Back to Journals » Infection and Drug Resistance » Volume 16
Severe Hemoptysis Secondary to Actinomycosis: A Case Report
Authors Zhao X ![]() , Huang J, Wang L, Guo C, Di J, Xiong Y
, Huang J, Wang L, Guo C, Di J, Xiong Y ![]() , Huang W, Ma J, Wang G
, Huang W, Ma J, Wang G ![]()
Received 18 March 2023
Accepted for publication 9 May 2023
Published 12 May 2023 Volume 2023:16 Pages 2933—2937
DOI https://doi.org/10.2147/IDR.S410499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiang Zhao,1 Junfang Huang,1 Lina Wang,1 Cuiyan Guo,1 JiTing Di,2 Yan Xiong,2 Weiming Huang,3 Jing Ma,1 Guangfa Wang1
1Department of Respiratory and Critical Care Medicine, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Pathology, Peking University First Hospital, Beijing, People’s Republic of China; 3Department of Thoracic Surgery, Peking University First Hospital, Beijing, People’s Republic of China
Correspondence: Junfang Huang, Department of Respiratory and Critical Care Medicine, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel +86 13466716682, Email [email protected]
Abstract: Pulmonary actinomycosis (PA) is an uncommon, asymptomatic, and frequently misdiagnosed pulmonary infectious illness. Our patient remained undiagnosed despite extensive regular and invasive testing, significant intermittent hemoptysis, and repeated bronchial artery embolization. Ultimately, a left lower lobectomy was performed via video-assisted thoracoscopic surgery, and a histopathological examination revealed an actinomycete infection.
Keywords: actinomycosis, hemoptysis, bronchoscopy
Introduction
Actinomycosis is a rare, invasive infection caused by Actinomyces, a gram-positive, facultatively anaerobic bacterium.1 Pulmonary actinomycosis (PA) has nonspecific symptoms, physical indicators, and radiological abnormalities, and its diagnosis is frequently delayed or misdiagnosed as tuberculosis, lung cancer, lung abscess, or nocardiosis. Large hemoptysis is a rare life-threatening complication of pulmonary actinomycosis associated with the risk of asphyxia and haemodynamic instability. The majority of cases require arterial embolism and surgical treatment.2,3 There are few accounts of PA accompanied by extensive hemoptysis and its subsequent treatment. We describe a rare case of massive hemoptysis secondary to PA. The patient had massive, recurrent hemoptysis of unknown cause. After arterial embolism, massive hemoptysis occurred again, with a total hemoptysis volume of more than 2000 mL, and the patient underwent emergency video-assisted thoracic surgery (VATS). Histopathological examination revealed an actinomycete infection.
Case Report
A 45-year-old man visited our hospital on May 12, 2021, due to hemoptysis with a four-month duration. The patient had a history of hypertension, diabetes, lipid metabolism disorders and coronary heart disease. In 2019, he experienced sudden cardiac death and required endotracheal intubation and tracheotomy, but he survived; the patient had a higher limb muscle tone and minor cognitive impairment after taking aspirin for a long time. Four months prior, he experienced recurrent bouts of blood-tinged sputum. Laboratory parameters were within the normal limits. Computed tomography (CT) scans showed consolidation of the outer basal segment of the left lung’s lower lobes and a few cord shadows surrounding it. The results of the clinical examination were inconclusive. He was admitted to a local hospital for a trial of antibiotics and hemostasis, and his condition quickly improved.
