Back to Journals » Clinical Ophthalmology » Volume 16
Serum Vitamin D Levels and Status in Thai Optic Neuritis Subjects: A Case-Control Study
Authors Puangsricharoen B, Vanikieti K, Jindahra P ![]() , Padungkiatsagul T
, Padungkiatsagul T ![]()
Received 25 July 2022
Accepted for publication 30 September 2022
Published 12 October 2022 Volume 2022:16 Pages 3381—3389
DOI https://doi.org/10.2147/OPTH.S383703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Busayanut Puangsricharoen,1 Kavin Vanikieti,1 Panitha Jindahra,2 Tanyatuth Padungkiatsagul1
1Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Tanyatuth Padungkiatsagul, Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Bangkok, 10400, Thailand, Tel +662 201 1526, Fax +662 201 2729, Email [email protected]
Objective: To measure serum total vitamin D or 25-hydroxyvitamin D [25(OH)D] levels and status in immune-based optic neuritis (ON) including neuromyelitis optica spectrum disorder (NMOSD)-ON, myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD)-ON, autoimmune-ON, and idiopathic-ON and compare them with age- and sex-matched healthy controls. The secondary objective was to analyze the association between serum 25(OH)D levels and ON attack severity (nadir best-corrected visual acuity; nadir BCVA).
Materials and Methods: This was a single-center, case–control study. We enrolled 59 subjects (19 NMOSD-ON, 6 MOGAD-ON, 11 autoimmune-ON, 23 idiopathic-ON) diagnosed with acute immune-based ON (any ON attacks) over 11 years. Electronic medical records were reviewed and demographic data (age at sampling, sex, aquaporin-4 immunoglobulin (AQP4-IgG); myelin oligodendrocyte glycoprotein immunoglobulin G (MOG-IgG); other biomarkers of autoimmune disorders), ON attack severity (nadir BCVA), and serum 25(OH)D levels in the acute phase of ON were collected. Serum 25(OH)D levels of 236 age- and sex-matched healthy controls were assessed.
Results: Mean serum 25(OH)D levels were significantly lower in each group of immune-based ON compared with healthy controls (p < 0.001 for each ON group). However, mean serum 25(OH)D levels were not significantly different between four ON groups (NMOSD-ON, 20.18± 5.90 ng/mL; MOGAD-ON, 23.07± 4.94 ng/mL; autoimmune-ON, 21.14± 5.29 ng/mL; idiopathic-ON, 19.56± 5.12 ng/mL; p = 0.525). All immune-based ON subjects had vitamin D insufficiency or vitamin D deficiency. The prevalences of vitamin D insufficiency and vitamin D deficiency were significantly higher than in healthy controls in each ON group (both p < 0.05 in each ON group). No associations were observed between serum 25(OH)D levels and ON attack severity (nadir BCVA).
Conclusions: Thai immune-based ON subjects had lower serum 25(OH)D levels and higher prevalence of vitamin D insufficiency and vitamin D deficiency compared with age- and sex-matched healthy controls. Serum 25(OH)D levels were not associated with ON attack severity (nadir BCVA). We highly recommend that serum 25(OH)D levels be screened in all subjects with acute immune-based ON.
Keywords: vitamin D insufficiency, vitamin D deficiency, optic neuritis, NMOSD, MOGAD, autoimmune-optic neuritis
Introduction
Optic neuritis (ON) is an acute inflammation of the optic nerve based on an immune-based process. The worldwide incidence of ON ranges from 1 to 6.4 per 100,000 adults.1,2 Typical ON, also known as multiple sclerosis-associated ON, is commonly reported in Europeans, whereas idiopathic-ON is widely described among Asians.3,4 Correspondingly, idiopathic-ON is the most common etiology of ON in Thais (51.5%), followed by neuromyelitis optica spectrum disorder (NMOSD, 30.9%), autoimmune disorder (9.9%), myelin oligodendrocyte glycoprotein antibody-associated disorder (MOGAD, 5.3%), multiple sclerosis (MS, 1.8%), and postinfection (0.6%).5
Recent studies reported associations between vitamin D and various immune-based diseases. The proposed mechanism might involve low serum vitamin D levels associated with the dysregulated suppression of innate immune responses.6 Several studies have shown that serum vitamin D levels were low in subjects with autoimmune disorders including systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA).7 In addition, low serum vitamin D levels are a well-established risk factor for the development of demyelinating diseases such as MS and NMOSD.8–11 Serum vitamin D levels were significantly lower in patients with MS and NMOSD compared to healthy controls.7,11 Another study reported that vitamin D insufficiency and deficiency were frequent in Thais with clinically isolated syndrome (CIS), MS, and NMOSD.12 Despite the significant associations between low serum vitamin D levels and several ocular inflammatory diseases such as dry eye syndrome, thyroid eye disease, vernal keratoconjunctivitis, allergic conjunctivitis, and uveitis,13 ON and its association with vitamin D is poorly understood.
The primary objective of this study was to measure the serum total vitamin D or 25-hydroxyvitamin D [25(OH)D] levels and their status in immune-based ON subjects and compare this with serum 25(OH)D levels and status in age- and sex-matched healthy controls. The secondary objective was to study the association between serum 25(OH)D levels and ON attack severity (nadir best-corrected visual acuity; nadir BCVA) in Thai immune-based ON. To the best of our knowledge, this is the first study to assess serum 25(OH)D levels and status in NMOSD with a focus on subjects with ON exclusively, as well as assessing vitamin D levels and status in MOGAD-ON, autoimmune-ON, and idiopathic-ON. Thus, it is the first study to analyze vitamin D levels and status among the most comprehensive causes of immune-based ON.
