Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Severe COPD Exacerbators Requiring Multiple ICU Admissions Over Time: Insights of a French Cohort
Authors Ferré A ![]() , Sahki N
, Sahki N ![]() , Puechoultres P, Diop S
, Puechoultres P, Diop S ![]() , Abi-Abdallah G
, Abi-Abdallah G ![]() , Legriel S
, Legriel S ![]()
Received 30 March 2026
Accepted for publication 4 June 2026
Published 18 June 2026 Volume 2026:21 613270
DOI https://doi.org/10.2147/COPD.S613270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Zijing Zhou
Alexis Ferré,1 Nassim Sahki,2 Pauline Puechoultres,1 Sylvain Diop,3 Georges Abi-Abdallah,4,5 Stéphane Legriel1,6
1Intensive Care Unit, Versailles Hospital, Le Chesnay, France; 2DRCI, Versailles Hospital, Le Chesnay, France; 3Department of Anesthesiology and Intensive care, Marie Lannelongue Hospital, Le Plessis Robinson, France; 4Department of Anesthesiology and Critical Care, Hôpital Européen Georges Pompidou, APHP, Paris, France; 5IThEM, INSERM, Université de Paris Descartes, Paris, France; 6CESP, INSERM, Université Paris-Saclay et UVSQ, Villejuif, France
Correspondence: Alexis Ferré, Intensive Care Unit, Versailles Hospital, 177 Rue de Versailles, Le Chesnay, 78150, France, Email [email protected]
Introduction: Data on COPD patients who experience multiple intensive care unit (ICU) admissions for severe acute exacerbations (AECOPD) are scarce. We aimed to describe and compare patients’ characteristics by recurrent admission status and to identify factors associated with recurrent ICU-level exacerbations.
Methods: We conducted a single-centre, retrospective cohort study including all patients admitted to our ICU between 2015 and 2022 for a severe AECOPD. Patients with more than one ICU admission during the study period were classified as “recurrent exacerbator” phenotype. Multivariable regression and competing-risk models were used.
Results: We included 328 patients who had a total of 445 admissions. Seventy-two (22.0%) patients had multiple ICU admissions. Compared with non-recurrent patients, recurrent exacerbators were younger (median 67 vs 70 years, p=0.037), had a lower prevalence of impaired Performance Status (13.9% vs 25.8%, p=0.035), and had higher blood eosinophil counts (0.06 vs 0.04 G/L, p=0.025). One-year mortality was similar between groups (18.1% vs 18.4%, p=0.95). In multivariate model, factors independently associated with recurrent severe exacerbation were long-term oxygen therapy (HR = 1.79, p=0.045) and initial blood eosinophil count (HR per +0.1 G/L = 1.10, p< 0.001). A Performance Status ≥ 3 was inversely associated with recurrence (HR per point = 0.41, p=0.030).
Conclusion: Patients with recurrent ICU admission for severe COPD exacerbations were younger and had higher blood eosinophil counts than those with a single admission. These findings may suggest that phenotyping—including blood eosinophils—could help stratify the risk of recurrent severe exacerbations and personalised treatment.
Keywords: COPD, exacerbation, mortality, exacerbator, phenotype
Background
Patients with chronic obstructive pulmonary disease (COPD) frequently experience acute exacerbations (AECOPD) with worsening of symptoms requiring temporary escalation of treatment. In the most severe cases, exacerbations may require intensive care unit (ICU) admission and ventilatory support.1 Mortality following such exacerbations remains high, with reported rates around 25% at 3 months.2
Several COPD phenotypes have been identified such as emphysema, systemic inflammation, eosinophilic inflammation and frequent exacerbator phenotypes.3–8 Over the last two decades, the frequent exacerbator phenotype has received scientific attention as exacerbations play a crucial role in the disease progression by accelerating the decline of the lung function, altering quality of life, and worsening survival prognosis.9–13 The real incidence of AECOPD is difficult to assess because of self-management unreported episodes.14 Factors associated with exacerbation are well studied and included previous episode of exacerbation, severity of COPD, comorbidities, and presence of chronic bronchitis.13,14 For an AECOPD leading to hospital, the overall mortality rate is around 12% which increases up around 40% in patients who required readmission for a subsequent episode.15
However, data regarding severe exacerbator phenotype leading to ICU or recurrent ICU admissions remain scarce. Yet, there is no data on patients admitted several times in ICU for severe life-threatening COPD exacerbations. Understanding the pathogenesis, clinical and biological characteristics and phenotyping recurrent severe COPD exacerbators could help to develop targeted clinical approaches and improve patient care. This may have direct implications for treatment strategies and prognosis, in terms of precision medicine to find an approach that could reduce future ICU admissions.
In this study, our aims were to compare patient clinical and biological characteristics according to recurrent ICU admission for severe AECOPD, to evaluate the impact on management and outcomes, and to identify factors associated with the severe ICU recurrent exacerbator phenotype of patients which lead to subsequent ICU admissions.
Study Design and Methods
This monocentric, observational, retrospective human study adhered to the Declaration of Helsinki and French regulations. It was approved by ethic committee of the French Intensive Care Society-FICS (N°#21-66) and the protocol was registered at the French National Institute for Health Data (#MR2516271119). Upon recovery, according to French legislation and regulations, oral informed consent was sought from the patients including a written form of objection in case of refusal to participate. The verbal informed consent process was approved by the FICS ethic committee. The study complies with the STROBE statement on guidelines for publishing observational studies.
Patient and Public Involvement
Patients and members of the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Patients
We screened all ICU patients with known COPD admitted between January 2015 and October 2022. We included in the study patients over 40 years of age admitted for a first severe AECOPD which was defined by the presence of acute respiratory failure and/or hypercapnic acidosis requiring ICU admission. We excluded patients admitted to the ICU with known asthma diagnosis according to international definition and patient refusal to participate.
The ICU management of patients admitted for severe AECOPD in our study has been described in a previous publication related to this cohort.16 It followed good clinical practices, international and French guidelines for non-invasive ventilation (NIV), invasive mechanical ventilation (MV), antibiotics, systemic steroids, and inhaled bronchodilators.17,18
The two groups of patients were defined according to the number of ICU admissions for severe AECOPD during the study period: patients with multiple occurrences were named “recurrent exacerbator phenotype” whereas patients with only one occurrence were named “non-recurrent exacerbator phenotype”. We compared these 2 groups of patients. Only the data of the first admission have been taken into account for the group of recurrent exacerbators. After analysing medical records, we excluded early ICU readmission (<30 days) considered as a relapse of the index COPD exacerbation episode. Deaths in ICU were excluded and so patients who had a decision of non-ICU-readmission after their discharge as they could not have, per se, a second ICU occurrence.
Data Collection
As we described it previously,19 data collection included demographics and COPD characteristics (COPD classification according to ambulatory or hospital pulmonologist medical record and/or the last available spirometry data before ICU admission); pre-admission baseline Performance Status (PS); chronic comorbidities; exacerbation triggers; Simplified Acute Physiology Score II (SAPS II); physiological and laboratory parameters at ICU admission; ventilatory support (standard oxygen, NIV, and invasive MV); ICU and hospital lengths of stay; and mortality at predefined time points. For each patient, the follow-up ended at last news listed in the hospital electronic medical records. Mortality was assessed using the same procedure, and we consulted the French national register of deaths via the INSEE’s (National Institute of Statistics and Economic Studies) open-access database.