He subsequently visited our hospital for recurrent hemoptysis and deterioration and ceased taking aspirin. On admission, his physical symptoms were normal. The white blood cell count was 10.4 ×109/L, the percentage of neutrophils was 78%, the C-reactive protein level was 15 mg/L, and the procalcitonin level was 0.03 ng/mL. The serology for HIV was negative. Chest CT showed consolidation of the outer basal segment of the left lower lobe, measuring 2.8 ×3.0× 3.5 cm (Figure 1A and B). To stop the haemorrhage, bronchial artery embolization was performed, and the patient was treated with intravenous phentolamine, tranexamic acid, and haemagglutin. The tumour markers (CEA, CYFRA21-1, SCC, NSE, proGRP) were normal. Additional tests were performed, including the T-cell spot test for tuberculosis infection, cryptococcal antigen tests, G-tests, galactomannan antigen detection tests, extractable nuclear antigen tests, and anti-neutrophil cytoplasmic antibody tests, which were within the normal limits. Antinuclear antibody positivity was 1:100. For diagnosis, bronchoscopy with R-EBUS, bronchial brushing (BB), a transbronchial biopsy (TBB), and bronchial washing were performed. The specimens were sent to the lab and pathologist as soon as possible; however, the results of the pathological examination only showed inflammation and a small amount of necrosis in the bronchial mucosa, with no indication of malignancy. Moreover, conventional cultures for bacterial, fungal, and tuberculosis infection were all negative. He underwent a second bronchial artery embolization for massive hemoptysis (approximately 400 mL) on June 12, 2021. Persistent hemoptysis led to repeat chest CT, which revealed a reduced consolidation lesion measuring 2.0 cm × 2.6 cm × 3.0 cm, with ground glass density foci and cords surrounding the lesion (Figure 1C and D). We considered that the lesion was complicated with bacterial infection and administered amoxicillin clavulanate potassium orally.
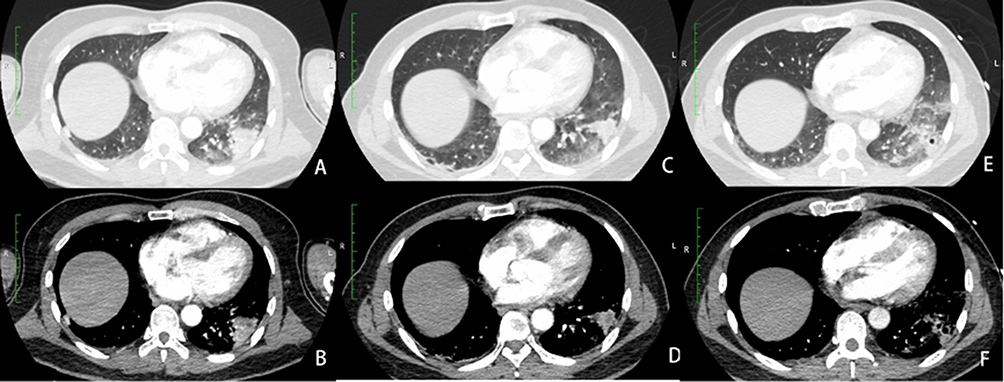 |
Figure 1 (A and B) Chest CT showed consolidation of the outer basal segment of the left lower lobe, measuring 2.8×3.0× 3.5 cm, (C and D) Chest CT showed a reduced consolidation lesion measuring 2.0 cm × 2.6 cm × 3.0 cm, with ground glass density foci and cords surrounding the lesion, (E and F) Chest CT showed an increase in the size of consolidation to 2.0 cm × 2.7 cm × 3.1 cm and bilateral ground-glass opacities. |
Hemoptysis recurred on June 29. The patient had intermittent bouts of massive hemoptysis (>150 mL) every few hours, and intravenous injection of hemostatic drugs was ineffective. The third bronchial artery embolization showed no bleeding. On July 6, 2021, the patient experienced extensive hemoptysis, which was voluminous, and bright red; the estimated volume of blood was 700 mL. CT showed an increase in the size of consolidation to 2.0 cm × 2.7 cm × 3.1 cm and bilateral ground-glass opacities (Figure 1E and F). Bronchoscopy revealed the presence of old blood clots in the upper and lower left lungs, as well as scattered evidence of recent blood in the trachea. We decided to perform emergency VATS. The left lower lung was resected. The patient did not have hemoptysis after the operation and was given meropenem, which was degraded to ceftriaxone. Histopathology revealed a grey‒white area with a range of 1.8×1.5×1.3 cm in the gross lung tissue, bronchiectasis in the lung, disintegration of the tube wall, and acute inflammatory exudate in the lumen. Under a microscope, chrysanthemum shapes in the lumen and dense centres of intertwined, branched hyphae surrounded by radially-arranged eosinophilic long hyphae were observed; Glan staining was positive, and epithelioid cells surrounded the granules, macrophages, lymphocytes, and other inflammatory cells, which were positive for hexamine silver and Periodic Acid-Schiff stain (Figure 2). The final diagnosis was pulmonary actinomycosis. His condition was stabilized with oral amoxicillin following discharge. He has remained in a stable condition for a year while receiving routine follow-up.
