Back to Journals » Patient Preference and Adherence » Volume 17
Setting Organ Allocation Priorities: A Discrete Choice Experiment with German Patients and Their Relatives
Authors Bartling T ![]() , Oedingen C
, Oedingen C ![]() , Schrem H, Kohlmann T, Krauth C
, Schrem H, Kohlmann T, Krauth C ![]()
Received 6 January 2023
Accepted for publication 9 March 2023
Published 24 March 2023 Volume 2023:17 Pages 827—838
DOI https://doi.org/10.2147/PPA.S402203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Tim Bartling,1,2 Carina Oedingen,1,2 Harald Schrem,2,3 Thomas Kohlmann,4 Christian Krauth1,2
1Hannover Medical School, Institute of Epidemiology, Social Medicine and Health Systems Research, Hannover, Germany; 2Center for Health Economics Research Hannover, Hannover, Germany; 3General, Visceral and Transplant Surgery, Medical University Graz, Graz, Austria; 4Department of Methods of Community Medicine, Institute for Community Medicine, University of Greifswald, Greifswald, Germany
Correspondence: Tim Bartling, Medizinische Hochschule Hannover / Hannover Medical School, Institute of Epidemiology, Social Medicine and Health Systems Research, Carl-Neuberg-Str, 1, Hannover, Lower Saxony, 30625, Germany, Tel +49 511 532 9462, Fax +49 511 532 5376, Email [email protected]
Purpose: Organ transplantation systems benefit from guidelines that are harmonious with the preferences of the people involved. Discrete choice experiments are useful tools for eliciting preferences.
Patients and Methods: This study evaluated the preferences of patients and their relatives (n=285) to identify their priorities in organ allocation using a discrete choice experiment. In eight hypothetical allocation decisions, the participants were asked to select the candidate they considered the most suitable The candidates differed in years of life gained after transplantation, quality of life after transplantation, waiting time until transplantation, age, compliance and social support.
Results: The most important aspects for setting priority in organ allocation were lack of compliance (β= − 2.5, p< 0.001) and good quality of life after transplantation (β = +1.4, p< 0.001). The lack of social support (ß = − 0.8, p< 0.05) and the more years of life gained after transplantation (β = +0.5, p< 0.001) had less but still a significant amount of influence on this decision, while the waiting list was not considered significantly important (β = 0.1, p> 0.05). The comparison of the different relations to transplantation showed that life years gained after transplantation was of high relevance to posttransplant patients (+10 years: β = +0.709, p< 0.001 / +15 years: β = +0.700, p< 0.001) and of no importance to waitlisted patients (+10 years: β = +0.345, p> 0.05 / + 15 years: β = +0.173, p> 0.05) and relatives (+ 10 years: β = +0.063, p> 0.05 / +15 years: β = +0.304, p> 0.05).
Conclusion: This study provides useful insights into the unique perspective of patients and their relatives on priority-setting in the allocation of donor organs that should be reflected in improved donor organ allocation rules.
Keywords: organ transplantation, health priorities, health resources, ethics, patient involvement, resource allocation, discrete choice experiment
Introduction
Organ transplantation has been firmly established for the treatment of end-stage organ failure.1 The worldwide shortage of deceased donor organs calls all stakeholders involved in the process of transplantation to make value judgments implied in the priority-setting of donor organ allocation, as not every patient who could benefit from organ transplantation is able to receive a donor organ.2,3 This involves all physicians/medical experts who evaluate patients and decide on the listing of patients for transplantation. Furthermore, it is necessary to find a consensus on donor allocation rules that are socially acceptable within national legal frameworks. Ethical considerations also suggest taking the perspectives of transplant patients and their relatives into account, because end-stage organ failure is typically a life-threatening long-term burden for patients and their relatives. Therefore, the patient’s attitude toward organ allocation is unique and will be the focus of this study.
This study investigates trade-offs in organ allocation decisions that reflect a complex dilemma. One of the central aspects in this context is the debate on the weighing of urgency versus effectiveness in organ allocation, as patients who are considered to be of high urgency usually have smaller chances of success and vice versa.4
An earlier systematic review5 identified one discrete choice experiment (DCE)6 that has already been conducted with patients. In that publication, the trade-off between effectiveness and urgency was not directly addressed. This study therefore adds a new perspective to the scientific discourse. The aims of the current study are to explore the preferences and perspectives of transplantation patients and their relatives regarding the allocation of deceased donor organs, to understand their preferences in the context of relevant attributes and characteristics of a potential donor organ recipient and to investigate how the different sociodemographic factors of the respondents influence their choice decisions.
Materials and Methods
A DCE was developed, which is a quantitative instrument eliciting preferences from multiattributive scenarios. In a DCE, respondents choose their preferred alternative from two hypothetical alternatives in a direct comparison. Both alternatives are described using the same attributes but differ in the levels of these attributes.7,8
For this DCE, the participants had to choose between two different hypothetical patients who received an organ offer. The alternatives were characterized by six different attributes, each with between 2 and 4 levels:
- Life years gained after transplantation (Gain): +5 years, + 10 years, + 15 years.