Statistical Analysis
Patient characteristics at ICU admission are described overall and according to exacerbator phenotype. Quantitative variables are summarized as median and interquartile range (IQR), as the vast majority of variables showed asymmetric and did not satisfy normality distribution, often with extreme values. Categorical variables as counts and percentages. Missing data are reported for each variable. To ensure consistency and uniformity in statistical comparisons, quantitative variables were compared between groups using the Mann–Whitney–Wilcoxon test. Comparisons of categorical variables were performed using the χ2-test or Fisher’s exact test, as appropriate.
Time to second ICU admission for severe acute exacerbation is analyzed from the date of the index ICU admission. Because death precludes recurrence, cumulative incidence functions are estimated using the Fine–Gray competing-risk approach, considering death as a competing event. Stratified cumulative incidence curves are compared using Gray’s test according to clinically relevant covariates. Factors associated with recurrence are first explored in univariate analyses. Variables with p < 0.05 in univariate analysis and those considered clinically relevant are entered into a multivariable Fine–Gray regression model, and results are expressed as subdistribution hazard ratios (HR) with 95% confidence intervals (CI).
Overall survival is estimated using the Kaplan–Meier method from the date of ICU admission to last follow-up, and survival curves are compared between groups using the Log rank test.
All statistical analyses are performed using R© (version 2024.09.0+375). A two-sided p-value < 0.05 is considered statistically significant.
Results
Patient Characteristics
Figure 1 is the patient flowchart and Table 1 reports patients characteristics at ICU admission. During the study period, we noted 445 cases of COPD exacerbation for 328 patients, of whom 214 (65.2%) were male, with a median age of 69 (IQR, 62–76) years. The GOLD stage (1 to 4) was known for 261 (79.6%) patients and was ≥3 for 176 (67.4%) patients. The baseline Performance Status (PS) score was altered (scores 3 and 4) for 76 (23.2%) patients. Eighty-one (24.7%) patients were on long-term oxygen therapy at home and 37 (11.3%) patients were on chronic homecare non-invasive ventilation (NIV).
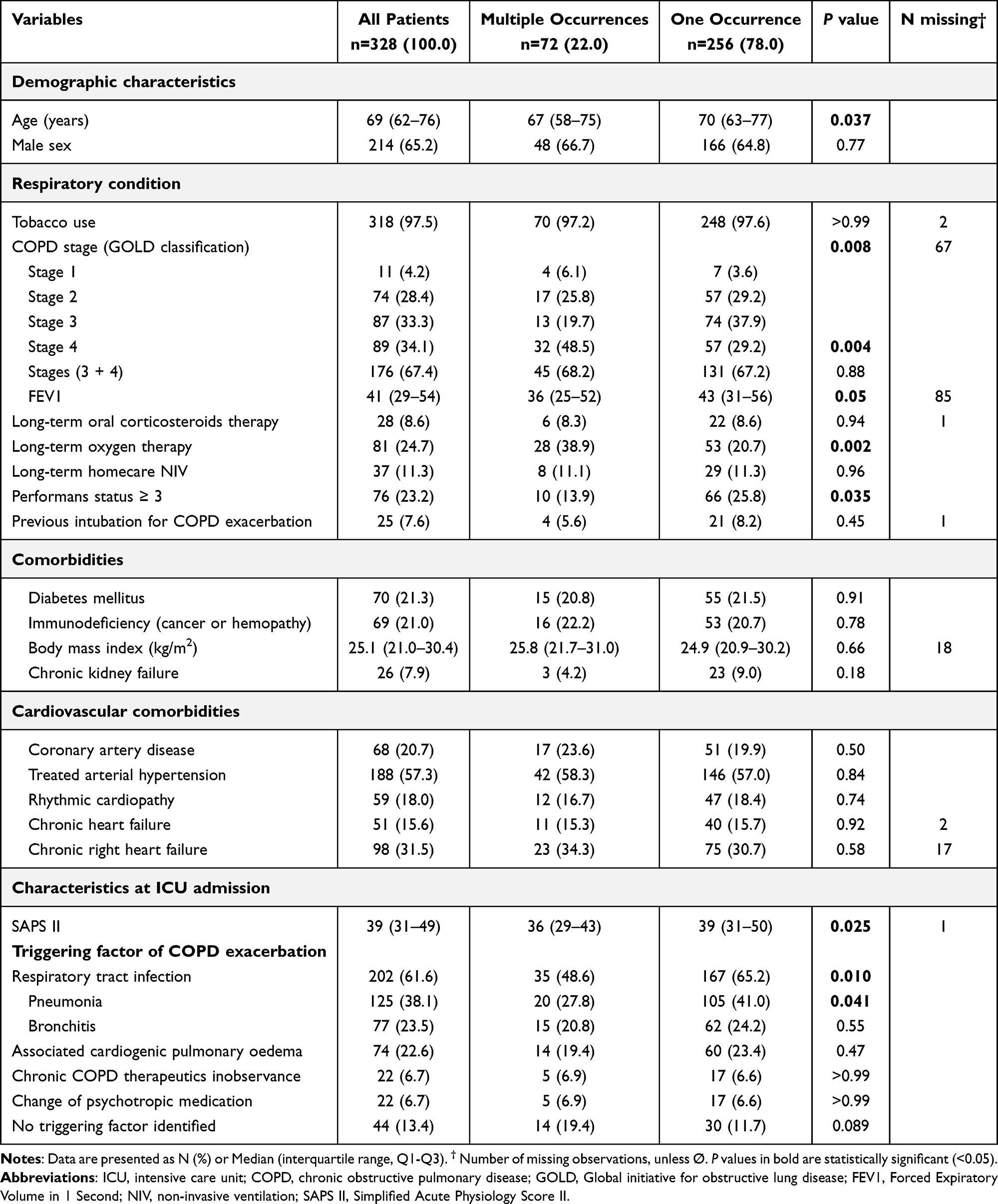 |
Table 1 Baseline and ICU Characteristics in Patients Admitted for a Severe Acute Exacerbation of COPD According to the Number of Patients ICU Occurrences |
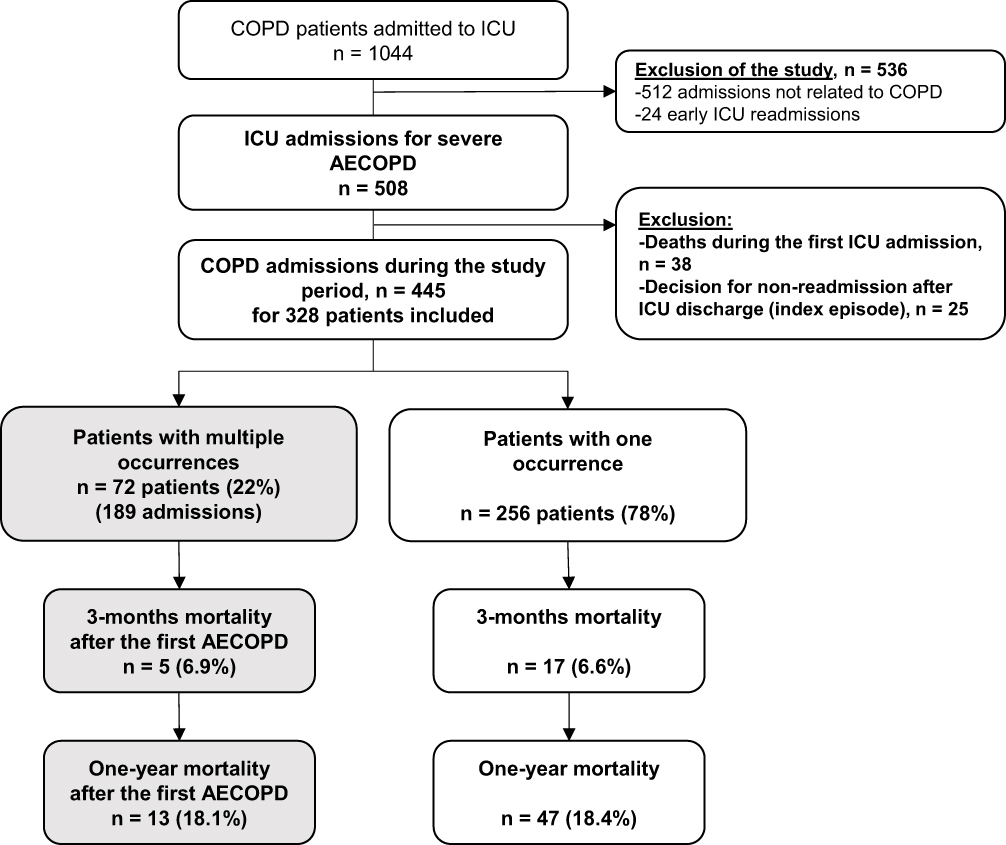 |
Figure 1 Flow chart. Abbreviations: COPD, Chronic Obstructive Pulmonary Disease; ICU, Intensive Care Unit; AECOPD, Acute Exacerbation of Chronic Obstructive Pulmonary Disease. |
Results in Table 1 show significant differences according to severe exacerbator phenotype. Recurrent exacerbator patients exhibited lower median of age (67 vs 70 years, p=0.037), lower median of Force Expiratory Volume in 1 second (36% vs 43% of theorical value, p=0.05), higher long-term oxygen therapy (38.9% vs 20.7%, p=0.002), lower altered (≥3) PS score (13.9% vs 25.8%, p=0.035). Sixty-nine (21.0%) patients were considered as immunosuppressed without group difference. Metabolic and cardiovascular comorbidities were statistically similar in the two groups. In addition, Table 1 shows a similar proportion of exacerbation triggering factors except for respiratory tract infection, especially pneumonia, with significant higher proportion in the non-recurrent exacerbator group (65.2 vs 48.6%, p=0.01). Recurrent exacerbators had lower median SAPS II (36 vs 39, p=0.025).
