Back to Journals » Cancer Management and Research » Volume 13
Serum Untargeted UHPLC-HRMS-Based Lipidomics to Discover the Potential Biomarker of Colorectal Advanced Adenoma
Authors Zhu Y ![]() , Wang L, Nong Y, Liang Y, Huang Z, Zhu P, Zhang Q
, Wang L, Nong Y, Liang Y, Huang Z, Zhu P, Zhang Q ![]()
Received 27 August 2021
Accepted for publication 29 October 2021
Published 26 November 2021 Volume 2021:13 Pages 8865—8878
DOI https://doi.org/10.2147/CMAR.S336322
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Seema Singh
Yifan Zhu,1,* Lisheng Wang,1,* Yanying Nong,2 Yunxiao Liang,3 Zongsheng Huang,3 Pingchuan Zhu,4 Qisong Zhang1
1Medical College of Guangxi University, Guangxi University, Nanning, Guangxi, 530004, People’s Republic of China; 2Department of Gastroenterology, Ruikang Hospital Affiliated to Guangxi University of Chinese Medicine, Nanning, Guangxi, 530011, People’s Republic of China; 3Department of Gastroenterology, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, People’s Republic of China; 4State Key Laboratory for Conservation and Utilization of Subtropical Agro-Bioresources, Guangxi University, Nanning, Guangxi, 530004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qisong Zhang
Medical College of Guangxi University, Guangxi University, No. 100, East Daxue Road, Nanning, Guangxi, 530004, People’s Republic of China
Tel +86 0771-3387105
Email [email protected]
Background: As a key precancerous lesion, colorectal advanced adenoma (CAA) is closely related to the occurrence and development of colorectal cancer (CRC). Effective identification of CAA-related biomarkers can prevent CRC morbidity and mortality. Lipids, as an important endogenous substance, have been proved to be involved in the occurrence and development of CRC. Lipidomics is an advanced technique that studies lipid metabolism and biomarkers of diseases. However, there are no lipidomics studies based on large serum samples to explore diagnostic biomarkers for CAA.
Methods: An integrated serum lipid profile from 50 normal (NR) and 46 CAA subjects was performed using ultra-high performance liquid chromatography tandem high-resolution mass spectrometry (UHPLC-HRMS). Lipidomic data were acquired for negative and positive ionization modes, respectively. Differential lipids were selected by univariate and multivariate statistics analyses. A receiver operator characteristic curve (ROC) analysis was conducted to evaluate the diagnostic performance of differential lipids.
Results: A total of 53 differential lipids were obtained by combining univariate and multivariate statistical analyses (P < 0.05 and VIP > 1). In addition, 12 differential lipids showed good diagnostic performance (AUC > 0.90) for the discrimination of NR and CAA by receiver operating characteristic curve (ROC) analysis. Of them, the performance of PC 44:5 and PC 35:6e presented the outstanding performance (AUC = 1.00, (95% CI, 1.00– 1.00)). Moreover, triglyceride (TAG) had the highest proportion (37.74%) as the major dysregulated lipids in the CAA.
Conclusion: This is the first study that profiled serum lipidomics and explored lipid biomarkers with good diagnostic ability of CAA to contribute to the early prevention of CRC. Twelve differential lipids that effectively discriminate between NR and CAA serve as the potential diagnostic markers of CAA. An obvious perturbation of TAG metabolism could be involved in the CAA formation.
Keywords: colorectal advanced adenoma, biomarker, serum lipidomics, UHPLC-HRMS, colorectal cancer
Introduction
Colorectal cancer (CRC), a common digestive system malignancy globally, is one of the top three causes of cancer-related mortality in both men and women, according to the latest cancer statistics.1 Colorectal carcinogenesis has generally been acknowledged as an adenoma-carcinoma sequence. That is, CRC develops mainly from colorectal adenoma (CA), which is precancerous lesions of the colorectum and take 10–15 years to develop CRC.2–4 Study showed that the removal of CA can prevent cancer and reduce the mortality rate of CRC by as much as 50%.5 Colorectal advanced adenoma (CAA) refers to any CA ≥ 1 cm in diameter or villous or serrated adenoma of high-risk pathological type, and/or high-grade intraepithelial tumor.6 At a median follow-up, researchers found that participants with CAA were more likely to develop CRC than participants without CAA (rate, 2.7 [95% CI, 1.9–3.7]; P < 0.001).7 Therefore, screening and resection of CAA should be an effective way to reduce CRC mortality. However, the diagnostic strategy for CAA is relatively scarce at present in clinical.
Colonoscopy, as the “gold standard” in clinical practice, has high accuracy and can effectively detect various histological subtypes of colorectal polyps, including CAA and CA.8 However, patients’ poor compliance with its invasive examination and high technical requirement resulted in difficulties in early diagnosis limiting their mass screening.9 In addition, the diagnostic indicators for CRC include the traditional diagnostic means (fecal immunochemistry test (FIT) and abdominal computed tomography scan) and the new screening means (fecal DNA test), which have low sensitivity or specificity for CAA. The sensitivity of FIT-DNA test to detect advanced precancerous lesions (advanced adenomas and sessile serrated polyps measuring ≥1 cm) was low with 42% (95% CI, 39%–46%).10−12 In addition to clinical diagnostic methods, several scholars have made preliminary explorations of diagnostic markers for CAA. Respiratory volatile organic compounds,13 serum autoantibodies,14 serum M2-pyruvate kinase,15 fecal miRNA-135b,16 plasma matrix metalloproteinase,17 serum circulating tumor DNA (ctDNA),18,19 and miRNA-21/59220,21 are still lack of high sensitivity or specificity for the CAA diagnosis. Furthermore, although the levels of nine amino acids in CAA tissue are significantly different from those in normal intestinal mucosa, reliance on colonoscopy and invasive tissue samples is not suitable for its early screening.22 Plasma macrophage-suppressive cytokine-1 and urinary prostaglandin E2 metabolites have also been reported as potential markers of CAA, but their diagnostic efficacy is still unknown.23,24 Accordingly, there is an urgent need for a minimally invasive diagnostic strategy with high performance (sensitivity and specificity) to improve the CAA diagnosis and screening.
As endogenous mediators, lipids involve in many physiological functions, such as cell signal transduction, apoptosis, proliferation, and membrane transport.25 Dysregulation of lipid homeostasis has become an established hallmark of numerous cancers including CRC.26,27 With the exception of CRC, dysregulation of lipid metabolism has also been confirmed in CAA patients. Fecal metabolomics studies of CAA patients have found significantly altered levels of some bioactive lipids (including polyunsaturated fatty acids, secoiric acid, glycerolipids, glycerophospholipids, sterolipids, and sphingolipids) in CAA patients relative to controls.28,29 Furthermore, some researchers have reported a close link between levels of blood lipid and risk of CA development. For instance, higher serum triglyceride levels were significantly associated with an increased prevalence of CAA, while there was an inverse association between levels of plasma HDL cholesterol and hazard of CA formation.30,31 With the increasing importance of lipid metabolism and functions, lipidomics, a important subdiscipline of metabolomics, has become a hot topic in scientific research of cancers currently. It not only provides insight into the physiological functions of lipid molecules but also offers a novel approach to the discovery of diagnostic biomarkers for diseases.32 Ultra-high-performance liquid chromatography-high resolution mass spectrometry (UHPLC-HRMS) is an attractive analytical platform and is preferred for lipid analysis due to its high sensitivity, throughput, and resolution.33 Presently, few lipidomic studies involved in CRC progression mainly focus on the stage of CRC by LC-MS. In the plasma, triacylglycerols (TAGs), plasminogen (PlsEtns), and fatty acids (FAs) metabolism display obvious metabolic disturbances in CRC patients.4,33 Moreover, lysophatidycholines (LPCs) and phosphatidylcholines (PCs) in tissues are reported as the biomarkers most closely associated with the development of CRC.34 However, no lipidomic studies with large-scale serum samples have been performed based on UHPLC-HRMS technique to explore the biomarkers for CAA diagnosis.