- Quality of life after transplantation (QoL): good, moderate, bad.
- Waiting time (Wait): 3 weeks, 3 months, 3 years.
- Age (Age): 25 years, 40 years, 55 years, 70 years.
- Compliance (Comp): always compliant, partly compliant, rarely compliant.
- Social Support (Supp): yes, no.
These levels were based on both a systematic review5 and single interviews,9 as recommended by the respective ISPOR guidelines (ISPOR-The Professional Society for Health Economics and Outcomes Research).10 The full scope of this research project has been presented in an earlier study protocol.11 To select the final attributes and levels, the authors focused on the results of semi-structured patient interviews, and used the insight obtained during these interviews to create attributes and levels that are of high importance to transplantation patients as well as realistic to everyday practice. To guarantee the comparability of this DCE to previously published studies, the levels of the attributes Gain, QoL and Age were designed in a manner similar to those of a DCE that targeted the general public about the same question,12 which was itself based on earlier focus group discussions.13 The levels for Age are presented in the way they are to focus on adults only, as the inclusion of children or young adults might a) heavily skew the decision of the respondent and b) create nonrealistic scenarios in which eg, a child and an elderly person are both a possibility for the same organ.
During the earlier systematic review,5 it was identified that the attributes differ from their wording between medically detailed terms for professionals, and more general, potentially easier-to-understand terms for patients. Therefore, even though all stakeholders’ perspectives are important in this topic, for the creation of this DCE the focus was placed on providing easy-to-understand and realistic, close-to-practice attributes. One of the trade-offs identified in this review, if not the major one, was that between effectiveness and urgency. Earlier research5,9 has shown that this trade-off is heavily skewed by the idea of not wanting anybody to die and allocating organs to heavily urgent patients with survival chances lower than 10%. To circumvent this and elicit this trade-off from a different perspective, the aspect of urgency was presented only indirectly via the proxy-attribute “waiting time” in the choice sets, based on the theory that while the indicated waiting time might still give a hint to the urgency of the situation, it allows for a more open approach in this regard.
As a full factorial choice design (confronting all respondents with every combination of attributes and levels possible) was not feasible (21*34*41 = 648 combinations), a fractional factorial design was chosen to conduct this study,14 using the minimal sample size calculation obtained from Johnson & Orme  , n = minimal sample size, t = no. of choice sets, a = no. of alternatives and c = highest no. of levels in the attributes included). As reaching a result of at least 1000 in this formula is considered desirable, we aimed to include 250 participants
, n = minimal sample size, t = no. of choice sets, a = no. of alternatives and c = highest no. of levels in the attributes included). As reaching a result of at least 1000 in this formula is considered desirable, we aimed to include 250 participants  .15,16 Three blocks of 8 different choice sets each were created, and each participant was randomly assigned to one of the three blocks. Therefore, 24 different choice sets were used throughout the course of this study (relative D effectiveness 87.1186; D-Error 0.0478). Choice sets were designed using cloud-based SAS® OnDemand for Academics following the procedures of Kuhfeld.17
.15,16 Three blocks of 8 different choice sets each were created, and each participant was randomly assigned to one of the three blocks. Therefore, 24 different choice sets were used throughout the course of this study (relative D effectiveness 87.1186; D-Error 0.0478). Choice sets were designed using cloud-based SAS® OnDemand for Academics following the procedures of Kuhfeld.17
Before these eight choice sets were presented, each participant was confronted with a dominant choice set, which was created as a validity check. This choice set included one alternative that was clearly preferable over the other and was used to exclude participants from the study who appeared clearly irrational in selecting the obviously unfavorable alternative.
Participants had to make a choice for every choice set. We did not include an opt-out option to mirror the real-life situation where organs are a precious resource and situations in which there is no allocation must be prevented to reduce wasting resources.
The questionnaire contained three parts. In the first part, the participants were presented with sociodemographic questions to gather information on the participants. The second part contained the DCE and asked the participants to choose an alternative in 8 (+1 dominant) choice sets. The last part of the questionnaire asked the participants about their experiences with the DCE (eg, how difficult they found it to make a decision) and presented them with more questions specific to organ allocation and transplantation to gain a more profound understanding of their preferences. The questionnaire was pilot-tested with board members of the BDO, all being patients or relatives themselves, who did not take part in the actual survey later on. The full questionnaire can be found in the Appendix. The study received approval from the ethics committee of Hannover Medical School (vote number: 7921_BO_K_2018).