Table 2 reports clinical parameters and biological findings at ICU admission. There were no statistical differences between groups regarding vital parameters or arterial blood gas results. Recurrent exacerbators had higher eosinophilic blood cells (0.06 vs 0.04 G/L, p=0.025), lower C-reactive protein (16 vs 39 mg/L, p=0.017), and lower procalcitonin (0.09 vs 0.12 ng /mL, p=0.011).
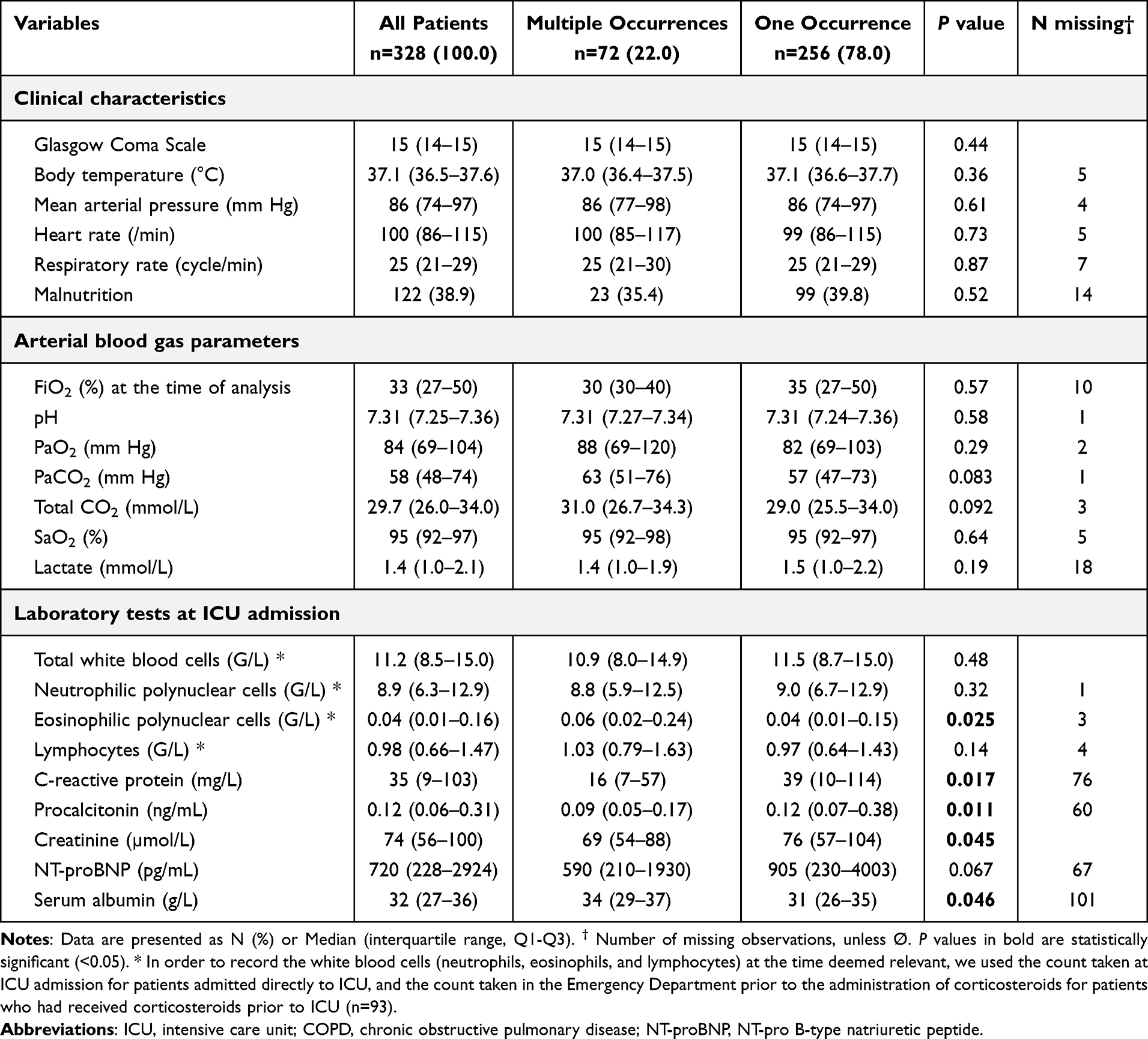 |
Table 2 Clinical and Biological Parameters at Admission in Patients Admitted for Severe Acute Exacerbation of COPD According to the Number of Patients ICU Occurrences |
Phenotype Differences in ICU Management and Outcomes
The median time before the second exacerbation in the recurrent exacerbators group was 7.2 (IQR, 2.3–17.6) months. Table 3 reports ICU management and outcomes. NIV was used for 285 (86.9%) patients, with 65 (23.9%) failures defined as need for intubation or death with a do not intubation order/decision. The median duration of NIV was higher in the recurrent exacerbator group (3 vs 2 days, p=0.006). Ninety-three (28.4%) patients were intubated with a median duration of invasive MV of 5 (IQR, 3–11) days. Results are similar for all the data of ventilatory management in the 2 groups except for NIV and ventilatory assistance duration. Median length of stay in ICU was 6 (IQR, 4–9) days, without group difference.