Therefore, we conducted a lipidomic study with large-scale serum samples of NR and CAA based on UHPLC-HRMS technique, aiming to disclose global serum lipid profiles of CAA and to explore lipid biomarkers with good diagnostic performance for CAA conducting to the early prevention of CRC.
Materials and Methods
Chemicals
Methanol, dichloromethane, isopropanol, and acetonitrile were of HPLC grade from Merck & Co. (Billerica, MA, USA). Ultrapure water was prepared by a Millipore Milli-Q system (Billerica, MA, USA).
Subjects and Serum Sample Collection
The protocol of this study was approved by the Ethics Committee of Guangxi Zhuang Autonomous Region People’s Hospital (No. KY-DZX-202008), including collection of the details about serum samples and the subjects, and the written consent of all subjects before enrolling them in the study. A total of 50 NR subjects and 46 CAA patients were enrolled in this study, and the main clinical details are provided in Table 1. Inclusion criteria for NR subjects were as follows: (1) No CRC or other malignant tumor; (2) No family history of CRC; (3) No metabolic diseases, such as hypertension, hyperlipidemia and diabetes; (4) Did not take medicine that affects lipid metabolism before one month; (5) without any intestinal neoplasm by colonoscopy exam. The inclusion criteria of CAA subjects were as follows: (1) CA ≥ 1 cm in diameter with colonoscopy and pathological diagnosis; (2) Histological types with villous or serrated adenomas, and/or high-grade intraepithelial neoplasia; (3) No history of other metabolic diseases or malignancy. After 8-hour fasting before surgery, the serum samples were collected in a coagulation tube and centrifuged at 5000 rpm/min, 4°C for 10 min. Finally, the supernatants were transferred into a new Eppendorf tube and stored at –80°C until further use.
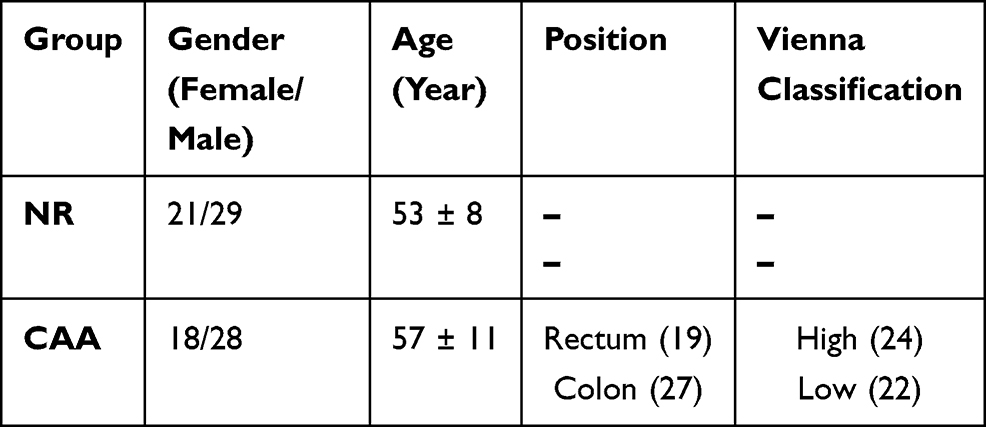 |
Table 1 Information of Clinical Characteristics for Study Subjects |
Sample Preparation
Serum sample: 500 μL of a mixture of pre-cooling dichloromethane-methanol (3:1, v/v) solution was added to 50 μL serum. After being vortexed for 5 min and placed in an ice bath for 10 min, the solution was centrifuged at 13,000 rpm/min at 4°C for 10 min. 300 μL lower dichloromethane solution was dried in vacuum at room temperature. The dried samples were redissolved with 600 μL acetonitrile-isopropanol (1:1 v/v) solution, then vortexed for 2 min and ultrasonicated in ice bath for 5 min. After mixing for 1 min, the vials were centrifuged at 13,000 rpm/min at 4°C for 15 min, and the supernatants were collected for lipidomics analysis. 5 μL of each sample was mixed together to serve as quality control (QC) samples. Before formal sample injection, the repeatability and stability of the analytical system and method was verified by balancing the analytical system with 6 blank samples and 6 QC samples.
UHPLC-HRMS Analysis
Aliquots of 5 µL of serum were subjected to a Dionex Ultimate 3000 liquid chromatography system (Sunnyvale, CA, USA) (SN: 7254012) equipped with a Waters Acquity UPLC HSS T3 column (1.8 μm, 2.1 × 100 mm; Milford, MA, USA) for the separation analysis. The mobile phase was represented by a gradient of eluent A (water: acetonitrile = 4:6, v/v, containing 0.1% formic acid and 10 mM ammonium formate) and eluent B (isopropanol: acetonitrile = 9:1, v/v, containing 0.1% formic acid and 10 mM ammonium formate) with flow rate of 0.3 mL/min. The gradient conditions were set as follows: 0.0–4.0 min, 30% to 60% B; 4.0–9.0 min, 60% to 100% B; 9.0–15.0 min,100% B; 15.0–18.0 min,100% B to 30% B. The column temperature was 50°C.
The mass spectrometry analysis was performed on a Thermo Fisher Q Exactive Orbitrap mass spectrometry system (Waltham, MA, USA) (SN: SN02386L, operating in both ESI+ and ESI- mode. The mass range was set between m/z 100–1200. The key detected parameters were as follows: spray voltage, 3.5 kV; sheath gas flow rate, 50 psi; auxiliary gas flow rate, 13 arb; capillary temperature, 320°C; auxiliary gas heater temperature, 420°C; scan modes, full MS (resolution of 70,000) combined ddMS2 (resolution of 17,500) scan with stepped collision energy (10, 20, and 40 eV). All data were acquired using the Thermo Scientific Xcalibur 3.1 software (Waltham, MA, USA).
Data Processing and Statistical Analyses
The original MS data files of both two sets of samples were imported into the Compound Discoverer TM Software Version 3.1 (Thermo Scientific, Fremont, CA, USA). Three-dimensional data (including RT, m/z, and peak intensity of all lipid features) were extracted to identify lipid metabolites and perform differential analysis (Student’ t-test or Mann–Whitney U-Test). A list of potential lipid species were generated according to Thermo mzCloud and mzVault with lipidomics database. The main parameters were as follows: minimum peak intensity, 500,000, Mass error, 5 ppm, RT tolerance, 0.2 min, Peak intensity tolerance, 30%, S/N, 3.
The data were imported into SIMCA-P version 14.1 (Umetrics, UMEA, Sweden) to conduct multivariate statistical analysis including the principal component analysis (PCA) and orthogonal partial least-squares discriminant analysis (OPLS-DA). The UV- or Pareto-scaling was applied to normalize the intensities of lipid features prior to analytical model fitting. The quality of OPLS-DA model was evaluated by values of explanatory parameter, R2 and predictive parameter, Q2. To avoid overfitting of analytical mode, 200 permutations test was carried out on the model. The QC normalization was applied to uncover differential lipids between CAA and NR. Criteria of VIP > 1 and P < 0.05 were further used to select the differential lipids between the two groups. Finally, MetaboAnalyst 5.0 was used to analyze the receiver operating characteristic curve (ROC) of the differential lipids to explore the potential biomarkers to differentiate CAA from NR.