Recruitment
Recruitment for this study was carried out in cooperation with the “Federal Association of the Organ-transplanted” (“Bundesverband der Organtransplantierten”, ie, BDO), a self-help organization for transplant patients and their relatives, using multiple approaches. At first, information about this study and a link to the online questionnaire were placed in their member’s journal, which was delivered by post to 700 of their 880 members, who have chosen to receive this journal. Furthermore, the study was further spread among transplantation patients using the BDO social media pages in October 2021, which at the time were followed by 378 people on Facebook and 308 on Instagram. Last, the study was spread using the BDO’s e-mail newsletter, which had 300 subscribers at the time. Considering that some people may have received the invitation via multiple channels and the fact that the member’s magazine may be shared in households between patients and their relatives, the BDO’s press officer conservatively estimated that the invitation to this study reached approximately 1500 people in total. The questionnaire was hosted online and was accessible to participants from October 1, 2021, to December 31, 2021.
Statistical Analysis
The survey was hosted, and the data were gathered by Umfragenwerk – Evartis GmbH. The data were provided via Microsoft Excel sheets and analyzed using STATA MP 16. The underlying theory used for DCEs is random utility theory, specified as Uij=Vij+εij.18,19
The data were analyzed using a conditional (fixed-effects) logit model (CL), a mixed logit model (MXL), and a latent class analysis (LCA).
A CL is often used to analyze DCE data, based on the random utility theory by McFadden.19 The CL can calculate the estimated preference weight for the attributes in the DCE; however, it has limitations in regard to accounting for unobserved systematic differences (preference heterogeneity). For this, an MXL (or “random-parameters logit”) is usually carried out, which can identify preference heterogeneity across the sample. If this is the case, an LCA, which assumes heterogeneous effects between different groups across the sample, is used to understand the potentially heterogeneous nature of answers/respondents in the dataset.20
Results
Sample Characteristics
In total, 415 questionnaires were returned, which constitutes a response rate of 27.6% (based on the estimation of 1500 people reached as described in the methods). Of those 415 questionnaires, 100 were excluded since the questionnaires were not answered completely. Another 19 were excluded for stating implausible birth years, and another 9 were excluded for irrationally answering the dominant choice set. Two more questionnaires were excluded by hand search, as they were highly likely duplicates, sent in by the same person. Thus, 285 questionnaires were ultimately analyzed for this study. More characteristics of the participants are summarized in Table 1.
 |
Table 1 Demographic Characteristics of the Study Sample |
Conditional Logit Model
The preferences estimated from the CL for this DCE are shown in Figure 1 and Table 2.
 |
Table 2 Conditional Logit Model |
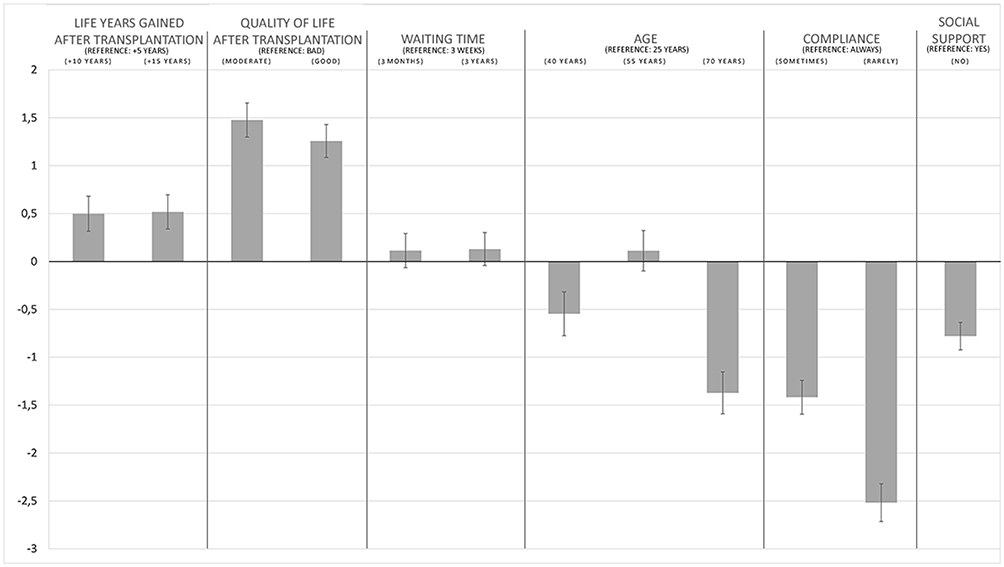 |
Figure 1 Conditional logit model, β-coefficients and 95% confidence intervals. |
Regression coefficients indicate to what extent a certain level of an attribute increases (positive value) or decreases (negative value) the chances that an alternative is chosen. The coefficients in this model demonstrate that compliance, quality of life, and being aged 70 years are the most important factors. Waiting time is not relevant for the participants and is the only attribute with no significant levels. Lack of social support during the process is seen as a significant negative influence, ie, more important than the gain in life years and being aged 40 or 55 years. The age of 55 years is an outlier level for the attribute of age, since it is not significantly different from the reference age of 25; however, being 40 and 70 years old both have a negative effect on the chances of receiving the donor organ according to the choices by the participants.