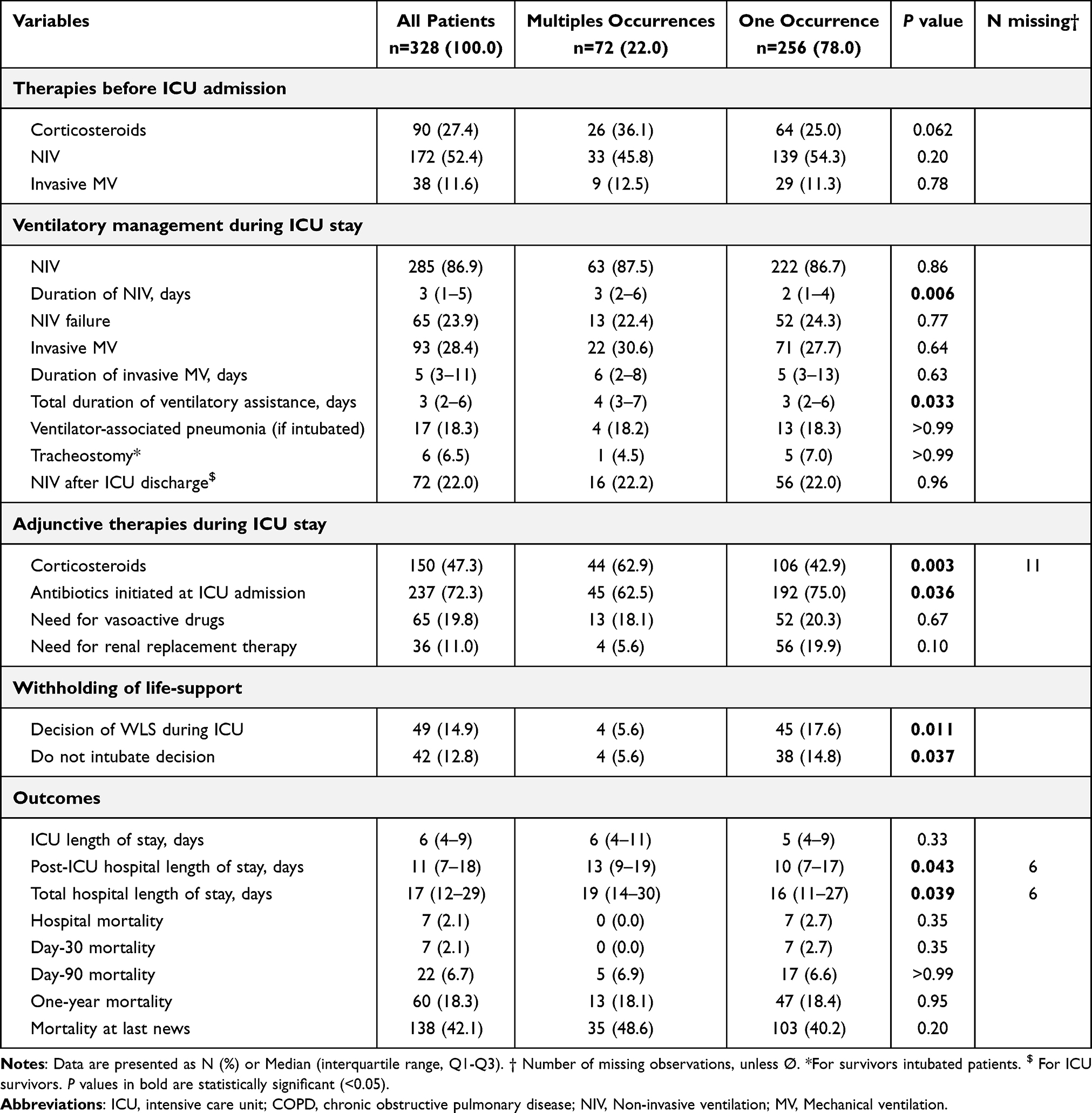 |
Table 3 Management and Outcomes in Patients Admitted for Severe Acute Exacerbation of COPD According to the Number of Patients ICU Occurrences |
Regarding adjunctive therapies, recurrent exacerbator patients had higher during ICU (62.9% vs 42.9%, p=0.003), and lower antibiotics initiated at ICU admission (62.5% vs 75%, p=0.036). As compared to non-recurrent exacerbators, recurrent exacerbators had lower rate of withholding life-support decision (5.6% vs 17.6%, p<0.011).
Results did not show significant difference for mortality rates between groups at any point of the study. At last news, with a median duration of follow-up of 31.2 (IQR, 13–54) and 16.5 (IQR, 6.5–35.5) months for recurrent and non-recurrent severe exacerbators respectively (Table 4), mortality was similar (48.6 vs 40.2%, p=0.20). The distribution of mortality until patients last news according to the Kaplan–Meier survival analysis is illustrated in Figure 2.
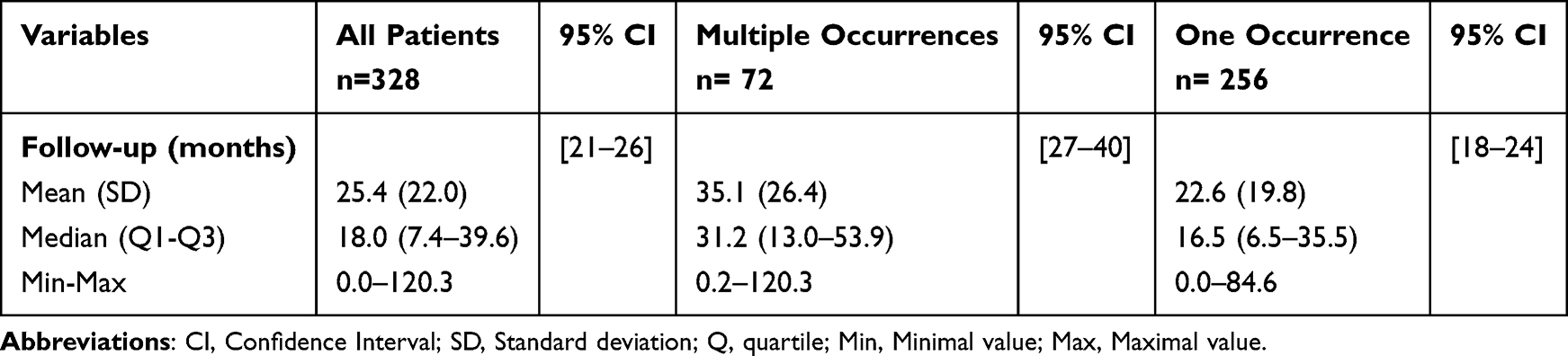 |
Table 4 Follow-up of Patients According to the Number of Patients ICU Occurrences |
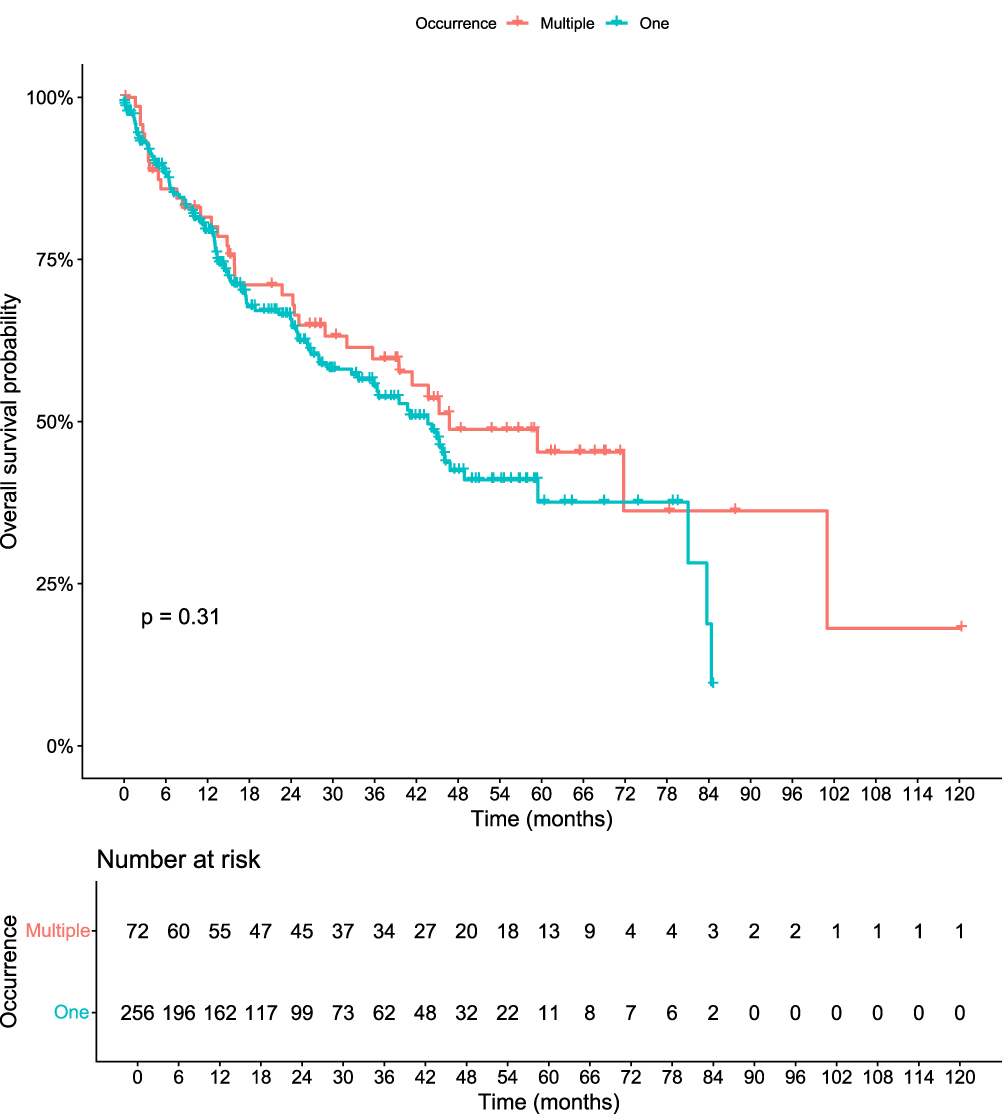 |
Figure 2 Kaplan-Meier survival curves at the date of patients last news according to the number of ICU occurrences (multiples vs one). |
Factors Associated with the second ICU Occurrence for Severe Exacerbation
Figure 3 shows the cumulative incidence of a new exacerbation taking death into account for competing risk. Table 5 details the univariate and multivariate analysis of factors associated with the second ICU occurrence for AECOD including death as a competing risk. Age and respiratory tract infection were inversely associated with severe exacerbation recurrence in univariate but not in our multivariate model analysis. COPD stage 4 (GOLD classification) and steroids use during ICU were associated with severe exacerbation ICU recurrence in univariate but not in multivariate analysis. In our model of multivariate analysis, PS score ≥ 3 was inversely associated with recurrent ICU admission (HR = 0.41, CI 95% [0.18–0.92], p=0.03) whereas long-term oxygen therapy (HR = 1.79, CI 95% [1.01–3.17], p=0.045) and blood eosinophilic polynuclear cells at admission (HR = 1.10, HR per +0.1 G/L, CI 95% [1.04–1.16], p < 0.001) were associated with recurrent ICU admission for severe AECOPD.
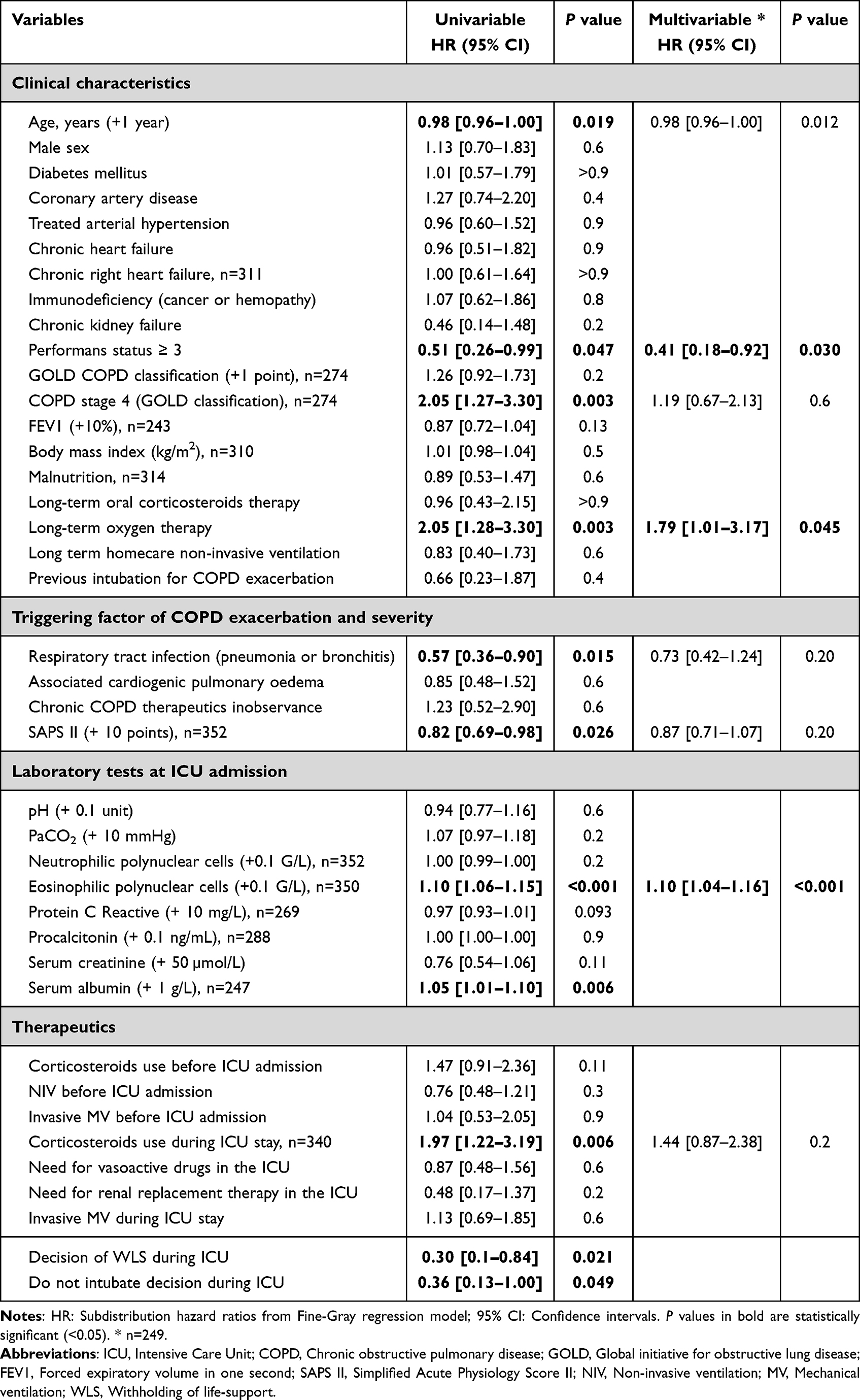 |
Table 5 Univariate and Multivariate Fine-Gray Analysis of Factors Associated with second ICU Occurrence with Death as a Competing Risk |
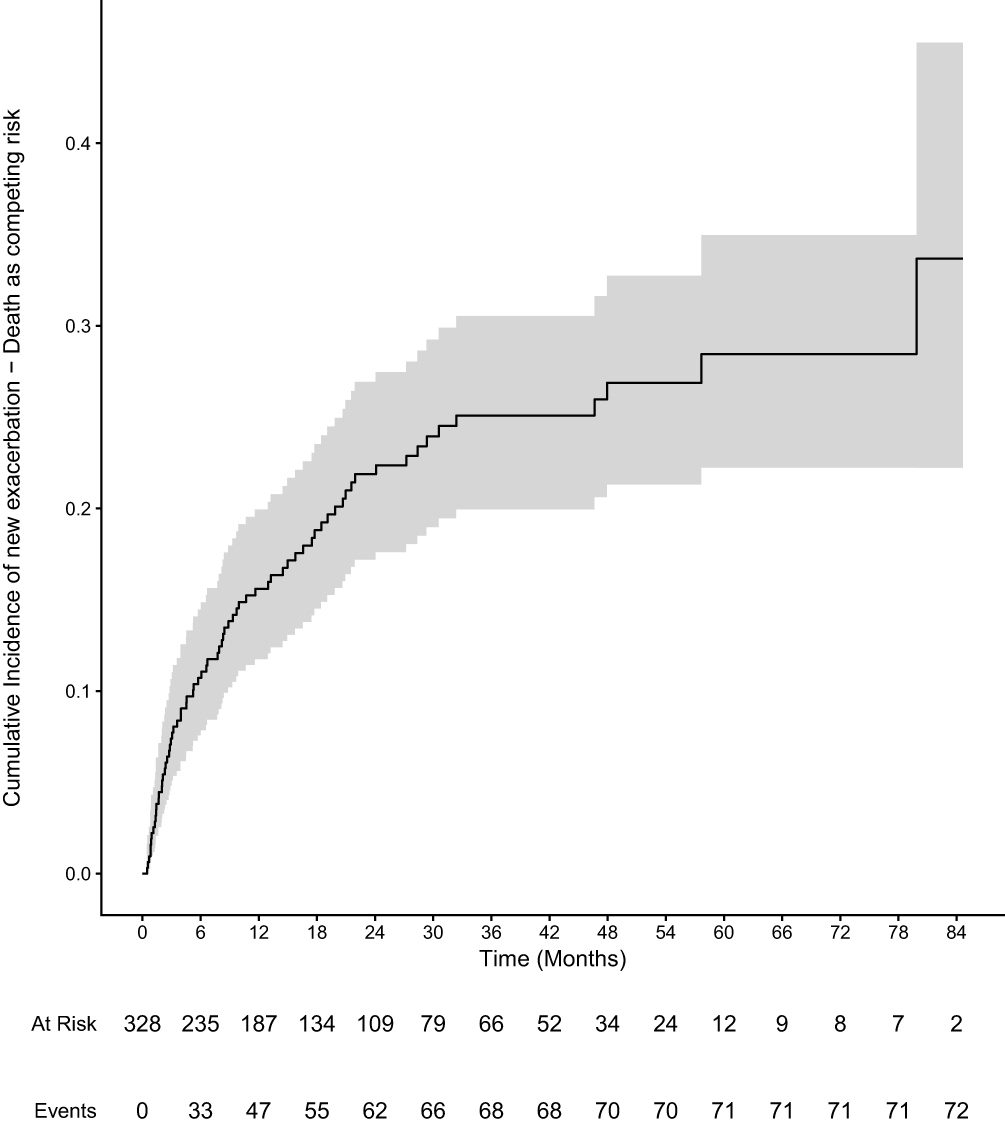 |
Figure 3 Cumulative incidence of a new exacerbation over time taking death into account for competing risk. |