Results
The Differential Lipid Profiles Between NR and CAA
Direct observation of serum lipid profiles by TIC chromatography revealed the obvious differences between NR and CAA groups in both ESI modes (Figure 1A-D). The tight clustering of QC samples in the PCA scoring plot in both ESI modes demonstrated that the analytical system met the requirement of lipidomic analysis (Figure 2A and B). In both ESI modes, the individual differences in lipid profiles were relatively small in the CAA group compared to the NR group, due to the better aggregation manifested by CAA patients (Figure 2A and B). In addition, lipid profiles were well differentiated between NR and CAA samples, which implies that there were some evident differences in serum lipids between the two groups (Figure 2A and B). In particular, the degree of separation was more pronounced in the ESI+ model relative to ESI- mode. To more clearly describe the differences in lipid profiles between NR and CAA, an OPLS-DA model was constructed using all detected lipid features. The two groups were clearly separated at ESI+ mode (R2X [cum] = 0.379, R2Y [cum] = 0.981, Q2 [cum] = 0.976) and ESI- mode (R2X [cum] = 0.522, R2Y [cum] = 0.951, Q2 [cum] = 0.870), which indicated obvious difference of lipid features. Additionally, to guard against overfitting of the OPLS-DA model, 200 permutations test with R2Y (0.415 and 0.696) and Q2 (−0.270 and −0.366) values was provided (Figure 2E and F) in ESI+ and ESI- modes, respectively, showing that the analytical model has high validity and predictability. Based on OPLS-DA model, VIP > 1 was used to select 7154 and 621 lipid features responsible for group differentiation under both modes, respectively. Together, a total of 53 differential lipids with VIP > 1 and P < 0.05 were selected as potential lipid markers, including 44 in ESI+ mode and 9 in ESI- mode (Table 2). These lipid species mainly consisted of FA (9.43%), SL (7.55%), DAG (13.21%), LPC (7.55%), PC (13.21%), TAG (37.74%), PE (7.55%), PG (1.89%), and PI (1.89%) (Figure 3). Hence, the percentage of TAG as a major component was more than 37%, suggesting that dysregulation of TAG metabolism may be an important factor in the development of NR to CAA. To further investigate the distribution and trend of differential lipids in individuals, we then performed a clustering heatmap analysis with 53 differential lipids between the two groups. Through sample clustering, we observed that both NR and CAA groups showed good clustering, indicating that the intra-group difference and inter-group proximity of these lipid profiles were relatively pronounced. For example, compared with NR, palmitic acid, docosanamide, and PC 35:6e showed a significantly up-regulated in CAA, while TAG 57:1 displayed an obviously up-regulated (Figure 4 and Table 2).