Mixed Logit Model
To assess preference heterogeneities, which can be elaborated further with an LCA, an MXL was conducted. The results of the MXL are shown in the Appendix. The MXL indicates possible preference heterogeneities in five attribute levels: (Gain) + 10 years and + 15 years, (wait) 3 months and 3 years and (Age) 55 years. This constitutes the basis for an LCA in which these preference heterogeneities can be observed more deeply.
Latent Class Analysis
Following up to the AIC and BIC numbers of the respective model, as well as theoretical considerations, an LCA was carried out for two classes (Classes 1 and 2). This analysis yielded the following results (Figure 2, also in the Appendix).
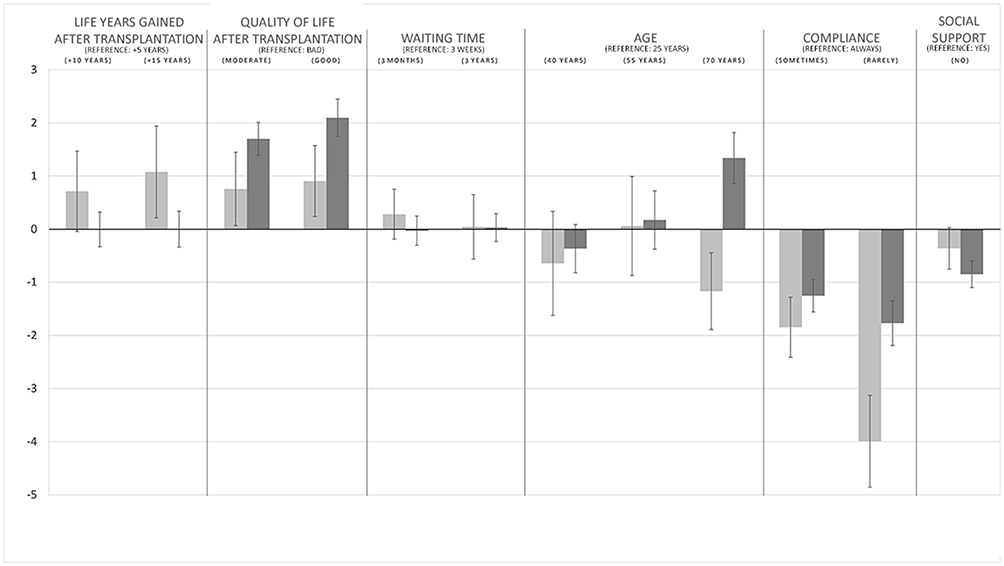 |
Figure 2 Latent class analysis, β-coefficients and 95% confidence intervals. Light: Class 1; Dark: Class 2. |
The classes’ demographic characteristics are shown in Table 3.
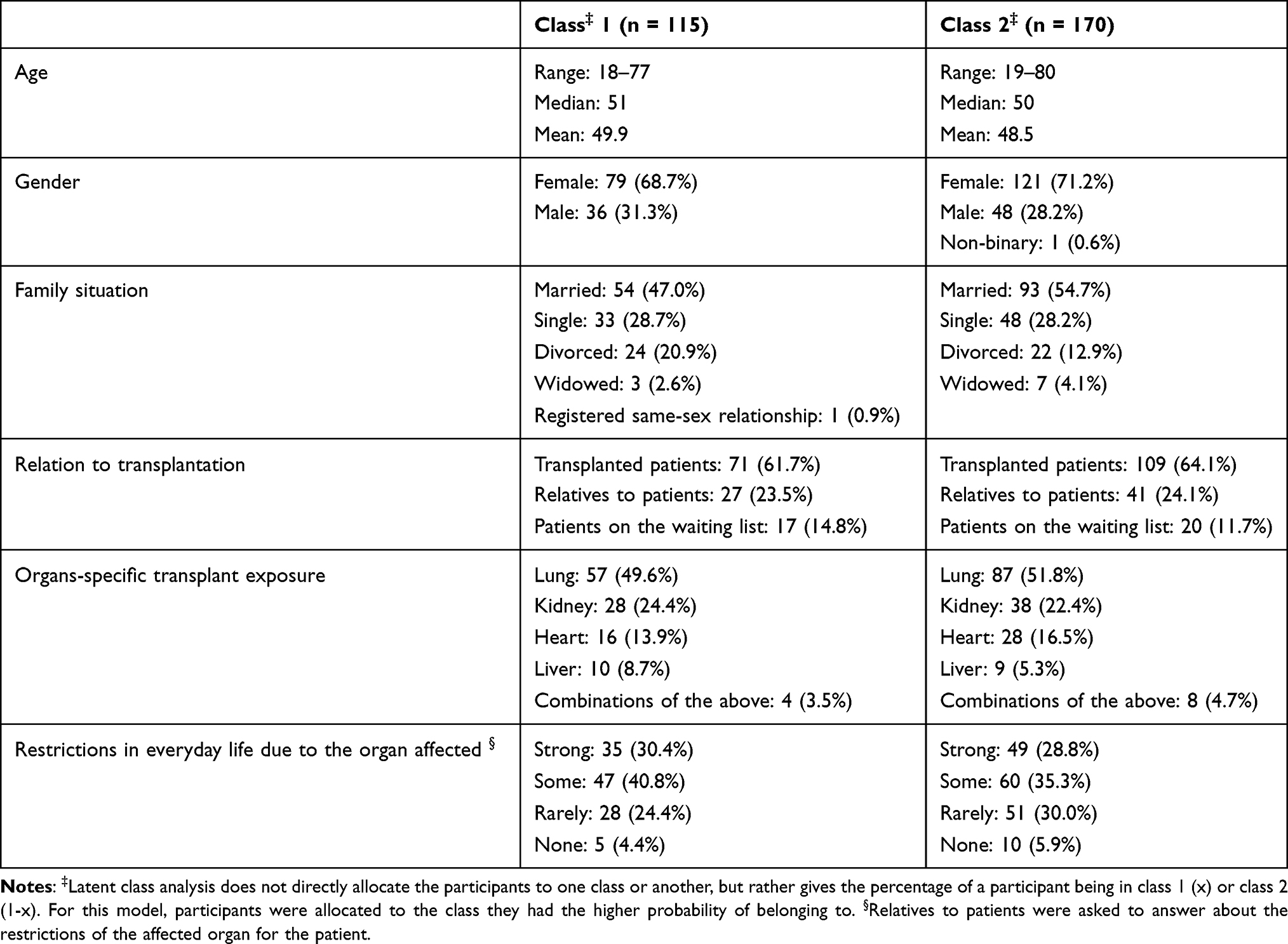 |
Table 3 Demographic Characteristics of the Identified Classes |
From these data, it is possible to distinguish the latent classes as follows: Class 1 is a group that is focused heavily on compliance aspects and gives very little attention to the other attributes of the DCE; however, the attribute “Age: 70”, “QoL: moderate & good” and “Gain: +15 years” are still of importance to them (although none of them are found to have p<0.001). Class 2 has a very high preference (p<0.001) for a multitude of attributes and levels: “QoL: moderate & good”, “Age: 70”, “Comp: sometimes & rarely” and “Supp: no”. However, they show no preference regarding the gain of life years through transplantation. Participants in Class 1 are more likely to be on the waiting list, divorced and have higher restrictions in their everyday life (71.2% “strong” or “some”), whereas those in Class 2 are more likely to be married, have already received a transplant and have fewer restrictions in their everyday life (64.1% “strong” or “some”).
Conditional Logit Models for Other Subgroups
Since the participants reported their sex, age and relation to transplantation over the course of the questionnaire, it was possible to calculate CLs for these subgroups as well and compare them to each other. The result tables can be found in the appendix.