Materials and Methods
This study followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand (IRB number: COA.MURA2021/875), which waived the need for written informed consent from the subjects and controls due to the retrospective nature of the study. All confidential data were kept in our database.
Subjects and Controls and Diagnoses
This was a case-control study of serum 25(OH)D levels and status in Thai immune-based ON subjects. We retrospectively reviewed the electronic medical records of subjects who were diagnosed with acute immune-based ON (any ON attacks) in the neuro-ophthalmology clinic, Faculty of Medicine Ramathibodi Hospital, Bangkok, Thailand between January 2011 and January 2022. The subject’s inclusion and exclusion criteria are described below.
Inclusion Criteria
- All Thai acute immune-based ON subjects (any ON attacks)
- Available serum 25(OH)D levels tested within 2 weeks of ON attack with age at sampling ≥ 16 years.
Exclusion Criteria (Any of the Followings)
- Subjects who were treated with systemic glucocorticoids before sampling within the past 3 months
- Subjects with disorders that might affect serum 25(OH)D levels including renal disease, liver disease, or pregnancy
- Subjects who were taking any medications including immunosuppressive drugs or supplements that might affect serum 25(OH)D levels
- Subjects whose affected eye had visually significant cataracts and/or ocular diseases (other than ON) affecting the nadir BCVA.
Demographic data (age at sampling and sex), autoantibody serology results (aquaporin-4 immunoglobulin (AQP4-IgG); myelin oligodendrocyte glycoprotein immunoglobulin G (MOG-IgG); antinuclear antibody (ANA); anti-double-stranded DNA antibody (anti-dsDNA); anti-centromere antibody, anti-Ro/SSA, anti-La/SSB, rheumatoid factors (RF); c-antineutrophil cytoplasmic antibody (c-ANCA); anti-Jo1 antibody), ON attack severity (nadir BCVA measured by Snellen chart), and serum 25(OH)D levels during the acute phase of ON were reviewed. Immune-based ON subjects were categorized into four groups in this study: NMOSD-ON, MOGAD-ON, autoimmune-ON, and idiopathic ON.
NMOSD was diagnosed based on the 2015 International Panel for NMO Diagnostic criteria.14 MOGAD was diagnosed based on the 2018 MOG-IgG-associated disorder diagnostic criteria.15 Serum AQP-4-IgG and MOG-IgG were detected using the gold standard live flow cytometry cell-based assays (CBAs). Autoimmune-ON was further classified into two subgroups: specific and non-specific autoimmune disorders. Specific autoimmune disorders included SLE, Sjogren’s syndrome, RA, c-ANCA, anti-centromere antibody, and anti-Jo1 antibody, and non-specific autoimmune disorders were defined as subjects with positive ANA but which did not fulfill any of the criteria for a specific autoimmune disorder. SLE, Sjogren’s syndrome, and RA were diagnosed based on the 2019 American College of Rheumatology/European League Against Rheumatism Collaborative (ACR/EULAR) initiative classification criteria for SLE, the 2012 American College of Rheumatology classification criteria for Sjogren’s syndrome, and the 2010 ACR/EULAR classification criteria for RA, respectively.16–18 Idiopathic-ON was diagnosed when no cause was identified despite comprehensive investigation.
The control group included age- and sex-matched healthy controls with available serum 25(OH)D levels between January 2002 and March 2022 were randomly recruited from the Data Health for Analysis Informatics Section, Faculty of Medicine Ramathibodi Hospital, Mahidol University. A 4:1 ratio of controls to subjects was used to determine the number of age- and sex-matched controls enrolled in this study. They had no obvious disorders including renal disease, liver disease, or pregnancy and were not taking any medications or supplements that might affect serum 25(OH)D levels. Demographic data (age at sampling, sex) and serum 25(OH)D levels were reviewed from the control group.
Serum 25(OH)D Levels and Status
Blood samples were obtained during the acute phase of ON (within 14 days of ON attack onset) and transferred to a central laboratory where they were kept at −80°C. Serum total vitamin D levels or 25(OH)D levels (ng/mL) were measured by an in vitro automated chemiluminescent immunoassay analyzer LIAISON® XL (DiaSorin, Sialuggia, Italy).
For serum 25(OH)D status, a serum 25(OH)D level below 20 ng/mL, 20 to < 30 ng/mL, and ≥ 30 ng/mL were defined as vitamin D deficiency, vitamin D insufficiency, and vitamin D sufficiency, respectively.19 These are summarized in Table 1.