Discussion
To our knowledge, this is the first study providing detailed information on recurrent ICU admissions following an index admission for severe AECOPD.
Principal Findings
In this cohort, one in five patients experienced at least one further ICU admission during follow-up. Compared with patients with a single admission, recurrent exacerbators were younger, more frequently receiving long-term oxygen therapy and had higher blood eosinophil counts. Mortality did not differ significantly between groups.
Patients’ Characteristics and Frailty
Our cohort’s baseline age, sex distribution and severity are comparable to contemporary ICU series of AECOPD highlighting severe respiratory impairment and overall health frailty.5,15–19 Patients presented high rates of metabolic and cardiovascular comorbidities as commonly reported.20–22 Recurrent severe exacerbators are younger yet had more chronic respiratory failure reflected by a higher rate of COPD stage 4 and long-term oxygen therapy, nevertheless they had a lower rate of altered PS score. This profile could have contributed to subsequent decision-making around ICU readmission in the context of chronic disease burden and frailty, as we demonstrated in a previous study that higher PS was associated with a decision of withholding of care.19
However, in our univariate analysis, the GOLD stage was not associated with subsequent ICU occurrence, whereas age, long-term oxygen therapy and specific COPD stage 4 were; this could reflect collinearity between advanced COPD stages and the need for long-term oxygen therapy - an indicator of disease severity/frailty23 - which exerts greater statistical weight than GOLD stage variable. Of note, PS ≥ 3 was observed in 23.2%, whereas GOLD stage ≥ 3 accounted for 67.4%. In multivariate analyses, age was not associated with subsequent ICU occurrence while long-term oxygen therapy was. Patient frailty is commonly associated with withholding life-sustaining treatments in ICU; a PS score ≥ 3 was inversely associated with ICU readmission for severe AECOPD (HR 0.40; p=0.030) as a surrogate of rejected decision for ICU readmission.19 This inverse association most likely reflects treatment limitation decisions and selection for ICU readmission rather than protection from exacerbations per se. All patients with a decision of non-readmission in ICU (n=25) were excluded of the study but we are not able to provide data on a such decision in the wards or in the respiratory medicine department (after ICU discharge or later in the history of COPD patients). This is an important factor in classifying patients into each group, and our results must be interpreted with caution.