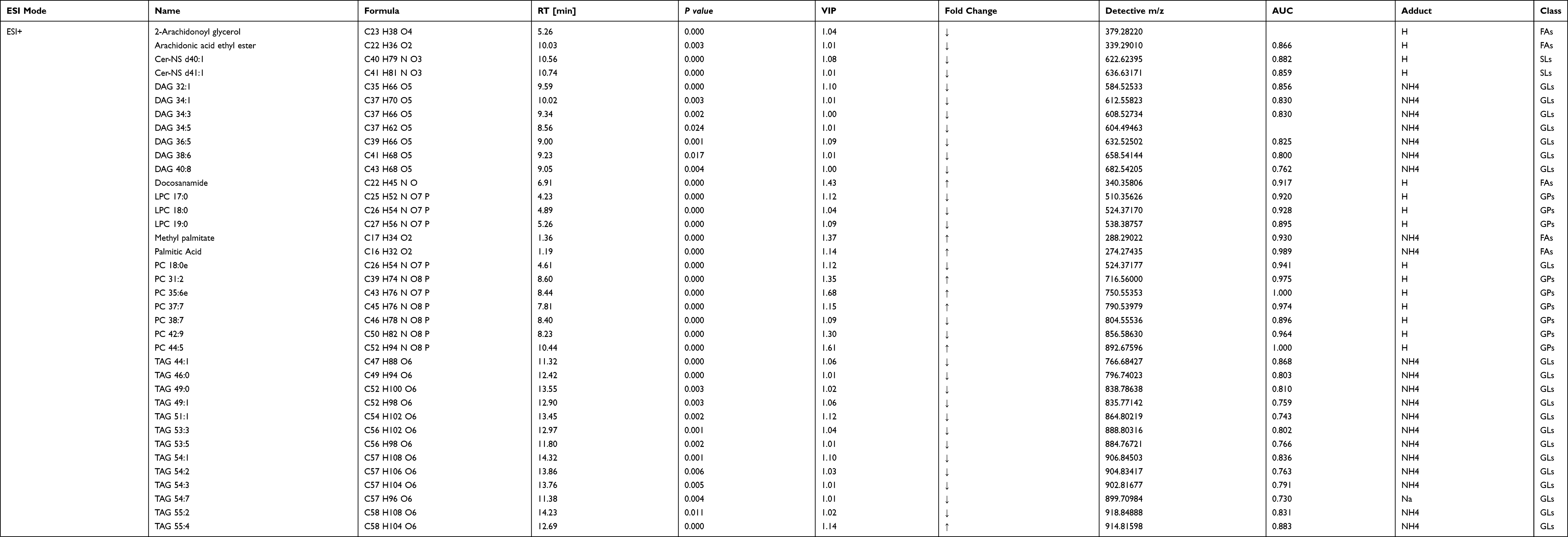 |
Table 2 53 Differential Lipids Between NR and CAA Groups in Both ESI Modes |
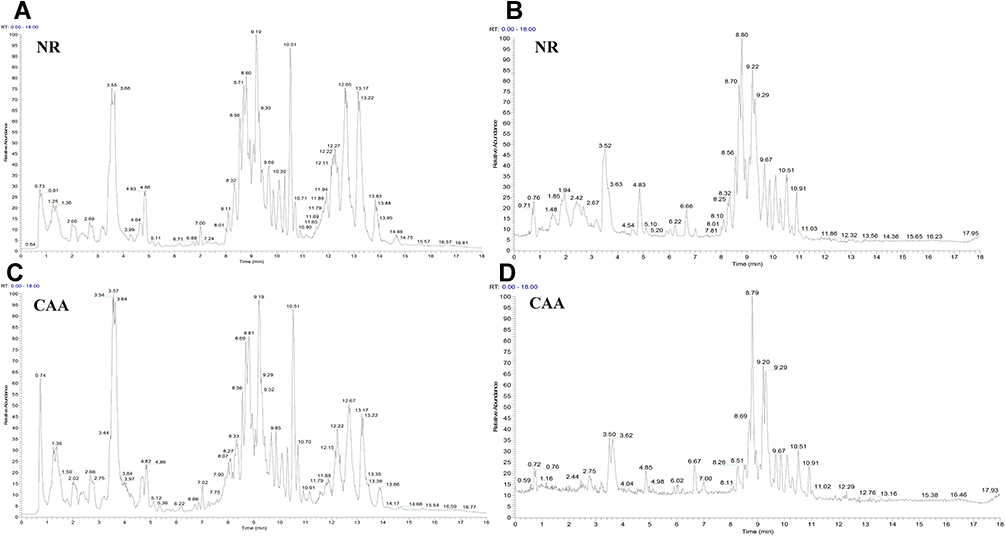 |
Figure 1 The TIC chromatography of normal (NR) and colorectal advanced adenoma (CAA) groups in both ESI modes. (A and B) TIC chromatography of NR in ESI+ and ESI- modes, respectively; (C and D) TIC chromatography of CAA in ESI+ and ESI- modes, respectively. |
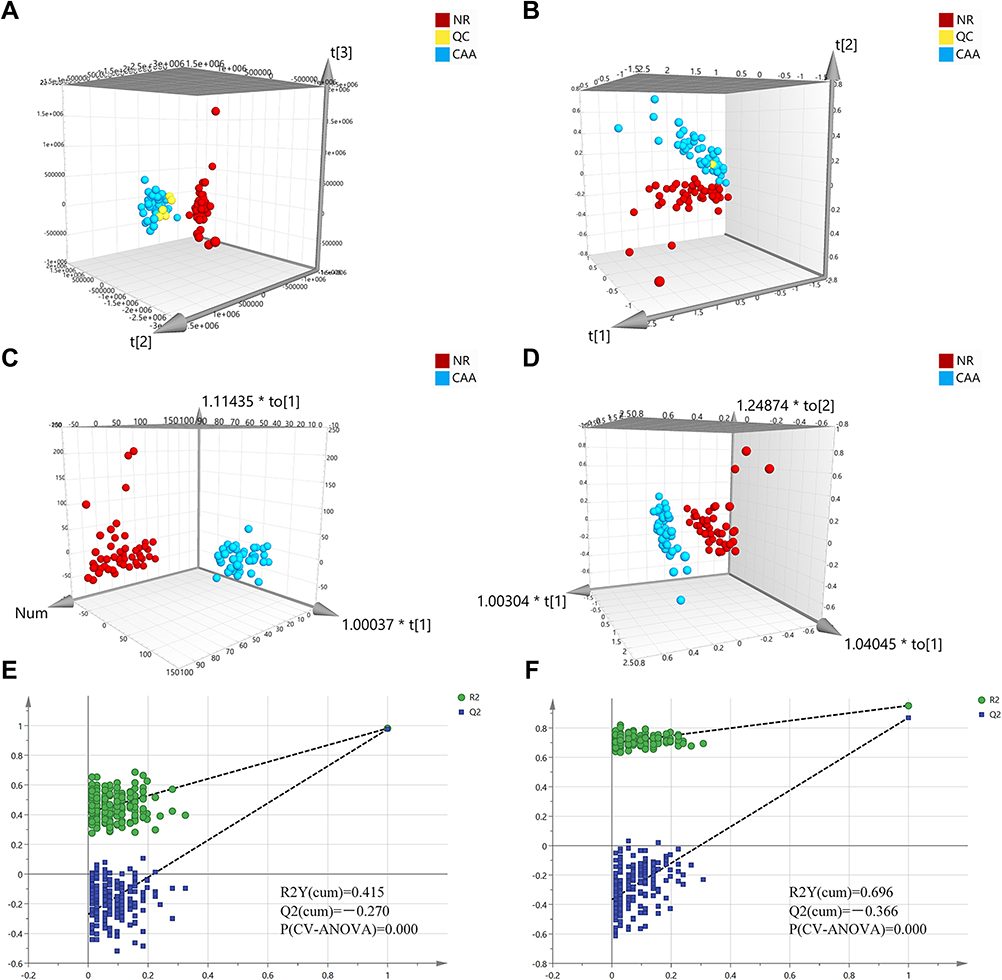 |
Figure 2 Multivariate statistical analysis for lipid profile between the NR and CAA groups. (A and B) 3D PCA analysis of the two groups in ESI+ and ESI- modes, respectively; (C and D) 3D OPLS-DA analysis of the two groups in ESI+ and ESI- modes, respectively. R2X[cum] = 0.379 and 0.522, R2Y[cum] = 0.981 and 0.951, Q2[cum] = 0.976 and 0.870; (E and F) Permutation test (200 permutations) corresponding to OPLS-DA model in ESI+ and ESI- modes, respectively. |
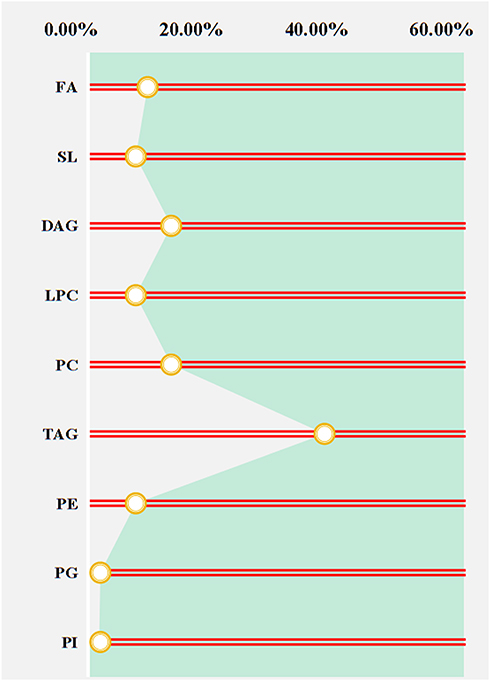 |
Figure 3 The proportion of differential lipids between two groups. Abbreviations: FA, fatty acid; SL, sphingolipid; DAG, diacylglycerol; LPC, lysophosphatidylcholine, PC, phosphatidylcholine; TAG, triacylglycerol; PE, phosphatidylethanolamine; PG, phosphatidylglycerol; PI, phosphatidylinositol. |
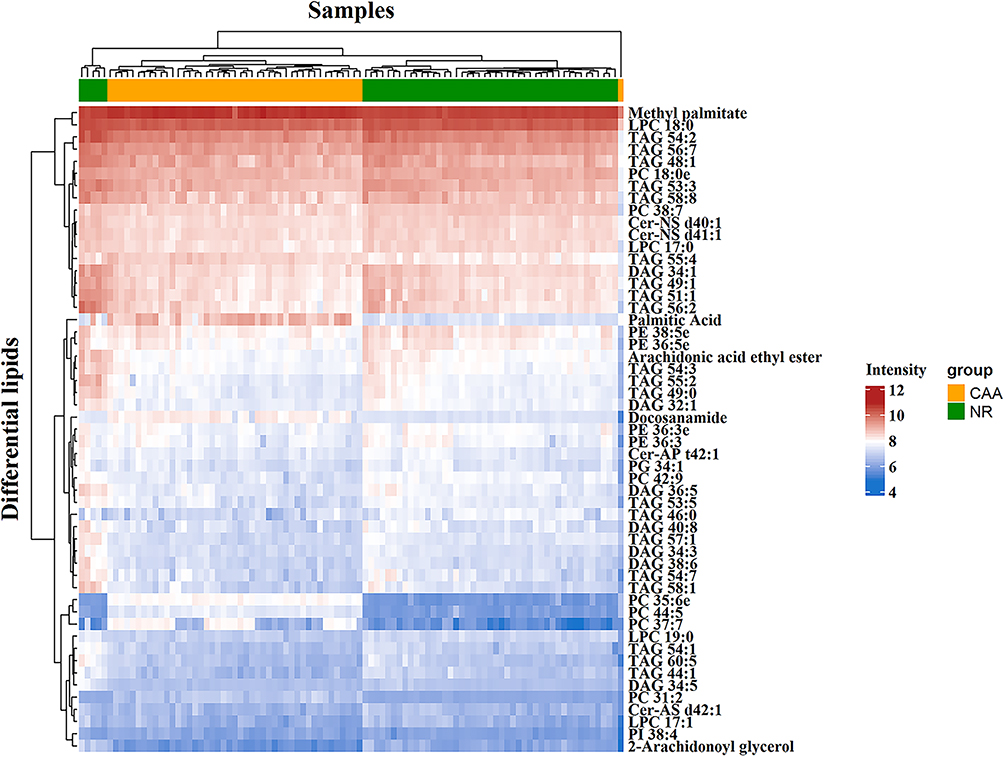 |
Figure 4 Heat map analysis of 53 differential lipids between NR and CAA groups. The color bars represent the log10 value of the ratio for each lipid species and only statistically significant changes are shown (VIP > 1, P < 0.05). |
Evaluation of Diagnostic Performance of Serum Differential Lipids Between NR and CAA Groups
After selecting the lipids with notable difference between groups, potential lipid biomarkers of CAA were further defined based on the diagnostic ability of these 53 differential lipids. Prior to ROC analysis, samples and differential lipids were normalized using sum and auto scaling methods to reduce the effects of individual differences and systematic errors (Figures 5A-D). After that, we eventually 12 differential lipids were identified with good diagnostic performance (AUC > 0.900) (Figure 6) and their identification results based on MS fragments and retention time matched with Thermo Lipidblast and mzCloud databases are presented in Figure 7. Among them, PC 35:6e and PC 44:5 had the highest AUC values (AUC = 1.000, (95% CI, 1–1)), indicating excellent diagnostic performance for CAA, while docosanamide had the relatively low AUC values (AUC = 0.919, (95% CI, 0.847–0.981)) (Figures 6A and L).