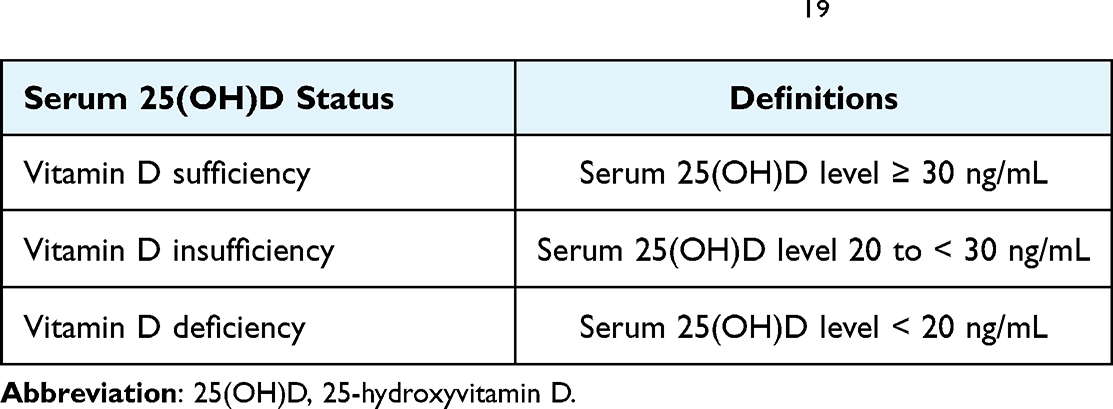 |
Table 1 Definitions of Each Serum 25(OH)D status19 |
Statistical Analysis
Categorical variables are presented as frequencies (percentages). Continuous variables are expressed as the mean ± standard deviation (SD) for normally distributed variables or median (min, max) for non-normally distributed variables. Statistical comparisons of mean age at sampling and mean serum 25(OH)D levels between each group of immune-based ON and healthy controls were performed using an independent t-test. Mean serum 25(OH)D levels were compared among the four ON groups by analysis of variance (ANOVA) test. The Chi-squared test was used for the comparison of categorical variables (sex, serum 25(OH)D status). Snellen BCVA measurements were converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. To analyze visual acuity levels of counting fingers, hand motion, light perception, and no light perception, the BCVA values were defined as 2.6, 2.7, 2.8, and 2.9 logMAR, respectively.20,21 To assess ON attack severity, the nadir BCVA was adjusted for age at sampling and sex using multiple linear regression. Spearman’s rho correlation coefficient was used to analyze the associations between the number of previous ON attacks and ON attack severity (nadir BCVA) and the associations between serum 25(OH)D levels and ON attack severity (nadir BCVA). Statistical analyses were conducted and analyzed using IBM SPSS version 27.0 software (IBM, Armonk, New York, USA). P-values < 0.05 were considered statistically significant.
Results
The medical records of 59 immune-based ON subjects and 236 age- and sex-matched healthy controls were retrospectively reviewed. Immune-based ON subjects were categorized into four groups in this study. The first group consisted of 19 subjects diagnosed with NMOSD-ON. Eighteen subjects (18/19, 94.7%) had positive serum AQP4-IgG. The remaining subject had acute unilateral ON with enhancement extending over more than one-half of the optic nerve length on neuroimaging. This subject had a history of acute myelitis with intramedullary lesion extending 4 contiguous segments on neuroimaging. The second group consisted of 6 MOGAD-ON subjects, which were all confirmed by positive serum MOG-IgG. The third group consisted of 11 autoimmune-ON subjects including specific and non-specific autoimmune disorders. The fourth group consisted of 23 subjects with idiopathic-ON. Overall mean age at sampling of 59 immune-based ON subjects and 236 healthy controls were 48.98±17.63 and 48.98±17.51 years, respectively (p = 1.000). Overall mean serum 25(OH)D levels of 59 immune-based ON subjects and 236 healthy controls were 20.41±5.37 and 31.72±2.21 ng/mL, respectively (p < 0.001). There was no difference in age at sampling and sex between each ON group and its healthy control group (Table 2).
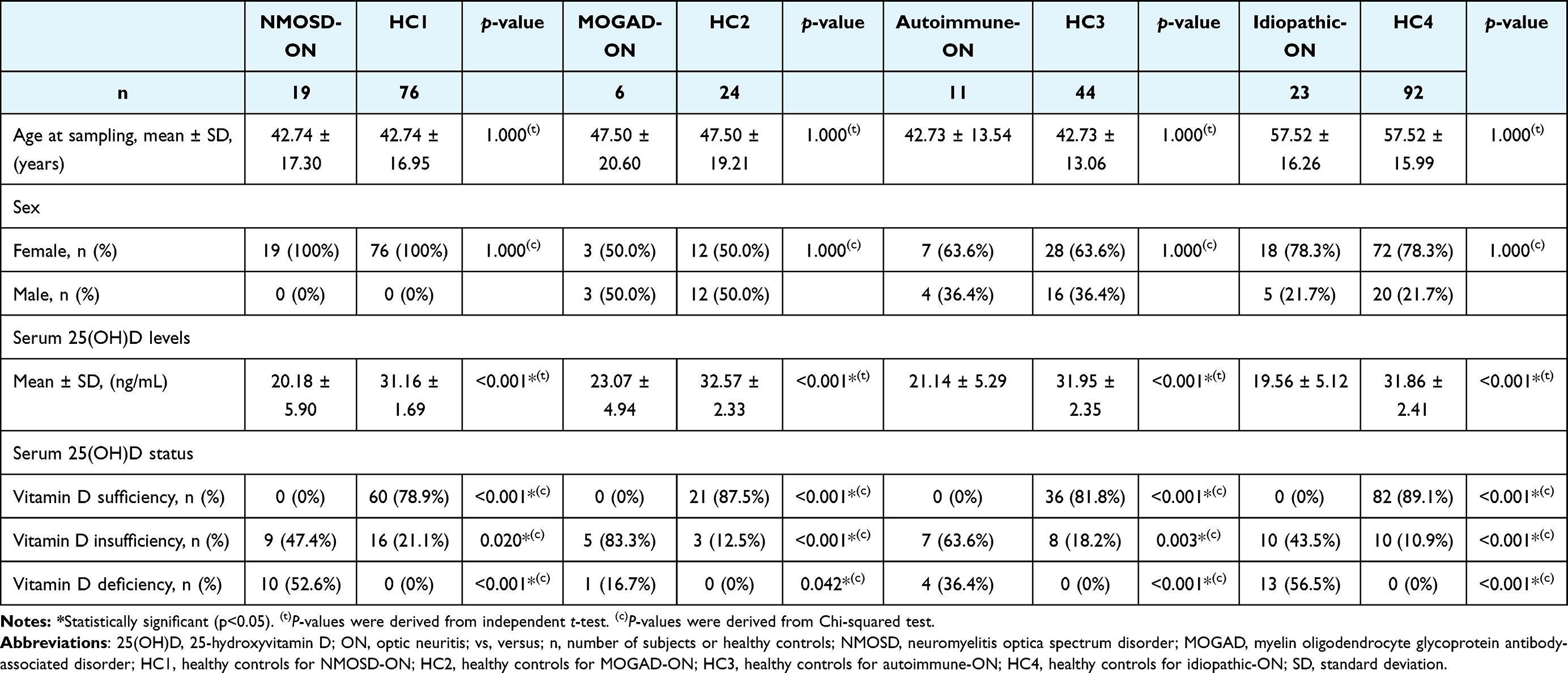 |