Only a few differences between genders were observable. In the age attribute levels, the level “40 years old” was significant for women, but not for men. Apart from that, there were minor observable differences regarding the relative strength of some attributes, but no changes in significance or orientation of the attributes.
To investigate differences in the age groups, the sample was split into two groups according to the age median: participants younger than 50 and participants 50 and older. Similar to the comparison between men and women, only a few differences were observed between these groups. The biggest difference was again observable in the age attribute, where the level “40 years old” was of negative significance for those under 50 years and not significant for those 50 years and older. Again, only minor other differences were observable, and again, this was true only according to the relative strength of some attributes.
Separated by relation to transplantation, the CL for transplanted patients, patients on the waiting list, and relatives were compared to each other. Here, more differences were observable. Although both levels of “Gain” were of high relevance to transplant patients, they were of no relevance to either waitlisted patients or relatives. Furthermore, in the age attribute, the level “40 years old” was of significance for transplanted patients and relatives but not for waitlisted patients. Other minor differences can be found throughout the models, but none change the significance or orientation of the attributes.
Stated Importance
After the DCE, the participants had to state what importance they personally would attribute to each attribute, ranging from “very important” to “not important at all”. A majority of participants (57%) rated compliance as “very important”, while quality of life after transplantation and life years gained after transplantation were rated as “important” by the majority of the people (44% and 39%, respectively). Waiting time was the only aspect rated “less important” by the majority of people (35%). The full results of these questions are shown in Table 4.