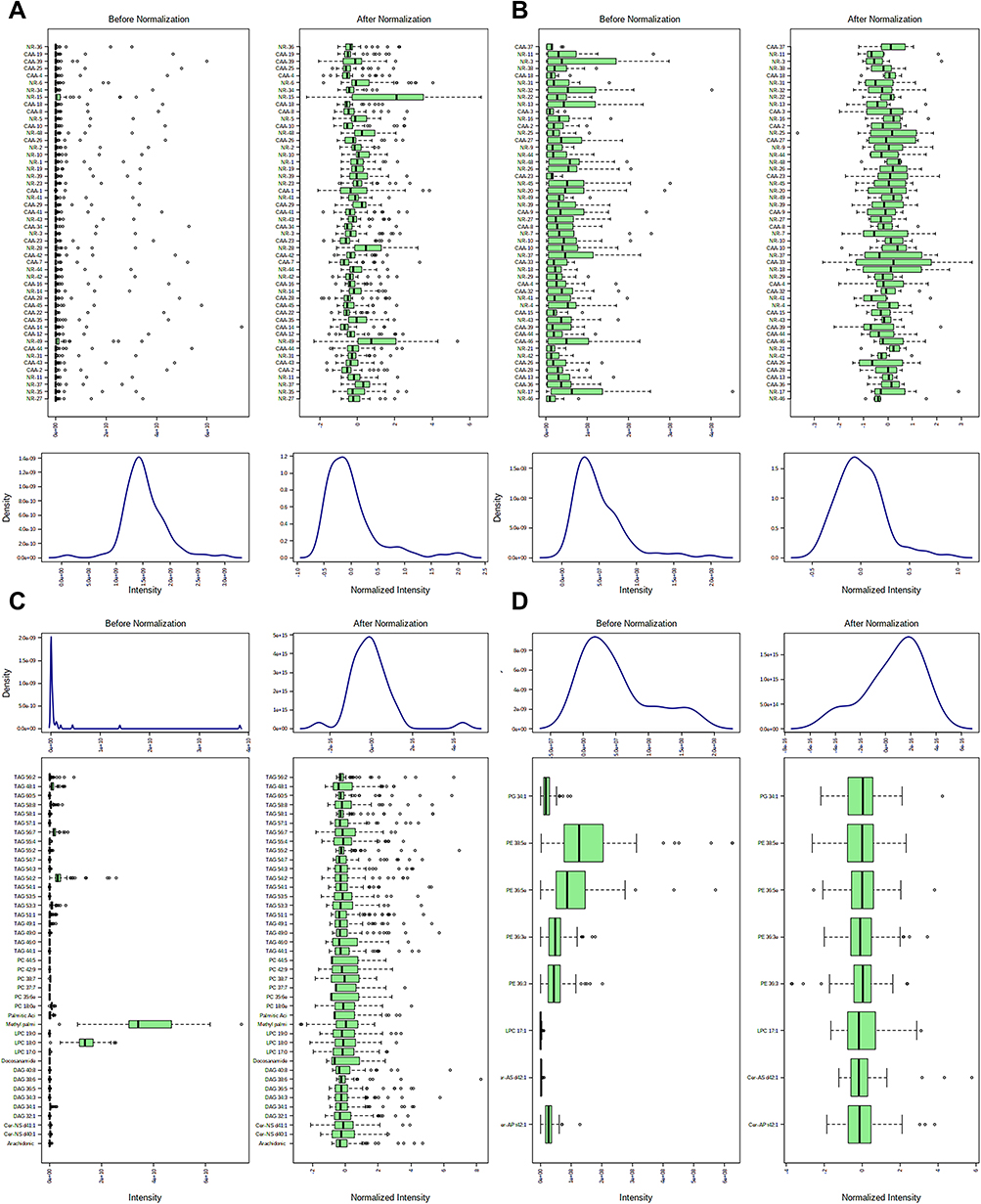 |
Figure 5 Normalization of the differential lipids between the NR and CAA groups. (A and B) Sample normalization of two groups in ESI+ and ESI- modes, respectively; (C and D) Lipids normalization of two groups in ESI+ and ESI- modes, respectively. |
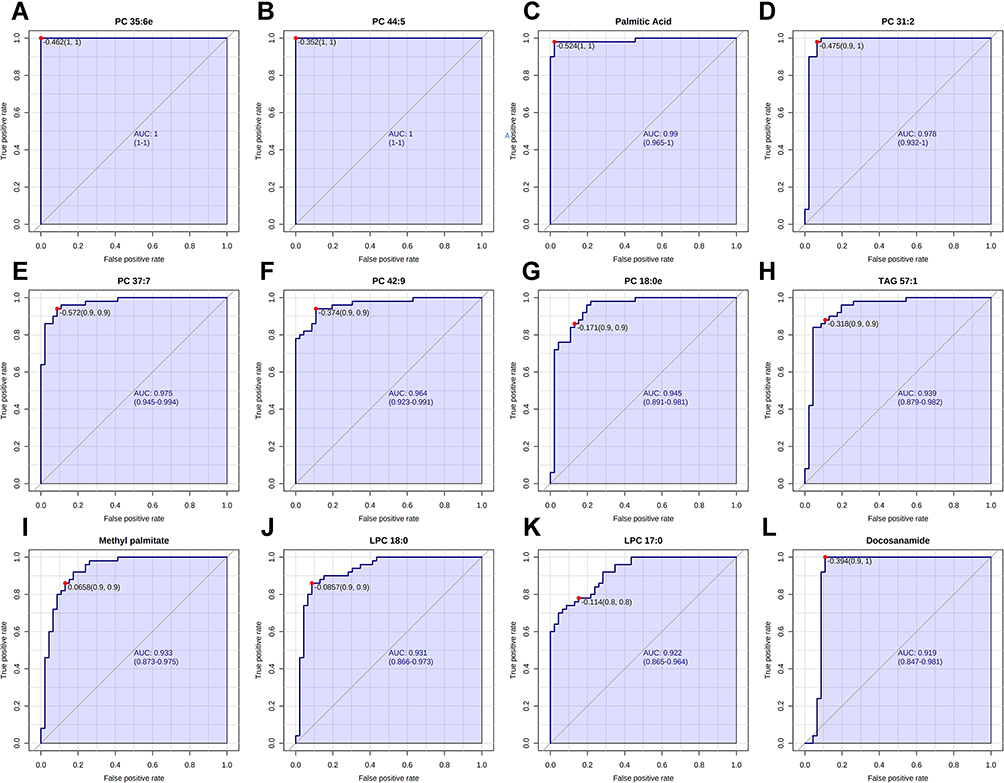 |
Figure 6 Performance evaluation of differential lipids between NR and CAA groups. (A) PC 35:6e; (B) PC 44:5; (C) Palmitic acid; (D) PC 31:2; (E) PC 37:7; (F) PC 42:9; (G) PC 18:0e; (H) TAG 57:1; (I) Methyl palmitate; (J) LPC 18:0; (K) LPC 17:0; (L) Docosanamide. |
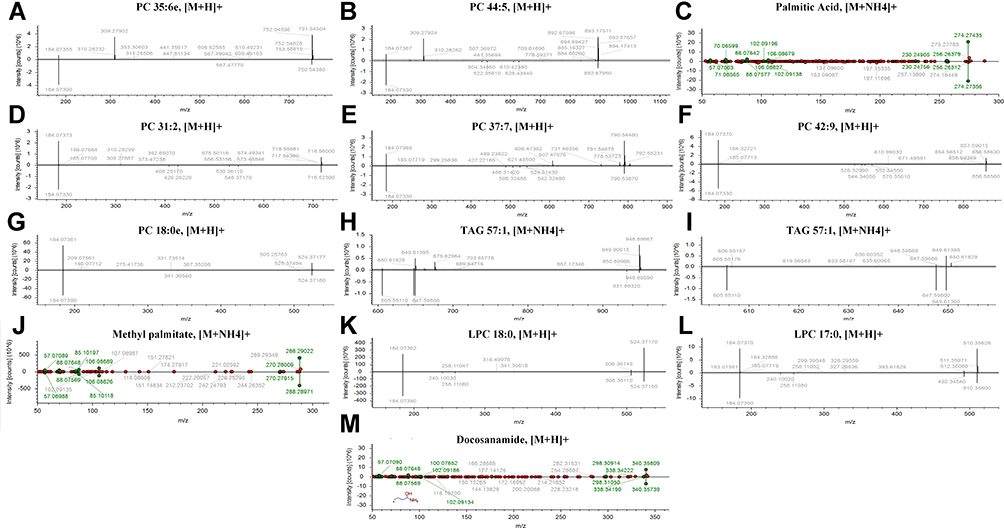 |
Figure 7 The identification of 12 differential lipids with good diagnosis between NR and CAA groups. (A) PC 35:6e; (B) PC 44:5; (C) Palmitic acid; (D) PC 31:2; (E) PC 37:7; (F) PC 42:9; (G) PC 18:0e; (H) TAG 57:1; (I) TAG 57:1; (J) Methyl palmitate; (K) LPC 18:0; (L) LPC 17:0; (M) Docosanamide. |
Based on the above ROC analysis results, we further studied the variation trend of these 12 lipids with good distinguishing performance between the two groups. The results suggested that the levels of docosanamide, methyl palmitate, palmitic acid, PC 31:2, PC 35:6e, PC 37:7, and PC 44:5 significantly increased, while LPC 17:0, LPC 18:0, PC 18:0e, PC 42:9, and TAG 57:1 were dramatically down-regulated in the CAA group (Figure 8). Of them, palmitic acid, PC 35:6e, PC 37:7, and PC 44:5 had the most significant change trend, which were consistent with the previous heat map results (Figure 4).