ICU Management and Outcomes
Non-invasive ventilation (NIV) remains the cornerstone of critical COPD management. NIV was used in 87% of cases, with a 24% failure rate, in line with previous reports.20,24,25
Invasive MV was required in 28.4% of cases (median duration 5 days). Median length of stay was 6 days in ICU and 11 days in hospital after ICU discharge; these findings are comparable to other cohorts.26–29 No significant differences were observed between the 2 groups in ventilatory strategies (either non-invasive or invasive).
Mortality
Day-90 and one-year mortality rates were 6.7% and 18.3%, respectively. Reported mortality in the literature shows considerable variability: ICU mortality 11–14% and in-hospital mortality 19–26% in prior studies,27,30 ICU 7–25%, and hospital 11–40% in a recent meta-analysis.29 In our cohort, mortality at last follow-up was similar in the two groups, around 42% (p=0.20), with a median follow-up of 18 months for the entire cohort. Our results reported lower mortality that previous studies and these rates were influenced by the study design excluding patients who have died in ICU and those who had a decision of ICU non-readmission, mainly because of frailty.
Eosinophilic/Type 2 Inflammation and Implications
Higher blood eosinophils count among recurrent exacerbators are consistent with the recognised eosinophilic/type-2 inflammation phenotype in COPD, which has been linked both to exacerbation risk and to differential responses to inhaled and systemic corticosteroids.6,8,31–35 In our multivariable model, blood eosinophil count was independently associated with the occurrence of a second severe exacerbation. Although the between-group differences in eosinophils were modest, their statistical significance supports the hypothesis that type-2 inflammation may contribute to multiple ICU-level exacerbations over time. This aligns with the broader literature and guidance describing distinct phenotypes, including systemic inflammation and eosinophilic inflammation profiles.9,10,18 Recent studies reported lower respiratory tract consolidation/infection and inflammatory biomarkers (CRP and PCT) for COPD patients with type-2 eosinophilic profile.36–38 We can assume that these different profiles could explain the lower rate of pneumonia and so lower SAPS II (lower respiratory and items related to sepsis) for recurrent exacerbators in our cohort. However, our results with a small difference between the two groups do not allow us to draw any firm conclusions without qualifying them.