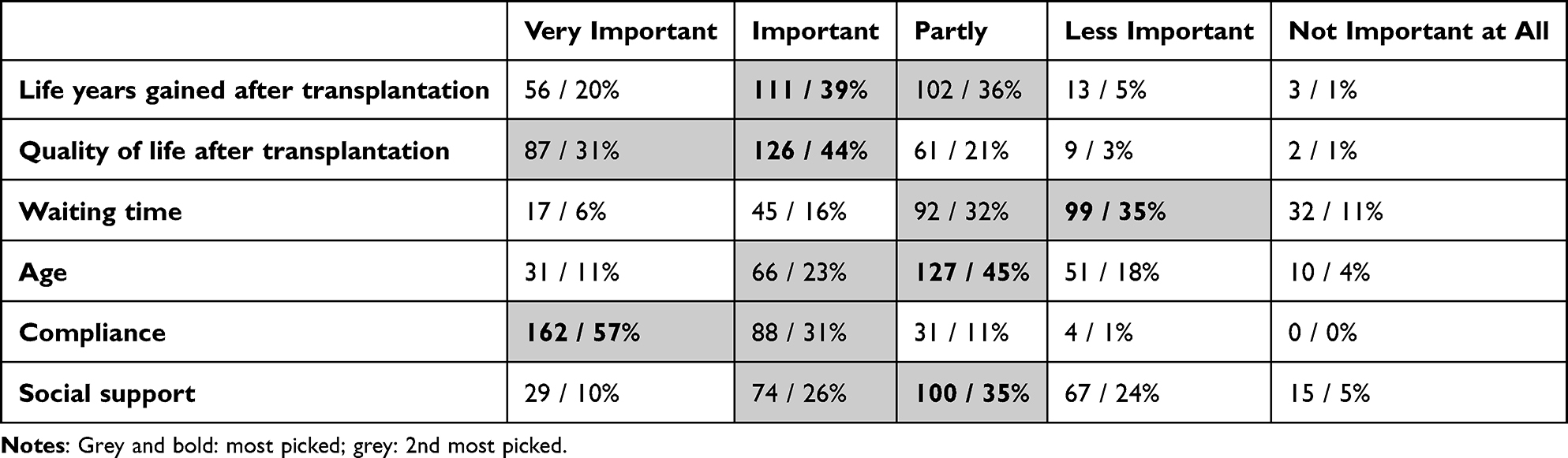 |
Table 4 Importance Directly Attributed to the Attributes of the DCE |
Discussion
This is the first study to conduct a DCE targeting transplant patients and their relatives on the topic of donor organ allocation independent of organ type. In the attribute “life years gained after transplantation” (Gain), participants clearly preferred 10 (β-coefficient: 0.498) and 15 (β-coefficient: 0.524) years of additional life expectancy after transplantation over the reference group of 5 years. Furthermore, there was no inherent preference when comparing 10 and 15 additional years with each other. Interestingly, when looking at the subgroups, relatives and waitlisted patients showed no preference for this attribute, which was in return highly important to transplanted patients. This confirms earlier qualitative research, in which a preference toward longevity of the donor organ by transplantation patients has been identified, predominantly under compliance aspects.9 The differences in the preferences between wait-listed patients and patients after transplantation may be rooted in the fact that posttransplant patients have already experienced a gain in quality of life due to a successful transplant and can therefore focus on prolonging their life, while wait-listed patients still feel a more persistent need to improve their quality of life. This is further reflected in how the participants are restricted by their current situation, where the posttransplant patients are less restricted (17% heavily restricted) than the wait-listed patients (73% heavily restricted) and those represented by relatives (40% heavily restricted).
Concerning quality of life after transplantation (QoL), both “moderate” (β = 1.477) and “good” (β = 1.252) levels were of nearly equally high and significant importance compared to the reference group of “bad”. While there were clear cutoff points in the minds of the participants, their preferences were influenced by the understanding that people will often not experience the optimal outcomes of transplantation. However, these candidates are still considered valuable and worthy of an organ. An earlier DCE with transplantation clinicians showed that a significant improvement of the quality of life with a transplant was of high importance for these patients as well.21
No significant differences were observed in the “waiting time” attribute. In an earlier study, waiting time was identified as a potential proxy for both fairness and urgency, as the link between these two aspects is very clear and easy to make.5 An earlier DCE21 identified this attribute as significant; however, it used a much longer timeframe as levels (3, 5 and 8 years) since the authors focused on renal patients. With the availability of dialysis as an organ replacement therapy in the field of kidney transplantation, waiting time in this context does not refer to a life-or-death situation but rather a continuous decrease in quality of life before transplantation.