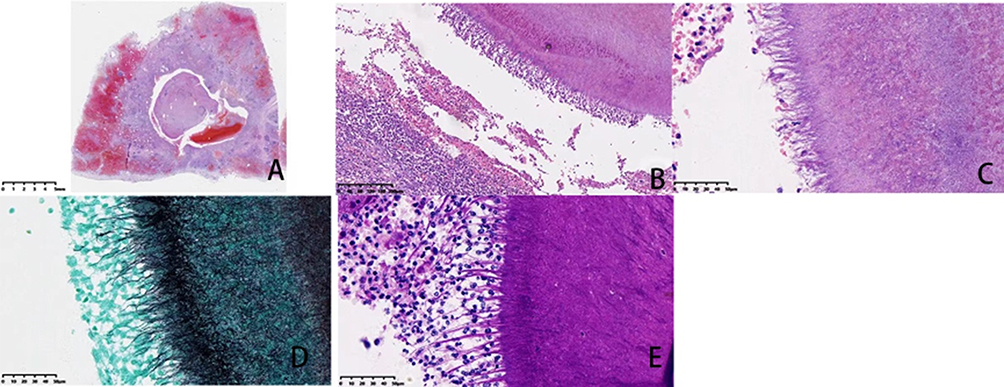 |
Figure 2 (A-E) Lobectomy histopathology images showing (A) the original magnification, 0.4×, (B) the original magnification, 10×, (C) the original magnification, 40×, and (D and E) Gomori methenamine silver and periodic acid-Schiff stain positivity of the bacterial colonies. |
Discussion
Actinomycosis is extremely rare, and hemoptysis as a presenting sign is even more uncommon. The total volume of hemoptysis in our patient exceeded 2000 mL. Actinomycosis is a subacute, asymptomatic, chronic bacterial infection with contiguous tissue spread, suppurative and granulomatous inflammation, and numerous abscesses and sinuses releasing sulphur granules.1,4,5 Sulphur granules in sputum are regarded as a defining feature of PA; however, they are uncommon in clinical practice. The clinical presentations of this disease were nonspecific. The primary symptoms included cough, fever, sputum, hemoptysis, chest pain, etc., which are also characteristic of other respiratory diseases.2,3 Hemoptysis was more common in patients with pulmonary comorbidities (71.3%) than in patients without pulmonary comorbidities (56.3%).6 In cases of PA, it is common to find masses, nodules, cavities, patchy or solid shadows, interlobular septal thickening, bronchiectasis, mediastinal lymphadenopathy, adjacent pleural thickening, pleural effusion, and empyema. Some of these can even coexist in the same patient’s lung.7–9 A localized consolidation of the lungs may be accompanied by pulmonary nodules in the early stages of the disease, but there are usually no associated symptoms.1 Bacterial culture is generally accepted as the gold standard for diagnosing infections; nevertheless, only 10%-20% of cases show positive cultures due to the anaerobic nature and slow reproduction.1,10 In most cases, PA is diagnosed based on histopathology, making the diagnosis challenging.
Our patient had no known risk factors for PA, such as poor oral hygiene, preexisting dental disease, and alcoholism.1 However, our patient had a history of sudden cardiac death and endotracheal intubation and increased muscle tone and may have had unrecognized coughing and aspiration. Our patient’s primary symptom was intermittent hemoptysis, and he never had a fever during his illness. The cultures for sputum and BAF bacterial, TB, and fungal infections were negative. Due to the ground-glass shadow surrounding the CT lesion, we suspected an infection and administered amoxicillin and clavulanate potassium; nevertheless, the patient continued to experience hemoptysis while on these medications. This may be a result of an inadequate antibiotic administration duration and dosage, as well as existing vascular damage. PA was diagnosed after the left lower lobe of the lung was surgically resected.