Table 2 Demographic Data (Age at Sampling, Sex), Serum 25(OH)D Levels, and Status of Immune-Based ON Vs Healthy Controls |
Comparison of Serum 25(OH)D Levels and Status Between Immune-Based ON Subjects, and Age- and Sex-Matched Healthy Controls (Table 2)
Comparison of Serum 25(OH)D Levels and Status Between 19 NMOSD-ON Subjects, and 76 Age- and Sex-Matched Healthy Controls
The mean serum 25(OH)D levels were significantly lower in subjects with NMOSD-ON compared with age- and sex-matched healthy controls (20.18±5.90 ng/mL vs 31.16±1.69 ng/mL; p < 0.001). For serum 25(OH)D status, approximately half of the NMOSD-ON subjects had vitamin D insufficiency, which was significantly higher than that of healthy controls (47.4% vs 21.1%; p = 0.020). Most NMOSD-ON subjects also had a significantly higher prevalence of vitamin D deficiency than the healthy controls (52.6% vs 0%; p < 0.001).
Comparison of Serum 25(OH)D Levels and Status Between 6 MOGAD-ON Subjects, and 24 Age- and Sex-Matched Healthy Controls
MOGAD-ON subjects had significantly lower mean serum 25(OH)D levels than age- and sex-matched healthy controls (23.07±4.94 ng/mL vs 32.57±2.33 ng/mL; p < 0.001). For serum 25(OH)D status, MOGAD-ON subjects had significantly higher prevalence of vitamin D insufficiency and vitamin D deficiency than the healthy controls (83.3% vs 12.5%; p < 0.001 and 16.7% vs 0%; p = 0.042, respectively).
Comparison of Serum 25(OH)D Levels and Status Between 11 Autoimmune-ON Subjects, and 44 Age- and Sex-Matched Healthy Controls
The mean serum 25(OH)D levels were significantly lower in autoimmune-ON subjects compared with age- and sex-matched healthy controls (21.14±5.29 ng/mL vs 31.95±2.35 ng/mL; p < 0.001). Compared with healthy controls, nearly two-thirds of autoimmune-ON subjects had vitamin D insufficiency and approximately one-third of autoimmune-ON subjects had vitamin D deficiency, which were more common than in the healthy controls (63.6% vs 18.2%; p = 0.003 and 36.4% vs 0%; p < 0.001, respectively).
Comparison of Serum 25(OH)D Levels and Status Between 23 Idiopathic-ON Subjects, and 92 Age- and Sex-Matched Healthy Controls
Mean serum 25(OH)D levels in the idiopathic-ON subjects were significantly lower than in the age- and sex-matched healthy controls (19.56±5.12 ng/mL vs 31.86±2.41 ng/mL; p < 0.001). Correspondingly, the prevalence of vitamin D insufficiency and vitamin D deficiency in idiopathic-ON subjects were also significantly higher than in their control groups (43.5% vs 10.9%; p < 0.001 and 56.5% vs 0%; p < 0.001, respectively).
Comparison of Serum 25(OH)D Levels and Status Among Immune-Based ON
The mean serum 25(OH)D levels were similar among the four groups of immune-based ON (NMOSD-ON, MOGAD-ON, autoimmune-ON, and idiopathic-ON). For serum 25(OH)D status, the prevalence of vitamin D insufficiency and vitamin D deficiency were comparable between the four ON groups. Comparisons of serum 25(OH)D levels and status among immune-based ON are summarized in Table 3.