The age of the recipient stands out when looking at the preferences associated with it. While a clear and understandable trend can be observed with preferences toward younger recipients (with 25 years > 40 years > 70 years), a potential recipient aged 55 years is of the same priority as a patient aged 25 years. A possible explanation for this could be that a large proportion of this cohort (median 50 years) might feel represented by the recipient aged 55, as 88 participants (30.9%) were between 50 and 59 years old at the time of the survey. Furthermore, 30.4% of all deceased donor organs are allocated to participants between 56 and 64 years of age,22 which supports the assumption that participants may be biased toward believing that these patients are especially suitable for transplantation. The analysis of subgroups showed that the preferences for young (25 years) or middle-aged (55 years) candidates and the dislike of candidates aged 40 and 70 years can be seen in various groups (women, under 50 years, transplant patients, relatives of patients). An analysis of age groups (<50 vs 50+) showed that the recipient’s age is less important in the older age group than in the younger group. An earlier DCE on public preferences in organ allocation identified a clear downward trend in preference for older recipients.12 This is definitely a field where deeper, qualitative research could yield more information, as earlier quantitative studies with patients have yielded divergent results regarding the importance of (younger) age.5,23,24
Earlier studies have identified that aspects of compliance are especially important to patients in regard to the allocation of donor organs,9 which can be confirmed with this DCE, where aspects of noncompliance account for the highest impact on the allocation decision of the participants. Transplantation patients have been identified as perceiving donor organs as important gifts, with the omnipresent thought that allocation to one patient means non-allocation to the many others who are waiting. The loss of organs due to noncompliance is therefore seen as unacceptable and those patients are seen as undeserving; these findings can be supported by our DCE.
Social support was assessed as important in an earlier DCE.21 This can be confirmed by this study, where patients with social support are preferred over those without social support.
During the course of this study, participants had to decide their preferences in a multitude of different trade-offs. In qualitative studies conducted prior to this DCE, the aspect of “fairness” was often mentioned by many different stakeholders, and there are many different interpretations of what the “fair” allocation of donor organs is. Some have advocated, that the principle of a waiting list is fair; ie, “first come, first serve.”.9 Others believed that it is fair to allocate organs only to the most urgent recipients to minimize the number of deaths of those on the waiting list.9 Then there is a group of people, who believe that in case there are multiple equally suitable matches of one donor organ to several recipients, a die should be rolled in order to guarantee true egalitarianism.25 Another opinion that has been expressed mainly by patients gives the highest priority in donor organ allocation to those patients who have demonstrated the highest degree of compliance and who are aware of the gift they are about to receive.9 Interestingly, this study confirms the high priority given by patients and their families to recipients who demonstrate compliance with regard to their prescribed medical treatment. Furthermore, the results of this questionnaire confirm previous qualitative work that have identified an increase in quality of life to be of higher priority than an increase in life years gained by transplantation.9 This was confirmed not only by the current DCE, but also by the self-attributed importance of the participants to the respective attributes (see Table 4).
Strengths and Limitations
To recruit a large number of participants for this study, social media channels of the BDO were used for recruitment, as well as their member’s magazine and their email newsletter. This approach provided us with a strong and reliable sample size and ensured that our survey was spread not only among those patients and relatives who became members of the BDO, but also to those who only follow their work on social media to stay informed but have decided against a more active membership. As a limitation, the actual number of participants reached with this questionnaire and the resulting conversion rate can only be estimated. As in all similar studies, the recruitment process may have introduced a certain degree of selection bias.
The lack of supervision and direct contact with participants in this online survey may have resulted in otherwise potentially avoidable uncertainties and insecurities due to the hypothetical dilemmas faced in this DCE. To mitigate these effects, a phone number and an email address were provided as means by which to contact the authors in such cases. However, we acknowledge that this is not as accessible as having someone directly present while filling out the survey.
Conclusion
This questionnaire and the related DCE provide unique insight into a highly relevant perspective of transplant patients and their relatives regarding the allocation of deceased donor organs, which is required for the improvement of donor organ policies. Patients and their relatives are the individuals who are most affected by the ubiquitous donor organ shortage and practical decisions made regarding donor organ allocation. It is striking that transplant patients and their relatives give the highest priority in donor organ allocation to compliance and quality of life aspects, while waiting time is not shown to be important.
Abbreviations
DCE, discrete choice experiment; BDO, Federal Association of the Organ-Transplanted (German: Bundesverband der Organtransplantierten); CL, Conditional Logit Model; MXL, Mixed Logit Model; LCA, Latent Class Analysis.
Ethics Approval and Informed Consent
This study received ethics approval from the ethics committee of Hannover Medical School (vote number: 7921_BO_K_2018). All participants provided informed consent for the use and publication of their questionnaires for the purpose of this study.
Acknowledgments
The authors thank the Federal Association of the Organ-transplanted/Bundesverband der Organtransplantierten e.V. for their support and collaboration.