Recent studies supported that simple phenotyping using blood eosinophils count could help stratify risk and inform more personalised strategies to mitigate disease progression by reducing the likelihood of severe AECOPD. Emerging targeted therapies for COPD with type-2 inflammation further underline the potential of phenotype-guided management to reduce exacerbation frequency and potentially modify disease prognosis.39–43
Strengths and Limitations
Firstly, this study raises awareness of severe exacerbator phenotype in COPD patients, defined as the need of multiple ICU admission for exacerbation, representing an original contribution to the field. Secondly, it provides an overview of this topic, emphasizing the need for more personalized approaches throughout the continuum of care. These findings highlight the importance of anticipating personalized strategies, particularly preventive interventions aimed at mitigating disease progression and reducing the risk of severe acute exacerbation. These results, highlighting eosinophilic type 2 inflammation as factor for AECOPD recurrence, are interesting. Future prospective studies are warranted to determine whether phenotype-specific factors could influence long-term outcomes beyond the ICU stay. In this way, the novel biotherapies (monoclonal antibodies) emerging in the field of COPD with several promising studies on eosinophilic inflammation phenotype in the recent years seem to be an interesting avenue to explore.
However, our study has several limitations. First, as a retrospective, single-centre study, interpretation and generalizability are limited. Second, the retrospective design led to some missing data. Third, we could not prespecified phenotypes prior to ICU admission – particularly the “frequent exacerbator” phenotype per GOLD or the emphysema phenotype according to baseline CT scan and spirometry data. Then, we could not provide data on health-related quality of life after discharge, owing the incomplete records. In addition, we arbitrarily defined groups based on recurrence of severe exacerbations leading to ICU admission; this construct is not yet defined in current guidelines. We could not ascertain the number of wards-level exacerbation admissions or ICU admissions at other hospitals, which would have enhanced phenotyping and data completeness. The difference of withholding decision between the 2 groups and its weight in our statistical model introduce bias and lead to cautious interpretation of our results. However, Finally, we excluded patients who died during the first ICU admission and those who had a decision of non-readmission in ICU after the index episode; by definition, they could not be readmitted, which may introduce selection bias when assessing factors associated with recurrence or mortality.
Conclusion
This study provides insight into the phenotypes of recurrent and non-recurrent severe exacerbators among ICU patients admitted with severe AECOPD. Recurrent exacerbators were younger and had higher blood eosinophils count, findings consistent with an eosinophilic/type-2 inflammation phenotype described in COPD guidance. Despite the contrasting baseline profiles, ventilatory support and outcomes were similar between groups. Our results may suggest that, in the setting of critical COPD exacerbations, the risk of subsequent ICU-level events could be linked to an eosinophilic/type-2 inflammation phenotype. Further multicentre, prospective studies are warranted to validate these observations and to determine whether phenotype-guided strategies—including steroid-sparing approaches and targeted monoclonal antibodies—can improve outcomes in this population at high risk of recurrent exacerbation.
Data Sharing Statement
The investigators will make the documents and individual data strictly required for monitoring, quality control, and audit of the study available to dedicated persons, in accordance with laws and regulations in force (Articles L.1121-3 and R.5121-13 of the Code de Santé Publique – CSP, French Public Health Code).
The datasets used and/or analysed during the study will be available from the corresponding author (Alexis Ferré) on reasonable request. The procedures carried out under the French data privacy authority (Commission Nationale de l’Informatique et des Libertés) do not permit the transmission of the database, nor do the informed consent documents signed by the patients. Consultation by the editorial board or interested researchers of individual participant data that underlie the results reported in the article after deidentification may nevertheless be considered, subject to prior determination of the terms and conditions of such consultation and in respect of compliance with the applicable regulations.
Ethics Approval and Consent to Participate
We conducted a monocentric, observational, and retrospective study. This study was performed in accordance with the principles of the Declaration of Helsinki. We carried out all procedures in accordance with current legislation and regulations. This human study was approved by ethic committee of the French Intensive Care Society (N°#21-66) and the protocol was registered at the French National Institute for Health Data (#MR2516271119). Upon recovery, oral informed consent was sought from the patients including a written form of objection in case of refusal to participate, in compliance with French legislation. The study complies with the STROBE statement on guidelines for publishing observational studies.
Acknowledgment
We thank the Centre Hospitalier de Versailles for editorial assistance.
Author Contributions
All authors (AF, NS, PP, SD, GAA, and SL) made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
Alexis Ferré, Nassim Sahki, Pauline Puechoultres, Sylvain Diop, and Georges Abi-Abdallah have no conflicts of interest to declare. Stéphane Legriel reports consulting fees from Becton Dickinson and meeting invitation from UCB, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Davidson AC, Banham S, Elliott M, et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax. 2016;71 Suppl 2:ii1–15. doi:10.1136/thoraxjnl-2015-208209
2. Galerneau LM, Bailly S, Terzi N, et al. Management of acute exacerbations of chronic obstructive pulmonary disease in the ICU: an observational study from the OUTCOMEREA database, 1997-2018. Crit Care Med. 2023;51(6):753–764. doi:10.1097/CCM.0000000000005807
3. Vestbo J. COPD: definition and phenotypes. Clin Chest Med. 2014;35(1):1–6. doi:10.1016/j.ccm.2013.10.010
4. Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. doi:10.1056/NEJMoa1105482
5. Agustí A, Edwards LD, Rennard SI, et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 2012;7(5):e37483. doi:10.1371/journal.pone.0037483
6. Singh D, Bafadhel M, Brightling CE, et al. Blood eosinophil counts in clinical trials for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;202(5):660–671. doi:10.1164/rccm.201912-2384PP
7. Singh D, Kolsum U, Brightling CE, et al. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697–1700. doi:10.1183/09031936.00162414
8. Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
9. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49(3):1700214. doi:10.1183/13993003.00214-2017
10. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
11. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
12. Le Rouzic O, Roche N, Cortot AB, et al. Defining the “frequent exacerbator” phenotype in COPD: a hypothesis-free approach. Chest. 2018;153(5):1106–1115. doi:10.1016/j.chest.2017.10.009
13. Mantero M, Rogliani P, Di Pasquale M, et al. Acute exacerbations of COPD: risk factors for failure and relapse. Int J Chron Obstruct Pulmon Dis. 2017;12:2687–2693. doi:10.2147/COPD.S145253
14. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. doi:10.1164/ajrccm.161.5.9908022
15. Pozo-Rodríguez F, López-Campos JL, Alvarez-Martínez CJ, et al. Clinical audit of COPD patients requiring hospital admissions in Spain: AUDIPOC study. PLoS One. 2012;7(7):e42156. doi:10.1371/journal.pone.0042156
16. Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A. Respiratory infection triggering severe acute exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:555–565. doi:10.2147/COPD.S447162
17. Jouneau S, Dres M, Guerder A, et al. Management of acute exacerbations of chronic obstructive pulmonary disease (COPD). Guidelines from the Société de pneumologie de langue française (summary). Rev Mal Respir. 2017;34(4):282–322. doi:10.1016/j.rmr.2017.03.034