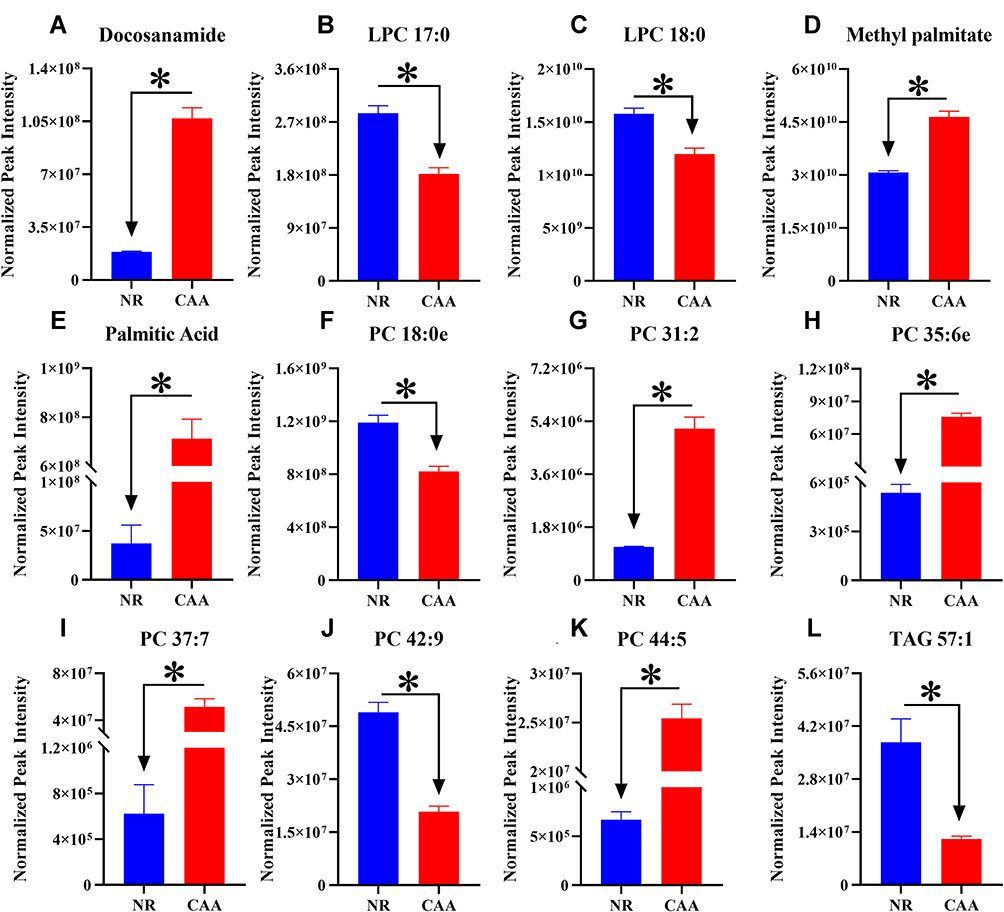 |
Figure 8 The trend of differential lipids in NR and CAA groups. (A) Docosanamide; (B) LPC 17:0; (C) LPC 18:0; (D) Methyl palmitate; (E) Palmitic Acid; (F) PC 18:0e; (G) PC 31:2; (H) PC 35:6e; (I) PC 37:7; (J) PC 42:9; (K) PC 44:5; (L) TAG 57:1. *Means the significant difference of levels of differential lipid between NR and CAA. The levels of differential lipids were displayed with mean ± SEM. |
Exploration of the Underlying Mechanism Associated with Formation of CAA
As shown in Table 2, we totally identified 53 differential lipids, which mainly include 5FAs, 4SLs, 7DAGs, 4LPCs, 7PCs, 20TAGs, 4PEs, 1PG and 1PI, of which 1/20 of TAG, 4/7 PC, 3/5 FA and 1 PI were significantly up-regulated, and the rest of them were all remarkably down-regulated in CAA group. These differential lipids are mainly involved in the metabolism of glycerophospholipids (GPs), fatty acids (FAs), and glycerides (GLs). Of them, the levels of 12 potential diagnostic lipid markers’ ability also showed a similar change trend with those of differential lipids between groups. Compared with NR group, FA (3/3) and PC (4/6) in the CAA group showed a significant up-regulation trend, while LPC (2/2) and TAG (1/1) all showed a significant down-regulation trend in CAA group. Therefore, TAG, as a lipid species that accounts for up to 37.74% in differential lipids, and its metabolic disturbance is considered to be the main influencing factor of CAA formation.
Discussion
In this study, we explored serum lipidomics with UHPLC-HRMS as a prospective approach to identify serum lipid biomarkers in CAA. Using this method, we detected a total of 53 differential lipids between NR and CAA and most of them belonged to TAG, indicating the disequilibrium of TAG metabolism was involved in CAA pathogenesis. Among them, 12 differential lipids with good diagnostic ability (AUC > 0.900) served as potential serum biomarkers of CAA.
GPs, characterized by phospholipids and their structural diversity, suggest their involvement in many physiological and pathological processes, including the progression of CRC.35 PC, a major component of GPs, was demonstrated to have a positive correlation between its metabolic disorder and CA risk.36 In addition, serum levels of PC 34:1 and PC 36:4 were disturbed in patients with benign colorectal disease compared to controls.37 Moreover, phospholipids associated with choline can be considered as good biomarkers of CRC.38,39 Similarly, in the current study, serum PC levels were also dysregulated in the CAA group and showed good diagnostic properties (AUC > 0.900) to distinguish NR from CAA. As a metabolite of PC, LPC is the most studied biomarker of CRC. It was reported that LPC (18:1) and LPC (18:2) were found to be significantly lower in the plasma of CRC patients than in healthy groups (P < 0.001).38 Another study based on plasma lipidomics also confirmed that LPC 18:2 and LPC 18:3 had good diagnostic performance (AUC > 0.900) as a potential biomarker for CRC.34 In addition, the increase n LPC in CRC tissue showed the possibility as potential biomarkers in CRC.40 Analogously, our study firstly found that LPC also showed favorable diagnostic performance for CAA, as shown by LPC 17:0 (AUC = 0.931, (95% CI, 0.866–0.973)) and LPC 18:0 (AUC = 0.922, (95% CI, 0.865–0.934)) (Figure 6).