Funding
This study was funded by the German Federal Ministry of Education and Research (grant number: 01EH1603B). This publication is funded by the Deutsche Forschungsgemeinschaft (DFG) as part of the “Open Access Publikationskosten” program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bezinover D, Saner F. Organ transplantation in the modern era. BMC Anesthesiol. 2019;19:32. doi:10.1186/s12871-019-0704-z
2. Calne RY. Organ transplantation has come of age. Sci Prog. 2010;93(2):141–150. doi:10.3184/003685010X12708274571283
3. Persad G, Wertheimer A, Emanuel EJ. Principles for allocation of scarce medical interventions. Lancet. 2009;373(9661):423–431. doi:10.1016/S0140-6736(09)60137-9
4. Schaubel DE, Guidinger MK, Biggins SW, et al. Survival benefit-based deceased-donor liver allocation. Am J Transplant. 2009;9(4 Pt 2):970–981. doi:10.1111/j.1600-6143.2009.02571.x
5. Bartling T, Oedingen C, Kohlmann T, Schrem H, Krauth C. Comparing preferences of physicians and patients regarding the allocation of donor organs: a systematic review. Transplant Rev. 2020;34(1):100515. doi:10.1016/j.trre.2019.100515
6. Clark MD, Gumber AK, Leech D, et al. Prioritising patients for renal transplantation? Analysis of patient preferences for kidney allocation according to ethnicity and gender. Diversity Health Care. 2009;6:181–191.
7. Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. doi:10.1002/hec.1697
8. Clark MD, Determann D, Petrou S, Moro D. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2014;32(9):883–902. doi:10.1007/s40273-014-0170-x
9. Bartling T, Oedingen C, Kohlmann T, Schrem H, Krauth C. How Should Deceased Donor Organs Be Allocated? The Patient’s Perspective Derived from Semi-Structured Interviews. PPA. 2022;16:2375–2385. doi:10.2147/PPA.S372603
10. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
11. Oedingen C, Bartling T, Krauth C. Public, medical professionals and patients preferences for the allocation of donor organs for transplantation: study protocol for discrete choice experiments. BMJ Open. 2018;8:e026040. doi:10.1136/bmjopen-2018-026040
12. Oedingen C, Bartling T, Schrem H, Mühlbacher AC, Krauth C. Public preferences for the allocation of donor organs for transplantation: a discrete choice experiment. Soc Sci Med. 2021;287:114360. doi:10.1016/j.socscimed.2021.114360
13. Oedingen C, Bartling T, Dierks M-L, Mühlbacher AC, Schrem H, Krauth C. Public preferences for the allocation of donor organs for transplantation: focus group discussions. Health Expect. 2020;23:670–680. doi:10.1111/hex.13047
14. Gunst RF, Mason RL. Fractional factorial design. Wiley Interdiscip Rev Comput Stat. 2009;1(2):234–244. doi:10.1002/wics.27
15. Johnson R, Orme B. Getting the Most from CBC: sawtooth Software Research Paper Series. 2003 Available from: https://sawtoothsoftware.com/resources/technical-papers/getting-the-most-from-cbc
16. Orme B. Sample Size Issues for Conjoint Analysis Studies: sawtooth Software Technical Paper. 1998 Available from: https://sawtoothsoftware.com/resources/technical-papers/sample-size-issues-for-conjoint-analysis-studies (updated version from 2019)
17. Kuhfeld WF Experimental Design: efficiency, Coding, and Choice Designs: SAS Technical Papers MR-2010C. Available from: http://support.sas.com/techsup/technote/mr2010c.pdf.
18. Gensch DH, Recker WW, Multinomial T. Multiattribute Logit Choice Model. J Marketing Res. 1979;16(1):124. doi:10.2307/3150883
19. McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Frontiers in Econometrics. Academic Press; 1974:104–143.
20. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical Methods for the Analysis of Discrete Choice Experiments: a Report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
21. Ladin K, Emerson J, Butt Z, et al. How important is social support in determining patients’ suitability for transplantation? Results from a National Survey of Transplant Clinicians. J Med Ethics. 2018;44(10):666–674. doi:10.1136/medethics-2017-104695
22. Eurotransplant. Transplants (deceased donor) in Germany, by year, by characteristics. Available from: https://statistics.eurotransplant.org/index.php?search_type=transplants&search_organ=&search_region=Germany&search_period=2021&search_characteristic=recipient+age&search_text=&search_collection=.
23. Geddes CC, Rodger RSC, Smith C, Ganai A. Allocation of deceased donor kidneys for transplantation: opinions of patients with CKD. Am J Kidney Dis. 2005;46(5):949–956. doi:10.1053/j.ajkd.2005.07.031
24. Umgelter KS, Tobiasch M, Anetsberger A, Blobner M, Thorban S, Umgelter A. Donor organ distribution according to urgency of need or outcome maximization in liver transplantation. A questionnaire survey among patients and medical staff. Transpl Int. 2015;28(4):448–454. doi:10.1111/tri.12512
25. Bartling T, Oedingen C, Schrem H, Kohlmann T, Krauth C. ‘As a surgeon, I am obliged to every single patient’: evaluation of focus group discussions with transplantation physicians on the allocation of donor organs. Curr Opin Organ Transplant. 2021;26(5):459–467. doi:10.1097/MOT.000000000000090
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.