 2011;5(2):128.
6. Erkonen G, Lamb F, Tobias JD. High-dose dexmedetomidine-induced hypertension in a child with traumatic brain injury. Neurocritical Care. 2008;9(3):366. doi:10.1007/s12028-008-9102-y
7. Shah S, Sangari T, Qasim M, et al. Severe hypertension and bradycardia after dexmedetomidine for radiology sedation in a patient with acute transverse myelitis. Pediatr Anesthesia. 2008;18(7):681–682. doi:10.1111/j.1460-9592.2008.02521.x
8. Mason KP, Zgleszewski S, Forman RE, et al. An exaggerated hypertensive response to glycopyrrolate therapy for bradycardia associated with high-dose dexmedetomidine. Anesthesia Analg. 2009;108(3):906–908. doi:10.1213/ane.0b013e3181948a6f
9. Kukoyi AT, Coker SA, Lewis LD, et al. Two cases of acute dexmedetomidine withdrawal syndrome following prolonged infusion in the intensive care unit Report of cases and review of the literature. Hum Exp Toxicol. 2012;32(1):107–110.
10. Muthiah T, Moni A, Mathews L, et al. Intravenous labetolol in treating hypertensive crisis following dexmedetomidine infusion for procedural sedation. J Clin Anesth. 2016;29:30–32. doi:10.1016/j.jclinane.2015.10.011
11. Flieller LA, Alaniz C, Pleva MR, et al. Incidence of rebound hypertension after discontinuation of dexmedetomidine. Pharmacotherapy. 2019;39(10):970–974. doi:10.1002/phar.2323
12. Salah J, Grgurich P, Nault K, et al. Identification of risk factors for hypertension and tachycardia upon dexmedetomidine discontinuation. J Crit Care. 2020;59:81–85. doi:10.1016/j.jcrc.2020.06.006
13. Wajima Z, Shiga T, Imanaga K. Does intravenous atropine affect stroke volume variation in man? Acta Anaesthesiologica Taiwanica. 2015;53(3):85–88. doi:10.1016/j.aat.2015.06.002
14. Congdon JM, Marquez M, Niyom S, et al. Evaluation of the sedative and cardiovascular effects of intramuscular administration of dexmedetomidine with and without concurrent atropine administration in dogs. J Am Vet Med Assoc. 2011;239(1):81–89. doi:10.2460/javma.239.1.81
15. Hunter JM, Flockton EA. The doughnut and the hole: a new pharmacological concept for anaesthetists. Br J Anaesth. 2006;97(2):123–126. doi:10.1093/bja/ael158
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.