FAs are essential components of biological membranes and are key substrates for energy metabolism. It has been found that many cancer cells contain higher levels of FAs than normal cells because cancer cells require more lipids for energy synthesis and more membranes for exuberant metabolism.41 Therefore, they are also key targets for tumor-preventive effects. Our results show that palmitic acid, methyl palmitate, and docosanamide showed good diagnostic performance (AUC > 0.900) for distinguishing NR from CAA. Likewise, palmitic acid (OR, 3.75; P = 0.04) was found to be more likely to present adenomas per unit increase relative to those without colonic polyps, and its ability to discriminate between CRC patients and controls was excellent (specificity and sensitivity >80%).42,43 In addition, a panel of biomarkers including palmitic acid was used to discriminate between early CRC patients and healthy controls achieved good diagnostic accuracy (sensitivity of 0.981 and specificity of 1.000) with an AUC value of 0.991, superior to carcinoembryonic antigen.44
As a class of glycerides, disturbances in serum or plasma TAGs levels have a close association with an increased risk of CA.30,45,46 Among the 53 differential lipids, TAGs account for 37.74% in the total composition, and their metabolic imbalance may be involved in the formation of NR to CAA. Meanwhile, study revealed that serum TAGs may influence colorectal tumorigenesis through the mechanisms involving bile acid excretion, circulating hormones, and energy supply to tumor cells.47 Besides, in our result, TAG 57:1 presented good diagnostic performance for CAA (AUC = 0.939, (95% CI, 0.879–0.982)). Similarly, the combined use of increased low-density lipoprotein cholesterol (LDL-C) and TAG levels to differentiate patients with polyps was effective on account of sensitivity of 50.0% and specificity of 89.6% (AUC = 0.733).48
Conclusion
To our knowledge, this is the first study to profile the serum lipidomics and explore the diagnostic biomarkers in CAA patients based on the global lipidomics using the UHPLC-HRMS technique. The serum lipid profiles present obvious difference and 53 differential lipids were found between NR and CAA. Of them, TAGs were the main differential lipids, indicating that the abnormal metabolism of TAG may be involved in the CAA formation. In addition, a total of 12 differential lipids exhibit the outstanding performance (AUC > 0.900) to discriminate between NR and CAA, serving as the potential diagnostic markers for CAA. Undoubtedly, further validation is needed for the clinical application of our discovery due to limitations in clinical samples and lipid standards.
Abbreviations
CRC, colorectal cancer; CA, colorectal adenoma; CAA, colorectal advanced adenoma; FIT, fecal immunochemistry test; UHPLC-HRMS, ultra-high-performance liquid chromatography-high resolution mass spectrometry; QC, quality control; TAGs, triacylglycerols; DAG, diacylglycerol; PlsEtn, plasminogen; FAs, fatty acids; PCs, phosphatidycholines; LPCs, lysophatidycholines; GPs, glycerophospholipids; GLs, glycerides; SLs, sphingolipids; PG, phosphatidyl glycerol; PI, phosphatidylInositol; OPLS-DA, orthogonal partial least-squares discriminant analysis; PCA, principal component analysis; ROC, receiver operating characteristic curve, AUC, area under the curve; LDL-C, low-density lipoprotein cholesterol.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Guangxi Zhuang Autonomous Region People’s Hospital (No. KY-DZX-202008), including collection of the details about serum samples and the subjects. In addition, all participants gave written consent prior to enrollment in the study and were informed of the purpose of this study.
Acknowledgments
This experiment was assisted and supported by the State Key Laboratory of Conservation and Utilization of Subtropical Agricultural Biological Resources, Guangxi University.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by the Fund Project of Guangxi University (No. A3370051006), the Natural Science Foundation of Guangxi (No. 2017GXNSFAA198310), and Bama County Science and Technology Special Project (No. AE33700024).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249.
2. Miyamoto Y, Muguruma N, Fujimoto S, et al. Epidermal growth factor receptor-targeted molecular imaging of colorectal tumors: detection and treatment evaluation of tumors in animal models. Cancer Sci. 2019;110:1921–1930.
3. Randrian V, Evrard C, Tougeron D. Microsatellite instability in colorectal cancers: carcinogenesis, neo-antigens, immuno-resistance and emerging therapies. Cancers. 2021;13:3063.
4. Liu T, Peng F, Yu J, et al. LC-MS-based lipid profile in colorectal cancer patients: tAGs are the main disturbed lipid markers of colorectal cancer progression. Anal Bioanal Chem. 2019;411:5079–5088. doi:10.1007/s00216-019-01872-5
5. Aepli P, Criblez D, Baumeler S, et al. Endoscopic full thickness resection (EFTR) of colorectal neoplasms with the Full Thickness Resection Device (FTRD): clinical experience from two tertiary referral centers in Switzerland. United Eur Gastroenterol J. 2018;6:463–470. doi:10.1177/2050640617728001
6. Tehranian S, Klinge M, Saul M, et al. Prevalence of colorectal cancer and advanced adenoma in patients with acute diverticulitis: implications for follow-up colonoscopy. Gastrointest Endosc. 2020;91:634–640. doi:10.1016/j.gie.2019.08.044
7. Click B, Pinsky PF, Hickey T, et al. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021–2031. doi:10.1001/jama.2018.5809
8. Song EM, Park B, Ha CA, et al. Endoscopic diagnosis and treatment planning for colorectal polyps using a deep-learning model. Sci Rep. 2020;10:30. doi:10.1038/s41598-019-56697-0
9. Taylor DP, Cannon-Albright LA, Sweeney C, et al. Comparison of compliance for colorectal cancer screening and surveillance by colonoscopy based on risk. Genetics Med. 2011;13:737–743. doi:10.1097/GIM.0b013e3182180c71
10. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA. 2016;315:2564–2575. doi:10.1001/jama.2016.5989
11. Imperiale TF, Gruber RN, Stump TE, et al. Performance characteristics of fecal immunochemical tests for colorectal cancer and advanced adenomatous polyps: a systematic review and meta-analysis. Ann Intern Med. 2019;170:319–329. doi:10.7326/M18-2390
12. Mojtabanezhad Shariatpanahi A, Yassi M, Nouraie M, et al. The importance of stool DNA methylation in colorectal cancer diagnosis: a meta-analysis. PLoS One. 2018;13:e0200735. doi:10.1371/journal.pone.0200735
13. van Keulen KE, Jansen ME, Schrauwen RWM, et al. Volatile organic compounds in breath can serve as a non-invasive diagnostic biomarker for the detection of advanced adenomas and colorectal cancer. Aliment Pharmacol Ther. 2020;51:334–346. doi:10.1111/apt.15622
14. Wang H, Zhang B, Li X, et al. Identification and validation of novel serum autoantibody biomarkers for early detection of colorectal cancer and advanced adenoma. Front Oncol. 2020;10:1081. doi:10.3389/fonc.2020.01081
15. Meng W, Zhu HH, Xu ZF, et al. Serum M2-pyruvate kinase: a promising non-invasive biomarker for colorectal cancer mass screening. World J Gastrointest Oncol. 2012;4:145–151. doi:10.4251/wjgo.v4.i6.145
16. Wu CW, Ng SC, Dong Y, et al. Identification of microRNA-135b in stool as a potential noninvasive biomarker for colorectal cancer and adenoma. Clin Cancer Res. 2014;20:2994–3002. doi:10.1158/1078-0432.CCR-13-1750
17. Gimeno-García AZ, Triñanes J, Quintero E, et al. Plasma matrix metalloproteinase 9 as an early surrogate biomarker of advanced colorectal neoplasia. Gastroenterol Hepatol. 2016;39:433–441. doi:10.1016/j.gastrohep.2015.10.002
18. Suehiro Y, Hashimoto S, Higaki S, et al. Blood free-circulating DNA testing by highly sensitive methylation assay to diagnose colorectal neoplasias. Oncotarget. 2018;9:16974–16987. doi:10.18632/oncotarget.24768
19. Junca A, Tachon G, Evrard C, et al. Detection of Colorectal Cancer and Advanced Adenoma by Liquid Biopsy (Decalib Study): the ddPCR Challenge. Cancers. 2020;12:1482.