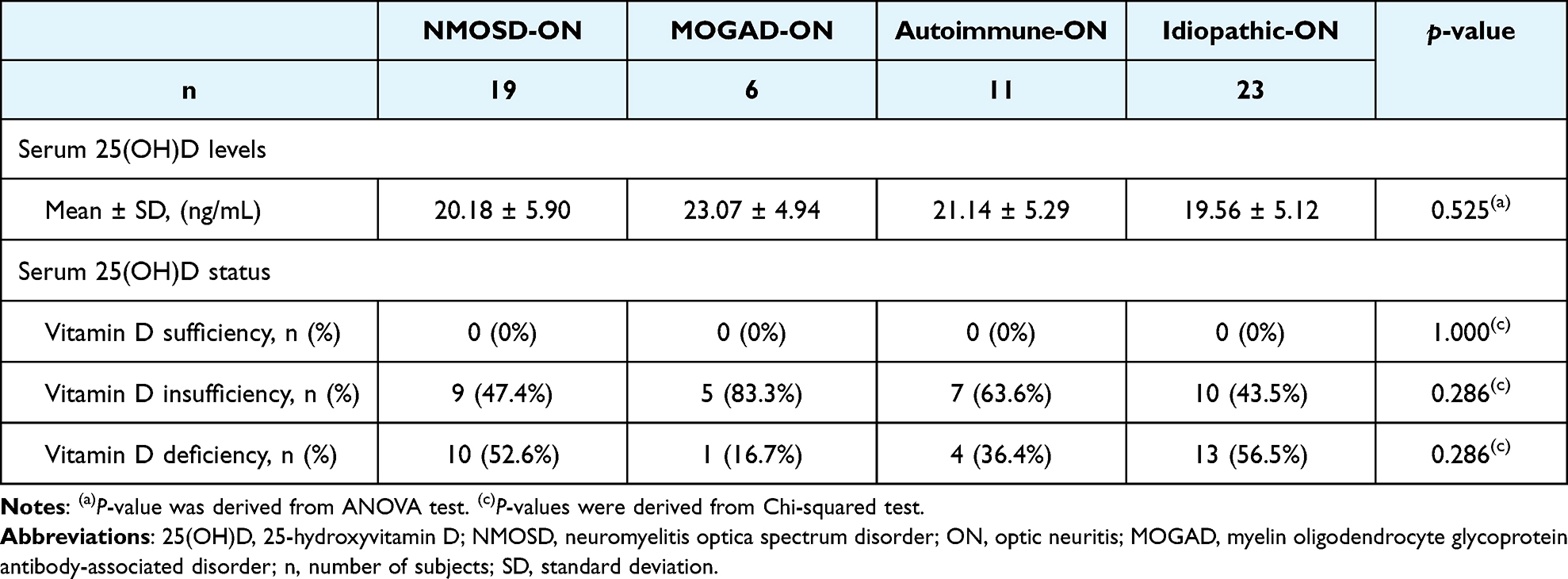 |
Table 3 Comparisons of Serum 25(OH)D Levels and Status Among NMOSD-ON, MOGAD-ON, Autoimmune-ON, and Idiopathic-ON |
Association Between Serum 25(OH)D Levels and ON Attack Severity (Nadir BCVA) in Immune-Based ON
There were 23 NMOSD-ON affected eyes, 9 MOGAD-ON affected eyes, 13 autoimmune-ON affected eyes, and 31 idiopathic-ON affected eyes included in this analysis. Because the number of previous ON attacks was not significantly associated with the nadir BCVA (r = 0.316, p = 0.142; r = 0, p = 1.000; r = 0, p = 1.000; r = −0.186, p = 0.315 for NMOSD-ON affected eyes, MOGAD-ON affected eyes, autoimmune-ON affected eyes, and idiopathic-ON affected eyes, respectively), all ON attacks were analyzed together. The median nadir BCVA during the acute ON attack of NMOSD-ON affected eyes, MOGAD-ON affected eyes, autoimmune-ON affected eyes, and idiopathic-ON affected eyes were 2.6 (0.55, 2.7) logMAR, 1.3 (1.0, 2.6) logMAR, 2.6 (1.0, 2.6) logMAR, and 1.3 (0.7, 2.6) logMAR, respectively. After adjusting for the clinical factors of age at sampling and sex, serum 25(OH)D levels showed no association with ON attack severity (nadir BCVA) in NMOSD-ON affected eyes (r = 0.125, p = 0.569), MOGAD-ON affected eyes (r = −0.547, p = 0.127), autoimmune-ON affected eyes (r = 0.177, p = 0.563), and idiopathic-ON affected eyes (r = 0.076, p = 0.683). In summary, no associations were observed between serum 25(OH)D levels and ON attack severity (nadir BCVA) in each group of immune-based ON.
Discussion
To the best of our knowledge, this is the first study to analyze serum 25(OH)D levels and status among the most comprehensive causes of immune-based ON. The main outcomes of our study were as follows: 1) all immune-based ON subjects (NMOSD-ON, MOGAD-ON, autoimmune-ON, idiopathic-ON) had significantly lower 25(OH)D levels than their age- and sex-matched healthy controls; and 2) vitamin D insufficiency and vitamin D deficiency were remarkably common in immune-based ON subjects compared with age- and sex-matched healthy controls.