18. Agusti A. Global strategy for prevention, diagnosis and management of COPD: 2025 report. GOLD. 2025;1–215.
19. Puechoultres P, Jamme M, Abi-Abdallah G, Diop S, Legriel S, Ferré A. Withholding of life-sustaining treatment and mortality in ICU patients with severe acute COPD exacerbations: a retrospective French cohort. Int J Chron Obstruct Pulmon Dis. 2025;20:1995–2009. doi:10.2147/COPD.S502019
20. Stolz D, Kostikas K, Loefroth E, et al. Differences in COPD exacerbation risk between women and men: analysis from the UK clinical practice research datalink data. Chest. 2019;156(4):674–684. doi:10.1016/j.chest.2019.04.107
21. Henoch I, Strang S, Löfdahl CG, Ekberg-Jansson A. Management of COPD, equal treatment across age, gender, and social situation? A register study. Int J Chron Obstruct Pulmon Dis. 2016;11:2681–2690. doi:10.2147/COPD.S115238
22. Li N, Li X, Liu M, Wang Y, Wang J. Sex differences in comorbidities and mortality risk among patients with chronic obstructive pulmonary disease: a study based on NHANES data. BMC Pulm Med. 2023;23(1):481. doi:10.1186/s12890-023-02771-3
23. Verduri A, Carter B, Laraman J, et al. Frailty and its influence on mortality and morbidity in COPD: A Systematic Review and Meta-Analysis. Intern Emerg Med. 2023;18(8):2423–2434. doi:10.1007/s11739-023-03405-6
24. Ucgun I, Metintas M, Moral H, Alatas F, Yildirim H, Erginel S. Predictors of hospital outcome and intubation in COPD patients admitted to the respiratory ICU for acute hypercapnic respiratory failure. Respir Med. 2006;100(1):66–74. doi:10.1016/j.rmed.2005.04.005
25. Teixeira C, da R Cabral C, Hass JS, et al. Patients admitted to the ICU for acute exacerbation of COPD: two-year mortality and functional status. J Bras Pneumol Publicacao of Soc Bras Pneumol E Tisilogia. 2011;37(3):334–340. doi:10.1590/s1806-37132011000300009
26. Gadre SK, Duggal A, Mireles-Cabodevila E, et al. Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD). Medicine. 2018;97(17):e0487. doi:10.1097/MD.0000000000010487
27. Berenyi F, Steinfort DP, Abdelhamid YA, et al. Characteristics and outcomes of critically ill patients with acute exacerbation of chronic obstructive pulmonary disease in Australia and New Zealand. Ann Am Thorac Soc. 2020;17(6):736–745. doi:10.1513/AnnalsATS.201911-821OC
28. Warwick M, Fernando SM, Aaron SD, et al. Outcomes and resource utilization among patients admitted to the intensive care unit following acute exacerbation of chronic obstructive pulmonary disease. J Intensive Care Med. 2021;36(9):1091–1097. doi:10.1177/0885066620944865
29. Messer B, Griffiths J, Baudouin SV. The prognostic variables predictive of mortality in patients with an exacerbation of COPD admitted to the ICU: an integrative review. QJM Mon J Assoc Physicians. 2012;105(2):115–126. doi:10.1093/qjmed/hcr210
30. Brown H, Dodic S, Goh SS, et al. Factors associated with hospital mortality in critically ill patients with exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:2361–2366. doi:10.2147/COPD.S168983
31. Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The copenhagen general population study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
32. Chen F, Yang M, Wang H, Liu L, Shen Y, Chen L. High blood eosinophils predict the risk of COPD exacerbation: a systematic review and meta-analysis. PLoS One. 2024;19(10):e0302318. doi:10.1371/journal.pone.0302318
33. Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037–2047.e10. doi:10.1016/j.jaci.2018.04.010
34. Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756. doi:10.1016/S2213-2600(19)30190-0
35. Ramakrishnan S, Jeffers H, Langford-Wiley B, et al. Blood eosinophil-guided oral prednisolone for COPD exacerbations in primary care in the UK (STARR2): a non-inferiority, multicentre, double-blind, placebo-controlled, randomised controlled trial. Lancet Respir Med. 2024;12(1):67–77. doi:10.1016/S2213-2600(23)00298-9
36. Bafadhel M, Greening NJ, Harvey-Dunstan TC, et al. Blood eosinophils and outcomes in severe hospitalized exacerbations of COPD. Chest. 2016;150(2):320–328. doi:10.1016/j.chest.2016.01.026
37. MacDonald MI, Osadnik CR, Bulfin L, et al. Low and high blood eosinophil counts as biomarkers in hospitalized acute exacerbations of COPD. Chest. 2019;156(1):92–100. doi:10.1016/j.chest.2019.02.406
38. Singh D, Agusti A, Martinez FJ, et al. Blood eosinophils and chronic obstructive pulmonary disease: a global initiative for chronic obstructive lung disease science committee 2022 review. Am J Respir Crit Care Med. 2022;206(1):17–24. doi:10.1164/rccm.202201-0209PP
39. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with Type 2 inflammation indicated by eosinophil counts. N Engl J Med. 2023;389(3):205–214. doi:10.1056/NEJMoa2303951
40. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with blood eosinophil evidence of Type 2 inflammation. N Engl J Med. 2024;390(24):2274–2283. doi:10.1056/NEJMoa2401304
41. Bhatt SP, Rabe KF, Hanania NA, et al. Effect of dupilumab on health-related quality of life and respiratory symptoms in patients with COPD and Type 2 inflammation: BOREAS and NOTUS. Chest. 2025;168(1):56–66. doi:10.1016/j.chest.2025.01.029
42. Christenson SA, Hanania NA, Bhatt SP, et al. Type 2 inflammation biomarkers and their association with response to dupilumab in COPD (BOREAS): an analysis of a randomised, placebo-controlled, Phase 3 trial. Lancet Respir Med. 2025;13(8):687–697. doi:10.1016/S2213-2600(25)00044-X
43. Çolak Y, Afzal S, Marott JL, Vestbo J, Nordestgaard BG, Lange P. Type-2 inflammation and lung function decline in chronic airway disease in the general population. Thorax. 2024;79(4):349–358. doi:10.1136/thorax-2023-220972
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics and Outcomes of Eosinophilic Exacerbations of COPD
Donnan M, Liu TL, Gvalda M, Chen X, Foo CT, MacDonald MI, Thien F
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1061-1070
Published Date: 13 April 2025
Characteristics and Outcomes of People With COPD Who Experience Exacerbations While on Inhaled Triple Therapy: Results of the SIRIUS I Cohort Study in the US (2015–2019)
Nordon C, Carstens D, Fagerås M, Müllerová H, Veeranki PS, Alves JA, Germack HD, Barnes TL, McCormack MC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1851-1864
Published Date: 11 June 2025
Withholding of Life-Sustaining Treatment and Mortality in ICU Patients with Severe Acute COPD Exacerbations: A Retrospective French Cohort
Puechoultres P, Jamme M, Abi-Abdallah G, Diop S, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1995-2009
Published Date: 18 June 2025
Validation Study of Rome Criteria for Assessing COPD Exacerbation Severity and Predicting Clinical Outcomes: Turkish Thoracic Society COPD Assembly
Baha A, Baysan C, Nayci SA, Ozgur ES, Karamustafalioglu T, Sen E, Selcuk E, Mit G, Alpaydin AO, Ozturk B, Karabacak KT, Kokturk N, Akbulut S, Baydar O, Varol Y, Kodalak S, Esendagli D, Gurgun A, Emdadian E, Toreyin ZN, Alkan A, Sertcelik U, Ozmen I, Elabed EU, Kilic H, Polatli M, Hilmioglu O
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3993-4003
Published Date: 10 December 2025
The Disproportionate Burden of Cardiovascular Disease in Mild-to-Moderate COPD
Zhang W, Wen J, Chew SY, Hao Y, Liao F, Koh MS, Xu Z, Wang G, Wang X, Tiew PY
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:603670
Published Date: 23 June 2026