Despite a lack of knowledge about the pathogenic mechanisms of Actinomyces, it has been hypothesized that the invasion of ruptured or necrotic tissue is the initial step in the organism’s penetration and proliferation in deeper bodily structures.1 Actinomycetes are able to grow gradually and consistently through anatomical boundaries. Similar to our patients, if the disease spreads to the arteries, life-threatening consequences such as major hemoptysis may develop. It is unclear how much this propensity to spread is attributable to the proteolytic enzymes of the bacterium. The disease can cause damage to the pleura, chest wall, soft tissues, and skeletal structures if left untreated.9
It is common for patients with PA to receive prolonged high doses of beta-lactam antibiotics, including penicillin G, cephalosporin, or amoxicillin. Due to avascularity and dense coaggregations of actinomyces, this rigorous treatment is likely necessary because of the poor penetration of the medication.9,11 A recent study has shown that patients receiving surgical treatment have a better prognosis, so surgical treatment is recommended for patients with complex PA (hemoptysis), patients who do not respond well to high-dose penicillin treatment, and patients for whom a cancer diagnosis is explicitly excluded. Surgery is regarded as an important adjunct option for patients suffering from recurrent or life-threatening hemoptysis, those with an unclear cancer diagnosis, or those with the potential need for complication management.11
Conclusion
The lack of specificity of clinical symptoms and radiological alterations may pose a diagnostic challenge. Patients with hemoptysis unaccounted for by other causes should be suspected of actinomycosis. The presence of sulphur particles in the purulent material of the infected tissue, a positive culture result, correlation with radiological and clinical characteristics, and a positive response to antibiotic therapy are all necessary for diagnosis. Our patient has a difficult diagnosis process, suggesting that actinomycosis should be suspected in patients with unexplained hemoptysis.
Data Sharing Statement
The data used and analysed in this study are available from the corresponding author upon reasonable request.
Statement of Ethics
This case study followed the international CARE guidelines. According to national norms, this study did not need ethical approval. The patient’s written informed consent was obtained before this case report and any related photographs were published.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; drafted, revised or critically reviewed the article; approved the final version of the manuscript; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183–197. doi:10.2147/idr.S39601
2. Huang MX, Ye B, Jiang Y, Tang LF, Chen ZM. 儿童肺放线菌病一例并文献复习 [Pulmonary actinomycosis in children: a case report and literature review]. Zhonghua Er Ke Za Zhi. 2021;59(1):33–36. Chinese.doi:10.3760/cma.j.cn112140-20200430-00453
3. Xu YY, Zhang J, Lu AL, Peng J, Xu XW. Clinical features of actinomycosis: a 20-year experience of a single institute in Southern China. J Mycol Med. 2021;31(3):101169. doi:10.1016/j.mycmed.2021.101169
4. de Montpréville VT, Nashashibi N, Dulmet EM. Actinomycosis and other bronchopulmonary infections with bacterial granules. Ann Diagn Pathol. 1999;3(2):67–74. doi:10.1016/s1092-9134(99)80032-x
5. Venkatnarayan K, Raj R, Krishnaswamy UM, et al. A 51-year-old woman with pellets in the sputum. Chest. 2020;157(2):e25–e29. doi:10.1016/j.chest.2019.09.037
6. Kim SR, Jung LY, Oh IJ, et al. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis. 2013;13:216. doi:10.1186/1471-2334-13-216
7. Han JY, Lee KN, Lee JK, et al. An overview of thoracic actinomycosis: CT features. Insights Imaging. 2013;4(2):245–252. doi:10.1007/s13244-012-0205-9
8. Chew SY, Tan CS, Puan Y, Koh JMK. A 78-year-old man with recurrent hemoptysis and persistent pulmonary nodule. Chest. 2020;157(3):e79–e84. doi:10.1016/j.chest.2019.10.046
9. Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003;21(3):545–551. doi:10.1183/09031936.03.00089103
10. Karadeniz G, Polat G, Ucsular F, Yalnız E. A difficult disease to diagnosis: pulmonary actinomycosis. Clin Respir J. 2020;14(4):416–418. doi:10.1111/crj.13136
11. Song JU, Park HY, Jeon K, Um SW, Kwon OJ, Koh WJ. Treatment of thoracic actinomycosis: a retrospective analysis of 40 patients. Ann Thorac Med. 2010;5(2):80–85. doi:10.4103/1817-1737.62470
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.