There was a lack of evidence for serum 25(OH)D levels and status in the NMOSD-ON population. A previous study of Thai subjects reported a mean serum 25(OH)D level of 23.54±9.30 ng/mL in NMOSD subjects. They also revealed that 43.42% and 35.52% of NMOSD subjects had vitamin D insufficiency and vitamin D deficiency, respectively.12 However, their study did not exclusively analyze NMOSD-ON subjects and there was no healthy control group for comparisons. The current study demonstrated that mean serum 25(OH)D levels were significantly lower in Thai NMOSD-ON subjects compared with age- and sex-matched healthy controls. We also revealed that the prevalences of vitamin D insufficiency and vitamin D deficiency were significantly higher in NMOSD-ON subjects compared with healthy controls of the same age and sex. These findings are in accord with previous reports. A previous study in Chinese subjects showed significantly lower serum 25(OH)D levels in NMOSD subjects compared with healthy controls.22 Additionally, studies in Chinese subjects and Korean subjects reported that serum 25(OH)D3 levels, another form of vitamin D, were significantly lower in NMOSD subjects compared with healthy controls.11,23 In contrast to our results, one study in Indonesian subjects showed that serum 25(OH)D levels in NMOSD subjects were not significantly different from those of healthy controls.24 Nevertheless, this study did not exclude NMOSD subjects or healthy controls who were taking vitamin D supplements. Moreover, the daily dose of vitamin D intake in NMOSD subjects was significantly higher than in the healthy controls in their study. This might explain the different results between the study findings. Although there is no conclusive hypothesis for the role of vitamin D in NMOSD pathogenesis, it was proposed that low serum vitamin D levels may be associated with immune dysregulation that involves innate immune suppression as described in MS.6 Inadequate serum vitamin D leads to a reduction in B-cell apoptosis and improper elimination of interleukin-6 and CD-19, both of which are related to NMOSD pathogenesis.25
We found that MOGAD-ON subjects had significantly lower mean serum 25(OH)D levels than age- and sex-matched healthy controls. This finding is comparable with previous studies of serum 25(OH)D levels in other demyelinating diseases such as MS and NMOSD, which demonstrated that serum 25(OH)D levels were significantly lower than those in healthy controls.22,23,26 The association between serum vitamin D and MOGAD-ON remains unclear; however, it may share the same underlying mechanism as other demyelinating diseases.6,25
Our results demonstrated that mean serum 25(OH)D levels in autoimmune-ON subjects were significantly lower than in age- and sex-matched healthy controls, which is consistent with previous reports of other autoimmune disorders such as SLE.7,27 Those studies reported a significantly lower mean serum 25(OH)D level of 21.60 ng/mL in African American and Caucasian subjects diagnosed with SLE compared with 27.40 ng/mL in healthy controls. The function of vitamin D as an immune modulator in SLE and its role in autoimmune-ON pathogenesis might share a common mechanism.7
We observed significantly lower mean serum 25(OH)D levels in idiopathic-ON subjects than in healthy controls of the same age and sex. This finding is comparable with previous studies of serum 25(OH)D levels in other ocular inflammatory diseases such as dry eye syndrome, where serum 25(OH)D levels were significantly lower than in healthy controls.28,29 Vitamin D was associated with T-helper cell inhibition and cytotoxic T-cell proliferation leading to a decrease in the production of proinflammatory cytokines.30 Presumably, low vitamin D levels may have a role in the inflammatory processes of dry eye syndrome and idiopathic-ON.
In our study, the prevalences of vitamin D insufficiency and vitamin D deficiency were significantly higher in immune-based ON subjects than in age- and sex-matched healthy controls. Therefore, serum 25(OH)D levels should be assessed in all acute immune-based ON subjects. To avoid vitamin D insufficiency and vitamin D deficiency-related complications such as osteoporosis, cardiovascular disease, and cancer, maintaining serum 25(OH)D at a level of 30 ng/mL or more is favorable.31 This should be aided by the increased accessibility of serum 25(OH)D laboratory tests.
No associations were observed between serum 25(OH)D levels and ON attack severity (nadir BCVA) in each group of immune-based ON. The present study reported that serum 25(OH)D levels were not associated with ON attack severity (nadir BCVA) in NMOSD-ON affected eyes, in accord with previous studies describing a dissociation between serum 25(OH)D levels and the Expanded Disability Status Scale (EDSS) in NMOSD.24,32 However, this result was inconsistent with studies in Korean and Chinese subjects, which evaluated serum 25(OH)D3 levels and their association with EDSS in NMOSD subjects.11,23 The difference in the form of vitamin D measured [25(OH)D3 vs 25(OH)D] might explain the differences seen compared with our study. We did not find an association between serum 25(OH)D levels and ON attack severity (nadir BCVA) in MOGAD-ON affected eyes. This finding was in accord with previous studies showing that serum 25(OH)D levels were not associated with the EDSS in demyelinating diseases such as MS and NMOSD.24,32 Additionally, there was no association between serum 25(OH)D levels and ON attack severity (nadir BCVA) in our autoimmune-ON affected eyes as observed in disease activity in other autoimmune disorders such as SLE and RA.33,34 These studies reported no associations between serum 25(OH)D levels and SLE Disease Activity Index (SLEDAI) in SLE or serum 25(OH)D levels and 3-variable Disease Activity Score (DAS28) in RA.33,34 We also found no association between serum 25(OH)D levels and ON attack severity (nadir BCVA) in idiopathic-ON affected eyes, which was consistent with earlier studies in dry eye syndrome.29,35 They reported no associations between serum 25(OH)D levels and Schirmer II test or serum 25(OH)D levels and ocular surface disease index scores in dry eye syndrome.29,35
There were key strengths in this study. To the best of our knowledge, this is the first study to assess vitamin D levels and status in NMOSD with a focus on subjects with ON exclusively, as well as investigating vitamin D levels and status in MOGAD-ON, autoimmune-ON, and idiopathic-ON. Second, it is the first study to analyze vitamin D levels and status among the most comprehensive causes of immune-based ON. Third, we compared serum 25(OH)D levels and status in each ON group with age- and sex-matched healthy controls.