20. Toiyama Y, Takahashi M, Hur K, et al. Serum miR-21 as a diagnostic and prognostic biomarker in colorectal cancer. J Natl Cancer Inst. 2013;105:849–859. doi:10.1093/jnci/djt101
21. Pan Z, Miao L. Serum microRNA-592 serves as a novel potential biomarker for early diagnosis of colorectal cancer. Oncol Lett. 2020;20:1119–1126. doi:10.3892/ol.2020.11682
22. Gao P, Zhou C, Zhao L, et al. Tissue amino acid profile could be used to differentiate advanced adenoma from colorectal cancer. J Pharm Biomed Anal. 2016;118:349–355. doi:10.1016/j.jpba.2015.11.007
23. Song M, Mehta RS, Wu K, et al. Plasma inflammatory markers and risk of advanced colorectal adenoma in women. Cancer Prev Res. 2016;9:27–34. doi:10.1158/1940-6207.CAPR-15-0307
24. Davenport JR, Cai Q, Ness RM, et al. Evaluation of pro-inflammatory markers plasma C-reactive protein and urinary prostaglandin-E2 metabolite in colorectal adenoma risk. Mol Carcinog. 2016;55:1251–1261. doi:10.1002/mc.22367
25. Grunt TW. Interacting cancer machineries: cell signaling, lipid metabolism, and epigenetics. Trends Endocrinol Metab. 2018;29:86–98. doi:10.1016/j.tem.2017.11.003
26. Bhadwal P, Dahiya D, Shinde D, et al. LC-HRMS based approach to identify novel sphingolipid biomarkers in breast cancer patients. Sci Rep. 2020;10:4668. doi:10.1038/s41598-020-61283-w
27. Wang Y, Hinz S, Uckermann O, et al. Shotgun lipidomics-based characterization of the landscape of lipid metabolism in colorectal cancer. Biochimica et biophysica acta. 2020;1865:158579. doi:10.1016/j.bbalip.2019.158579
28. Kim M, Vogtmann E, Ahlquist DA, et al. Fecal metabolomic signatures in colorectal adenoma patients are associated with gut microbiota and early events of colorectal cancer pathogenesis. mBio. 2020;11:e03186–19.
29. Cubiella J, Clos-Garcia M, Alonso C, et al. Targeted UPLC-MS metabolic analysis of human faeces reveals novel low-invasive candidate markers for colorectal cancer. Cancers. 2018;10:300.
30. Yang MH, Rampal S, Sung J, et al. The association of serum lipids with colorectal adenomas. Am J Gastroenterol. 2013;108:833–841. doi:10.1038/ajg.2013.64
31. Coppola JA, Shrubsole MJ, Cai Q, et al. Plasma lipid levels and colorectal adenoma risk. Cancer Causes Control. 2015;26:635–643. doi:10.1007/s10552-015-0555-y
32. Pu S, Liu Y, Liang S, et al. The metabolic changes of artesunate and ursolic acid on Syrian golden hamsters fed with the high-fat diet. Molecules (Basel, Switzerland). 2020;25(6):1392. doi:10.3390/molecules25061392
33. Liu T, Tan Z, Yu J, et al. A conjunctive lipidomic approach reveals plasma ethanolamine plasmalogens and fatty acids as early diagnostic biomarkers for colorectal cancer patients. Expert Rev Proteomics. 2020;17:233–242. doi:10.1080/14789450.2020.1757443
34. Shen S, Yang L, Li L, et al. A plasma lipidomics strategy reveals perturbed lipid metabolic pathways and potential lipid biomarkers of human colorectal cancer. J Chromatogr B Analyt Technol Biomed Life Sci. 2017;1068-1069:41–48. doi:10.1016/j.jchromb.2017.10.004
35. Cubiella J, Clos-Garcia M, Alonso C, et al. Targeted UPLC-MS metabolic analysis of human faeces reveals novel low-invasive candidate markers for colorectal cancer. Cancers. 2018;10(9):300. doi:10.3390/cancers10090300
36. Cho E, Willett WC, Colditz GA, et al. Dietary choline and betaine and the risk of distal colorectal adenoma in women. J Natl Cancer Inst. 2007;99:1224–1231. doi:10.1093/jnci/djm082
37. Guo Y, Ren J, Li X, et al. Simultaneous quantification of serum multi-phospholipids as potential biomarkers for differentiating different pathophysiological states of lung, stomach, intestine, and pancreas. J Cancer. 2017;8:2191–2204. doi:10.7150/jca.19128
38. Zhao Z, Xiao Y, Elson P, et al. Plasma lysophosphatidylcholine levels: potential biomarkers for colorectal cancer. J clin Oncol. 2007;25:2696–2701. doi:10.1200/JCO.2006.08.5571
39. Li S, Guo B, Song J, et al. Plasma choline-containing phospholipids: potential biomarkers for colorectal cancer progression. Metabolomics. 2013;9:202–212. doi:10.1007/s11306-012-0439-z
40. Joo EJ, Weyers A, Li G, et al. Carbohydrate-containing molecules as potential biomarkers in colon cancer. Omics. 2014;18:231–241. doi:10.1089/omi.2013.0128
41. Yi M, Li J, Chen S, et al. Emerging role of lipid metabolism alterations in Cancer stem cells. J Exp Clin Cancer Res. 2018;37:118. doi:10.1186/s13046-018-0784-5
42. Crotti S, Agnoletto E, Cancemi G, et al. Altered plasma levels of decanoic acid in colorectal cancer as a new diagnostic biomarker. Anal Bioanal Chem. 2016;408:6321–6328. doi:10.1007/s00216-016-9743-1
43. Pickens CA, Lane-Elliot A, Comstock SS, et al. Altered saturated and monounsaturated plasma phospholipid fatty acid profiles in adult males with colon adenomas. Cancer Epidemiol Biomark Prev. 2016;25:498–506. doi:10.1158/1055-9965.EPI-15-0696
44. Li F, Qin X, Chen H, et al. Lipid profiling for early diagnosis and progression of colorectal cancer using direct-infusion electrospray ionization Fourier transform ion cyclotron resonance mass spectrometry. Rapid Commun Mass Spectrometry. 2013;27:24–34. doi:10.1002/rcm.6420
45. Kim BC, Shin A, Hong CW, et al. Association of colorectal adenoma with components of metabolic syndrome. Cancer Causes Control. 2012;23:727–735. doi:10.1007/s10552-012-9942-9
46. Tian Y, Wang K, Li J, et al. The association between serum lipids and colorectal neoplasm: a systemic review and meta-analysis. Public Health Nutr. 2015;18:3355–3370. doi:10.1017/S1368980015000646
47. McKeown-Eyssen G. Epidemiology of colorectal cancer revisited: are serum triglycerides and/or plasma glucose associated with risk? Cancer Epidemiol Biomark Prev. 1994;3:687–695.
48. Xie C, Wen P, Su J, et al. Elevated serum triglyceride and low-density lipoprotein cholesterol promotes the formation of colorectal polyps. BMC Gastroenterol. 2019;19:195. doi:10.1186/s12876-019-1115-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.