Our study had some limitations. The lack of a comprehensive assessment of other components of visual function including color vision, contrast sensitivity, and visual field testing during ON attack limited the analysis of ON attack severity. The lifestyles of subjects, which might affect serum 25(OH)D levels and status, such as sunlight exposure and dietary were not considered or statistically adjusted for in this study. Future studies should assess the association between serum 25(OH)D levels and other components of visual function during ON attack as well as individual lifestyle factors that affect serum 25(OH)D levels and status. Furthermore, our study had the small number of subjects in MOGAD-ON and autoimmune-ON groups for subgroup analysis. Larger samples are needed to infer more generalizable conclusions.
Conclusions
Serum 25(OH)D levels were significantly lower in immune-based ON subjects compared with age- and sex-matched healthy controls. Furthermore, the prevalences of vitamin D insufficiency and vitamin D deficiency were significantly higher in immune-based ON subjects than in age- and sex-matched healthy controls. Serum 25(OH)D levels were not associated with ON attack severity (nadir BCVA). We highly recommend that serum 25(OH)D levels be screened in all subjects with acute immune-based ON.
Acknowledgments
The authors would like to thank Ms. Dollapas Punpanich, Department of Clinical Epidemiology and Biostatistics, Phramongkutklao College of Medicine, Bangkok, Thailand for her advice on the statistical analyses. We thank J. Ludovic Croxford, PhD, from Edanz (www.edanz.com/ac) for editing a draft of this manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Pau D, Zubidi NAI, Yalamanchili S, et al. Optic neuritis. Eye. 2011;25(7):833–842. doi:10.1038/eye.2011.81
2. Lee JY, Han J, Yang M, et al. Population-based incidence of pediatric and adult optic neuritis and the risk of multiple sclerosis. Ophthalmology. 2020;127(3):417–425. doi:10.1016/j.ophtha.2019.09.032
3. Amezcua L, McCauley JL. Race and ethnicity on MS presentation and disease course. ACTRIMS forum 2019. Mult Scler. 2020;26(5):561–567. doi:10.1177/1352458519887328
4. Wakakura M, Ishikawa S, Oono S, et al. Incidence of acute idiopathic optic neuritis and its therapy in Japan. Optic neuritis treatment trial multicenter cooperative research group (ONMRG). Nippon Ganka Gakkai Zasshi. 1995;99(1):93–97.
5. Vanikieti K, Janyaprasert P, Lueangram S, et al. Etiologies of acute optic neuritis in Thailand: an observation study of 171 patients. Clin Ophthalmo. 2020;14:2935–2942. doi:10.2147/OPTH.S271820
6. Yadav SK, Mindur JE, Ito K, Dhib-Jalbut S. Advances in the immunopathogenesis of multiple sclerosis. Curr Opin Neurol. 2015;28(3):206–219. doi:10.1097/WCO.0000000000000205
7. Agmon-Levin N, Theodor E, Segal RM, Shoenfeld Y. Vitamin D in systemic and organ-specific autoimmune diseases. Clin Rev Allergy Immunol. 2013;45(2):256–266. doi:10.1007/s12016-012-8342-y
8. Acheson ED, Bachrach CA, Wright FM. Some comments on the relationship of the distribution of multiple sclerosis to latitude, solar radiation and other variables. Acta Psychiatr Scand Suppl. 1960;35(147):132–147. doi:10.1111/j.1600-0447.1960.tb08674.x
9. Van der Mei IA, Ponsonby AL, Blizzard L, et al. Regional variation in multiple sclerosis prevalence in Australia and its association with ambient ultraviolet radiation. Neuroepidemiology. 2001;20(3):168–174. doi:10.1159/000054783
10. Van der Mei IA, Ponsonby AL, Dwyer T, et al. Past exposure to sun, skin phenotype, and risk of multiple sclerosis: case-control study. BMJ. 2003;327:316. doi:10.1136/bmj.327.7410.316
11. Min J-H, Waters P, Vincent A, et al. Low levels of vitamin D in neuromyelitis optica spectrum disorder: association with disease disability. PLoS One. 2014;9(9):e107274. doi:10.1371/journal.pone.0107274
12. Jitprapaikulsan J, Siritho S, Prayoonwiwat N. Vitamin D level status in Thai neuromyelitis optica patients. J Neuroimmunol. 2016;295–296:75–78. doi:10.1016/j.jneuroim.2016.03.016
13. Chan HN, Zhang XJ, Ling XT, et al. Vitamin D and ocular diseases: a systematic review. Int J Mol Sci. 2022;23(8):4226. doi:10.3390/ijms23084226
14. Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorder. Neurology. 2015;85(2):177–189. doi:10.1212/WNL.0000000000001729
15. López-Chiriboga AS, Majed M, Fryer J, et al. Association of MOG-IgG serostatus with relapse after acute disseminated encephalomyelitis and proposed diagnostic criteria for MOG-IgG-associated disorders. JAMA Neurol. 2018;75(11):1355–1363. doi:10.1001/jamaneurol.2018.1814
16. Aringer M, Costenbader K, Daikh D, et al. 2019 European league against rheumatism/American college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. 2019;71(9):1400–1412. doi:10.1002/art.40930
17. Shiboski SC, Shiboski CH, Criswell LA, et al. American college of rheumatology classification criteria for Sjögren’s syndrome: a data-driven, expert consensus approach in the SICCA cohort. Arthritis Care Res. 2012;64(4):475–487. doi:10.1002/acr.21591
18. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria. An American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheumatol. 2310;62(9):2569–2581. doi:10.1002/art.27584
19. Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B. Regional variation and determinants of vitamin D status in sunshine-abundant Thailand. BMC Public Health. 2011;11:853. doi:10.1186/1471-2458-11-853
20. Grover S, Fishman G, Anderson R, et al. Visual acuity impairment in patients with retinitis pigmentosa at age 45 years or older. Ophthalmology. 1999;106(9):1780–1785. doi:10.1016/S0161-6420(99)90342-1
21. McAnany J, Genead M, Walia S, et al. Visual acuity changes in patients with Leber congenital amaurosis and mutations in CEP290. JAMA Ophthalmol. 2013;131(2):178–182. doi:10.1001/2013.jamaophthalmol.354
22. Gao M, Yao X, Ding J, et al. Low levels of vitamin D and the relationship between vitamin D and Th2 axis-related cytokines in neuromyelitis optica spectrum disorder. J Clin Neurosci. 2019;61:22–27. doi:10.1016/j.jocn.2018.11.024
23. Shan Y, Tan S, Zhang L, et al. Serum 25-hydroxyvitamin D3 is associated with disease status in patients with neuromyelitis optica spectrum disorder in south China. J Neuroimmunol. 2016;299:118–123. doi:10.1016/j.jneuroim.2016.09.006
24. Kusumadewi W, Imran D, Witjaksono F, et al. Low vitamin D-25(OH) level in Indonesian multiple sclerosis and neuromyelitis optic patients. Mult Scler Relat Disord. 2018;25:329–333. doi:10.1016/j.msard.2018.08.030
25. Brett N, Agellon S, Vanstone C, et al. Vitamin D status positively associates with interleukin-6 and tumor necrosis factor alpha in healthy young children (40.8). FASEB J. 2014;28:40–48. doi:10.1096/fasebj.28.1_supplement.40.8
26. Niino M, Sato S, Fukazawa T, et al. Decreased serum vitamin D levels in Japanese patients with multiple sclerosis. J Neuroimmunol. 2015;279:40–45. doi:10.1016/j.jneuroim.2015.01.007
27. Kamen DL, Cooper GS, Bouali H, et al. Vitamin D deficiency in systemic lupus erythematosus. Autoimmun Rev. 2006;5(2):114–117. doi:10.1016/j.autrev.2005.05.009
28. Yoon SY, Bae SH, Shin YJ, et al. Low serum 25-hydroxyvitamin D levels are associated with dry eye syndrome. PLoS One. 2016;11(1):e0147847. doi:10.1371/journal.pone.0147847
29. Dikci S, Akatlı AN, Yıldırım T. Conjunctival impression cytology and tear-film changes in cases with vitamin D deficiency. Int Ophthalmol. 2020;40(7):1687–1694. doi:10.1007/s10792-020-01336-1
30. Lee V, Rekhi E, Hoh Kam J, et al. Vitamin D rejuvenates aging eyes by reducing inflammation, clearing amyloid beta and improving visual function. Neurobiol Aging. 2012;33(10):2382–2389. doi:10.1016/j.neurobiolaging.2011.12.002
31. Souberbielle JC, Body JJ, Lappe JM, et al. Vitamin D and musculoskeletal health, cardiovascular disease, autoimmunity and cancer: recommendations for clinical practice. Autoimmun Rev. 2010;9(11):709–715. doi:10.1016/j.autrev.2010.06.009
32. Fragoso YD, Adoni T, Alves-Leon SV, et al. No correlation was observed between vitamin D levels and disability of patients with multiple sclerosis between latitudes 18° and 30° South. Arq Neuropsiquiatr. 2017;75(1):3–8. doi:10.1590/0004-282x20160173
33. López-Robles C, Rios-Fernández R, Callejas-Rubio JL, et al. Vitamin D deficiency in a cohort of patients with systemic lupus erythematous from the South of Spain. Lupus. 2011;20(3):330–331. doi:10.1177/0961203310378670
34. Craig SM, Yu F, Curtis JR, et al. Vitamin D status and its associations with disease activity and severity in African Americans with recent-onset rheumatoid arthritis. J Rheumatol. 2010;37(2):275–281. doi:10.3899/jrheum.090705
35. Jeon DH, Yeom H, Yang J, et al. Are serum vitamin D levels associated with dry eye disease? Results from the study group for environmental eye disease. J Prev Med Public Health. 2017;50(6):369–376. doi:10.3961/jpmph.17.089
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Different Immune Response Between Onset and Remission of AQP4 Antibody-Positive Optic Neuritis Based on RNA Sequencing of Whole Blood
Shi R, Luo Y, Chen Y, Chen X, Li S, Chen Z, Wang K, Zou W
Journal of Inflammation Research 2025, 18:10283-10293
Published Date: 30 July 2025